Back to Journals » Patient Preference and Adherence » Volume 13
Patient interpretation of the Patient-Generated Subjective Global Assessment (PG-SGA) Short Form
Authors Balstad TR ![]() , Bye A, Jenssen CRS
, Bye A, Jenssen CRS ![]() , Solheim TS, Thoresen L
, Solheim TS, Thoresen L ![]() , Sand K
, Sand K ![]()
Received 11 February 2019
Accepted for publication 2 May 2019
Published 16 August 2019 Volume 2019:13 Pages 1391—1400
DOI https://doi.org/10.2147/PPA.S204188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Trude R Balstad,1,2 Asta Bye,3,4 Cathrine RS Jenssen,1 Tora S Solheim,1,2 Lene Thoresen,2,5 Kari Sand1,2,6
1Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, NTNU, Norwegian University of Science and Technology, Trondheim, Norway; 2Cancer Clinic, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; 3Department of Nursing and Health Promotion, Faculty of Health Sciences, OsloMet – Oslo Metropolitan University, Oslo, Norway; 4European Palliative Care Research Centre (PRC), Department of Oncology, Oslo University Hospital and Institute of Clinical Medicine, University of Oslo, Oslo, Norway; 5National Advisory Unit on Disease-related Malnutrition, Oslo University Hospital, Oslo, Norway; 6SINTEF Digital, Department of Health Research, Trondheim, Norway
Correspondence: Trude R Balstad
Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, NTNU – Norwegian University of Science and Technology, Postbox 8905, Trondheim 7491, Norway
Tel +47 7 282 6060
Email [email protected]
Background: The Patient-Generated Subjective Global Assessment (PG-SGA) is a patient-reported instrument for assessment of nutrition status in patients with cancer. Despite thorough validation of PG-SGA, little has been reported about the way patients perceive, interpret, and respond to PG-SGA. The aim of this study was to investigate how patients interpret the patient-generated part of the PG-SGA, called PG-SGA Short Form.
Methods: Purposive sampling was used to identify participants that had experienced weight loss and/or reduced dietary intake and/or had a low body mass index. Data were collected from 23 patients by combining observations of patients filling in the PG-SGA Short Form, think-aloud technique and structured interviews, and analyzed qualitatively using systematic text condensation.
Results: Most of the participants managed to complete the PG-SGA Short Form without problems. However, participant-related and questionnaire-related sources of misinterpretation were identified, possibly causing misinterpretations or wrong/missing answers. Participants either read too fast and skipped words, or they struggled to find response options that were suitable for covering their entire situation perfectly. The word “normal” was perceived ambiguous, and the word “only” limited the participants’ possibility to accurately describe their food intake. Long recall periods in the questions and two-pieced response options made it difficult for patients to select only one option.
Conclusion: The results of this study provide a unique patient perspective of using the PG-SGA Short Form and valuable input for future use and revisions of the form. The identified sources of misunderstanding could be used to develop a standardized instruction manual for patients and health care personnel using the PG-SGA Short Form.
Keywords: validation studies, PG-SGA, qualitative research, patient involvement, patient-reported outcome measures
Introduction
Patients living with cancer may have different nutritional challenges; early identification and treatment of malnutrition and disturbed metabolism are of critical importance. European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines strongly recommend to screen for risk of malnutrition in all cancer patients and further perform a nutritional assessment in patients at risk to identify those who are malnourished.1
The Patient-Generated Subjective Global Assessment (PG-SGA) is well recognized in clinical research as the reference method for assessing nutrition status in patients with cancer,2–10 and is a modified version of the nutritional assessment instrument Subjective Global Assessment.11,12 The first part of PG-SGA is completed by the patients, and have been used as a screening instrument for nutritional risk/deficit and is referred to as PG-SGA Short Form.8,13,14
The PG-SGA (full and Short Form) has been validated on various levels. A high construct validity, ie, sensitivity and specificity to predict nutritional status compared to a reference method, has been reported.4,13 Numerous studies have shown PG-SGA’s ability to predict clinical outcomes (predictive validity), such as survival,6,13,15 postoperative complications16 and reduced tolerance to chemotherapy.17 A recent systematic review reported that PG-SGA (including Short Form) was among very few (four out of 37) instruments covering all the domains in the ESPEN and American Society for Parenteral and Enteral Nutrition definition of malnutrition (content validity).18
Despite the extensive use and validation of PG-SGA, very little has been reported about the patients’ perspective, ie, about the way patients perceive, interpret, and respond to the items in the patient-generated part constituting PG-SGA Short Form.19 Validity of an instrument relies also on a common understanding of the meaning of the questions and the response options. Patients might interpret questions in different and unexpected ways, compared to what was intended.20 Data gathered from self-report instruments are only useful to the extent that people make sense of the questions in an intended manner.21 If a questionnaire fails to represent the patients’ perspective, it may result in patients failing to complete the questionnaire properly and consequently a possible negative impact on the validity.22
Experiences from the use of PG-SGA Short Form in clinical trials have questioned how well it works with regard to patient use and understanding. Challenges regarding patients’ understanding of the form were observed in a feasibility study of a multimodal intervention for cachexia23 and in a cross-sectional study examining the prevalence of cachexia and areas of unmet need in patients with cancer.24 Therefore, the aim of this study was to investigate how patients interpret the patient-generated part of PG-SGA.
Methods
Ethics approval and participants
The Regional Committee for Medical and Health Research Ethics evaluated the protocol and concluded that no formal ethical approval was required for this study (Reference 2017/979 REK) since the study was not within the scope of the Norwegian Health Research Act. The study was therefore ethically approved by the Norwegian Centre for Research Data (Reference 54934/3/STM) and the internal review board of the Cancer Clinic, St. Olavs hospital, Trondheim University hospital. Participants were recruited from the inpatient clinics at the Cancer Clinic, St. Olavs hospital, Trondheim University hospital between August and December 2017. All participants provided written informed consent. Purposive sampling was used to identify participants that during the last week had experienced weight loss and/or reduced dietary intake and/or had a BMI<20.5 as identified by Nutrition Risk Screening 2002.25 Inclusion criteria included a verified cancer diagnosis, 18 years or older, ability to understand Norwegian language and to provide written informed consent.
PG-SGA Short Form
In the PG-SGA Short form (consisting of four text boxes), patients report on current and former body weight (Box 1); changes in food intake and current type of food/nutritional intake (Box 2); nutritional impact symptoms and other factors that negatively influence food intake/absorption/utilization of nutrients (Box 3); and activities and function based on Eastern Cooperative Oncology Group performance status,26 converted to layman’s language (Box 4)14 (Figure 1). The PG-SGA Short Form numerical scoring range from 0 (no problems) to 36 (worst problem), whereof Box 1 has a maximum score of 5, Box 2 has a maximum score of 4, Box 3 has a maximum score of 24, and Box 4 has a maximum score of 3. Multiple answers where only one answer is intended (applies to all boxes) by eg, ticking “no problems eating” in Box 3 in combination with other symptoms, the sum of problems scores are reported. The Norwegian version of PG-SGA Short form 155–004 v01.18.17 was used in this study.
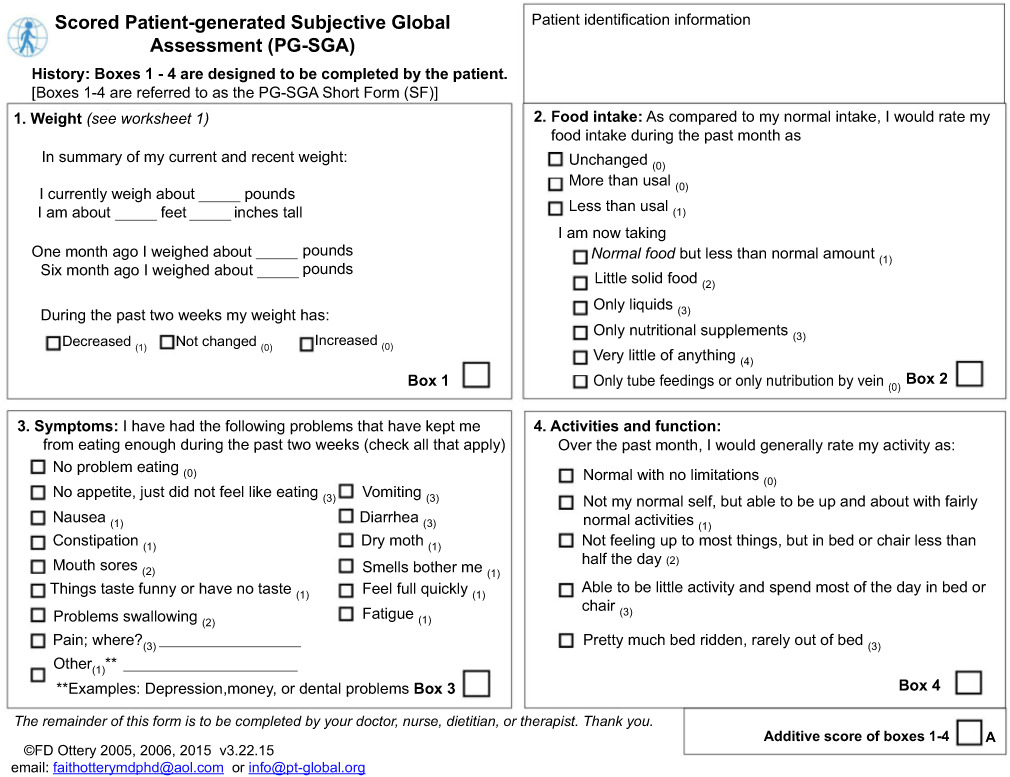 |
Figure 1 English language version of the Scored Patient-Generated Subjective Global Assessment (PG-SGA©), also known as PG-SGA Short Form©.Notes: Reproduced with permission from Ottery FD. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition. 1996;12(1 Suppl):S15–19. Copyright © 1996 FD Ottery. |
Data collection
A combination of observation, think-aloud technique, and structured debriefing interviews was selected to identify how the patients interpreted the items in and layout of PG-SGA Short Form, and whether problems occurred during the completion.27 Patients were asked to complete the PG-SGA Short Form and verbalize what they think while completing the form. Observation notes were taken based on a template with broad categories addressing how the participants navigate in the form; whether they read fast or slowly; misreadings; whether and where they hesitated before answering; and words that seemed of particular interest in the participant, or to cause problems or frustration. The categories were partly predefined based on previous research on participants’ interpretation of self-reported questionnaires28,29 and on empirical experience of patients’ use of PG-SGA in clinical trials.23,24 Also, any other behavior of relevance was registered, which were the basis for also generating new categories of behavior during data collection. Whether patients read slowly or fast were based on the two researchers’ subjective interpretations. After completing the form, the patients were interviewed based on a structured interview guide containing questions about the participants’ subjective evaluation of the questions and response options, their choice of reading strategies, whether questions were found to be easy or difficult, and how they selected response options. The questions were repeated for each of the four sections of the form (Boxes 1–4; Figure 1). Additionally, observed patient behavior and/or patients’ comments during the completion of the form were addressed in the interviews when relevant. The interviews were conducted by a nurse (CRSJ). Two researchers (one nurse (CRSJ) and one communication researcher (KS)) were present during each data collection session. Observations and interviews were audio recorded. Demographic and medical background data were collected from medical journals. Performance status was assessed using the Karnofsky Performance Score (KPS).30
Data analysis
The audiotaped material was transcribed verbatim and combined with the observation notes before analysis. The analysis followed the principles of systematic text condensation,31 which is a four-step procedure for analysis of qualitative data. A condensation approach implies to identify patterns and diversity within the participants’ accounts, and not quantifications. The unit of analysis is experiences, not individuals.32 First, two researchers (CRSJ and KS) read and reread transcriptions to obtain an overall impression of the material, and preliminary themes were identified inductively (eg, “did not notice all the words”, “selecting more than one response option”, “assistance from family member”, “negative thoughts”, “changing their mind”). In the second step, units of meaning – ie, all pieces of the transcripts of relevance for the research aim, in this case, aspects of how patients filled in PG-SGA Short Form – were identified. A detailed coding scheme was developed based on the preliminary themes, and all meaning units were coded by use of this. In the third step, the coded material was condensed into code groups (eg, the codes “asked for help from family”, “asked what a word mean” and “asked for confirmation from researcher” were combined into the code group “did not want to do anything wrong”). The code groups were classified into two overall categories: participant-related and questionnaire-related sources of misinterpretation and associated sub-themes (eg. “reading fast and skipping words”, “the need to tell the whole story” as participant-related sub-categories and “imprecise words” and “two-pieced response options” as questionnaire-related sub-categories”). In the last step, the condensates were summarized and illustrative quotes were selected for all themes. The phases of developing preliminary themes, codes, sub-categories, and categories were continuously reflected on and discussed between two researchers (CRSJ and KS). The researchers continuously returned to the original text to ensure that the core meaning was preserved.
Results
A total of 46 patients were approached, and of these 23 wanted to participate in the study. Twenty-two participants were in-patients and one was an outpatient. Eleven patients were included from the palliative care unit at the Cancer Clinic, 11 participants were included at the general oncology unit at the Cancer Clinic, and one was included from the Gastro surgery unit. All interviews took place at the hospital, either in patients’ rooms or in a conference room. None of the participants had filled in PG-SGA Short Form before their participation in this study. Patient characteristics and results from PG-SGA Short Form are presented in Table 1. Almost half of the patients (n=11, 48%) had gastric cancer and according to tumor staging, eight had a local disease (35%), nine had locally advanced disease (39%), and six had metastatic disease (26%). All patients except one received anti-cancer treatment, most commonly chemotherapy. Patients’ performance status ranged from KPS 30–90 whereof half of the group had KPS ≥70. Weight loss last six months reported in PG-SGA showed a mean (SD) % weight loss (kg) of 10.6 (10.4) %, ranging from −13.0% (increase in weight) to 29.2%. When calculating the score of PG-SGA Short Form, the median (IQR) total score was 13 (8), ranging from 3 to 28 (Table 1). One patient had a score of 3, three patients a score from 4 to 8, and the remaining 19 patients had a score ≥9. Six patients chose more than one response in single response questions and/or no response at all in two or more of the boxes, 11 chose more than one response in single response questions and/or no response at all in one of the boxes, and the remaining five patients completed the form as intended. More specifically, in Box 1 data regarded previous weight were missing, or multiple responses on weight loss last two weeks were given; in Box 2 patients selected several options when they were supposed to select only one item in their answer to “I am currently taking”; in Box 3 patients selected the option “no problems eating” in combination with several symptoms that had kept them from eating; and in Box 4 patients selected several options about their level of activity and function when they were supposed to select only one. One patient did not report body weight last month, and one did not report weight six months ago, and therefore weight loss could not be calculated from those time points.
 |
Table 1 Patient characteristics |
Most of them had no problem filling in the form or understanding the words used in it. The mean (SD) time spent on the entire session (ie, filling in PG-SGA Short Form while verbalizing their thoughts and participating in the interview) were 25 (10) minutes, ranging from 9.5 to 49.5 mins. Thirteen of the participants read and fill in the form in the intended order, ie, starting with Box 1, going on to number 2, 3, and finally number 4, while 10 filled in Box 3 before number 2, ie, in a vertical direction.
Even if the form were perceived and evaluated by the patients as relatively easy and straightforward to complete, some sources of misinterpretation were identified causing participants to answer the questionnaire in an unintended manner, or for them to struggle finding sufficient response options. These sources of misinterpretation were categorized into two main categories: participant-related or as questionnaire-related.
Participant-related sources of misinterpretation
One reason for misreading or giving wrong answers, was that the patients read the questions and answered quickly. Box 1 asks about current weight and weight history, but most participants read neither headlines nor the question. They started right on the answer in the third line and wrote only their current weight. In Boxes 2–4, most participants seemed to read the questions before they answered. However, during the subsequent interviews, it became apparent that several of them had not read the question or response options well enough. When they were asked specific questions about the content of the form, or how they selected their responses, they realized that they had neither noticed all the words in the questions nor in the response options, as the following quotes illustrate:
When I read it now, I find the question a little bit long. But I didn’t think about it when I read it the first time. I didn’t notice it, because you only read every third word. But now that I had to go over each word, it turned out to be a long sentence. (Participant 22, man)
I had to go back, because I didn’t give a precise answer. I need to write “Pain in left shoulder” here. (Participant 8, man)
Now I have to see if I have responded correctly, I started to think a little more. (Participant 9, woman)
Some participants spend more time than others on completing PG-SGA Short Form because they strived to give precise answers covering their unique situation. They reported that they had to think thoroughly to understand the question and to find one correct answer. Often, they felt that more than one response option was needed to allow for a better description of their situation, such as one participant explained regarding the question about food intake in Box 2:
My food intake has changed because now I eat several and smaller meals. What do I do? “More than usual”? “Less than usual”? Perhaps I eat what I normally eat, but in smaller portions. In total, perhaps half the amount of food compared to what I usually would have eaten. What do I choose in order to get it correct? “Less than usual”? “More than usual”? You can’t throw a dice, you know. (Participant 18, man)
Thirteen of the patients selected more than one response option on questions in Box 1 (body weight and weight history), 2 (food intake), and 4 (activities and function). For instance, in Box 1, one participant checked off that his weight had both “decreased” and “increased” during the past two weeks.
I kind of had to read the question twice in order to figure out what suited best for me. And it was easier when I realized that I could select more than one option. But still, I was not able to illustrate my special situation. I think it is very special. (Participant 12, man)
When participants had trouble selecting a response option, they often sought a confirmation of their choice from the researchers or from present family members:
I don’t know if this is how you wanted me to answer this question? (Participant 7, man)
The content of the PG-SGA Short Form made some of the patients more aware of their body weight, reduced food intake and/or reduced level of activities, and this was observed to be distressing for them. Some of them became sad when they had to talk about their weight loss or reduced level of activity due to their disease.
Oh my God, I want to avoid this! [refers to question about weight loss]. The hardest thing is when you lose weight when you actually don’t want to. (Participant 13, woman)
When the form asked about aspects of the participant’s situation, such as functional decline and weight loss, it was difficult for some patients to answer honestly. One participant, who had always been active, also as part of his work, found it very hard to admit that he had to select the last response option in Box 4: “Pretty much bed ridden, rarely out of bed”. In the interview, he hesitated before he commented:
I wish I could have selected “able to do little activity and spend most of the day in bed or chair”. But to be honest, I have been lying in bed. (Participant 16, man)
Questionnaire-related sources of misinterpretation
In general, the words used in PG-SGA Short Form were easy to understand for most participants. Still, it was difficult to interpret the meaning of some of the words as they were used in the form. The most frequent word causing misunderstandings was “normal”, used in phrases such as “normal food” (Box 2 (food intake)) and “not my normal self” (Box 4) (activities and function). The phrase “normal food” was found to be ambiguous, since it could refer to “the type food I normally eat”, “the amount of food I normally eat”, or “normal food in general/in my culture”.
“Normal food”, is it hotdog, pizza, what is it? (Participant 24, man)
I wonder if enteral nutrition is normal food, but I concluded that it isn’t. (Participant 5, woman)
In Box 2 (Food Intake), the second item consists of the heading “I am now taking” followed by a list of six response options regarding nutritional intake (“normal food but less than normal amount”; “little solid food”; “only liquids”; “only nutritional supplements”; “very little of anything”; “only tube feedings or only nutrition by vein”). The word “only”, used in four of the options, limited the participants’ possibility to convey what they wanted, since it prevented them from telling that they ingested both solid food and oral nutritional supplements. It was commented by some that they chose to ignore the word “only” when they answered. One of the participants even drew a line through the word to delete it.
If it hadn’t said “only tube feedings”, if it had said “tube feeding or nutrition by vein” as a response options for “I am now taking”, then it would be suitable for me. But when it says “only”, it doesn’t fit, because it is in combination with something else. (Participant 23, man)
In three of the four text boxes of PG-SGA, no instructions are given regarding how many options one is supposed to select, while in Box 3 (nutrition impact symptoms) it is stated that one is to “check all that apply”. When filling in the form, some participants asked the researcher to clarify how many options they were supposed to select. For some, it seemed to be regarded mandatory to select only one, indicating that this is how it is usually done, or this is what they were mostly used to do filling in questionnaires in general, even if they felt that one option was not sufficient, as the following quote illustrates:
Although I do not see that it’s written, you do not allow yourself to fill in more [than one option], it’s not common. (Participant 3, woman)
The relatively long recall periods caused challenges for the participants. During the past month (the recall period used in Box 2 (food intake) and Box 4 (activities and function)), several of the participants had experienced variations that made it impossible for them to select only one response option. Consequently, some participants checked off for more than one option. The variations over a month could be so extensive that most of or all the response options were appropriate.
Yes, the last month, it feels like cycles. First, I don’t eat much and then I eat a lot when I’m feeling better. During one month, it’s really going through all phases from usable to good intake to minimal like intravenous. (Participant 17, man)
It changes daily, I choose two options, “little solid food” and “only liquids” because I eat bread in the morning and receive parenteral nutrition as well. (Participant 1, man)
Four of the five response options in Box 4 (activities and function) are two-pieced, for instance: “not my normal self, but able to be up and about with fairly normal activities” or “not feeling up to most things, but in bed or chair less than half of the day”. Consequently, half of one option and half of the other could be suitable, and consequently, it was difficult to select only one.
But when it says that I “spend less than half the day in bed or chair” that’s correct [option 3], but I also feel familiar with option number two “up and about with fairly normal activities”. (Participant 4, man)
Discussion
When participants in this study interpreted and used PG-SGA Short Form, most of them had no problem reading the questions and answering them. However, some sources of misinterpretation were identified. Many of the participants read and responded to the questions quickly. For some this resulted in failing to notice all the words, such as the recall period in the question or all the response options. Another source of misinterpretation was phrases participants found to be imprecise, such as “normal food” or “normal activity level”. More than half of the participants also selected more than one response option in questions where they were supposed to select only one. Reasons for this were that the recall periods were perceived as long that only one option did not capture the entire period, and that the options in Box 4 (activities and function) were too unspecific.
The challenges with long recall period in some of the questions in the PG-SGA Short Form raised the question of whether it would be easier for patients to relate for example “now” than “past month”. However, in a previous study of the patient-rated instrument Edmonton Symptom Assessment Scale, in which the assessed time frame was “now”, it was found that this was not an unambiguous term that patients easily related to. Patients answered either how they felt yesterday or how they thought they would feel in the future. They experienced that the intensity of symptoms varied and if they answered how they were at the moment, then the situation could be different in the next moment.28 The need to tell the whole story seems to be so important for patients that it is difficult to relate to predefined recall periods.
Many of the participants in our study read too fast and ignored words. A possible consequence of this is that the form is not filled in as intended, and the results/total score could thus be incorrect or misleading. There are different reasons for patients reading the questions inaccurately. Some of the participants were frail, malnourished, tired, sad, and/or had lack of concentration due to their disease and/or medication, which could make it difficult for them to read and answer all the questions properly. For others, however, answering questionnaires is familiar and an easy task, and they probably found it unnecessary to read thoroughly to be able to respond.
Patient responding to a questionnaire is not a neutral task where one just gives a mark and move on to the next question. When a patient answers a questionnaire, it involves a separate interaction between the patient and the questionnaire, which can start a thinking process, either for the better or for worse for the patient.33 Answering a questionnaire can make the patient more aware of his/her situation, either positively or negatively. We observed that some patients became more aware of the negative aspects of their situation, and such negative thoughts may have affected their motivation for our ability to answer questions on such topics.
That the content of PG-SGA Short Form seemed to provoke negative thoughts among some of the participants, was something we were not sufficiently prepared for before the study started. For some, for example, it was hard to be reminded of how much weight they had lost, while others were very tired of a constant focus on food. In future similar studies, consideration should be given to whether participants should be offered a consultation with, for example clinical dietitian, nurse or doctor after participation.
Patients in this study were very eager to tell their own unique story and many experienced that it was not possible to tell it completely by the use of PG-SGA Short Form in its current form. However, since questionnaires never could be individually customized for each patient, we suggest, based on the results of this study, that a standardized manual for instruction to patients is developed, addressing examples of what the health care provider and/or researchers could explain to patients who are asked to fill in PG-SGA Short Form. We have summarized some ideas for content in such an instruction manual based on our results (Box 1). Such a manual could be useful as beforehand instructions and/or as assistance if patients want help during the complementation.34
 |
Box 1 Ideas for content in a Patient-Generated Subjective Global Assessment (PG-SGA) instruction manual |
In able to give these instructions to patients, the health care professionals need to have sufficient knowledge of the form and to be familiar with the instrument’s use.
Due to advances in medical nutritional therapy, combination of treatments such parenteral nutrition support in addition to using oral nutritional supplements and eating some food, is more common. Such a treatment combination is difficult to express in when answering the current question about food intake in PG-SGA (Box 2, second half), since you cannot express a combination treatment by use of the current available response options. Therefore, PG-SGA should be amended and elaborated accordingly.
The present study is to our knowledge the first study to evaluate patients use and interpretation of PG-SGA Short Form, an under-researched field in the development of nutritional screening and assessment instruments. A high number of patients were included in this qualitative study, which strengthen our findings. Combining observation with the think-aloud technique and interviews made it possible to obtain more detailed and complete data from the participants, than by using only retrospective debriefing interview. Nevertheless, this study had some limitations such as single-site inclusion, inclusion of a relatively frail cancer population predominantly included at inpatient units. Our results are not necessarily transferable to an outpatient population. Still, questionnaire-related sources of misinterpretation, such as the phrase “normal food” being ambiguous, could have been identified in outpatient population as well. ESPEN guidelines strongly recommend to screen for (risk of) malnutrition in patients with advanced cancer, thus it is essential to have a valid tool that fits all. In general, qualitative data are limited by the possibility of losing information and nuances when oral data are transcribed into written text, and also when translating quotes.
Conclusion
The PG-SGA Short Form was found to be easy to use and understand for the majority of the participants in this study. However, sources to misinterpretations were also identified, both participant-related and questionnaire-related sources. In order to reduce misinterpretation and missing/wrong answers when using PG-SGA, a standardized instruction manual could be used as guidance and training of patients and health care professionals. All future revisions of PG-SGA Short Form should be based on regular patient involvement in order to maintain and increase comprehensibility and relevance of the form.
Acknowledgments
We wish to thank all the patients we have met in the study period for their willingness to spend valuable time and energy on this trial, and the staff at the Cancer Clinic, St. Olavs Hospital, Trondheim University Hospital for their valuable assistance in the recruitment phase.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflict of interests in this work.
References
1. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
2. Guerra RS, Fonseca I, Sousa AS, Jesus A, Pichel F, Amaral TF. ESPEN diagnostic criteria for malnutrition – a validation study in hospitalized patients. Clin Nutr. 2017;36(5):1326–1332. doi:10.1016/j.clnu.2016.08.022
3. Britton B, McCarter K, Baker A, et al. Eating As Treatment (EAT) study protocol: a stepped-wedge, randomised controlled trial of a health behaviour change intervention provided by dietitians to improve nutrition in patients with head and neck cancer undergoing radiotherapy. BMJ Open. 2015;5(7):e008921. doi:10.1136/bmjopen-2015-008921
4. Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr. 2002;56(8):779–785. doi:10.1038/sj.ejcn.1601412
5. Rodrigues CS, Chaves GV. Patient-Generated Subjective Global Assessment in relation to site, stage of the illness, reason for hospital admission, and mortality in patients with gynecological tumors. Support Care Cancer. 2015;23(3):871–879. doi:10.1007/s00520-014-2409-7
6. Rodrigues CS, Lacerda MS, Chaves GV. Patient Generated Subjective Global Assessment as a prognosis tool in women with gynecologic cancer. Nutrition. 2015;31(11–12):1372–1378. doi:10.1016/j.nut.2015.06.001
7. Isenring E, Bauer J, Capra S. The scored Patient-generated Subjective Global Assessment (PG-SGA) and its association with quality of life in ambulatory patients receiving radiotherapy. Eur J Clin Nutr. 2003;57(2):305–309. doi:10.1038/sj.ejcn.1601552
8. Abbott J, Teleni L, McKavanagh D, Watson J, McCarthy AL, Isenring E. Patient-Generated Subjective Global Assessment Short Form (PG-SGA SF) is a valid screening tool in chemotherapy outpatients. Support Care Cancer. 2016;24(9):3883–3887. doi:10.1007/s00520-016-3196-0
9. Spotten L, Corish C, Lorton C, et al. Subjective taste and smell changes in treatment-naive people with solid tumours. Support Care Cancer. 2016;24(7):3201–3208. doi:10.1007/s00520-016-3133-2
10. Isenring E, Cross G, Daniels L, Kellett E, Koczwara B. Validity of the malnutrition screening tool as an effective predictor of nutritional risk in oncology outpatients receiving chemotherapy. Support Care Cancer. 2006;14(11):1152–1156. doi:10.1007/s00520-006-0070-5
11. Detsky AS, McLaughlin JR, Baker JP, et al. What is subjective global assessment of nutritional status? JPEN J Parenter Enteral Nutr. 1987;11(1):8–13. doi:10.1177/014860718701100108
12. Ottery FD. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition. 1996;12(1 Suppl):S15–S19.
13. Gabrielson DK, Scaffidi D, Leung E, et al. Use of an abridged scored Patient-Generated Subjective Global Assessment (abPG-SGA) as a nutritional screening tool for cancer patients in an outpatient setting. Nutr Cancer. 2013;65(2):234–239. doi:10.1080/01635581.2013.755554
14. Jager-Wittenaar H, Ottery FD. Assessing nutritional status in cancer: role of the Patient-Generated Subjective Global Assessment. Current Opinion in Clinical Nutrition and Metabolic Care. 2017;20(5):322–329. doi:10.1097/MCO.0000000000000389
15. Hsieh MC, Wang SH, Chuah SK, Lin YH, Lan J, Rau KM. A prognostic model using inflammation- and nutrition-based scores in patients with metastatic gastric adenocarcinoma treated with chemotherapy. Medicine (Baltimore). 2016;95(17):e3504. doi:10.1097/MD.0000000000004864
16. Harter J, Orlandi SP, Gonzalez MC. Nutritional and functional factors as prognostic of surgical cancer patients. Support Care Cancer. 2017;25(8):2525–2530. doi:10.1007/s00520-017-3661-4
17. Vigano AL, di Tomasso J, Kilgour RD, et al. The abridged patient-generated subjective global assessment is a useful tool for early detection and characterization of cancer cachexia. Journal of the Academy of Nutrition and Dietetics. 2014;114(7):1088–1098. doi:10.1016/j.jand.2013.09.027
18. Sealy MJ, Nijholt W, Stuiver MM, et al. Content validity across methods of malnutrition assessment in patients with cancer is limited. Journal of Clinical Epidemiology. 2016;76:125–136. doi:10.1016/j.jclinepi.2016.02.020
19. Wiering B, de Boer D, Delnoij D. Patient involvement in the development of patient-reported outcome measures: a scoping review. Health Expect. 2017;20(1):11–23. doi:10.1111/hex.12442
20. Mallinson S. Listening to respondents: a qualitative assessment of the Short-form 36 health status questionnaire. Soc Sci Med. 2002;54(1):11–21.
21. Willis GB, Artino AR
22. Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity–establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO Good Research Practices Task Force report: part 2–assessing respondent understanding. Value Health. 2011;14(8):978–988. doi:10.1016/j.jval.2011.06.013
23. Solheim TS, Laird BJA, Balstad TR, et al. A randomized phase II feasibility trial of a multimodal intervention for the management of cachexia in lung and pancreatic cancer. J Cachexia Sarcopenia Muscle. 2017;8(5):778–788. doi:10.1002/jcsm.12201
24. Vagnildhaug OM, Balstad TR, Almberg SS, et al. A cross-sectional study examining the prevalence of cachexia and areas of unmet need in patients with cancer. Support Care Cancer. 2018;26(6):1871–1880. doi:10.1007/s00520-017-4022-z
25. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z, Ad Hoc EWG. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003;22(3):321–336.
26. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655.
27. Paap MC, Lange L, van der Palen J, Bode C. Using the three-step test interview to understand how patients perceive the St. George’s Respiratory Questionnaire for COPD patients (SGRQ-C). Qual Life Res. 2016;25(6):1561–1570. doi:10.1007/s11136-015-1192-3
28. Bergh I, Kvalem IL, Aass N, Hjermstad MJ. What does the answer mean? A qualitative study of how palliative cancer patients interpret and respond to the edmonton symptom assessment system. Palliat Med. 2011;25(7):716–724. doi:10.1177/0269216310395985
29. Watanabe S, Nekolaichuk C, Beaumont C, Mawani A. The Edmonton symptom assessment system–what do patients think? Support Care Cancer. 2009;17(6):675–683. doi:10.1007/s00520-008-0522-1
30. Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: reliability, validity, and guidelines. J Clin Oncol. 1984;2(3):187–193. doi:10.1200/JCO.1984.2.3.187
31. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40(8):795–805. doi:10.1177/1403494812465030
32. Polkinghorne DE. Language and meaning: data collection in qualitative research. Journal of Counseling Psychology. 2005;52(2):137–145. doi:10.1037/0022-0167.52.2.137
33. Thayssen S, Hansen DG, Sondergaard J, Hoybye MT, Christensen PM, Hansen HP. Completing a questionnaire at home prior to needs assessment in general practice: a qualitative study of cancer patients’ experience. Patient. 2016;9(3):223–230. doi:10.1007/s40271-015-0144-x
34. Wintner LM, Sztankay M, Aaronson N, et al. The use of EORTC measures in daily clinical practice – a synopsis of a newly developed manual. Eur J Cancer. 2016;68:73–81. doi:10.1016/j.ejca.2016.08.024
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.