Back to Journals » Patient Preference and Adherence » Volume 11
"Patients' understanding is the problem": physicians' views of nonadherence among Arabs with type 2 diabetes
Authors Waheedi M ![]() , Jeragh-Alhaddad FB, Awad AI
, Jeragh-Alhaddad FB, Awad AI ![]() , Enlund H
, Enlund H
Received 31 March 2017
Accepted for publication 25 July 2017
Published 17 August 2017 Volume 2017:11 Pages 1413—1421
DOI https://doi.org/10.2147/PPA.S138468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mohammad Waheedi,1 Fatima B Jeragh-Alhaddad,1 Abdelmoneim Ismail Awad,1 Hannes Enlund2
1Faculty of Pharmacy, Kuwait University, Kuwait; 2Finnish Medicines Agency, Kuopio, Finland
Purpose: Nonadherence to diabetes medication is a significant barrier toward achieving positive treatment outcomes. There is an abundance of research looking at the problem from the patient perspective, but less from the provider perspective. The Middle East region has one of the highest prevalences of type 2 diabetes in the world, with special cultural characteristics, which require research attention. The aim of this study was to explore the views of primary-care physicians on medication nonadherence among type 2 diabetes patients.
Materials and methods: A descriptive qualitative study was performed using one-on-one semistructured interviews of 21 primary-care physicians who were selected using stratified and random sampling from polyclinics in the five health districts in Kuwait. The interviews elicited the participants’ views about barriers and facilitators of medication adherence in type 2 diabetes patients. The interviews were audio-recorded and transcribed verbatim. Thematic content analysis with constant comparison was used to generate the codes and themes to arrive at a core category.
Results: Patient understanding, including knowledge, beliefs, and attitudes, was identified by respondents as the core determinant of medication nonadherence in type 2 diabetes. This was composed of six major themes: four against understanding and two for understanding. The ones against were “Patients do not understand diabetes”, “Patients do not understand the importance of medications”, “What the patient hears from friends is more important than what the doctor says”, “Patients are in denial (or difficult)”. Themes for understanding were “I need to educate more” and “Patients must hear it from other sources”.
Conclusion: That lack of understanding among patients results in medication nonadherence is the dominant view of primary-care physicians. This finding has implications in relation to the evolution of diabetes care toward more patient-centeredness within the cultural context.
Keywords: medication adherence, primary-care providers, qualitative, patient-centeredness, Kuwait
Introduction
Diabetes is a major clinical and public health concern in the Middle East, and particularly in Kuwait. The most recent figures on the overall prevalence rate of type 2 diabetes among Kuwaiti adults aged 20–79 years were between 14.3% and 17.9%.1,2 In a household survey, it was found that about half of persons aged ≥50 years have type 2 diabetes.3
Medication therapy plays a central role together with dietary measures and physical activities in the management of type 2 diabetes patients. In general, nonadherence to medication has ranged from 7% to 64% for oral antidiabetic medications and 19% to 46% for insulin therapy.4 In Kuwait, parallel to findings elsewhere, only 47% were found to be optimally adhering to medication regimens in type 2 diabetes.5
Research in the Middle East has identified that factors related to poor health knowledge, different beliefs, and culture, together with sedentary lifestyles, play a significant role in patients’ self-management of type 2 diabetes.6 Traditional Western perspectives used to explain nonadherence to medication may not fully explain these behaviors in Arab patients. Cultural factors and lifestyle, including religious beliefs, add to the complexity of issues, which need to be addressed when taking medication.7
The health-care providers’ perspective has received less attention from research exploring the medication adherence problem in type 2 diabetes: only nine of 86 studies reviewed on the topic focused primarily on the providers’ perspective.8 In the Middle East, the providers’ perspective is even more scarce.9,10 This is a particularly important point, since how physicians view the adherence problem influences their approach and strategies in managing nonadherence in daily practice. Insight gained from the physician perspective in this cultural context may help in designing effective interventions to improve adherence and outcomes of treatment. As such, this study aimed to explore the views of primary-care physicians (PCPs) on nonadherence in type 2 diabetes, specifically on the reasons and ways to unravel the problem in the Kuwaiti context.
Materials and methods
Study design and population
Interviews were conducted during January to May 2016. The study population consisted of PCPs from the country’s five health-care districts. Ethical approval for this study was obtained from the research ethics committee of the Ministry of Health, State of Kuwait. All the participants were informed of the details of the study and signed a consent form before the beginning of interviews.
A sample of 25 PCPs was selected using stratified and random sampling. In qualitative methods, there is no gold standard to calculate the number of people to interview; in practice, however, 12–26 persons is considered sufficient to most researchers.11 The aim is to provide rich descriptions of participants’ experiences, rather than quantifying a phenomenon within a large number of participants. The appropriate sample size is reached when the researchers find no new information emerging from additional interviews, reaching what is referred to as data “saturation”.12
The stratification of the sample was at the level of the five health-care districts of Kuwait. Five PC centers that provide outpatient diabetes clinics were selected randomly from each health-care district, a total of 25 clinics. Physicians were approached while they were working in their clinics and invited to participate. Those agreeing to participate were either interviewed at around the same time if they were available or were interviewed at a later day/time by appointment. All interviews were completed at the PC clinic where the PCP was serving.
The interviews were completed with 21 PCPs, achieving saturation of data. Semistructured face-to-face interviews were conducted to elicit PCPs’ views and perspectives. The interview schedule was developed based on a review of the literature8,13,14 and the findings of a similar study, but with patients in Kuwait.15 Topics included in the schedule focused on how medication adherence is defined in type 2 diabetes, how it is assessed, barriers, interventions that address medication nonadherence, and support needed from health-care providers, specifically pharmacists, in addressing nonadherence. The duration of the interviews was 35–85 minutes. All interviews were conducted by the first author, audio-recorded, and transcribed verbatim.
Data analysis
The verbatim transcriptions were content-analyzed using a thematic analysis method, first by open coding and then by refining and grouping codes into categories representing themes emerging from the data.16 The analysis process was carried out using qualitative data analysis software (MAXQDA version 12) to facilitate the systematic process of sifting, charting, and sorting material according to key issues and themes. An emerging core theme was continually refined, tested, and revised using constant comparison.12,17
To ensure the reliability and validity of coding, the second author, who has particular experience in qualitative research, in addition to her competence in the Kuwaiti language and culture as a native speaker, was involved in the analysis. Five interview transcripts were cocoded separately and independently by the first and second authors. Intercoder reliability was estimated using a formula of intercoder reliability = number of agreements/(number of agreements + number of disagreements) and found to be 91% on average. In addition, several measures were taken to ensure the validity of findings. For example, a large number of quotes with rich data were used; this allowed illustration of contexts within which the data emerged. If new codes were added, all previous interviews were revisited and examined for the relevance of these codes. This ensured consistency and thoroughness of coding.
The generated themes and the emerging core category from data were tested by going back to the transcripts and searching for negative cases. When there were opposing views, explanations were sought for the new findings. This also ensured the inclusion of all findings, rather than selected views.
Results
A total of 21 PCPs were approached and agreed to participate in the study. The sample was composed of eight (38%) females and 13 (62%) males, with an average experience in diabetes PC of 11 years, ranging 1–25 years. A variety of specialties were represented: seven (33%) from internal medicine, six (29%) from family medicine, five (24%) from endocrinology or diabetes, and three (14%) with no postgraduate specialty. The five health districts in Kuwait were represented in the sample: five participants from the capital, five from Farwaniya, four from Jahra, four from Ahmadi, and three from Hawalli.
In response to the interviewer request to define the term “medication adherence” in type 2 diabetes patients, all respondents gave answers referring to the traditional compliance conception: the patient follows a prescribed regimen with no reference to patient agreement or participation. The emerging core category of “patient understanding” related to patients’ knowledge, attitudes, and beliefs that were recurrently appearing in PCPs verbatim as core influencers of medication adherence in type 2 diabetes patients. This core category is represented by six major themes (Figure 1) and described in the following sections, supported by verbatim quotes from the PCPs for clarity. The first four themes represent forces against patient understanding, while the remaining two are forces for patient understanding.
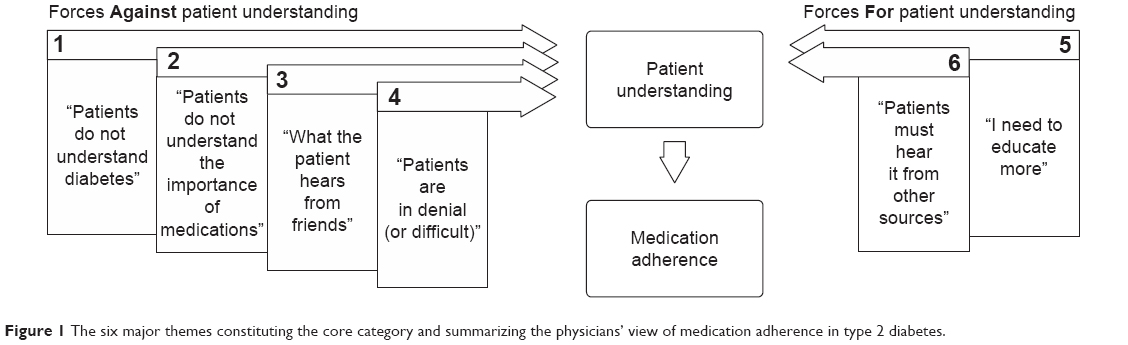 | Figure 1 The six major themes constituting the core category and summarizing the physicians’ view of medication adherence in type 2 diabetes. |
Theme 1: “Patients do not understand diabetes”
In general, the participants in this study perceived patients to have insufficient knowledge about diabetes and its consequences. All (n=21) of the respondents brought up misconceptions in the patient’s mind as a role in nonadherence, with about half (n=11) of them pointing to it as the first and primary source of medication nonadherence:
The principal problem goes back to the level of knowledge that a patient possesses. [Interviewee 14]
Some patients still don’t understand what diabetes is. Even after providing them with an explanation, it is not enough: they still don’t comprehend the complications that could occur. I repeat the same information during every visit but they still don’t get it … even though diabetes is supposed to be a well-known disease. [Interviewee 9]
The problem with diabetes is that the patient does not know that they have a problem; if a patient stops taking their medication for a day or two, a week or two, they don’t feel anything different. [Interviewee 4]
Rejection of the disease and refusal to accept the disease; so they would tell you that they have high blood sugar levels because they ate too much last night or they were stressed out. So they avoid taking their medicine and eventually their blood sugar levels rise, leading to a dire situation where they need complex interventions. [Interviewee 15]
A commonly perceived problem in patients’ conception of diabetes is that they believe a cure is possible and are in constant search for a cure. Some patients deal with diabetes as an acute illness that they think they can be healed from somehow:
Some of the elderly who are resistant don’t believe they are sick; they consider it a temporary disease and believe it will go away. [Interviewee 19]
Additionally, some patients test and rechallenge the diagnosis and try to prove that they are cured, as in the following example:
When you tell a patient that they are diabetic, they go and stop eating sugars and other things, then come back and tell you they don’t have diabetes anymore, that they are healthy now, and that’s because they had stopped eating and their weight has gone down, but then they go back to their normal stressful life and their old eating habits resume, and diabetes shows up again. [Interviewee 11]
Theme 2: “Patients do not understand the importance of medications”
The vast majority of respondents (n=18) felt that misunderstanding and misconceptions about medications in patients and in society as a whole is another primary cause of patient nonadherence:
They don’t understand the danger in stopping the medication, because of ignorance of the diseases and of its consequences, that it can lead to stroke or heart attack or death. [Interviewee 18]
Participants also referred to a general dislike of medicines among patients as a reason behind nonadherence:
Kuwaiti patients have a phobia from medicines. [Interviewee 13]
They like to feel “normal”, because once they start taking medications they admit a sickness, or they don’t like the idea of others seeing them taking medications. They feel alienated or feel the medications are not for their age, but maybe for someone older. So they drink green tea or take a specific herbal/alternative medicine, or someone convinces them to quit taking their medicine and take this herb instead. [Interviewee 6]
Almost all (n=20) of the respondents mentioned patients experiencing a side effect as a cause of discontinuing medications and reluctance to retake them:
For example, Glucophage [metformin] causes bloating, constipation, and diarrhea, so they discontinue it after their first try … Some people get hypoglycemia with other medications, sudden falling in blood glucose levels; they start hating the medicine and discontinue it. [Interviewee 2]
Increased weight is another cause and a big factor [for nonadherence], especially with women. [Interviewee 6]
Theme 3: “What the patient hears from friends is more important than what the doctor says”
Many of the study participants (n=14) expressed some form of a struggle with patients in correcting the misinformation patients brought with them from the social environment. They talked about the diwaniya, which is a popular gathering place where men meet at night to socialize, as the main source of rumors and inaccurate information. The PCPs often spend a great deal of time with patients to correct this misinformation:
Arabs tell you that a friend had a particular experience; therefore, the friend talks about an experience … their [low] opinion of the doctor is due to their lack of belief in science; they believe science is something that came from the West to profit off of them … due to lack of education, or they never studied science or understood it, so they think science can include delusions, while what their friend tells them is a personal experience, and that is a credible reality to them. [Interviewee 5]
Social rumors and myths about side effects are common in this context of local society. Participants talked about patients confusing complications of diabetes with side effects of the medication. For example, patients hearing about someone losing a limb shortly after the addition of insulin to the treatment regimen: the insulin introduction is mistaken as causing such amputation:
Not a real side effect; they hear it from a patient in a diwaniya. They tell them that this medicine affects the kidney and that they should not take it. They listen to what their friend says. [Interviewee 1]
In reference to the widespread rumors/myths and misinformation in the social interactions of patients, one physician referred to it as “negative culture”:
Negative culture: a person goes to a diwaniya and hears that this medicine damages the liver or kidney, or that someone took it and got cancer, so culture plays a role. [Interviewee 21]
[they get their information] from the diwaniyas, friends’ gatherings. We have, as an Arab society, strong relations, so we listen to friends in gatherings, diwaniya, or café, or family evenings, when they talk they share experiences: so and so went to the doctor and the doctor told them to stop taking their medicine because of kidney failure. It is not the medicine that caused the kidney failure; however, they start thinking that the medicine must have caused the kidney failure and that’s why their doctor told them to stop taking it. So they miss that the cause was actually diabetes, and instead misinform others about an imaginary harm of this medicine. [Interviewee 16]
Social rumors and myths about claims of a cure using herbal treatment are also common in Arab society. Respondents attributed the use of alternative medicine or herbals to either a patient’s desire to find a cure or as a substitution to medications that are thought to cause long-term harm:
Along with their desire to take something to heal their diabetes, they feel the need to hear something that gives them hope, so someone comes along and tells them if they take this herbal/alternative medicine for a period of a month or so, their diabetes will disappear. Therefore, it is their desire to completely heal and not have to take drugs ever after. [Interviewee 10]
The patient is ignorant of the nature of the disease; some patients believe that this disease has a cure! [Interviewee 18]
Once in a while, a patient brings up a new herb/plant and tells you this will cure diabetes; not control, but cure it completely. Therefore, they believe they don’t need to take their medicine; but after a while, they come back with high blood glucose levels after stopping their medication. [Interviewee 9]
Theme 4: “Patients are in denial (or difficult)”
The study participants often regarded patients as difficult or in denial of their disease, which included a fatalistic outlook on their future:
Here [in this area] they are all Kuwaitis and are highly educated … but Kuwaitis have a hard time changing their behavior; it is very difficult to teach them to take their medicine every day. The Kuwaiti patient is challenging. [Interviewee 9]
… they resist. In this case they don’t want needles: “It’s enough, let me die. If I have to die, it is my fate,” they say. [Interviewee 10]
Some would say that death only comes once, so they don’t care. [Interviewee 9]
Some deny that they have diabetes and that diabetes is no more and has disappeared, and they think that they are not diabetic anymore. [Interviewee 10]
Theme 5: “I need to educate more”
All the participants (n=21) recommended more patient education to improve medication adherence. The main source of such education was first the PCP; however, the need for more education from other health-care personnel was also repeatedly mentioned, especially the need for hiring of specialized diabetes educators, along with more education from nurses and pharmacists:
I am insisting on education; it will solve the whole problem. [Interviewee 3]
Diabetes is an illness that needs more education … so that the patient understands very well the complications of [uncontrolled] diabetes from the first diagnostic encounter: what does diabetes mean, that diabetes can cause problems that the patient would suffer from all their life, for example, eyesight problems, kidney problems, might lead to kidney dialysis, or they could lose a foot or a limb. Of course, this is if they don’t adhere to treatment. This is not to scare them, but to allow them to comprehend that it is a must that they adhere to their treatment to avoid these consequences. [Interviewee 3]
It requires time to sit with a patient and explain to them in detail, and make sure they understand. We must educate the patient about the importance of the medication, and explain the complications of untreated diabetes. [Interviewee 2]
We have too many patients; we can’t cover all aspects. Therefore, there should be a separate educator … all over the world, there are special diabetes educators available, trained as educators. [Interviewee 5]
[the pharmacist] should explain to the patient how to take the medicine, and reduce my burden to provide details, and save me some time with the patient to do other things. [Interviewee 21]
The need for better communication skills was proposed by most (n=13) of the respondents. To achieve their goal to educate patients effectively, they emphasized the importance of having appropriate communication skills:
The diabetic patient needs time, and with all the crowdedness sometimes the patient does not get their fair share of education, and this needs communication skills … the ability to sit with a patient and listen to them so the patient trusts you and so will listen to what you say and take their medicine. [Interviewee 2]
Compliance is closely related to communication skills. If a doctor provides information with anger, the patient will leave with no recall of the information given; this is because they were not treated well. Some doctors do that. [Interviewee 17]
Theme 6: “Patients must hear it from other sources”
Respondents also suggested the need for education and awareness raising support from society as a counterforce against misconceptions within lay society:
[the patient] must hear it from all sides: they must hear from the radio, from television, from their neighbors and from their friends, at school and at work, they must hear from someone outside the medical establishment. They know that this is what the doctor says, but when they hear it from another source it becomes convincing. [Interviewee 10]
For example, educational workshops for patients … useful educational programs that the patients view as pleasant and attractive, and therefore useful … using all media, including TV. [Interviewee 21]
Educational interviews, communication between us and the community through one of these mediums; TV or the Internet or magazines or newspapers or even inside health centers; small clips about diabetes, a video instead of talking; patients sit and watch it on their screens. [Interviewee 15]
Discussion
The PCPs in this study perceived medication nonadherence as a result of lack of patient understanding: insufficient patient knowledge about diabetes, misunderstanding and misconceptions about the disease and medications, including fear of side effects, and the dissemination of misinformation by family members and friends. The solutions suggested by respondents included the provision of education at the clinic by health-care providers and professional diabetes educators, and at a societal level throughout formal and informal societal institutions to counteract the “negative culture”. This study highlights aspects of knowledge and understanding that have received little attention in the adherence literature.
Patients’ lack of knowledge and misconceptions
Although reviews of the literature on the topic concluded that there was contradictory evidence about the relationship between patient knowledge and adherence,6,8 the providers still perceive that knowledge is an important determinant of adherence, as previous research has shown repeatedly.18–20 Similarly, the PCPs in our study saw insufficient patient knowledge and misconceptions as core factors affecting medication adherence. They saw patients’ basic knowledge about diabetes as a chronic disease and debilitating consequences as poor. Examples of patient misconceptions included the perception of diabetes as an acute illness and the belief and hope that there is a cure to diabetes, which are also common findings in previous studies on non-Westernized populations.21–24 Such beliefs contribute to inaccurate understanding, make patients continuously seek unobtainable cures, and add to complexity in terms of physicians’ ability to educate diabetes patients. Diabetes as a chronic disease is unlike what patients have experienced in acute illnesses, where the effect of taking a medicine is evident to the patient by the relief they get or cure they will have within a short period of time. In diabetes, the consequences for not taking the medications are distant and unobservable to the patient.
In the 1980s, Conrad reported on the general dislike of medicines and that taking medications continuously reminds the patient about the illness, despite feeling well after stopping the medication.25 As physicians in our study view it, many patients with diabetes still operate according to the acute model of illness, as illustrated in the quotes herein.
Contributing to the generally negative attitudes toward medications, fear of side effects is a concern for most patients, as reported by our participants and other previous studies.6,15,26 An actual episode of side effects, such as hypoglycemia accompanying skipping meals without adjustment of doses of sulfonylurea or insulin, can exaggerate feelings of aversion and avoidance behavior. Other notable side effects related to diabetes medication reported were weight gain and gastrointestinal disturbances, leading to negative attitudes toward medications. These are rather well known and recognized side effects from clinical trials and everyday practice.
A profound finding in the views of our participants was the power of the misinformation that comes from the social surrounding of the patients, which was a repeatedly recurring topic during the interviews. Although unfounded fears of harm from medication, such as fear of dependence on diabetes medication, has been reported in the Western literature,26 the “negative culture” described here is unique to the Arab context, and is thought of as interfering with accurate knowledge about the illness and its treatment provided by health-care personnel. Family and friend gatherings and their negative effect appeared in such examples as when a patient might experience a problem with a medication, which might not be applicable to other patients, and generalized it to other contexts, as illustrated in our results. A study in Saudi Arabia supports these findings related to the widespread misconceptions related to diabetes and its treatment.21
In addition to what the patients hear about the inaccurate harms of medication, they also hear about the claimed healing ability of certain herbal medicines. Now and then, a new “magic herb” with curing ability shows up in the conversation with the patient, according to one PCP. Disputing these misconceptions and convincing patients becomes a continuous struggle for providers. The PCPs expressed a sense of frustration when they had exhausted all arguments in support of the importance of taking medication to the patient to no avail. As also shown by others,15 the patients may resort to expressions of denial or fatalism: “I feel just fine”, or “If Allah will take me, so be it”. The physician has no more to say here.
Educating and raising awareness in society
The counterforces to lack of understanding were summarized by two means: to give more education from the providers of care in the clinic and PCPs perceiving that society is also responsible for supporting their efforts in raising awareness. Giving more education in the clinic was the most frequent intervention suggested by our participants in order to provide a solution for the lack of understanding and low awareness among patients. Diabetes educators, who are still rare in PC practice in Kuwait, were seen as a solution and an efficient way for educating patients. In addition, the PCPs wanted more information provision from pharmacists about medication and more from nurses in their current role in teaching patients how to inject insulin.
Due to the significant role of information coming from the social environment and how it shapes diabetes patients’ conception of the disease and its treatment, and cognizant of limitations in their ability to influence patients’ knowledge and beliefs, the physicians hoped for educational interventions from society at large. In that context, they included national campaigns, an introduction of diabetes concepts in school curricula, work-based education, and the like. These educational methods parallel the traditional population approaches to health education that focus mainly on information provision, and ignore the more patient-centered approaches of empowerment and shared decision making within the broader determinants of health, such as cultural, economic, and environmental factors.27
Issues arising from the PCP perspective
The paradigm of the PCPs in dealing with nonadherence is a traditional biomedical one, where the solution is seen in educating and providing information.28 It assumes that knowledge will lead to behavioral change, such as taking the medication. This paradigm relies on sending messages to patients without enough attention to the patients’ needs to share their stores and struggles. An understanding of the wider implications of adherence in patients’ lives is necessary for the PCP’s ability to be of help.
Evidence has shown the effectiveness of more patient-centered interactions in chronic care. Accumulated evidence over two decades in adopting the chronic care model suggests that redesigning care according to the model improves patient care and produces better health outcomes.29 Newer strategies of communication that are more patient-centered, such as motivational interviewing, have been shown to outperform traditional advice giving in the treatment of a broad range of behavioral problems and diseases.30
The most recent standards of medical care in diabetes call on PCPs specifically to target two strategies to improve care:31 patient-centered communication incorporating patient preferences, assessing levels of literacy and numeracy, and addressing cultural barriers; and the model of care should be aligned with the components of the chronic care model to ensure successful interactions between the health-care team and an informed, motivated patient.
Such standards currently represent the “state of the art” in relation to diabetes care; however, they came through decades of evolutionary process.28 Previously, patients were most often considered to be passive receivers of information and care, incapable of making decisions on their own behalf. Today, however, there is a new growing alliance between the doctor and patient, based on cooperation and shared decision making, which determines the most appropriate course of action for an individual patient. The role of the care provider in this patient-centered model is to provide a link between evidence-based medicine and the personal experiences and needs of the patient.
In the context of Arab culture, doctors may still be separated from their patients in terms of scientific outlook and educational background. The doctor–patient relationship here is more impersonal and remote;32 therefore, patient empowerment and shared decision making might still need time to become common practice. As societal values evolve, these aspects of care will evolve alongside.
Strengths and limitations
This study was conducted in a PC setting with ample coverage of diverse geographical areas in the country, with PCPs of diverse backgrounds in terms of education and practice experience. Therefore, the results should be representative of PCPs in Kuwait. However, to what extent the result can be generalized to other countries in the region is unknown. For example, the diwaniya social system could be unique to Kuwait. Although other Arab countries have similar venues for social interactions, such as the café in Egyptian culture, the social interactions might be different in the diwaniya, due to the closer social relationships of its dwellers. To some extent, the socioeconomic context in Kuwait might be different from neighboring countries. Kuwaitis, as well as residents of Kuwait, have access to almost free medical care and prescription medicines.
Another strength relates to the qualitative methodology used and its rigor. This was evident by achieving data saturation before exhausting the number of targeted participants. For the analysis, several checks on validity and reliability were used, as described. Interviews were conducted by an experienced interviewer, who was also the main analyzer of data, which supports the validity of the results.
Impact on practice
In the opinions of PCPs, there is a clear need for educational support. First, they need support at two levels: at the clinic and in society at large. At the clinical level, there is considerable need for professional diabetes educators to take some of the burden off PCPs. At the societal level, concerted effort is needed to disseminate evidence-based knowledge about diabetes and its prevention, management, and consequences throughout formal and informal societal institutions. This is what was felt by the PCPs as appropriate to counteract the “negative culture”.
Still, the centrality of patient-related factors in PCPs’ views in this study, as well as their overlooking of providers and system-related factors, should be of concern. The providers’ attitude to medication adherence is part of the health-care environment in which patients receive care and could influence adherence. The providers in this study did not seem to see that many of the barriers to medication adherence reside in the structures and policies of the health-care system (eg, availability of clinical coaching and self-management support), as well as within a specific PCP’s abilities (eg, goal setting and motivational interviewing). Health-care policy makers and medical school educators should consider where future interventions are best placed: within medical school education and/or continuing professional development. The content of intervention would provide opportunities to broaden PCPs’ knowledge and skills to include providers and system-related factors that were found to be useful in facilitating medication adherence.
In order to tackle the burden of improving treatment adherence in diabetes more effectively, the health-care system needs a comprehensive approach that includes not only education but also strategies for behavioral change and emotional support. It has been shown that the combination of the three interventions – education, behavioral strategies, and emotional support – were twice as effective as education standing alone.33 To deliver such intervention in a health-care system similar to Kuwait, where most diabetes patients are served by public PC, a program can be established of interdisciplinary health teams in each PC clinic. The team would comprise both a PCP and a nonphysician practitioner, which could include a nurse, a pharmacist, a behavioral health consultant, or a community health advisor. The nonphysician team member will be trained and certified to play the role of clinical health coach and work closely with a physician to engage the patient in his/her own care. The clinical health coach addresses knowledge barriers to medication, targets motivational and mental health factors related to nonadherence, and identifies and helps remove barriers to adherence that may be due to lack of resources. The effectiveness of such a program could be assessed by threefold measures: improvements in adherence (eg, gaps in medication refills, patient self-report instruments), reaching treatment targets (eg, glycosylated hemoglobin, blood-pressure values, lipid level), and ultimately by improvements in patient-reported outcomes (eg, quality of life, satisfaction) and the program’s impact on short- and long-term health-care cost.
Conclusion
Patient lack of understanding as the driver of medication nonadherence is the dominant view of PCPs. This is significant in relation to elucidating PCPs’ struggle in their daily work and in relation to evolution of the diabetes-care model within the cultural context.
Acknowledgments
The authors thank the physicians who shared their experiences and perceptions. Special thanks to Dr Rihab Al-Watayn, head of the Primary Care Department at the Ministry of Health, for her help in getting the study approved by the ethics committee and providing access and support while collecting data. Also, thanks to Ms Shaimaa Abdulmagid from the Faculty of Pharmacy at Kuwait University for her transcription of audio recordings and her help in the literature search and retrieval. The authors also want to thank Mr Chris Williams, Ms Fatima Waheedi, and Mr Hasan Waheedi for their English language review and editing at different stages of writing this article.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
International Diabetes Federation. IDF Diabetes Atlas. 6th ed. Brussels: IDF; 2013. | ||
International Diabetes Federation. IDF Diabetes Atlas. 7th ed. Brussels: IDF; 2015. | ||
Shah NM, Behbehani J, Shah MA. Prevalence and correlates of major chronic illnesses among older Kuwaiti nationals in two governorates. Med Princ Pract. 2010;19:105–112. | ||
Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27:1218–1224. | ||
Waheedi M, Awad A, Hatoum HT, Enlund H. The relationship between patients’ knowledge of diabetes therapeutic goals and self-management behaviour, including adherence. Int J Clin Pharm. 2017;39:45–51. | ||
Alsairafi ZK, Taylor KM, Smith FJ, Alattar AT. Patients’ management of type 2 diabetes in Middle Eastern countries: review of studies. Patient Prefer Adherence. 2016;10:1051–1062. | ||
Horne R, Graupner L, Frost S, Weinman J, Wright SM, Hankins M. Medicine in a multi-cultural society: the effect of cultural background on beliefs about medications. Soc Sci Med. 2004;59:1307–1313. | ||
Brundisini F, Vanstone M, Hulan D, DeJean D, Giacomini M. Type 2 diabetes patients’ and providers’ differing perspectives on medication nonadherence: a qualitative meta-synthesis. BMC Health Serv Res. 2015;15:516. | ||
Alhyas L, Nielsen JD, Dawoud D, Majeed A. Factors affecting the motivation of healthcare professionals providing care to Emiratis with type 2 diabetes. JRSM Short Rep. 2013;4:14. | ||
Abdulhadi N, Al-Shafaee MA, Ostenson CG, Vernby A, Wahlström R. Quality of interaction between primary health-care providers and patients with type 2 diabetes in Muscat, Oman: an observational study. BMC Fam Pract. 2006;7:72. | ||
Luborsky MR, Rubinstein RL. Sampling in qualitative research: rationale, issues, and methods. Res Aging. 1995;17:89–113. | ||
Strauss A, Corbin J. Basics of Qualitative Research. Newbury Park (CA): Sage; 1990. | ||
Wens J, Vermeire E, Van Royen P, Sabbe B, Denekens J. GPs’ perspectives of type 2 diabetes patients’ adherence to treatment: a qualitative analysis of barriers and solutions. BMC Fam Pract. 2005;6:20. | ||
Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research – a comprehensive review. J Clin Pharm Ther. 200;26:331–342. | ||
Jeragh-Alhaddad FB, Waheedi M, Barber ND, Brock TP. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2015;9:1491–1503. | ||
Ritchie J, Spencer L. Analyzing Qualitative Data. London: Routledge; 1994. | ||
Hallberg LR. The “core category” of grounded theory: making constant comparisons. Int J Qual Stud Health Well-being. 2006;1:141–148. | ||
Nam S, Chesla C, Stotts NA, Kroon L, Janson SL. Barriers to diabetes management: patient and provider factors. Diabetes Res Clin Pract. 2011;93:1–9. | ||
Jeavons D, Hungin AP, Cornford CS. Patients with poorly controlled diabetes in primary care: healthcare clinicians’ beliefs and attitudes. Postgrad Med J. 2006;82:347–350. | ||
Patel N, Stone MA, Chauhan A, Davies MJ, Khunti K. Insulin initiation and management in people with type 2 diabetes in an ethnically diverse population: the healthcare provider perspective. Diabet Med. 2012;29:1311–1316. | ||
Al-Saeedi M, Elzubier AG, Bahnassy AA, Al-Dawood KM. Treatment-related misconceptions among diabetic patients in western Saudi Arabia. Saudi Med J. 2002;23:1243–1246. | ||
Barnes L, Moss-Morris R, Kaufusi M. Illness beliefs and adherence in diabetes mellitus: a comparison between Tongan and European patients. NZ Med J. 2004;117:U743. | ||
Bean D, Cundy T, Petrie KJ. Ethnic differences in illness perceptions, self-efficacy and diabetes self-care. Psychol Health. 2007;22:787–811. | ||
Abubakari AR, Jones MC, Lauder W, et al. Ethnic differences and socio-demographic predictors of illness perceptions, self-management, and metabolic control of type 2 diabetes. Int J Gen Med. 2013;6:617–628. | ||
Conrad P. The meaning of medications: another look at compliance. Soc Sci Med. 1985;20:29–37. | ||
Mishra SI, Gioia D, Childress S, Barnet B, Webster RL. Adherence to medication regimens among low-income patients with multiple comorbid chronic conditions. Health Soc Work. 2011;36:249–258. | ||
Whitehead D. Health promotion and health education: advancing the concepts. J Adv Nurs. 2004;47:311–320. | ||
Kaba R, Sooriakumaran P. The evolution of the doctor-patient relationship. Int J Surg. 2007;5:57–65. | ||
Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009;28:75–85. | ||
Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract. 2005;55:305–312. | ||
American Diabetes Association. Standards of medical care in diabetes – 2015 abridged for primary care providers. Clin Diabetes. 2015;33:97–111. | ||
Abdulhadi N, Al Shafaee M, Freudenthal S, Ostenson CG, Wahlström R. Patient-provider interaction from the perspectives of type 2 diabetes patients in Muscat, Oman: a qualitative study. BMC Health Serv Res. 2007;7:162. | ||
Roter DL, Hall JA, Merisca R, Nordstrom B, Cretin D, Svarstad B. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138–1161. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.