Back to Journals » Research and Reports in Urology » Volume 12
Peri-Operative Factors Affecting Blood Transfusion Requirements During PCNL: A Retrospective Non-Randomized Study
Authors Ketsuwan C ![]() , Pimpanit N, Phengsalae Y, Leenanupunth C, Kongchareonsombat W, Sangkum P
, Pimpanit N, Phengsalae Y, Leenanupunth C, Kongchareonsombat W, Sangkum P
Received 12 May 2020
Accepted for publication 13 July 2020
Published 22 July 2020 Volume 2020:12 Pages 279—285
DOI https://doi.org/10.2147/RRU.S261888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Chinnakhet Ketsuwan, Narutsama Pimpanit, Yada Phengsalae, Charoen Leenanupunth, Wisoot Kongchareonsombat, Premsant Sangkum
Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Premsant Sangkum Tel +66-2-2011315
Fax +66-2-2794704
Email [email protected]
Background: Percutaneous nephrolithotomy (PCNL) is accepted as the gold standard of care for the treatment of large renal calculi. Kidney hemorrhage, which requires blood transfusion, is one of the most common complications after percutaneous kidney stone surgery.
Objective: To evaluate perioperative factors associated with transfusion requirements during PCNL.
Materials and Methods: A total of 226 patients with kidney calculi undergoing PCNL between January 2011 and December 2019 were reviewed retrospectively. We analyzed the impact of perioperative clinical factors on the necessity of blood transfusion during PCNL.
Results: The overall blood transfusion rate was 9.29%. Multiple perioperative determinants were significantly correlated with the application of packed red blood cells (PRCs), including larger stone size (p = 0.006), multiple tract punctures (p = 0.029), presence of staghorn calculi (p = 0.026), and long operative time (OT; p = 0.017). Multivariate analysis demonstrated that only multiple tract punctures independently affected blood transfusion requirements during PCNL (p = 0.038).
Conclusion: In accordance with the present study, only the multiple tract punctures were associated with blood transfusion requirements in PCNL.
Keywords: kidney calculi, percutaneous nephrolithotomy, blood transfusion
Introduction
According to the guidelines of the European Association of Urology 1 and the American Urological Association,2 percutaneous nephrolithotomy (PCNL) remains the gold standard of treatment for large and complex kidney stones. Previous studies of percutaneous nephrostomy have reported blood transfusion rates in the range of 1.5–3.2%.3,4 However, the incidence of hemorrhage requiring blood transfusion was found to increase to 3.8–25% in PCNL due to the larger percutaneous tract and the necessity of renal parenchymal manipulation.5–7 Although kidney hemorrhage is one of the most frightening complications of PCNL, only 0.8% of PCNL patients require angioembolization for significant, uncontrolled hemorrhaging.8 Therefore, urologists should recognize the immediate problems during and after PCNL operations to promptly ensure proper management. In the present study, we aimed to determine the perioperative factors associated with blood transfusion during PCNL.
Materials and Methods
The principles of the Helsinki Declaration were followed during the present study, ethical approval for this retrospective cross-sectional study was performed by the Institutional Review Board of the Faculty of Medicine at Ramathibodi Hospital (ID: COA. MURA2020/711). The patient consent to review the medical record was not required by the ethical committee due to the retrospective nature of the study. All data were encrypted and kept confidential. We studied 226 patients who had undergone PCNL for kidney stones at a tertiary care referral center. All operations were conducted by highly experienced endourologists. The inclusion criteria included patients who had undergone PCNL within the time frame of January 2011 to December 2019. The exclusion criteria excluded patients who were below 18 years of age, had incomplete preoperative computerized tomography (CT) imaging, or had inadequate clinical data. All CT imaging was evaluated by two urology residents, who performed one measurement per patient. Stone size was assessed in coronal view. Preoperatively recorded data included patients’ demographic information; histories of ipsilateral operations, including open renal surgery, PCNL, and extracorporeal shock wave lithotripsy (ESWL); histories of hypertension (HT), diabetes mellitus (DM), and dyslipidemia (DLP); stone size; stone side; skin-to-stone distance; stone density; staghorn stone presence; degree of hydronephrosis; hemoglobin (Hb) levels; and estimated glomerular filtration rates (eGFR). The analyzed operative determinants included number of access sites, puncture of the renal calyx, operative duration, and intraoperative complications. Complete blood cell counts were evaluated one day before surgery and during the immediate postoperative period. The primary outcome of this measurement was packed red blood cell (PRC) transfusion status during the intraoperative and postoperative periods. Blood transfusion was indicated in patients experiencing hypovolemic shock due to blood loss (blood pressure <90/60 mmHg; heart rate >100/min) and a 1 g/dl decrease in Hb levels.
Surgical Technique
PCNL was performed using a standard approach. Each patient was arranged into a supine frog-leg position, and an open-end ureteric catheter (6F) was passed through the ureteric orifice cystoscopically through the renal pelvis. Then, each patient was turned into a prone position. Under fluoroscopic guidance, access to the pelvo-calyceal system was achieved with a percutaneous access needle (18-gauge, 20 cm) using the bull’s eye technique. The nephrostomy tract was dilated using metallic dilators or balloon dilators, and an Amplatz sheath was inserted. Rigid nephroscopy was conducted with a 26F rigid nephroscope (Karl Storz, Munich, Germany), and the stones were fragmented with a Calcuson ultrasonic lithotriptor (Karl Storz Endoskope) and removed with an Endomat LC (Karl Storz Endoskope). The residual fragmented stones were sought out by fluoroscopy. A temporary 22F nephrostomy tube was used in place at the end of operation. A 6F ureteral catheter was routinely left in place for approximately one to two days postoperatively. Prophylactic antibiotics (typically, third-generation cephalosporin) or sensitive antibiotics with urine culture were injected during the anesthetic induction period and extended until the patient was discharged.
Statistical Analysis
Data analysis was performed using STATA version 14.1 (STATA Corp., TX, USA), and patient records were compared between groups. Categorical variables were evaluated using a Fisher’s exact test, and the resulting data were reported as numbers and percentages. Continuous variables were compared using a Wilcoxon rank-sum (Mann–Whitney) test, and the resulting data were reported as medians with interquartile ranges (IQRs). A p-value less than 0.05 was considered to be statistically significant. Logistics regression was used to analyze variables associated with the endpoint (blood transfusion) in a univariate analysis. A p-value <0.05 was considered significant in the multivariate analysis.
Results
Of the 264 patients who underwent PCNL between January 2011 and December 2019, 15 were excluded due to inadequate imaging and 23 were excluded due to poor clinical data. A total of 226 patients met the inclusion criteria, including 118 females and 108 males. The mean age was 58.3 ± 11.7 years (range: 18–83 y), and the mean body mass index was 25.6 ± 4.6 kg/m2 (range: 14.5–43.4 kg/m2). The average stone size was 567.9 ± 402.4 mm2 (range: 27–2176 mm2). Staghorn stones were found in 42.9% (n = 97) of the patients. Histories of same-sided open kidney surgery, ESWL, and PCNL were demonstrated in 9 (9.6%), 57 (60.6%), and 28 (29.8%) patients, respectively. A total of 218 (96.4%) patients were managed with one-percutaneous tract, and the remaining 3.6% underwent multiple-percutaneous tract. The average operative time (OT) was 125.3 ± 49.0 minutes (range: 40–300 min), and the overall blood transfusion rate was 9.3% (n = 21).
In terms of multiple-tract puncture, the average blood loss was 506.25 ± 236.70 mL (median 425 mL; range 300–1000 mL), an average decline of Hb was 1.35 ± 1.24 g/dL (median 0.8 g/dL; range 0.5–4.1 g/dL). The average blood loss in single-tract group was 286.70 ± 317.22 mL (median 200 mL; range 5–2000 mL), the mean decline of Hb was 1.00 ± 0.79 g/dL (median 0.8 g/dL; range 0.1–4.4 g/dL). According to the univariate analysis, the perioperative determinants that affected blood transfusion requirements were stone size (p = 0.006), number of access sites (p = 0.029), presence of staghorn stones (p = 0.037), and OT (p = 0.017). There was no significant correlation between higher transfusion rate with BMI, previous surgery and skin to stone distances as shown in Table 1. In accordance with the multivariate regression analysis, the necessity of multiple tracts was the most crucial factor for PRC transfusions necessary (Table 2).
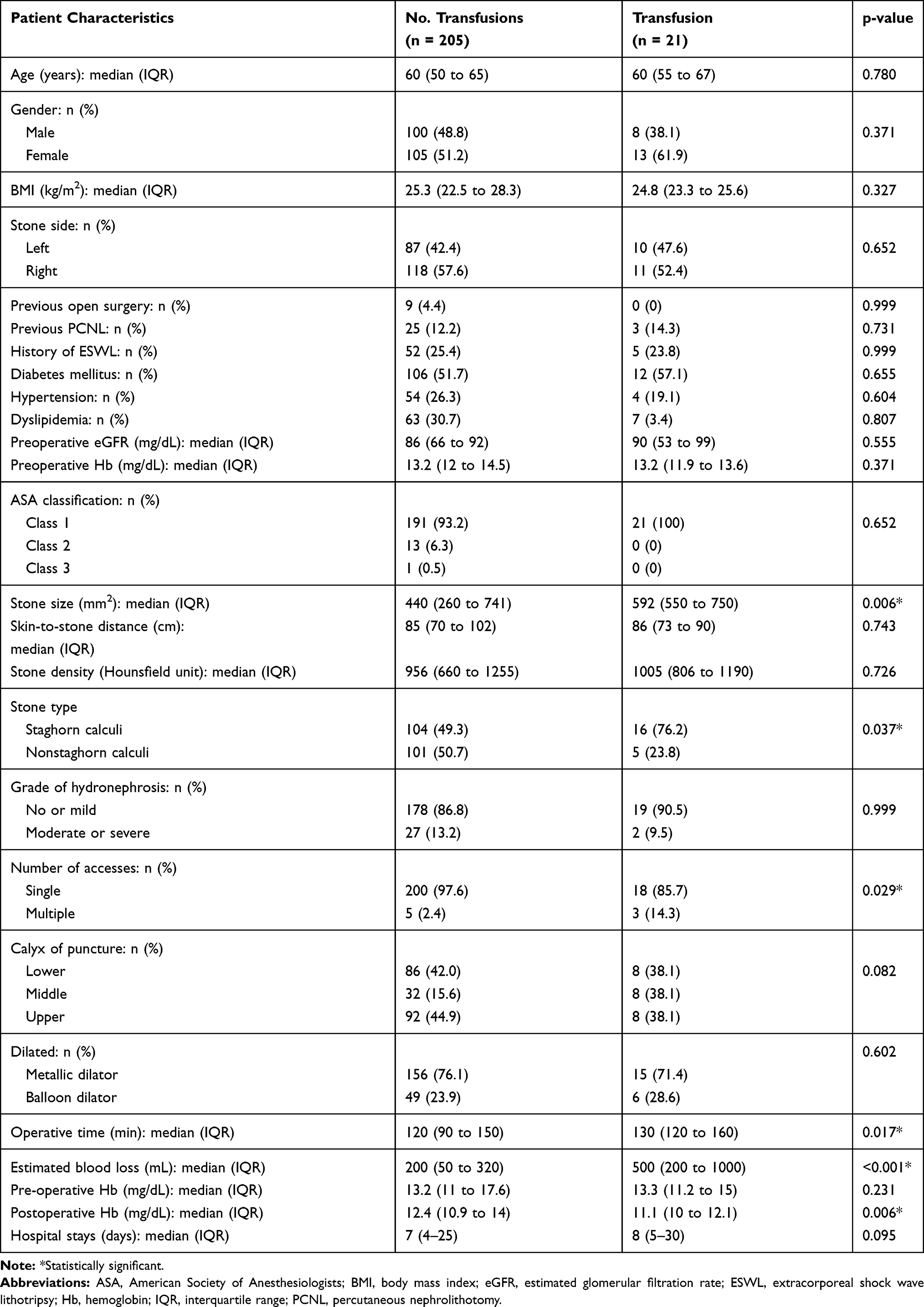 |
Table 1 Patient Characteristics |
 |
Table 2 Multivariate Analysis |
Discussion
The management of large kidney calculi has developed from open surgery to minimally invasive endoscopy procedures. The advantages of PCNL include the small incision size, shortened hospital stay requirements, the likelihood of a quicker return to work, and fewer significant complications.9,10 These advantages have resulted in a dramatic decrease in the number of open anatrophic nephrolithotomy and pyelolithotomy procedures. The goal of PCNL is to establish complete stone clearance with the lowest possible risk of morbidity or mortality. Stone burden and stone density are the most powerful predictors of the succession of this procedure.11 Nonetheless, PCNL is still associated with some complications, including pyrexia, hydrothorax, urinary septicemia, and bleeding necessitating blood transfusion.12 Among more than 5000 patients undergoing percutaneous renal surgery, slightly more than 10% experienced major complications according to the modified Clavien-Dindo system.13 Bleeding complications requiring blood transfusion were observed in these patients due to either traumatized kidney parenchyma or injury to the renal vessels.8,14 Generally, this type of hemorrhage is not significant, and hemostasis can be accomplished in such cases through conservative treatment by occluding a nephrostomy tube, applying pressure directly around the wound, and leaving the pelvo-calyceal system to clot off15 or using a 36 Fr occlusive Kaye tamponade balloon catheter.16 However, in the case of refractory to the aforementioned approaches, angioembolization may be needed. This requirement was less than 1%,5,17 with success rates above 90%8,18 in managing renal hemorrhages from arteriovenous fistulas and pseudoaneurysms.
The importance of underlying disease as a contributing factor to increased bleeding during PCNL remains a controversial subject. The present study demonstrated that patient-related factors, including HT, DM, and DLP, did not affect blood transfusion requirements. This result was similar to those of other publications. For example, Kukreja and associates19 did not find any strong association between bleeding and HT in a prospective study. However, Tolga and colleagues20 identified HT and DM as risk factors for increased renal bleeding after PCNL. Their explanation for this association was that the effect of DM on the entire arterial system contributes to microangiopathies, which are very susceptible to kidney hemorrhages.21 In terms of the influence of prior surgery (open surgery, PCNL, and ESWL) on operative difficulties in later percutaneous surgery, multiple studies have proposed that prior renal surgery does not affect bleeding complications.22,23 Our study confirmed that prior open surgery, PCNL, and ESWL are not perioperative factors for postoperative blood transfusion requirements (p = 0.999, p = 0.731, and p = 0.999, respectively).
Of the various operative factors, the univariate analysis in the present study demonstrated that high stone burden, presence of staghorn calculi, need for multiple tracts, and longer OTs are predictive determinants of blood transfusion requirements (p = 0.006, 0.037, 0.029, and 0.017, respectively). Staghorn stones and large renal calculi necessitate the extension of renal parenchyma manipulation to remove extensive stone fragmentation and consequently increase the risk of bleeding in the pelvicaliceal system. Srivastava and associates demonstrated that high stone burden is a significant predictive factor of post-PCNL renal hemorrhage.18 Additionally, Turna and colleagues found that staghorn stones had the most significant influence on bleeding in a multivariate analysis (p = 0.003).24
In the present multivariate analysis, we found that only the necessity of multiple tracts was correlated with transfusion requirements. The use of multiple percutaneous access tracts is often required in the management of patients with complex staghorn renal calculi. Hemorrhage was strongly correlated with the use of multiple tracts in the present study. We performed multiple-tract procedures with an average blood loss of 506.25 mL and a transfusion rate of 37.5%. The average decline of Hb was 1.35 g/dL, and the one-percutaneous tract group with lower bleeding was found in, average blood loss of 286.70 mL, transfusion rate of 5.5%. The mean decline of Hb was 1.00 g/dL. The effects of multiple-tract procedures on blood transfusion have been found in several studies. Akman and colleagues20 conducted multiple-tract surgery in 29.3% of procedures, necessitating transfusion 4.46 times more often than single-tract accession. Stoller and associates14 retrospectively analyzed 127 PCNL patients and found that the mean decrease in Hb for simple single-puncture and stage was 2.8 g/dL; however, the average amount of bleeding increased by twofold due to multiple punctures and/or renal pelvic perforation. The solid characteristic of the rigid nephroscope attacked the stones in different calices through multiple attempts at percutaneous access, contributing to injury of the kidney cortex and the caliceal infundibulum and therefore resulting in increased risk of bleeding.20
In the present univariate analysis of each polar puncture, we found that upper pole accession did not significantly affect bleeding any more than other approaches. Similarly, Singh and colleagues found that hemorrhagic complications did not differ significantly between upper and lower calyceal approaches.25 Although upper pole access may damage the posterior segmental artery, the aim of upper pole puncture is to accomplish exposure of the renal calices and kidney pelvis and break the stone at the upper ureter without applying torque to the kidney with the rigid nephroscope, which can cause kidney trauma and bleeding. A previous study of patients undergoing PCNL demonstrated a significant correlation between OT and blood loss in a multivariate analysis (p = 0.001).26 The present study also indicated that longer OT is correlated with an increased risk of requiring blood transfusion. Increased bleeding during prolonged operations may be due to extended injury to the renal cortex.
Multiple devices are being developed to reduce the disadvantageous effect of multiple steps of accession into the kidney. For example, the evolution of balloon dilation, considered to be the most modern and safe dilation equipment, has made PCNL dilatation easier. However, the present study did not demonstrate a significant difference between the blood transfusion rates of the two dilation groups. Our results were similar to those of Gonen and associates, who compared Amplatz dilation with balloon dilation for PCNL and demonstrated no significant differences in postoperative Hb concentrations or PRC transfusion rates between the two groups (p = 0.601 and p = 0.687, respectively).27 However, some studies have found balloon dilators to cause less blood loss than Amplatz fascial dilators.28
There were several limitations to the present study. First, the data analysis was retrospective and could have therefore been biased. Second, renal calculi were eliminated during the lithotripsy period in all patients using ultrasonic lithotripsy. Consequently, these determinants were not investigated in this study. Finally, the collection of data from multiple endourologists may have influenced the reliability and validity of the study.
Conclusion
In summary, multiple access sites significantly increased blood transfusion requirements during PCNL. Conversely, underlying disease, dilator type, and polar accession did not significantly affect blood transfusion requirements during PCNL.
Acknowledgments
We would like to express our appreciation for all the participants and health personnel involved in this study as well as the support of the section of Clinical Epidemiology and Biostatistics, Faculty of Medicine, Ramathibodi Hospital.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Turk C, Neisius A, Petrik A, Seitz C, Tepeler A, Thomas K Urolithiasis. 2018. Available from: https://uroweb.org/wp-content/uploads/EAU-Guidelines-onUrolithiasis_2017_10-05V2.pdf.
2. Preminger GM, Assimos DG, Lingeman JE, Nakada SY, Pearle MS. Wolf JS Jr Chapter 1: AUA guideline on management of staghorn calculi: diagnosis and treatment recommendations. J Urol. 2005;173:1991–2000.
3. Rana AM, Zaidi Z, El-Khalid S. Single-center review of fluoroscopy-guided percutaneous nephrostomy performed by urologic surgeons. J Endourol. 2007;21(7):688–691. doi:10.1089/end.2006.0281
4. Wah TM, Weston MJ, Irving HC. Percutaneous nephrostomy insertion: outcome data from a prospective multi-operator study at a UK training centre. Clin Radiol. 2004;59(3):255–261. doi:10.1016/j.crad.2003.10.021
5. Keoghane SR, Cetti RJ, Rogers AE, Walmsley BH. Blood transfusion, embolisation and nephrectomy after percutaneous nephrolithotomy (PCNL). BJU Int. 2013;111(4):628–632. doi:10.1111/j.1464-410X.2012.11394.x
6. Muslumanoglu AY, Tefekli A, Karadag MA, Tok A, Sari E, Berberoglu Y. Impact of percutaneous access point number and location on complication and success rates in percutaneous nephrolithotomy. Urol Int. 2006;77(4):340–346. doi:10.1159/000096339
7. Netto NR
8. Kessaris DN, Bellman GC, Pardalidis NP, Smith AG. Management of hemorrhage after percutaneous renal surgery. J Urol. 1995;153(3 Pt 1):604–608. doi:10.1016/S0022-5347(01)67659-6
9. White EC, Smith AD. Percutaneous stone extraction from 200 patients. J Urol. 1984;132(3):437–438. doi:10.1016/S0022-5347(17)49683-2
10. Al-Kohlany KM, Shokeir AA, Mosbah A, et al. Treatment of complete staghorn stones: a prospective randomized comparison of open surgery versus percutaneous nephrolithotomy. J Urol. 2005;173(2):469–473. doi:10.1097/01.ju.0000150519.49495.88
11. Ketsuwan C, Kongchareonsombat W, Sangkum P, Kijvikai K, Sananmuang T, Leenanupunth C. Perioperative renal calculus factors affecting percutaneous nephrolithotomy outcomes. Thai J Urol. 2019;40(2):01–08.
12. Taylor E, Miller J, Chi T, Stoller ML. Complications associated with percutaneous nephrolithotomy. Transl Androl Urol. 2012;1(4):223.
13. Labate G, Modi P, Timoney A, et al. The percutaneous nephrolithotomy global study: classification of complications. J Endourol. 2011;25(8):1275–1280. doi:10.1089/end.2011.0067
14. Stoller ML, Wolf JS
15. Lee KL, Stoller ML. Minimizing and managing bleeding after percutaneous nephrolithotomy. Curr Opin Urol. 2007;17(2):120–124. doi:10.1097/MOU.0b013e328010ca76
16. Kaye KW, Clayman RV. Tamponade nephrostomy catheter for percutaneous nephrostolithotomy. Urology. 1986;27(5):441–445. doi:10.1016/0090-4295(86)90411-5
17. El Tayeb MM, Knoedler JJ, Krambeck AE, Paonessa JE, Mellon MJ, Lingeman JE. Vascular complications after percutaneous nephrolithotomy: 10 years of experience. Urology. 2015;85(4):777–781. doi:10.1016/j.urology.2014.12.044
18. Srivastava A, Singh KJ, Suri A, et al. Vascular complications after percutaneous nephrolithotomy: are there any predictive factors? Urology. 2005;66(1):38–40. doi:10.1016/j.urology.2005.02.010
19. Kukreja R, Desai M, Patel S, Bapat S, Desai M. Factors affecting blood loss during percutaneous nephrolithotomy: prospective study. J Endourol. 2004;18(8):715–722. doi:10.1089/end.2004.18.715
20. Akman T, Binbay M, Sari E, et al. Factors affecting bleeding during percutaneous nephrolithotomy: single surgeon experience. J Endourol. 2011;25(2):327–333. doi:10.1089/end.2010.0302
21. Tefekli A, Kurtoglu H, Tepeler K, et al. Does the metabolic syndrome or its components affect the outcome of percutaneous nephrolithotomy? J Endourol. 2008;22(1):35–40. doi:10.1089/end.2007.0034
22. Yuruk E, Tefekli A, Sari E, et al. Does previous extracorporeal shock wave lithotripsy affect the performance and outcome of percutaneous nephrolithotomy? J Urol. 2009;181(2):663–667. doi:10.1016/j.juro.2008.10.016
23. Reddy SV, Shaik AB. Outcome and complications of percutaneous nephrolithotomy as primary versus secondary procedure for renal calculi. Int Braz J Urol. 2016;42(2):262–269. doi:10.1590/S1677-5538.IBJU.2014.0619
24. Turna B, Nazli O, Demiryoguran S, Mammadov R, Cal C. Percutaneous nephrolithotomy: variables that influence hemorrhage. Urology. 2007;69(4):603–607. doi:10.1016/j.urology.2006.12.021
25. Singh R, Kankalia SP, Sabale V, et al. Comparative evaluation of upper versus lower calyceal approach in percutaneous nephrolithotomy for managing complex renal calculi. Urol Ann. 2015;7(1):31–35. doi:10.1016/j.urology.2015.01.033
26. Yamaguchi A, Skolarikos A, Buchholz NP, et al. Operating times and bleeding complications in percutaneous nephrolithotomy: a comparison of tract dilation methods in 5,537 patients in the clinical research office of the endourological society percutaneous nephrolithotomy global study. J Endourol. 2011;25(6):933–939. doi:10.1089/end.2010.0606
27. Gonen M, Istanbulluoglu OM, Cicek T, Ozturk B, Ozkardes H. Balloon dilatation versus Amplatz dilatation for nephrostomy tract dilatation. J Endourol. 2008;22(5):901–904. doi:10.1089/end.2007.0167
28. Safak M, Gogus C, Soygur T. Nephrostomy tract dilation using a balloon dilator in percutaneous renal surgery: experience with 95 cases and comparison with the fascial dilator system. Urol Int. 2003;71(4):382–384.alis. doi:10.1159/000074090
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.