Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Post-stroke bacteriuria among stroke patients attending a physiotherapy clinic in Ghana: a cross-sectional study
Authors Donkor ES ![]() , Akumwena A, Amoo P, Owolabi M, Aspelund T, Gudnason V
, Akumwena A, Amoo P, Owolabi M, Aspelund T, Gudnason V
Received 14 June 2015
Accepted for publication 30 August 2015
Published 17 March 2016 Volume 2016:12 Pages 457—462
DOI https://doi.org/10.2147/TCRM.S90474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Eric S Donkor,1,5 Amos Akumwena,1 Philip K Amoo,2 Mayowa O Owolabi,3 Thor Aspelund,4,5 Vilmundur Gudnason4,5
1Department of Medical Microbiology, College of Health Sciences, University of Ghana, Accra, Ghana; 2Public Health Unit, Korle-Bu Teaching Hospital, Accra, Ghana; 3Department of Medicine, University College Hospital, University of Ibadan, Ibadan, Nigeria; 4Icelandic Heart Association Research Institute, Kopavogur, Iceland; 5Centre for Public Health Sciences, University of Iceland, Reykjavik, Iceland
Background: Infections are known to be a major complication of stroke patients. In this study, we evaluated the risk of community-acquired bacteriuria among stroke patients, the associated factors, and the causative organisms.
Methods: This was a cross-sectional study involving 70 stroke patients and 83 age- and sex-matched, apparently healthy controls. Urine specimens were collected from all the study subjects and were analyzed by standard microbiological methods. Demographic and clinical information was also collected from the study subjects. For stroke patients, the information collected also included stroke parameters, such as stroke duration, frequency, and subtype.
Results: Bacteriuria was significantly higher among stroke patients (24.3%, n=17) than among the control group (7.2%, n=6), with a relative risk of 3.36 (confidence interval [CI], 1.40–8.01, P=0.006). Among the control group, all six bacteriuria cases were asymptomatic, whereas the 17 stroke bacteriuria cases comprised 15 cases of asymptomatic bacteriuria and two cases of symptomatic bacteriuria. Female sex (OR, 3.40; CI, 1.12–10.30; P=0.03) and presence of stroke (OR, 0.24; CI, 0.08–0.70; P=0.009) were significantly associated with bacteriuria. The etiology of bacteriuria was similar in both study groups, and coagulase-negative Staphylococcus spp. were the most predominant organisms isolated from both stroke patients (12.9%) and the control group (2.4%).
Conclusion: Stroke patients in the study region have a significantly higher risk of community-acquired bacteriuria, which in most cases is asymptomatic. Community-acquired bacteriuria in stroke patients appears to have little or no relationship with clinical parameters of stroke such as stroke subtype, duration and frequency.
Keywords: stroke-related bacteriuria, asymptomatic, urinary tract infections, hypertension, coagulase-negative staphylococci, urine
Introduction
Urine samples are normally sterile, and the presence of bacteria in urine defines bacteriuria, which is considered significant if the bacterial count is greater than 1×105 per mL.1–3 Several bacterial organisms have been implicated in bacteriuria, but the common ones include Escherichia coli and Staphylococcus spp.3–5 In urinary tract infections (UTIs), bacteriuria is accompanied by symptoms such as dysuria, pyuria, and frequent urination.1,2 UTIs can be classified into lower tract (acute cystitis) or upper tract (acute pyelonephritis) infections.1,2,6 Cystitis is associated with bladder mucosal invasion, whereas pyelonephritis is related to inflammation of the renal parenchyma, calices, and pelvis.2,6,7 UTIs are among the most commonly diagnosed infections in both hospital-acquired and community-acquired infections, and constitute an important cause of bacteremia.1,8 Several risk factors of UTIs have been identified, and include female sex, being sexually active, use of spermicidal contraceptives, urinary tract abnormalities, and antibiotic exposure.9–11 In asymptomatic bacteriuria (ASB), the bacteriuria is without the accompanying symptoms of a UTI, and ASB is more common among elderly people and in patients with diabetes, bladder catheters, and spinal cord injuries.10,11 ASB does not directly affect health and is generally not treated, unless in cases where a UTI is particularly risky, such as in pregnancy or with a condition that suppresses the immune system.3,10,11
So far, studies that have investigated bacteriuria and UTIs among stroke patients have been related to hospital-acquired infections, and have been carried out mainly in the developed world.11–13 These studies reported prevalence rates of 3%–44%, which indicates that hospital-acquired UTIs may be a common medical problem among stroke patients.11–14 Studies on community-acquired UTIs are relatively uncommon, and very little is known about the risk of community-acquired UTIs among stroke patients in either the developed or the developing world.
Currently, the majority of stroke morbidity and mortality cases occur in sub-Saharan Africa, where many infectious diseases also exert their toll.15 To the best of our knowledge, the relationship between stroke and bacteriuria has not been previously studied in any sub-Saharan African country, though this information is likely to be relevant in the management of stroke in the sub-region. In the present study, we aimed to determine the risk of community-acquired bacteriuria and UTIs among the stroke patients and to identify factors associated with the condition.
Methods
Study design and sampling
This was a cross-sectional study comprising stroke patients and apparently healthy controls. The stroke patients were recruited from the physiotherapy clinic of the Korle-Bu Teaching Hospital in Accra, Ghana from October 2013 to March 2014. Korle-Bu Teaching Hospital is the largest hospital in Ghana, and its physiotherapy unit operates an outpatient service from Monday to Friday every week.16 Using a 95% confidence level, a 10% estimated bacteriuria prevalence reported previously among stroke patients,11 and a 5% allowable error, 70 stroke outpatients were consecutively recruited into the current study. The recruitment of stroke patients was based on definite clinical and/or radiological diagnosis of stroke, and patients with ambiguous diagnosis of stroke were excluded from the study. We also excluded stroke patients who had been discharged from hospital for less than 2 months and those who had taken antibiotics 2 weeks or earlier prior to the study. A control group comprising 83 age- and sex-matched subjects, without clinical evidence of stroke or any history of the disease, were recruited from the environs of the Korle-Bu Teaching Hospital. Information on demographic features of the study participants was collected. For the stroke patients, information on stroke type, frequency, duration, risk factors/comorbidities, and side of the body affected was also collected or was extracted from their clinical records. A mid-steam urine sample was obtained from each of the study participants and was analyzed in the bacteriology laboratory of the University of Ghana Medical School, Accra, Ghana.
Laboratory analysis of urine specimens
Urine specimens were inoculated onto plates of blood agar, MacConkey agar, and cysteine lactose electrolyte-deficient agar using a standard loop calibrated to hold 0.01 mL of urine. The plates were incubated at 37°C aerobically for 18–24 hours. After incubation, bacterial colonies on the agar plates were counted, and the results were multiplied by the loop volume. A bacterial count of ≥1×105 per mL was considered as significant bacteriuria, while counts of less than 1×105 per mL were considered as no significant bacterial growth.17,18 Bacterial isolates were identified based on colonial morphology, Gram stain, and a battery of biochemical tests including catalase, coagulase, triple sugar iron, urease, indole, and citrate utilization.17
Data analysis
Data were analyzed using SPSS version 11.0 (SPSS Inc, Chicago, IL, USA). First, descriptive analyses including computation of arithmetic means, frequencies, and percentages were carried out on the study variables. Variables were compared between the stroke patients and the control group using the Student’s t-test for numeric variables and the chi-square test for categorical variables.
Univariable associations were performed between bacteriuria and all the other study variables. Subsequently, variables significantly associated with bacteriuria were used as independent variables in a logistic regression analysis to identify determinants of bacteriuria. Significance of the independent variables was assessed by P-values, odds ratios (ORs), and confidence intervals (Cis) from Wald statistics; P-values <0.05 were regarded as significant.
Ethics statement
The study was approved by the Ghana Health Service Ethics Review Committee (ethics approval identification number, GHS-ERC: 03/07/11), and informed consent was obtained from the study participants.
Results
Demographic characteristics of the study participants
The demographic characteristics of the 70 stroke patients and 83 healthy control subjects who participated in the study are reported in Table 1. The mean age of stroke patients was 55.6±11.3 years, while that of healthy controls was 53.8±10.6 years. The male-to-female ratio of the stroke patients and healthy controls were 1.5:1 and 1.4:1, respectively. Among both the stroke patients and the healthy controls, the majority were married and educated to the secondary level. There was no significant difference between the stroke patients and the healthy controls in age, sex distribution, education, or marital status.
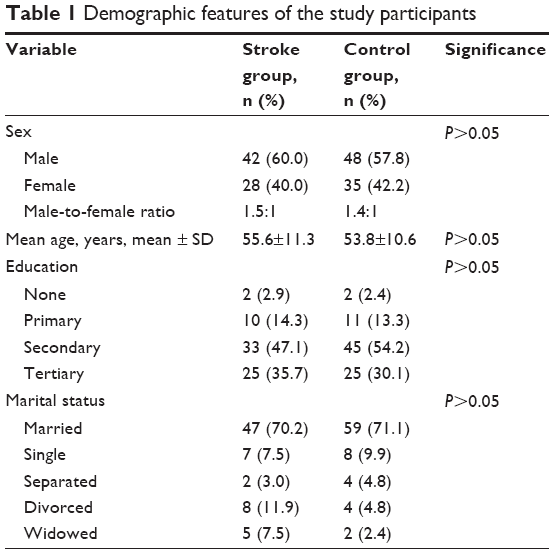 | Table 1 Demographic features of the study participants |
Clinical characteristics of the stroke patients
Sixty-three of the stroke survivors (90%) had experienced stroke once, six survivors (8.6%) had had two stroke episodes, while 1 survivor (1.4%) had had three stroke episodes; overall, the recurrence of stroke was 10%. The average period that stroke patients had lived with the disease was 12.7 (standard deviation [SD] =20.0) months. In 50.9% of the stroke cases, the disease had affected the right half of the body, while for 49.1% of the stroke cases, the left half of the body was affected. Based on radiological information (which was available for 22 patients), 27.3% of the strokes were hemorrhagic, while 72.7% of the strokes were ischemic infarctions. Hypertension was the commonest morbidity feature among the stroke patients (74%, n=52), followed by diabetes (4.3%, n=3) and asthma (1.4%, n=1).
Bacteriuria and causative organisms
Prevalence of bacteriuria, UTI, ASB, and causative organisms among the stroke patients and controls are reported in Table 2. Bacteriuria was significantly higher among stroke patients (24.3%, n=17) than among the control group (7.2%, n=6), and the relative risk was 3.36 (95% CI, 1.40–8.01). Among the 17 stroke patients who had bacteriuria, 15 had ASB, while two patients had UTI; thus, ASB and UTI prevalence among stroke patients was 21.4% and 2.9%, respectively. All six bacteriuria cases among the control group were asymptomatic; thus, prevalence of ASB and UTI among the control subjects was 7.2% and 0%, respectively. Prevalence of ASB was significantly higher among the stroke patients (21.4%) than among the control group (7.2%). However, there was no significant difference in UTI prevalence between stroke patients (2.9%) and the control group (0%).
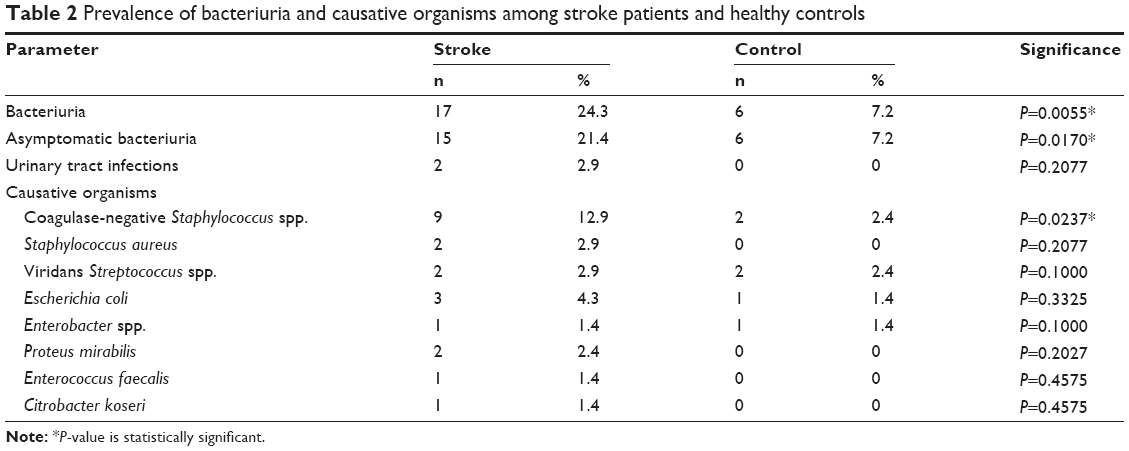 | Table 2 Prevalence of bacteriuria and causative organisms among stroke patients and healthy controls |
A wide range of bacterial organisms were isolated from the urine samples that were positive for bacteriuria (Table 2). The causative organisms fell into three groups including enterobacteriaceae, staphylococci, and streptococci. The enterobacteriaceae comprised five species (E. coli, Proteus mirabilis, Enterococcus faecalis, Citrobacter koseri, and Enterobacter spp.) and had a prevalence of 1.4%–4.3% among stroke patients and a prevalence of 0%–1.4% among the control group. Coagulase-negative Staphylococcus spp. were more predominant than Staphylococcus aureus, which was isolated exclusively from stroke patients. Overall, coagulase-negative Staphylococcus spp. were the most predominant bacteria isolated, with a prevalence of 12.9% among stroke patients and 2.4% among the control group. The streptococci isolated were all viridian streptococci and had similar prevalence rates among stroke patients (2.9%) and among the control group (2.4%). Causative organisms of bacteriuria did not show any significant differences in prevalence between the stroke patients and the control group, except for coagulase-negative staphylococcus.
The univariable analysis showed that several demographic features of the subjects, including age and education, did not have any effect on bacteriuria (Table 3). However, there was significant difference in bacteriuria between males and females, and also among different categories of marital status of the subjects (Table 3). Female subjects were significantly associated with bacteriuria (P=0.003). Subjects who were “single” were less likely to have bacteriuria (P<0.01). None of the stroke parameters including stroke frequency, duration, subtype, side of the body affected, or hypertension significantly affected bacteriuria in the univariable analysis (Table 3). In the multivariable analysis, female sex (OR, 3.40; 95% CI, 1.12–10.30; P=0.03) and the presence of stroke (OR, 0.24; 95% CI, 0.08–0.70; P=0.009) were identified as predictors of bacteriuria (Table 3).
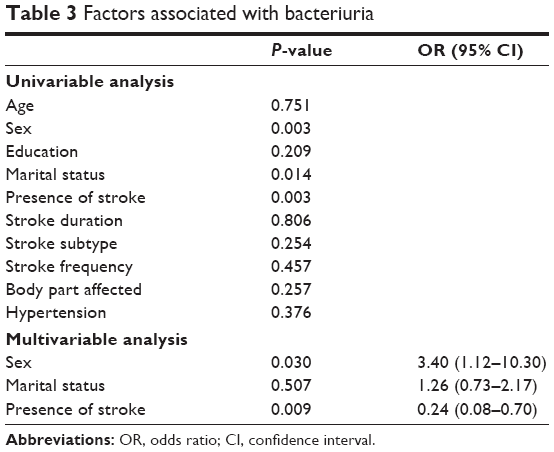 | Table 3 Factors associated with bacteriuria |
Discussion
In this study, we investigated bacteriuria among stroke patients attending a physiotherapy clinic and compared the results with bacteriuria among healthy controls recruited from environs of the study hospital. The background of the study sampling indicated that the sample was more of a community sample and that the bacteriuria cases were therefore community-acquired. Though evidence of bacteriuria occurred in 24.3% of the stroke patients, UTI occurred in only 2.9% of the stroke cases, and ASB was more common (21.4%). By comparison, a study among stroke inpatients in a hospital in Turkey reported a bacteriuria prevalence of 39.1%, and UTI and ASB prevalence rates were 27.3% and 11.8%, respectively.19 A systematic review on infections among stroke inpatients reported a UTI prevalence rate of 10%,13 which was higher than the 2.9% reported in our current study. Thus, hospital-acquired UTI appears to be a more common complication of stroke than community-acquired bacteriuria. However, further studies are required to confirm this observation.
We observed a significantly higher prevalence of bacteriuria among stroke patients (24.3%) than among the healthy controls (7.2%), which suggests that stroke predisposes an individual to community-acquired bacteriuria. The actual risk of community-acquired bacteriuria to a stroke patient was computed to be more than three-fold higher. The relatively greater susceptibility of stroke patients to infections can be attributed to several reasons. In the first place, the neurological impairment in stroke is known to cause immunodepression through several humoral and neural pathways.20 The defects in immune function in stroke patients include reduced peripheral blood lymphocyte counts, impaired T- and natural killer cell activity, and reduced mitogen-induced cytokine production and proliferation.20,21 Maximal neurological impairment occurs during the first 3 days of stroke,20 by which time the stroke patient is normally in the hospital. This situation, in addition to invasive hospital procedures (such as catheterization), may account for the higher prevalence of bacteriuria reported among stroke inpatients as compared to our stroke patients, who were outpatients. Secondly, stroke patients usually have comorbidities, which seem to make them more susceptible to infections.22 The commonest co-morbidity among our stroke patients was hypertension, but it did not show any significant association with bacteriuria. We were unable to investigate the relationship between diabetes and bacteriuria among our stroke patients, owing to the few cases of diabetes in our dataset.
In the present study, the etiology of bacteriuria was similar in stroke patients and in the healthy controls, and involved three groups/genera of organisms. Streptococcus spp. are indicative of community-acquired infections rather than hospital-acquired infections.13,23,24 The isolation of viridans streptococci from both stroke patients and from controls in the current study reflects the background of our study sample as a community sample. Staphylococcus spp. isolated from humans can be classified into two groups based on the coagulase test. These two groups are coagulase-negative staphylococci and S. aureus, which is coagulase-positive.23 S. aureus is the main staphylococcal pathogen and causes a wide range of infections, such as UTI, septicemia, carbuncles, food poisoning, and osteomyelitis.23,24 Interestingly, in the present study, coagulase-negative staphylococci, which are known to be less virulent, were more common in bacteriuria than were S. aureus. Similar findings have been reported,25,26 and these results highlight the importance of including coagulase-negative staphylococci in the surveillance of human pathogens as far UTI is concerned. Coagulase-negative staphylococci, particularly Staphylococcus epidermidis and Staphylococcus haemolyticus, are emerging as opportunistic pathogens in immunocompromised patients.27 Generally, coagulase-negative staphylococci cause infections related to prosthetic medical devices including bacteremia, endocarditis, UTIs, and endophthalmitis.27 One member of coagulase-negative staphylococci, Staphylococcus saprophyticus, is particularly associated with urinary infections.28 Enteric bacteria such as E. coli and Enterobacter spp. were commonly implicated in bacteriuria in our present study, which concurs with other studies.4,13
Antibiotic resistance has become a major problem with urinary isolates, especially with E. coli and other enteric bacteria. Owing to the small numbers of isolates of the different organisms, it was not statistically feasible to report on the antibiotic resistance patterns of urinary isolates in our current study. It has been reported that in Ghana, E. coli isolated from the urine of patients had multiple drug resistance prevalence of 40%, and the majority of the isolates (>70%) were resistant to tetracycline, ampicillin, and erythromycin.29
The significant association of bacteriuria with females in our study has previously been reported,4,10,11 and is probably due to the proximity of the female urinary system to the anus, which makes it easy for enterobacteriaceae (common etiological agents of UTI) to move into the urinary system.
Based on the results of this study, it is important to take a closer look at ASB in relation to stroke. Screening for ASB among stroke patients is rare at both hospital and community levels. However, the high ASB prevalence of 18% in the current study, coupled with immunodepression in stroke patients, seems to indicate that screening for ASB among stroke patients may be necessary, as well as its treatment. Our study was a cross-sectional study, and therefore we were not able to evaluate if ASB among stroke patients actually progresses to UTI. We hypothesize that this may be the case, given the immunodepression of stroke patients and the evidence of UTI among some of our stroke patients. Further studies to address these issues are necessary.
This study also gave us the opportunity to examine some of the epidemiological characteristics of stroke patients in the study area. The mean age of stroke patients in the present study was 55.6 years, which is quite similar to the mean age reported by a Nigerian study (59 years), but significantly lower than the mean age (69 years) of stroke patients in a German population.30 This disparity may be due to the longer life expectancy in Western countries and also the fact that age-specific incidence of stroke is relatively higher in younger age groups in sub-Saharan Africa. Hypertension was the most important co-morbidity among stroke patients, an observation that has also been reported by other studies in different parts of the world.31–33 Nevertheless, hemorrhagic stroke, which is related to hypertension, was less common among the stroke patients than ischemic stroke, which is related to comorbidities such as atrial fibrillation.
We conclude that stroke patients have a significantly higher risk of bacteriuria, which in most cases is asymptomatic. The etiology of community-acquired bacteriuria is similar in both stroke patients and healthy controls. Community-acquired bacteriuria appears to have little or no relationship with clinical parameters of stroke, such as stroke subtype, duration, and frequency.
There are a few limitations of the study. Since the stroke patients may have been hospitalized at some point, it is possible that the bacteriuria cases may be hospital-acquired, though this is less likely to be the situation considering the sampling strategy used. Additionally, coagulase-negative staphylococci are normal flora of the skin, and their occurrence in the urine samples may have been by contamination, though this is less likely, as we collected mid-stream urine to complete our sampling process.
Acknowledgments
The study was funded through a grant from the University of Iceland, and the funding received is gratefully acknowledged. The authors thank all the study participants, especially the stroke patients.
Disclosure
The authors report no conflicts of interest in this work.
References
Orenstein R, Wong ES. Urinary tract infections in adults. Am Fam Physician. 1999;59(5):1225–1234, 1237. | ||
Nicolle LE. Update in adult urinary tract infection. Curr Infect Dis Rep. 2011;13:552–560. | ||
Schnarr J, Smaill F. Asymptomatic bacteriuria and symptomatic urinary tract infections in pregnancy. Eur J Clin Invest. 2008;38(Suppl2):50–57. | ||
Alós JI. [Epidemiology and etiology of urinary tract infections in the community. Antimicrobial susceptibility of the main pathogens and clinical significance of resistance]. Enferm Infecc Microbiol Clin. 2005;23(Suppl 4):3–8. Spanish. | ||
Dias Neto JA, Martins ACP, Silva LD, et al. Community acquired urinary tract infection: etiology and bacterial susceptibility. Acta Cir Bras. 2003;18(5):33–36. | ||
Nicolle LE. Uncomplicated urinary tract infection in adults including uncomplicated pyelonephritis. Urol Clin North Am. 2008;35:1–12. | ||
Warren JW, Abrutyn E, Hebel JR, Johnson JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Clin Infect Dis. 1999;29:745–758. | ||
Hernández-Bou S, Trenchs V, Alarcón M, Luaces C. Afebrile very young infants with urinary tract infection and the risk for bacteremia. Pediatr Infect Dis J. 2014;33(3):244–247. | ||
Foxman B, Brown P. Epidemiology of urinary tract infections: transmission and risk factors, incidence, and costs. Infect Dis Clin North Am. 2003;17:227–241. | ||
Hooton TM, Scholes D, Hughes JP, et al. A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med. 1996;335:468–474. | ||
Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7:653–660. | ||
Stott DJ, Falconer A, Miller H, Tilston JC, Langhorne P. Urinary tract infection after stroke. QJM. 2009;102:243–249. | ||
Westendorp WF, Nederkoorn PJ, Vermeij JD, Dijkgraaf MG, van de Beek D. Post-stroke infection: a systematic review and meta-analysis. BMC Neurol. 2011;11:110. | ||
Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke. 1996;27:415–420. | ||
Murray CJL, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349:1269–1276. | ||
Korle-Bu Teaching Hospital. Annual Report of the Korle-Bu Teaching Hospital, 2009. Accra, Ghana: Korle-Bu Teaching Hospital; 2010. | ||
Fuller CE, Threatte GA, Henry JB. Basic examination of the urine. In: Henry JB, Davey FR, Herman CJ, et al, editors. Clinical Diagnosis and Management by Laboratory Methods. 20th ed. Philadelphia, PA: WB Saunders; 2001:367–402. | ||
Kass EH. Bacteriuria and the diagnosis of infections of the urinary tract; with observations on the use of methionine as a urinary antiseptic. AMA Arch Intern Med. 1957;100:709–714. | ||
Ersoz M, Ulusoy H, Oktar MA, Akyuz M. Urinary tract infection and bacteriuria in stroke patients: frequencies, pathogen microorganisms, and risk factors. Am J Phys Med Rehabil. 2007;86:734–741. | ||
Emsley HCA, Hopkins SJ. Acute ischaemic stroke and infection: recent and emerging concepts. Lancet Neurol. 2008;7:341–353. | ||
Chamorro A, Urra X, Planas AM. Infection after acute ischemic stroke: a manifestation of brain-induced immunodepression. Stroke. 2007;38:1097–1103. | ||
Johnsen SP, Svendsen ML, Ingeman A. Infection in patients with acute stroke. Open Infect Dis J. 2012;6:40–45. | ||
Todar K. Todar’s Online Textbook of Bacteriology. Madison, WI: University of Wisconsin-Madison; 2006. Available from: http://textbookofbacteriology.net/. Accessed June 14, 2015. | ||
Patterson MJ. Streptococcus. In: Baron S, editor. Medical Microbiology. 4th ed. Galveston, TX: University of Texas Medical Branch at Galveston; 1996. | ||
Kumari N, Rai A, Jaiswal CP, Xess A, Shahi SK. Coagulase negative Staphylococci as causative agents of urinary tract infections – prevalence and resistance status in IGIMS, Patna. Indian J Pathol Microbiol. 2001;44(4):415–419. | ||
Orrett FA, Shurland SM. Significance of coagulase-negative staphylococci in urinary tract infections in a developing country. Conn Med. 1998;62(4):199–203. | ||
Huebner J, Goldmann DA. Coagulase-negative staphylococci: role as pathogens. Annu Rev Med. 1999;50:223–236. | ||
Raz R, Colodner R, Kunin CM. Who are you – Staphylococcus saprophyticus? Clin Infect Dis. 2005;40(6):896–898. | ||
Odonkor ST, Mahami T, Addo KK. Antimicrobial sensitivity patterns of urine isolates from a large Ghanaian hospital. Int Res J Microbiol. 2011;2(7):237–241. | ||
Owolabi MO, Ugoya S, Platz T. Racial disparity in stroke risk factors: the Berlin–Ibadan experience; a retrospective study. Acta Neurol Scand. 2009;119:81–87. | ||
Bwala SA. Stroke in a sub-Saharan Nigerian hospital – a retrospective study. Trop Doct. 1989;19:11–14. | ||
Hajat C, Dundas R, Stewart JA, et al. Cerebrovascular risk factors and stroke subtypes: differences between ethnic groups. Stroke. 2001;32:37–42. | ||
Amoah AG. Hypertension in Ghana: a cross-sectional community prevalence study in greater Accra. Ethn Dis. 2003;13:310–315. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.