Back to Journals » Clinical Ophthalmology » Volume 14
Predictions of Residual Astigmatism from Surgical Planning for Topographic-Guided LASIK Based on Anterior Corneal Astigmatism (LYRA Protocol) vs the Phorcides Analytic Engine
Authors Motwani M ![]()
Received 14 July 2020
Accepted for publication 21 September 2020
Published 12 October 2020 Volume 2020:14 Pages 3227—3236
DOI https://doi.org/10.2147/OPTH.S272085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Manoj Motwani
Motwani LASIK Institute, San Diego, CA 92121, USA
Correspondence: Manoj Motwani
Motwani LASIK Institute, 4520 Executive Dr, Suite 230, San Diego, CA 92121, USA
Tel +1 (858) 554-0008
Email [email protected]
Purpose: To identify the laser programming strategy that achieves the highest refractive astigmatism outcomes accuracy between LYRA surgical planning and Phorcides surgical planning.
Methods: One hundred one eyes successfully treated with Contoura with LYRA Protocol were retrospectively surgically planned with Phorcides to determine its accuracy. Eighteen eyes that had inaccurate 3 month outcomes with LYRA were also retrospectively planned with Phorcides. Two patients with one eye treated with LYRA and one with Phorcides surgical planning were analyzed for outcomes.
Results: Retrospective Phorcides surgical planning deviated from already successful treatments with LYRA Protocol 51% of the time, with an average astigmatic deviation of 0.69 diopters (D) and an average deviation of 7.1 degrees. The percentage of eyes of the 101 successfully treated with LYRA Protocol then planned with Phorcides differed by 0.5D in 19.8%, by 0.75D in 23.8%, and by 1D in 7.9%. A retrospective analysis with Phorcides of patients treated with LYRA Protocol with residual post-operative astigmatism demonstrated that Phorcides would have increased accuracy in only 33% of patients, and not helped or decreased accuracy in the rest.
Conclusion: Phorcides was significantly less accurate in surgical planning than the LYRA Protocol overall and a 51% of primary patients could have a likelihood of significant residual astigmatism. Phorcides would also have provided a less accurate outcome in the majority of patients that needed secondary enhancement.
Keywords: Contoura, topographic-guided ablation, LYRA Protocol, Phorcides, uniform cornea
Introduction
The advent of topographic-guided ablation has brought with it a discussion on the most accurate way to plan surgically for accurate refractive outcomes while reducing light scattering higher order corneal aberrations. The initial protocols in the FDA study for Alcon WaveLight (Wavelight Inc, Erlangen, Germany) Contoura (the market name for the Alcon WaveLight topographic-guided ablation system) approval used the manifest refraction, but patients were chosen for which the Contoura measured astigmatism did not deviate dramatically from the manifest refraction.1 The authors published in 2017 the first protocol to create a more uniform cornea by using the Contoura measured astigmatism to treat the anterior corneal elevation, the LYRA Protocol (Layer Yolked Reduction of Astigmatism).1–3 Although Wallerstein et al published a study showing manifest refraction obtained good results, the study itself has issues with how it arbitrarily divides the data, does not address the topographic consequences of utilizing manifest refraction, the subjective patient quality of vision outcomes, and directly contradicts the vector astigmatism analysis study that demonstrates that manifest refraction does not work as well.
Subsequently, the Phorcides Analytic Engine (Mark Lobanoff, MD Minneapolis, Minnesota) was created and is now being supported by Alcon, Inc for use in surgical planning with Contoura.4–7 Phorcides takes the corneal higher order aberration map from the Contoura surgical planning software, re-analyzes it, requires the entry of the posterior corneal astigmatism from the Pentacam or the Gallelei, and then use other proprietary algorithms to calculate posterior ocular astigmatism which is combined with the refractive effect of the anterior HOA map in an attempt to create a more accurate refractive outcome. As Dr. Lobanoff describes in his paper. The Phorcides Analytic Engine thus considers the anterior corneal astigmatism, the topographic abnormalities that create higher order aberrations, the posterior corneal astigmatism, and the lenticular astigmatism … 7 It is an intriguing attempt to simulate in a surgical planning engine a similar goal to Ray Tracing technology (which is a different methodology utilizing hardware and software that attempts to correct all anterior or posterior astigmatism/aberrations that to focus a point of light perfectly on the retina), to correct ocular astigmatism posterior to the anterior corneal surface. This correction takes place on the anterior corneal surface in both methodologies.
To determine the accuracy of these surgical planning algorithms for clinical outcomes, this study retrospectively examined 3 categories of eyes: 101 eyes treated with Contoura with LYRA Protocol and retrospectively planned with Phorcides; 18 eyes that had inaccurate outcomes at 3 months with LYRA and retrospectively surgically planned with Phorcides, and a small sample of 2 patients with 1 eye performed with LYRA and 1 eye with Phorcides which was part of a study aborted due to results.
Materials and Methods
Patient data were retrospectively analyzed if they had myopic/astigmatic LASIK with Contoura with the LYRA Protocol (Table 1) and at least 3 month results had been obtained for stability.1–3 Patients who had greater than or equal to 0.50 diopters (D) of difference between manifest and Contoura measured astigmatism were selected. This difference of 0.5D would elucidate the differences between LYRA and Phorcides as patients with a small difference seem to result in surgical planning too close to elucidate differences between the two protocols. Each eye of each patient was required to have a plano result (in the case of a few eyes nearly plano but without subjective visual complaints) after treatment with Contoura with LYRA Protocol, and the Phorcides software was used for surgical planning in these patients retrospectively.
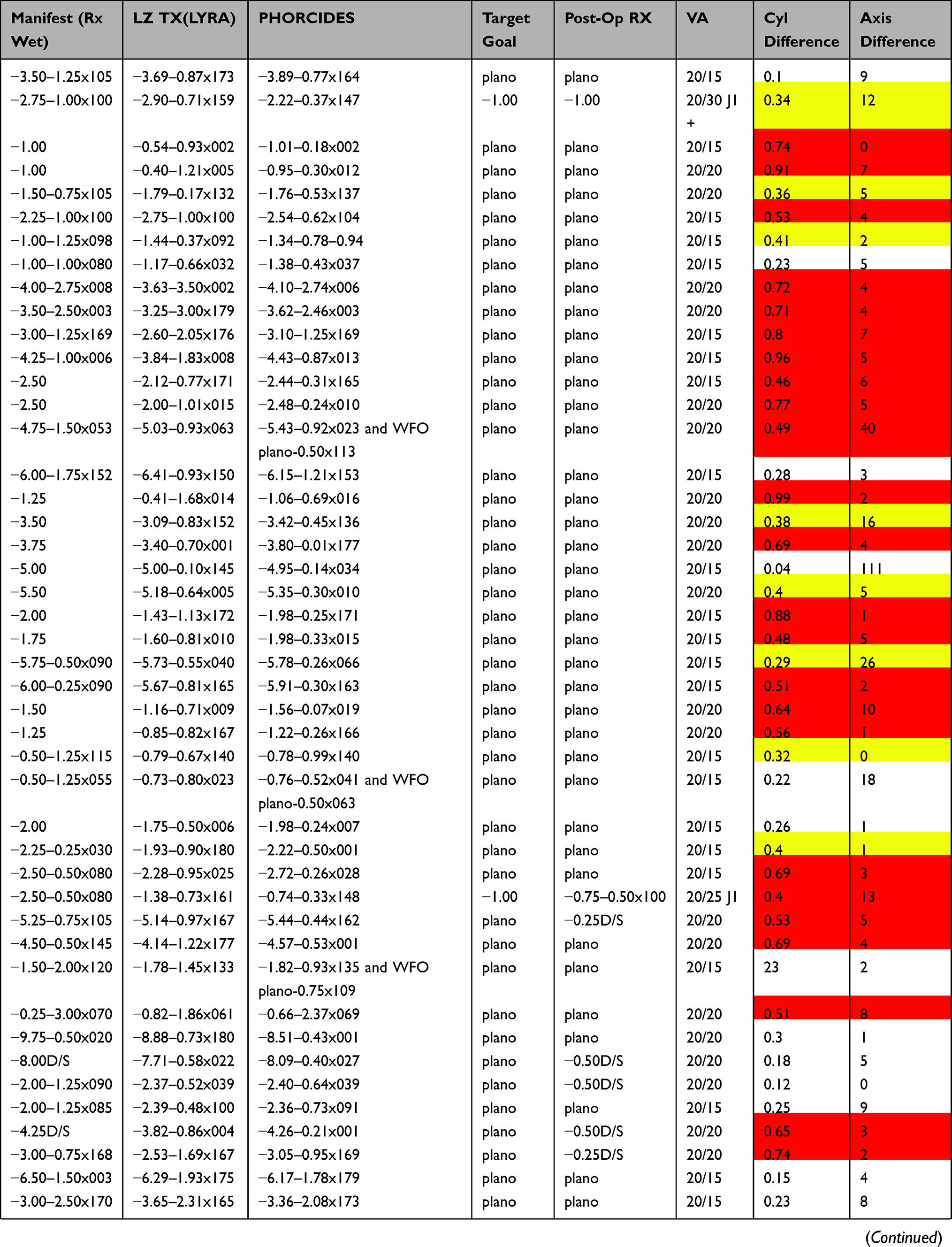 | 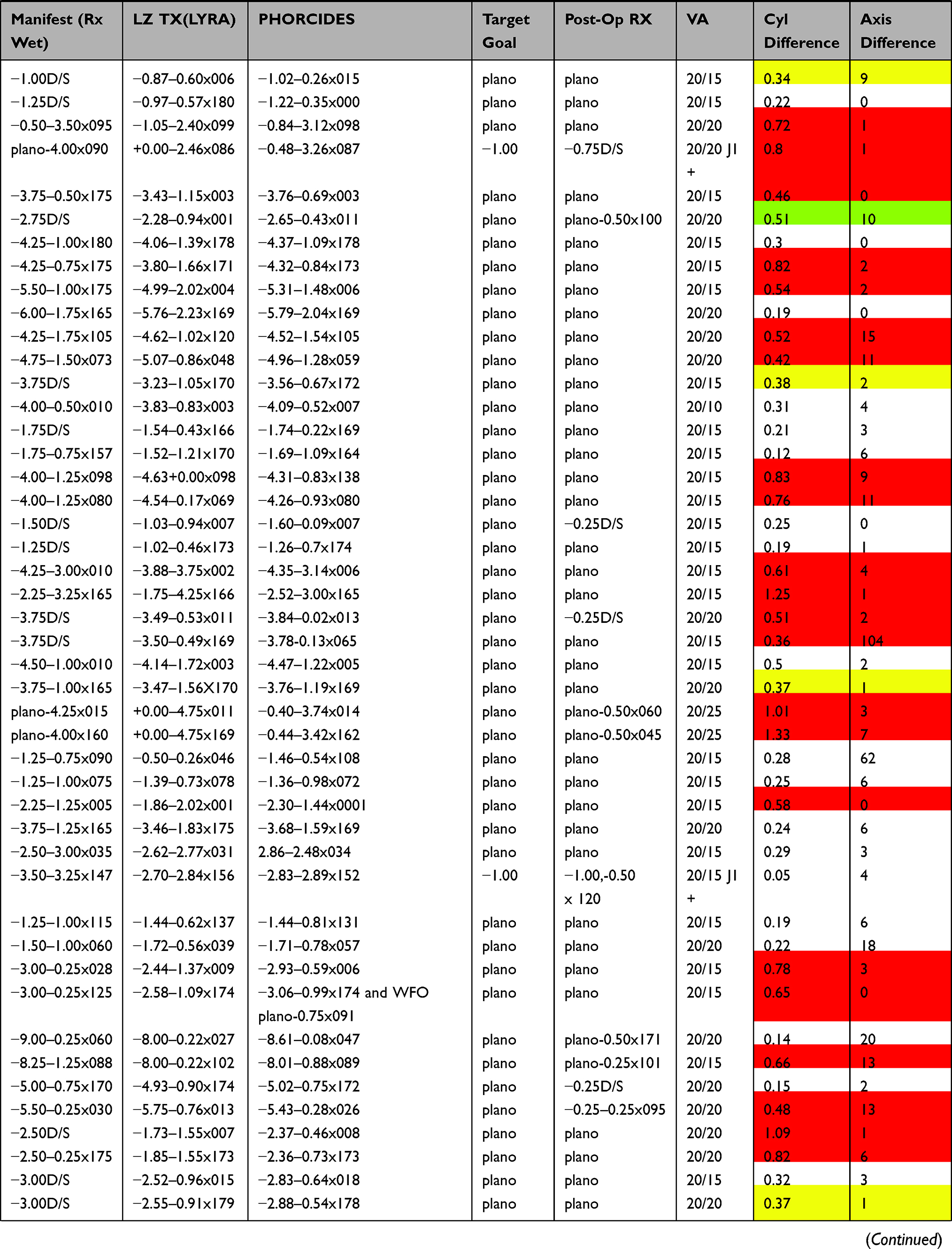 | 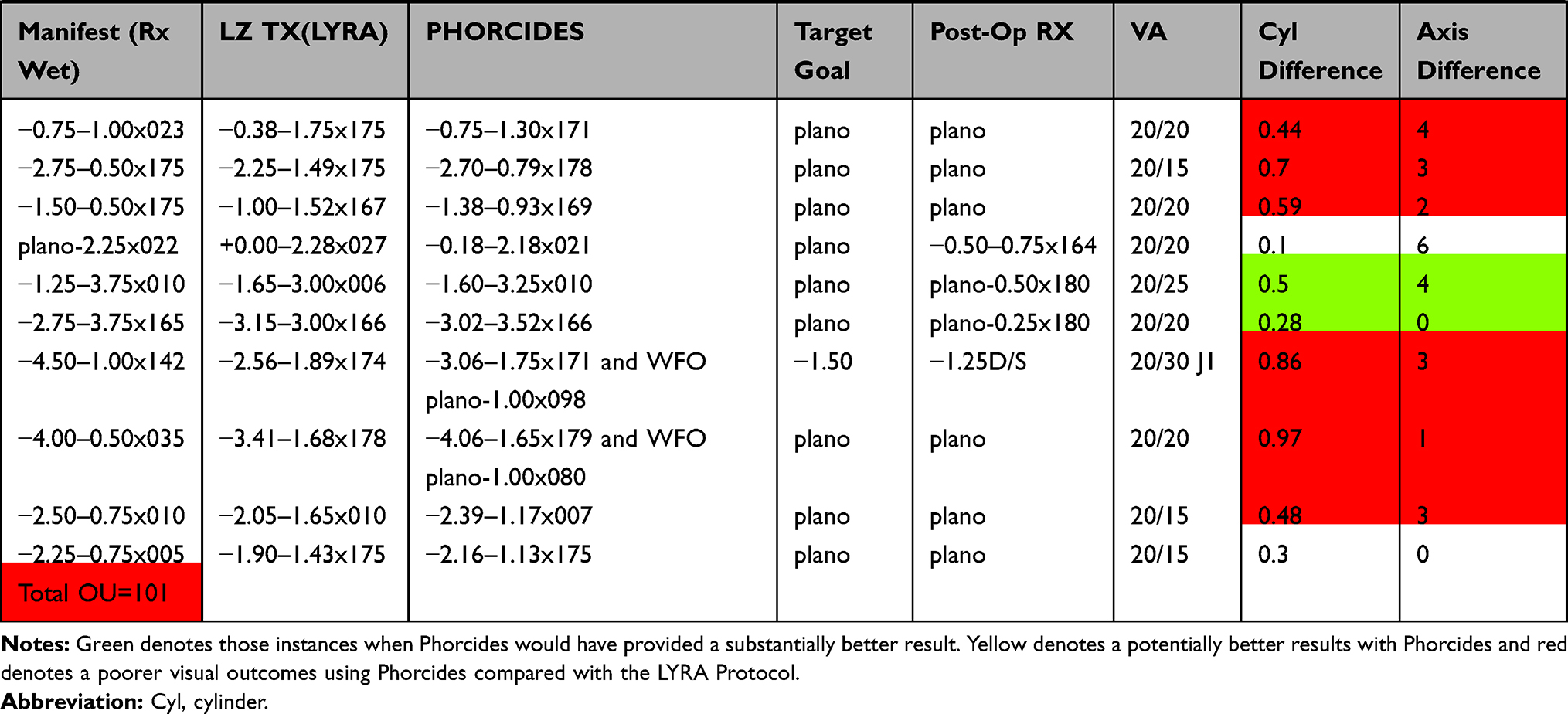 |
Table 1 Difference (in Diopters) Between Refractive Outcomes with Contoura Using the LYRA Protocol versus the Phorcides Software |
LYRA is an acronym for Layer Yolked Reduction of Astigmatism.1–3 This is a recognition of the fact that the Aberration Removal Layer is yolked/linked to the Refraction Correction layer. Contoura calculates the results of that linkage. The protocol is as follows:
- Enter the manifest/cycloplegic refraction into Contoura during Pre-surgical planning.
- Zero out the astigmatism and sphere to see ablation pattern for the Aberration Correction Layer.
- Enter Contoura measured astigmatism and axis for the final correction. The ablation map at this point should be similar to the Pentacam anterior elevation map. This will assist understanding the ablation when there is a significant discrepancy between manifest vs measured astigmatic power and axis.
- The sphere is now entered after adjustment for the spherical equivalent of the change in astigmatism.
The large difference between manifest and measured astigmatism (0.50 D or greater) was chosen to create a situation that accurately was able to demonstrate the outcomes of the different forms of planning, and to create a “stress test” for the Phorcides software to determine how the addition of calculated posterior data changed the outcome of the procedure. One hundred one (101) eyes were included in this part of the study, and each of these eyes had already been treated with Contoura with LYRA Protocol and had resulted in a successful result (ie, plano or within 0.5 D of a plano result). In addition, it was necessary for each patient to also be subjectively satisfied with their vision and have no subjective complaints. We have noted in patients who have more uniform corneas that the quality of the vision results in patients noting even small corrections or visual flaws. They rarely tolerate even 0.50 D of astigmatism, and only tolerate small amounts of sphere or astigmatism (such as 0.25 D). The majority of patients with 0.50 D of residual astigmatism requests enhancement in our clinic. Therefore, accuracy within 0.5 D of astigmatism became our standard benchmark. During the analysis comparing Phorcides planning with LYRA Protocol treatment results, a residual astigmatism close 0.5 D was rounded up to be significant, but anything less than 0.4 D was not deemed to be significant. This was performed by looking at eyes that had successful results not only by post-operative manifest refraction, but had no visual complaints that would indicate residual refractive error or incomplete aberration treatment with visual abnormalities caused by incoming light scatter.
Final manifest refraction pre-operatively and post-operatively was performed by the surgeon for the purposes of this study review, these were not performed only by technicians or ancillary staff.
Each eye was retrospectively surgically planned with Phorcides to determine if Phorcides was accurate in all of these patients (Table 1). Eighteen eyes that had residual astigmatic errors 3 months after initial correction with Contoura with LYRA protocol were then retrospectively planned with Phorcides to determine if a more accurate outcome would have resulted (Table 2). Finally, 2 patients were treated with LYRA Protocol in the right eye, and Phorcides in the left eye (Table 3).
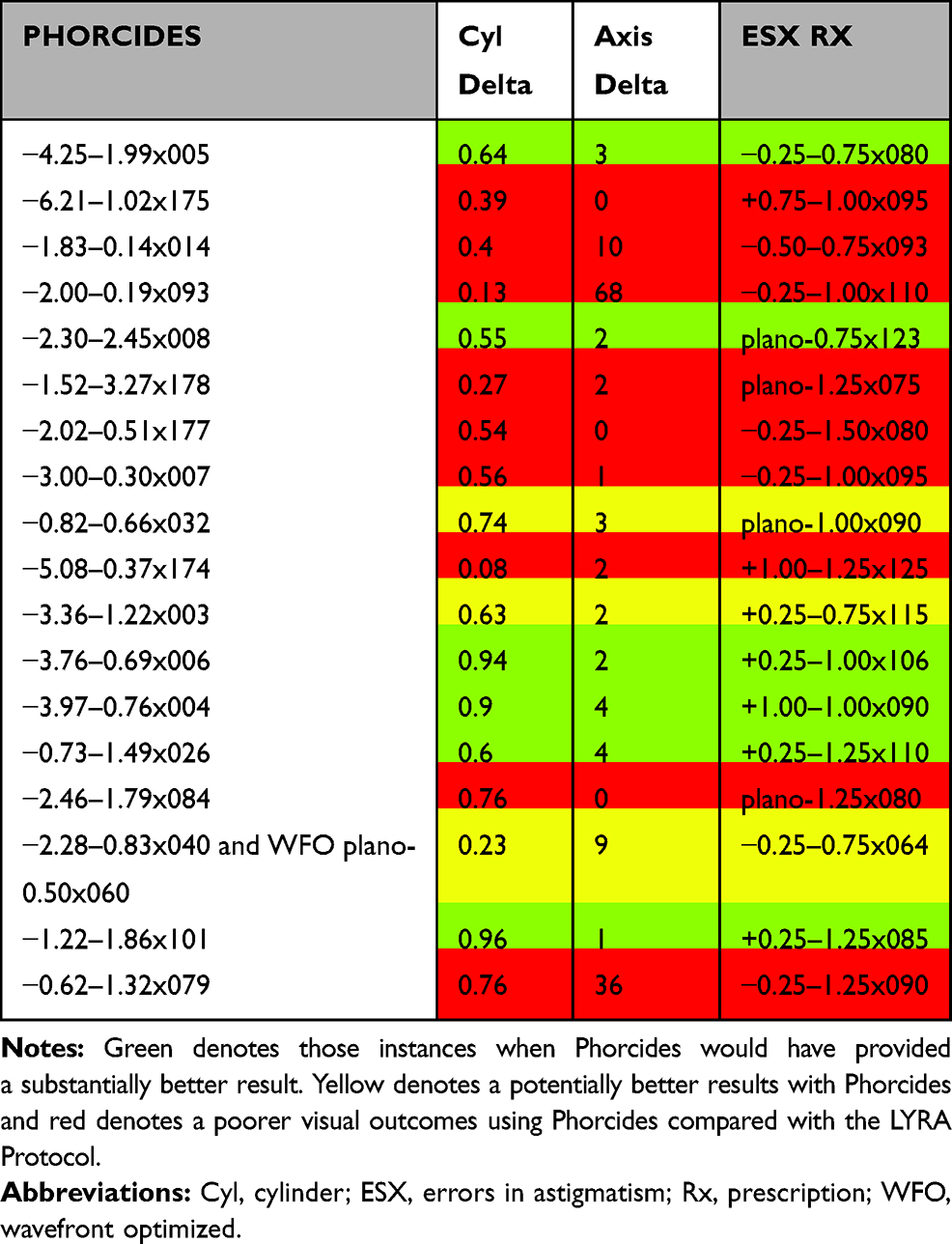 |
Table 2 Residual Astigmatic Errors 3 Months After Initial Correction with Contoura with LYRA Protocol versus Retrospectively Planning with Phorcides |
 |
Table 3 Refractive Outcomes of 2 Patients (4 Eyes) Using LYRA Protocol on the Right Eye and Phorcides on the Left Eye |
Planning for both surgical planning systems was conducted according to the recommended protocols. Phorcides planning is recommended to be performed by the technician, where the HOA pattern derived from the Contoura surgical planning station is entered into Phorcides, along with the Contoura measured astigmatism and also posterior astigmatism information from a Pentacam or Galilei Scheimpflug Analyzer. Phorcides 2.0 was used for surgical planning. Phorcides 3.0 has been released, but the author was unable to get a registered, functioning copy for this study as only Dr. Lobanoff can provide license keys and Alcon cannot. LYRA Protocol planning was done by the surgeon, eliminating disparate topographic images and then utilizing the Contoura measured astigmatism and axis along with the resultant calculated sphere to treat the patient.
Each surgery was performed by one surgeon (MM), at one center, utilizing the WaveLight EX500 laser.1–3 Flap creation was performed with either the FS200 femtosecond laser or the Moria M2 microkeratome. Patients were followed up at 1 day, 1 week, 1 month, 3 months, 6 months, and 1 year post-operatively, and uncorrected visual acuity, refraction, best corrected visual acuity, topography, epithelial thickness mapping was obtained for each visit.8 At 3 months a post-operative Pentacam image was also obtained. All of this testing was also done pre-operatively.
Although the term topography modified refraction (TMR) has been used somewhat interchangeable with Contoura measured astigmatism (CMA), we hesitate to do so as we simply have no experience with other topography units/topographic-guided software besides the WaveLight Contoura system to be able to generalize the term. We will not use TMR in this paper, but rather use Contoura measured astigmatism to be more accurate.
Patients were excluded if they could not achieve 20/20 vision before surgery, had prior refractive surgery, or were not within the FDA approved treatment parameters WaveLight Contoura treatment. Anterior segment abnormalities such as corneal ectasia or keratoconus, recurring eye disease such as severe dry eye, uncontrolled diabetes or hypertension, and pregnancy also disqualified patients from participating in the study.
All patients signed written informed consent forms allowing their data to be used in this study. This study falls under the exemption of the Health and Human Services (HHS) Policy for the Protection of Human Research Subjects 45 CFR 46.104 (d) for retrospective studies and 46.104 for exempt research, and thus, no Institutional Review Board approval was required.9,10 This study also conforms to the Declaration of Helsinki guidelines.11 There were no safety-related incidents that occurred or were reported to Alcon Inc. or WaveLight concerning patients involved in this study.
Results
Table 1 shows the results of the surgical planning of 101 eyes (Group 1) with the resultant outcomes. If Phorcides is more accurate than the LYRA Protocol, then virtually all of these eyes should have had planning results similar to those using the LYRA Protocol. The magnitude of cylinder difference between the outcome of treatment with Contoura with LYRA Protocol and the theoretical planning with Phorcides is denoted as “Cylinder Difference”, and the magnitude of axis difference is denoted as “Axis Difference.” The red highlights represent outcomes where Phorcides would have been inaccurate by 0.5 D or greater of astigmatism and would have left residual astigmatism requiring treatment. Some of these cases also had a significant difference in axis measurement as well. About half (52) of the 101 eyes (51%) were in this category, with Phorcides planning differing from LYRA by a substantial margin. The average difference in magnitude of astigmatism between Phorcides and LYRA was 0.69 D (range 0.36–1.33 D), and the average difference in axis was 7.1 degrees (range 0–76 degrees). The low of 0.36 in the range was included because it also had the highest axis deviation (76), so therefore became significant.
The cylinder difference between LYRA and Phorcides surgical planning outcomes for Group 1 was subjected to a 2-tailed T test and the outcomes were statistically significant p<0.05 (−0.00000486). The axis difference between LYRA and Phorcides was not statistically different when subjected to a 2-tailed t test, p>0.05 (0.248).
The percentage of eyes of the 101 that varied between LYRA and Phorcides in this group by 0.5D was 19.8%, by 0.75D was 23.8%, and by 1D was 7.9%.
There were 2 eyes with a post-operative outcome of −0.50 D of astigmatism from target, and one eye with an outcome −0.25 D of astigmatism from target for which Phorcides would have been more accurate than LYRA. These are highlighted in green. These 3 eyes represent 3% of the total.
The yellow highlights represent patient that do not reach the level of 0.5 D of astigmatism, but still may have an astigmatic axis of large enough difference combined with enough residual astigmatism that the patient may possibly have noticed. These included 12 eyes out of 101 (11.9%). Thirty-four eyes (33.7%) had similar surgical planning results between Phorcides and LYRA. These would have resulted in the same clinical outcomes.
Table 2 shows the results of 18 eyes (Group 2) that required secondary enhancement after treatment with Contoura using the LYRA Protocol. Here we determined if Phorcides would have provided a result that was more accurate than LYRA. Pre-op manifest refraction, Contoura with LYRA Protocol Laser Treatment, and Phorcides surgical planning utilizing pre-operative patient data are provided. The Residual Astigmatism column denotes the astigmatism that was present after laser treatment with the LYRA Protocol that needed to be enhanced (all enhancements were performed with Wavefront Optimized Treatment). Cylinder and Axis Difference denote the difference between the LYRA Protocol and Phoricdes surgical planning, and comparison to residual enhancement was made to determine if Phoricdes would have provided a more accurate outcome.
The cylinder difference between LYRA and Phorcides surgical planning outcomes for Group 2 was subjected to a 2-tailed T test and the outcomes were not statistically significant, but were very close to being so p>0.05 (0.5358). The axis difference between LYRA and Phorcides was not statistically different when subjected to a 2-tailed T test, p>0.05 (0.536).
Green denotes those instances when Phorcides would have provided a substantially better result as the post-operative residual astigmatism was approximated successfully by the difference between LYRA and Phoricdes surgical planning. This was the case for 6 eyes (33%) as Phorcides would have yielded a more accurate outcome. Yellow denotes a potentially better result and there were 3 (17%) of eyes in this category. Red denotes an outcome that Phorcides would not have provided a more accurate result, of which there were 9 eyes (50%).
Table 3 shows the refractive results of 2 patients (4 eyes) that had corrections using LYRA on the right eye and Phorcides on the left eye. Note that the planning outcomes differ significantly between Phorcides and LYRA Protocol on both eyes. The right eye on both patients was performed utilizing LYRA Protocol planning, and the left eye utilized Phorcides. Note the delta of 1.19 D on the left eye of patient 1 and the 0.58 D on the left eye of patient 2 between LYRA Protocol and Phorcides and how it relates to post-operative manifest refraction.
Discussion
In a multi-center study by Stulting et al that used vector analysis for surgical planning outcomes on patients utilizing manifest, LYRA Protocol, and Phorcides, it was noted that LYRA and Phorcides were more accurate than manifest refraction.6 Phorcides appeared to be more accurate but the study did not measure clinical outcomes, only theoretical ones. Theoretical outcomes are not the same as clinical outcomes, as the eye does not always function as a Gullstrand model and does have variability and biological reaction to treatment such as epithelial compensation. The differences between LYRA and Phorcides in this study were not large, but this study did seem to show that Phorcides was theoretically more accurate.
In this particular study, we examined 101 eyes successfully treated with the LYRA Protocol retrospectively with the Phorcides Analytic Engine. In particular, we chose eyes that had a significant difference in between manifest astigmatism and Contoura measured astigmatism to create a large enough difference to test the accuracy of Phorcides. If this difference is not large, it has been our experience that Phorcides results in treatment parameters very similar to LYRA Protocol, something that the recent Lobanoff et al study also demonstrated.7 With the understanding that Phorcides considers not just the anterior corneal aberrations and anterior corneal astigmatism that LYRA Protocol does, but in addition also considers the posterior corneal astigmatism and lenticular astigmatism, we expected to find that Phorcides would at least be similar in accuracy, and very possibly more accurate if these additional factors were significant and also accurately measured by Phorcides. It was not, with 51% of eyes evaluated likely would have resulted in worse outcomes with substantial residual astigmatism. Using Phorcides, the average deviation from LYRA was 0.69 D with an average axis deviation of 7.1 degrees. In some of these cases, a large axis difference could have incurred corneal higher order aberrations resulting in irregular astigmatism. We already know each degree of deviation of astigmatic axis during correction not only decreases astigmatic correction efficiency by 3%, but also creates a new aberrant, irregular astigmatism along a different axis.2,10 This would result in optical abnormalities and require topographic-guided ablation to correct.
Five of the eyes had Phorcides surgical outcomes that recommended a Contoura treatment followed by a WFO treatment, which would have required a second per procedure cost. As we had no access to the algorithm, we cannot explain why this would have been a recommended procedure. In none of these eyes did Phorcides appear to offer a better refractive outcome than LYRA.
We then examined 18 eyes that needed secondary enhancement after the LYRA Protocol, to see if Phorcides would be more accurate than LYRA. It was definitely more accurate in 1/3 of the eyes, but not accurate in ½ of eyes. If the remaining 3 eyes that the new analytic software could have possibly improved were included, Phorcides could have improved visual outcomes at best on ½ of the eyes needing secondary enhancement.
If Phorcides had been as accurate as LYRA in Group 1 then we could say that Phorcides is more accurate clinically than LYRA since it did provide a degree of more accuracy in the patients requiring secondary enhancements. Unfortunately, Phorcides provided worse visual outcomes than LYRA in Group 1, and at best only would have helped prevent enhancement in Group 2 about 50% of the time.
Interestingly, one of the patients that Phorcides would have benefitted was a patient in which significant epithelial compensation of corneal higher order aberration had been documented, and was actually significant enough to warrant inclusion in a separate epithelial compensation of aberration manuscript.8 As far as we know, the algorithm for Phorcides does not include any analysis of epithelial compensation of corneal higher order aberrations, so it is unknown if the increased accuracy on these two eyes is somehow coincidental.
The Phorcides surgical planning on these patients was distinctly different from manifest refraction and LYRA Protocol planning. Since each patient already had successful correction with plano outcome via LYRA Protocol, it is not difficult to see that planning with manifest or Phorcides would have resulted in a significantly different outcome. In our experience, patients treated with Contoura do not tolerate 0.50 D or greater of astigmatism post-operatively. These patients may be 20/20 and be considered a “success” via other standards, in our experience that patients are not satisfied with their vision and wish to be corrected. As previously mentioned, we find that patients with more uniform cornea and decreased corneal high order aberrations are less tolerant of any flaws in their vision. Essentially residual aberration may cause blur that masks residual astigmatism, but we have seen a more uniform cornea seems to unmask every flaw that is residual, including significant flaws and astigmatism posterior to the anterior cornea.
If Phorcides is used for smaller differences between manifest and Contoura measured astigmatism, it shows a relatively small delta with LYRA Protocol in magnitude of astigmatism and axis, and the result would likely be well tolerated. Why this is so is difficult to answer completely as the proprietary algorithm of Phorcides is not known. The one factor that stands out with Phorcides analysis, is that the astigmatism never exceeds the Contoura Measured Astigmatism (CMA) UNLESS that number is less than the manifest refraction. CMA exceeds manifest refraction in the vast majority of cases, and in these cases Phorcides has always resulted in an astigmatism in between manifest and CMA. If Phorcides accurately determines posterior astigmatism as a factor, there would be some case where the corneal and posterior astigmatism would interact in these patients and result in a number not between manifest and CMA, yet we have never seen that occur. Not having any access to the proprietary Phorcides algorithm, it is difficult to say with any certainty why this is the case.
Lobanoff et al published a study in JCRS in 2020 comparing results utilizing Phorcides surgical planning to treatment with manifest refraction. This is the first published clinical results for Phorcides, but there are a series of issues with this study. First, although the authors state that there was a significant difference between manifest astigmatism patients and those treated with Phorcides, the average difference was actually quite small, only about 0.3D or less. Furthermore, the Contoura measured astigmatism was almost exactly that of the Phorcides treatment (1.07D vs 1.11D of astigmatism) demonstrating that this study did not test the Phorcides system at all. Essentially this study shows that Phorcides essentially tracks the same as LYRA Protocol when the differences between manifest astigmatism and Contoura measured astigmatism are not large, something that we already noted in this study. Unfortunately, this study does not provide axis differences so it is impossible to tell if that was significant, and it does not provide any statistical analysis to show if the differences in astigmatism between manifest, Contoura measured and Phoricdes were significant.
Second, the results show more eyes achieving 20/15 in the Phorcides group vs the manifest astigmatism group, but interestingly, the refractive outcomes were worse for Phorcides. Based on this and the results of this particular study, Phorcides may actually be worse than not only LYRA, but manifest treatment as well.
Third, this study shows a small but significant loss of best corrected visual acuity post-operatively with Phoricdes surgical planning, something that may be occurring as Phorcides in attempting to treating lenticular astigmatism would not correctly treat the anterior elevation of the cornea, and likely leave residual higher order aberration behind. Notably, it would not make a more uniform if it differed significantly from the Contoura Measured astigmatism, and this may be the cause of best corrected visual acuity loss, something that we simply have not seen in any significant capacity in utilizing LYRA Protocol. Since this study did not look at the topographic effects at all, there is absolutely no information on the resultant corneal shape.
Fourth, the authors make some claims that I find curious, that Phorcides utilizes corneal elevation implying that somehow that Contoura without Phorcides does not. Contoura utilizes corneal elevation, and the Contoura measured astigmatism in the LYRA Protocol has been shown to treat the anterior corneal elevation creating a more uniform cornea.
Finally, in the Lobanoff study, there is no subjective patient data given at all, purely refractive and visual outcomes. The entire goal of reducing corneal aberrations is to improve vision both subjectively and objectively. No information was given as to which eye the patients preferred, the manifest or the Phorcides treatment or equally. LYRA Protocol has already shown to provide extremely high levels of subjective patient satisfaction.
Jankov et al in 200612 also questioned the wisdom of
trying to correct the anterior corneal surface using the ablation profile based on the whole eye aberrations when the anterior corneal surface aberrations are clearly preponderant.
Furthermore, they also pointed out that posterior aberrations can change with age, and postulated that recreating the natural aspheric shape and a uniform cornea might well be the ideal.
Manns et al in 200213 noted that because the corneal reshaping alters the path of light rays propagating in the eye, and although the lens and posterior corneal surface are unchanged after surgery, their contributions to the ocular aberrations will likely be different from pre-operatively.
Furthermore, as mentioned prior, the authors have noted that if the anterior elevation is not treated on a cornea, residual aberration may be left behind. In other words, anterior corneal aberrations may be left behind that cancel out posterior astigmatism/aberrations. Unfortunately, as we are learning via the use of OCT epithelial thickness mapping, this may create a reaction via epithelial hyperplasia that may affect the refractive outcome.8 We have seen even small amounts of epithelial compensation to corneal HOA (2–3 µm) can cause residual astigmatism.
It is unknown if the Ray Tracing procedure ultimately will be subject to the same issues, as it also attempts to treat aberrations at a specific time to make each incoming light ray focus on the corresponding retina. It does not account for internal structures changing with age, nor does it account for the variability of the epithelial layer. If utilized in a LASIK procedure, Ray Tracing also cannot compensate for the biomechanical corneal changes that occur in some patients after flap creation that lead to an inaccurate outcome.
The author attempted to treat patients with a similarly large difference between manifest and Contoura measured astigmatism with one eye treated with LYRA and one treated with Phorcides surgical planning. The first two patients both showed residual astigmatism via refraction post-operatively in the Phorcides eye, even though they had good outcomes for both eyes based on solely vision results (20/20 or better). This measurable astigmatism was equivalent to the difference between LYRA Protocol and Phorcides, and remained through the 6-month follow-up. This trial was then discontinued.
The authors had high hopes for Phorcides initially, as the idea behind it has great appeal. It is difficult to analyze if further development of Phorcides would increase accuracy as the underlying algorithm is not known to us nor has it been published anywhere. We are also unaware of any published clinical results. These data demonstrate that Phorcides not only does not increase the accuracy of surgical outcomes, but actually decreases accuracy in the majority of patients to an amount unacceptable in our clinical practice. We do not yet understand why the vector calculations show a greater level of accuracy in the aforementioned study, but theoretical calculations are not as important as clinical outcomes.
Although Phorcides would have helped with accuracy on a number of patients that needed secondary enhancements with LYRA, it showed significantly worse performance in Group 1 than the LYRA Protocol and would have resulted in large number of patients with significant residual astigmatism. As the axis was also different in many patients, the possibility of residual astigmatism was also present. Although the small sample size of two patients in Group 3 was not anywhere near statistical significance, the combination of the retrospective data obtained, as well as the inaccurate outcomes of the first two eyes treated with Phorcides surgical planning resulted in the discontinuation of Phorcides use in our center.
Finally, the authors repeat the cautions of past authors of correcting posterior astigmatism/aberrations on the anterior corneal surface, as the fact remains that changing corneal structures with age, issues with the treatment of posterior astigmatism on the anterior surface, and epithelial compensation of residual anterior corneal aberration remain challenging issues for of treatment protocols that attempt to treat posterior astigmatism/aberrations on the anterior corneal surface. The authors agree with Jankov et al12 and Manns et al13 that the best way to treat corneas is to attempt to create a uniform, aspheric shape to minimize light scatter and epithelial compensation, and to maximize visual clarity and accurate, stable corrections.
Acknowledgments
Acknowledgments to Guillermo Lizano for data collection and organization, Mina Botros for data organization, Athenna Menjivar for data organization and statistical analysis, and Julie Crider for editing and formatting the manuscript.
Disclosure
Dr. Motwani has received a grant from Alcon for a previous unrelated study in 2017, during the conduct of the study. Dr. Motwani received non-financial support from Optovue, Inc. (loan of Optovue Avanti, clinical support in understanding analysis of data). Dr. Motwani has a patent pending on a theoretical device that could combine corneal HOA data and epithelial thickness data to achieve a more accurate refractive outcome; and reports patents pending for: the use of topographic-guided ablation for the creation of a uniform cornea; and the use of a device to utilize both epithelial thickness and corneal aberration to make a uniform cornea. The author reports no other potential conflicts of interest for this work.
References
1. Motwani M. The use of Wavelight® Contoura to create a uniform cornea: the Lyra Protocol. Part 3: the results of 50 treated eyes. Clin Ophthalmol. 2017;11::915–921. doi:10.2147/OPTH.S133841
2. Motwani M. The use of WaveLight® Contoura to create a uniform cornea: the LYRA Protocol. Part 2: the consequences of treating astigmatism on an incorrect axis via excimer laser. Clin Ophthalmol. 2017;Volume 11:907–913. doi:10.2147/OPTH.S133840
3. Motwani M. The use of Wavelight® Contoura to create a uniform cornea: the Lyra Protocol. Part 1: the effect of higher-order corneal aberrations on refractive astigmatism. Clin Ophthalmol. 2017;11::897–905. doi:10.2147/OPTH.S133839
4. Stulting R, Lobanoff M, Stonecipher K, Wexler S. Topography-guided lasik planning: taking your outcomes to the next level. Ophthalml Times. 2019;2:15.
5. Kent C. Topography-guided ablation: state of the art. Rev Ophthalmol. 2020;22–32.
6. Stulting RD, Durrie DS, Potvin RJ, et al. Topography-guided refractive astigmatism outcomes: predictions comparing three different programming methods. Clin Ophthalmol. 2020;14:1–10. doi:10.2147/OPTH.S244079
7. Lobanoff M, Stonecipher K, Tooma T, Wexler S, Potvin R. Clinical outcomes after topography-guided lasik: comparing results based on a new topography analysis algorithm with those based on manifest refraction. J Cataract Refract Surg. 2020;46(6):814–819.
8. Motwani M. A protocol for topographic-guided corneal repair utilizing the US Food and Drug Administration-approved Wavelight Contoura. Clin Ophthalmol. 2017;11:573–581. doi:10.2147/OPTH.S127855
9. Electronic Code of Federal Regulations. Part 46-Protection of Human Subjects. 46.101. 2018. Available At: Https://Www.Ecfr.Gov/Cgi-Bin/Text-Idx?M=07&D=19&Y=2020&Cd=20200825&Submit=Go&Sid=83cd09e1c0f5c6937cd9d7513160fc3f&Node=Pt45.1.46&Pd=20180719.
10. Electronic Code of Federal Regulations. Part 46-Exempt Research. Available At: Https://Www.Law.Cornell.Edu/Cfr/Text/6/46.104. Accessed September 4, 2020.
11. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
12. Jankov MR, Panagopoulou SI, Tsiklis NS, Hajitanasis GC, M Aslanides I, G Pallikaris I. Topography-guided treatment of irregular astigmatism with the wavelight excimer laser. J Refract Surg. 2006;22(4):335–344. doi:10.3928/1081-597X-20060401-07
13. Manns F, Ho A, Parel JM, Culbertson W. Ablation profiles for wavefront-guided correction of myopia and primary spherical aberration. J Cataract Refract Surg. 2002;28(5):766–774. doi:10.1016/S0886-3350(01)01322-0
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.