Back to Journals » Clinical Ophthalmology » Volume 10
Pars plana vitrectomy combined with internal limiting membrane peeling for recurrent macular edema due to branch retinal vein occlusion after antivascular endothelial growth factor treatments
Authors Shirakata Y, Fukuda K, Fujita T, Nakano Y ![]() , Nomoto H, Yamaji H, Shiraga F, Tsujikawa A
, Nomoto H, Yamaji H, Shiraga F, Tsujikawa A
Received 31 March 2015
Accepted for publication 7 October 2015
Published 5 February 2016 Volume 2016:10 Pages 277—283
DOI https://doi.org/10.2147/OPTH.S85751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yukari Shirakata,1 Kouki Fukuda,1 Tomoyoshi Fujita,1 Yuki Nakano,1 Hiroyuki Nomoto,2 Hidetaka Yamaji,3 Fumio Shiraga,4 Akitaka Tsujikawa1
1Department of Ophthalmology, Faculty of Medicine, Kagawa University, Miki-cho, 2Nomoto Eye Clinic, Himeji, 3Department of Ophthalmology, Shirai Eye Hospital, Mitoyo, 4Department of Ophthalmology, Okayama University, Okayama, Japan
Purpose: To evaluate the anatomic and functional outcomes of pars plana vitrectomy combined with internal limiting membrane peeling for recurrent macular edema (ME) due to branch retinal vein occlusion (BRVO) after intravitreal injections of antivascular endothelial growth factor (anti-VEGF) agents.
Methods: Twenty-four eyes of 24 patients with treatment-naive ME from BRVO were treated with intravitreal injections of anti-VEGF agents. Recurred ME was treated with pars plana vitrectomy combined with internal limiting membrane peeling.
Results: After the surgery, ME was significantly reduced at 1 month (P=0.031) and the reduction increased with time (P=0.007 at the final visit). With the reduction in ME, treated eyes showed a slow improvement in visual acuity (VA). At the final visit, improvement in VA was statistically significant compared with baseline (P=0.048). The initial presence of cystoid spaces, serous retinal detachment, or subretinal hemorrhage under the fovea, as well as retinal perfusion status, showed no association with VA improvement. However, the presence of epiretinal membrane showed a significant association with the visual recovery. Although eyes without epiretinal membrane showed visual improvement (-0.10±0.32 in logarithm of the minimum angle of resolution [logMAR]), eyes with epiretinal membrane showed greater visual improvement (-0.38±0.12 in logMAR, P=0.012).
Conclusion: For recurrent ME due to BRVO after anti-VEGF treatment, particularly when accompanied by epiretinal membrane, pars plana vitrectomy combined with internal limiting membrane peeling might be a possible treatment option.
Keywords: antivascular endothelial growth factor, branch retinal vein occlusion, internal limiting membrane peeling, macular edema, pars plana vitrectomy
Introduction
Macular edema (ME) is a complication of branch retinal vein occlusion (BRVO) with serious adverse effects on vision.1,2 Increased intravascular pressure and reduced blood flow in the macular capillaries lead to dysfunction of the endothelial blood–retinal barrier and to increased vascular permeability, resulting in ME.3 Although grid laser photocoagulation was previously the only established treatment for ME secondary to BRVO, visual recovery was slow and limited.1 Vascular endothelial growth factor (VEGF) has been reported to play an important role in the pathogenesis of ME secondary to BRVO,4–6 and the introduction of intravitreal anti-VEGF treatment has improved the visual prognosis of BRVO;7–10 this treatment has consequently been adopted as the standard treatment. The effect of anti-VEGF treatment on the absorption of ME is rapid, but most eyes need to be treated repeatedly. In the HORIZON trial, the mean number of injections of ranibizumab was 2.0–2.4 in the second year after the initiation of the treatment for ME associated with BRVO.11
Previously, some investigators reported the efficacy of pars plana vitrectomy combined with internal limiting membrane peeling for ME associated with BRVO.12–20 It was reported that the reduction in ME was not rapid after the surgery but the effect was maintained for years. For eyes with ME refractory to repeated intravitreal injections of anti-VEGF agents, surgical intervention may be a possible treatment option. Recently, Yunoki et al reported the efficacy of pars plana vitrectomy with internal limiting membrane peeling for recurrent ME associated with BRVO after intravitreal injections of bevacizumab.21 So far, however, limited information is available on this surgical intervention for recurrent or persistent ME after anti-VEGF treatment. In the study described herein, we retrospectively investigated the anatomic and functional outcomes of eyes treated with pars plana vitrectomy combined with internal limiting membrane peeling for recurrent ME due to BRVO, in spite of anti-VEGF treatment.
Patients and methods
For this retrospective study, we reviewed the medical records of 24 eyes of 24 consecutive patients who underwent pars plana vitrectomy combined with internal limiting membrane peeling for recurrent ME due to BRVO after anti-VEGF treatment at Kagawa University Hospital from October 2009 through December 2012. Patients were offered pars plana vitrectomy with internal limiting membrane peeling if they had visual loss caused by recurred ME after intravitreal injections of anti-VEGF agents. Exclusion criteria were proliferative diabetic retinopathy, vitreous hemorrhage, central retinal vein occlusion, dense cataract, or a short follow-up period of <6 months after the surgery. Eyes with previous focal scatter photocoagulation were included, but eyes with any previous treatments for ME were excluded from the current study (eg, intravitreal injections of any anti-VEGF agent or triamcinolone acetonide, or grid laser photocoagulation). This retrospective study was approved by the Institutional Review Board of the Faculty of Medicine, Kagawa University. The study adhered to the tenets of the Declaration of Helsinki. We did not obtain written informed consent from each participant, because according to the guidelines of the Institutional Review Board of the Faculty of Medicine, Kagawa University, it is not necessarily mandatory to obtain informed consent from the patients for a retrospective study in which the researchers reviewed only the patients’ medical records.
The diagnoses of BRVO and ME were made by fundus examination and confirmed by fluorescein angiography and optical coherence tomography (OCT). Each patient supplied a medical history and then underwent a complete ophthalmologic examination, including best-corrected visual acuity (VA) measurement with a Landolt chart, slit-lamp biomicroscopy, indirect fundus ophthalmoscopy, and OCT examination. In each patient, digital fundus photographs and fluorescein angiography were obtained using a digital fundus camera (TRC-50LX; Topcon, Tokyo, Japan) after pupil dilatation. Eyes with BRVO were classified as ischemic when the area of nonperfusion was >5 disk diameters in size.22 Macular perfusion status was also determined as complete or incomplete, according to the previous report of Finkelstein.23 Repeated fluorescein angiography was performed if necessary. To evaluate the condition of ME, OCT examination was performed (Cirrus; Carl Zeiss Meditec AG, Jena, Germany) at each visit. OCT examination included vertical and horizontal cross-sectional scans centered on the fovea. Central retinal thickness (CRT) was determined as the average retinal thickness in a 1 mm diameter circular region at the fovea.
In the current study, patients who suffered visual disturbances due to ME associated with BRVO were offered intravitreal injection of bevacizumab (Avastin; Genentech, Inc., South San Francisco, CA, USA). The inclusion criterion was eyes with a CRT >300 μm. In this study, pseudophakic eyes were included, but eyes that had undergone a prior vitrectomy were excluded. The dosage of bevacizumab was 1.25 mg/0.05 mL per injection. A retreatment was performed when eyes showed recurrence of ME with visual loss. Off-label use of bevacizumab was approved by the Institutional Ethics Committee; the study protocol adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from each patient. Intravitreal injection of ranibizumab (Lucentis; Novartis International AG, Basel, Switzerland) was also used for the recurred ME after its approval in Japan. The dosage of ranibizumab was 1.25 mg/0.05 mL per injection.
For the treatment for recurrent ME, all eyes in the current study underwent a standard 25-G three-port pars plana vitrectomy. After core vitrectomy, posterior vitreous detachment was induced if the cortical vitreous was adherent to the retina. The internal limiting membrane was peeled ~3.0 disk diameters around the fovea with the use of brilliant blue G. During the surgery, no laser photocoagulation was performed on the nonperfusion area of BRVO. For 14 phakic eyes, phacoemulsification and intraocular lens implantation were also performed.
Statistical analysis was performed using IBM SPSS Statistics Version 21.0 (IBM Corporation, Armonk, NY, USA). Values are presented as mean ± standard deviation. For statistical analysis, VA measured with a Landolt chart was converted to the logarithm of the minimum angle of resolution (logMAR). Repeated measurement of analysis of variance was used to analyze CRT and VA after the initiation of the treatment. Student’s t-test was used for comparisons of the change in VA during the treatment between eyes classified by the initial retinal features. A P-value of <0.05 was considered statistically significant.
Results
In the current study, 24 eyes of 24 patients with BRVO (ten women and 14 men) were included (Table 1). At the initial visit, all eyes showed ME with symptomatic visual disturbance. VA ranged from 0.05 to 1.05 (average, 0.44±0.31) in logMAR. No eyes had previously been treated with intravitreal injections of any anti-VEGF agent or triamcinolone acetonide, or grid laser photocoagulation.
 | Table 1 Baseline characteristics of eyes treated with pars plana vitrectomy with internal limiting membrane peeling for recurrent macular edema associated with branch retinal vein occlusion |
After the comprehensive ophthalmic examinations, each eye was treated with an intravitreal injection of bevacizumab. Immediately after treatment, a reduction in ME was achieved. Compared with baseline, CRT was decreased significantly at 1 month (P=0.0018). VA was also significantly improved at 1 month after the initial injection (P=0.0050). However, all eyes showed recurrence of ME, and 14 eyes were received additional injection of anti-VEGF agents (bevacizumab or ranibizumab). Mean number of injections of anti-VEGF agent was 2.33±1.46 (Table 2). One eye was also treated with a subtenon injection of triamcinolone acetonide for recurrent ME. The duration of the initiation of anti-VEGF treatment to undergoing pars plana vitrectomy was 2–32 months (mean, 10.8±9.0 months).
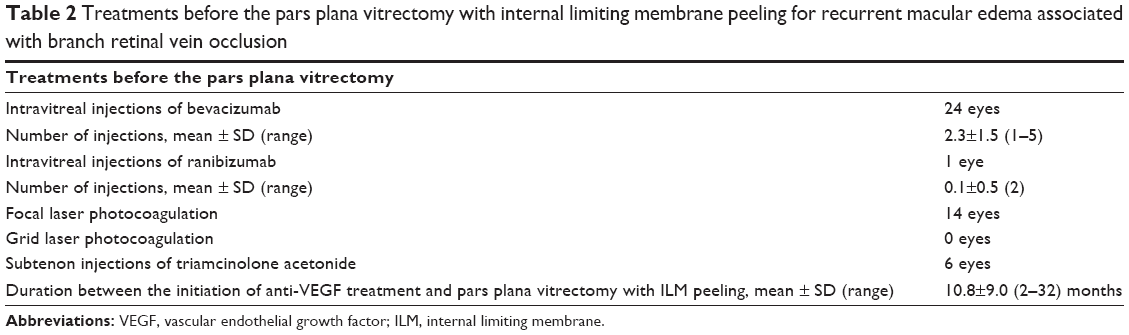 | Table 2 Treatments before the pars plana vitrectomy with internal limiting membrane peeling for recurrent macular edema associated with branch retinal vein occlusion |
In spite of the treatment for ME, all eyes showed recurrent ME with subjective visual disturbance. Each eye was treated with pars plana vitrectomy with internal limiting membrane peeling. Phacoemulsification extraction of cataract and intraocular lens implantation were performed in 14 patients. A subtenon injection of triamcinolone acetonide was performed in six eyes. Figure 1 shows the changes in CRT and VA after the surgery. CRT was significantly reduced at 1 month (P=0.031) after the surgery, and the reduction increased with time (P=0.007 at the final visit). With the reduction in CRT, VA also improved albeit slowly. Mean follow-up after the surgery was 13.8±10.8 months. At the final visit, however, improvement in VA was statistically significant compared with baseline VA (P=0.048), although not significant compared with VA before the surgery (P=0.078). No serious complications were seen during or after the surgery.
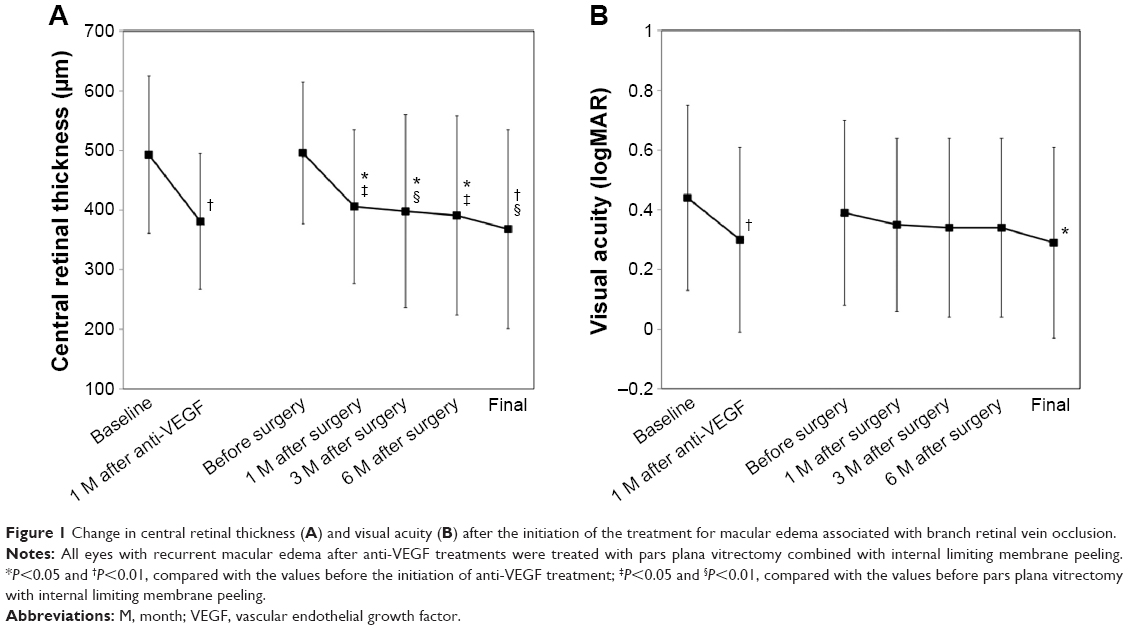 | Figure 1 Change in central retinal thickness (A) and visual acuity (B) after the initiation of the treatment for macular edema associated with branch retinal vein occlusion. |
In the current study, mean follow-up after the initial treatment was 24.5±10.8 months. Table 3 shows the comparisons of the change in VA and CRT during the treatment between eyes classified by the initial retinal features. The presence of cystoid spaces, serous retinal detachment, or subretinal hemorrhage under the fovea had no significant association with the change in VA. Perfusion status in either the extramacular or the macular area showed no significant association. However, the presence of epiretinal membrane showed a significant association with the visual recovery. Although eyes without epiretinal membrane showed visual improvement (−0.10±0.32) with the treatment, eyes with epiretinal membrane showed greater visual improvement (−0.38±0.12, P=0.012, Figure 2).
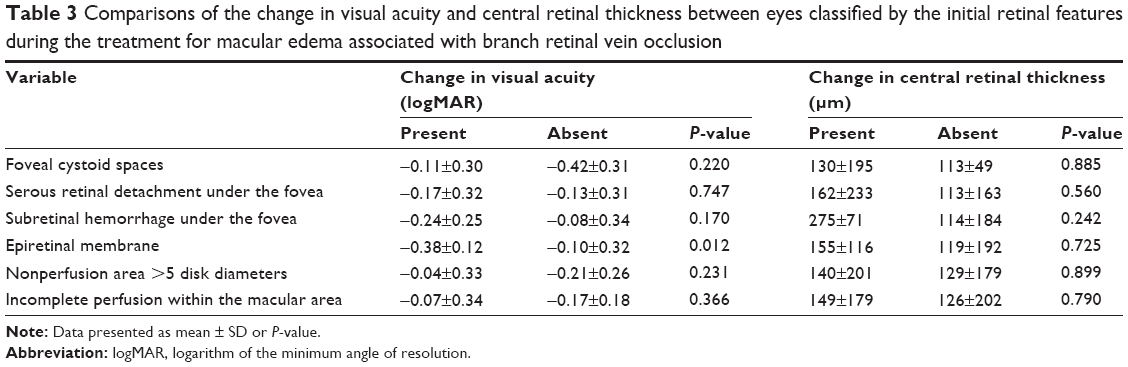 | Table 3 Comparisons of the change in visual acuity and central retinal thickness between eyes classified by the initial retinal features during the treatment for macular edema associated with branch retinal vein occlusion |
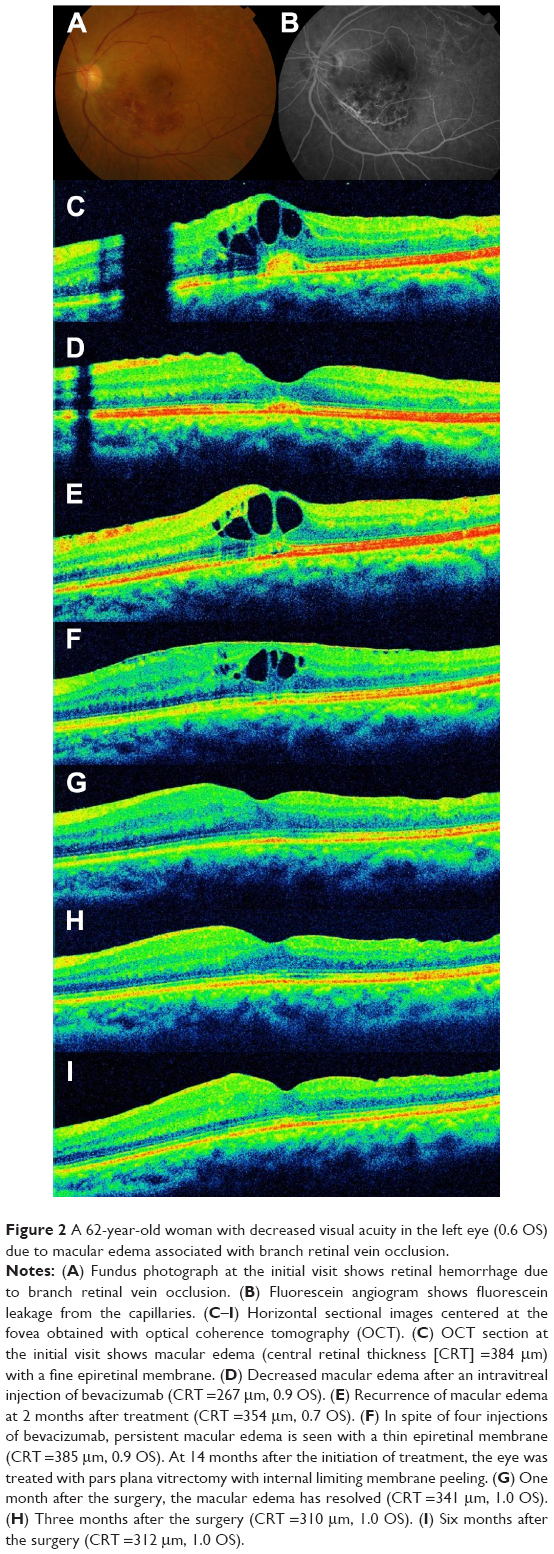 | Figure 2 A 62-year-old woman with decreased visual acuity in the left eye (0.6 OS) due to macular edema associated with branch retinal vein occlusion. |
Discussion
Since the Branch Vein Occlusion Study Group reported the efficacy of grid laser photocoagulation for chronic ME associated with BRVO,1 grid laser photocoagulation has been the only established treatment for ME associated with BRVO. However, the visual recovery is slow and limited because the average number of lines gained in treated eyes is limited to 1.33. Now, anti-VEGF treatment is generally accepted as the first choice for ME associated with BRVO.7–9,24 Indeed, the effect of anti-VEGF treatment is rapid and remarkable. In the BRAVO study, the mean improvement in VA was 16.6 and 18.3 letters with 6 monthly injections of ranibizumab (0.3 mg and 0.5 mg, respectively).10 However, most eyes need to be treated repeatedly. In the HORIZON trial, the mean number of injections of ranibizumab was 2.0–2.4 in the second year after the initiation of the treatment for ME associated with BRVO.11 The RETAIN study showed that long-term outcomes in BRVO treated with ranibizumab were excellent but that approximately half of the cases still required occasional injections after 4 years.25 Although the anti-VEGF treatment for ME is convenient and has a rapid effect, repeated injections may be a burden for patients.
In the current study, an intravitreal injection of bevacizumab achieved rapid reduction in ME. In spite of repeated treatment for ME, however, all eyes showed recurrent ME with subjective visual disturbance. All our patients treated with pars plana vitrectomy with internal limiting membrane peeling achieved reduction in ME. To date, some investigators have reported the efficacy of this surgical intervention for ME associated with BRVO.12–20 However, most reports show efficacy for treatment-naive ME, and limited information is available on recurrent ME. Recently, Yunoki et al showed promising effects of pars plana vitrectomy with internal limiting membrane peeling for recurrent ME due to BRVO after intravitreal injections of bevacizumab.21 In their report, the improvement in VA was achieved as early as 1 month after the surgery while our patients did not as long as 6 months. This surgical intervention may be a treatment option for ME refractory to the anti-VEGF treatment.
The precise mechanism by which this surgical intervention reduces ME remains uncertain. Vitrectomy may have beneficial effects on retinal ischemia by allowing oxygenated fluid to circulate in the vitreous cavity.26 In addition, vitreomacular attachment is suggested to be involved in persistent ME in eyes with BRVO. Takahashi et al reported that the incidence of ME was higher in eyes with no or partial posterior vitreous detachment.27 Therefore, induction of posterior vitreous detachment may contribute primarily to the absorption of ME associated with BRVO. Internal limiting membrane peeling may contribute to the complete removal of traction in the macular area.
Previous reports showed that fovea cystoid spaces, fovea serous retinal detachment, and subretinal hemorrhage are signs of poor visual prognosis in BRVO.28–31 In the current study, these features had no significant association with the change in VA. Finkelstein reported incomplete macular perfusion as a sign of good VA prognosis in ischemic ME.23 In the current study, perfusion status in either the extramacular or the macular area showed no significant association with VA improvement. However, the presence of epiretinal membrane showed a significant association with the visual recovery. Physicians sometimes see eyes with ME due to BRVO together with a fine epiretinal membrane. In case the epiretinal membrane is the primary cause of visual disturbance, surgical intervention is indicated. Because the treatment effect of anti-VEGF agents is limited in vitrectomized eyes because of rapid clearance,32 physicians tend to choose anti-VEGF agents as the initial treatment for ME even if it is accompanied by a fine epiretinal membrane. Previously, Marticorena et al reported that intravitreal bevacizumab may be associated with early development of epiretinal membrane in eyes with retinal vein occlusion.33 When such eyes show persistent ME, surgical intervention may help.
This study has several limitations, mainly the small sample size (especially eyes with epiretinal membrane) and retrospective study design. In the current study, epiretinal membrane showed a significant association with the postoperative visual recovery. A recent report by Yunoki et al showed no favorable VA change in eyes with epiretinal membrane or vitreomacular traction after surgery. Small sample size in the current study may account for the discrepancy.21 In addition, the noncomparative design of this study prevented determination of whether surgical intervention improved the visual prognosis. In the current study, phacoemulsification extraction of the cataract and intraocular lens implantation was performed in 14 patients. Accordingly, VA results in our patients may be relatively difficult to interpret. However, as shown in Figure 1, while the reduction in CRT was already significant at 1 month, postoperative improvement in VA was slow. In addition, mean VA change at 1 month in eyes with combined cataract surgery (−0.06±0.33) was not different, compared with eyes without (0.00±0.12, P=0.525; data not shown). The effect of cataract surgery on VA improvement would be limited.
Conclusion
In the retrospective study reported herein, pars plana vitrectomy combined with internal limiting membrane peeling showed efficacy for recurrent ME associated with BRVO after anti-VEGF treatment. There is no doubt that anti-VEGF treatment is the first choice for ME associated with BRVO. For recurrent ME, particularly when accompanied by epiretinal membrane, surgical intervention may be a possible option. This is a small case series; therefore, a prospective study with larger sample populations is necessary to evaluate the efficacy of surgical interventions in such eyes.
Acknowledgments
This study was supported, in part, by the Japan Society for the Promotion of Science (JSPS, Tokyo, Japan, grant-in-aid for Scientific Research). The authors have full control of all primary data and they agree to allow Clinical Ophthalmology to review their data upon request.
Disclosure
The authors report no conflicts of interest in this work.
References
The Branch Vein Occlusion Study Group. Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol. 1984;98(3):271–282. | ||
Glacet-Bernard A, Coscas G, Chabanel A, Zourdani A, Lelong F, Samama MM. Prognostic factors for retinal vein occlusion: prospective study of 175 cases. Ophthalmology. 1996;103(4):551–560. | ||
Rehak J, Rehak M. Branch retinal vein occlusion: pathogenesis, visual prognosis, and treatment modalities. Curr Eye Res. 2008;33(2):111–131. | ||
Noma H, Funatsu H, Yamasaki M, et al. Pathogenesis of macular edema with branch retinal vein occlusion and intraocular levels of vascular endothelial growth factor and interleukin-6. Am J Ophthalmol. 2005;140(2):256–261. | ||
Noma H, Minamoto A, Funatsu H, et al. Intravitreal levels of vascular endothelial growth factor and interleukin-6 are correlated with macular edema in branch retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 2006;244(3):309–315. | ||
Noma H, Funatsu H, Yamasaki M, et al. Aqueous humour levels of cytokines are correlated to vitreous levels and severity of macular oedema in branch retinal vein occlusion. Eye. 2008;22(1):42–48. | ||
Prager F, Michels S, Kriechbaum K, et al. Intravitreal bevacizumab (Avastin) for macular oedema secondary to retinal vein occlusion: 12-month results of a prospective clinical trial. Br J Ophthalmol. 2009;93(4):452–456. | ||
Wu L, Arevalo JF, Berrocal MH, et al. Comparison of two doses of intravitreal bevacizumab as primary treatment for macular edema secondary to branch retinal vein occlusions: results of the Pan American Collaborative Retina Study Group at 24 months. Retina. 2009;29(10):1396–1403. | ||
Kreutzer TC, Alge CS, Wolf AH, et al. Intravitreal bevacizumab for the treatment of macular oedema secondary to branch retinal vein occlusion. Br J Ophthalmol. 2008;92(3):351–355. | ||
Campochiaro PA, Heier JS, Feiner L, et al; BRAVO Investigators. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1102–1112e1101. | ||
Heier JS, Campochiaro PA, Yau L, et al. Ranibizumab for macular edema due to retinal vein occlusions: long-term follow-up in the HORIZON trial. Ophthalmology. 2012;119(4):802–809. | ||
Arai M, Yamamoto S, Mitamura Y, Sato E, Sugawara T, Mizunoya S. Efficacy of vitrectomy and internal limiting membrane removal for macular edema associated with branch retinal vein occlusion. Ophthalmologica. 2009;223(3):172–176. | ||
Baharivand N, Hariri A, Javadzadeh A, Heidari E, Sadegi K. Pars plana vitrectomy and internal limiting membrane peeling for macular edema secondary to retinal vein occlusion. Clin Ophthalmol. 2011;5:1089–1093. | ||
Kumagai K, Furukawa M, Ogino N, Larson E, Uemura A. Long-term visual outcomes after vitrectomy for macular edema with foveal hemorrhage in branch retinal vein occlusion. Retina. 2007;27(5):584–588. | ||
Ma J, Yao K, Zhang Z, Tang X. 25-gauge vitrectomy and triamcinolone acetonide-assisted internal limiting membrane peeling for chronic cystoid macular edema associated with branch retinal vein occlusion. Retina. 2008;28(7):947–956. | ||
Mandelcorn MS, Mandelcorn E, Guan K, Adatia FA. Surgical macular decompression for macular edema in retinal vein occlusion. Can J Ophthalmol. 2007;42(1):116–122. | ||
Mandelcorn MS, Nrusimhadevara RK. Internal limiting membrane peeling for decompression of macular edema in retinal vein occlusion: a report of 14 cases. Retina. 2004;24(3):348–355. | ||
Mester U, Dillinger P. Vitrectomy with arteriovenous decompression and internal limiting membrane dissection in branch retinal vein occlusion. Retina. 2002;22(6):740–746. | ||
Raszewska-Steglinska M, Gozdek P, Cisiecki S, Michalewska Z, Michalewski J, Nawrocki J. Pars plana vitrectomy with ILM peeling for macular edema secondary to retinal vein occlusion. Eur J Ophthalmol. 2009;19(6):1055–1062. | ||
Shah GK, Rosenblatt BJ, Blinder KJ, Grand MG, Smith M. Triamcinolone-assisted internal limiting membrane peeling. Retina. 2005;25(8):972–975. | ||
Yunoki T, Mitarai K, Yanagisawa S, Kato T, Ishida N, Hayashi A. Effects of vitrectomy on recurrent macular edema due to branch retinal vein occlusion after intravitreal injection of bevacizumab. J Ophthalmol. 2013;2013:415974. | ||
Branch Vein Occlusion Study Group. Argon laser scatter photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. A randomized clinical trial. Arch Ophthalmol. 1986;104(1):34–41. | ||
Finkelstein D. Ischemic macular edema. Recognition and favorable natural history in branch vein occlusion. Arch Ophthalmol. 1992;110(10):1427–1434. | ||
Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology. 2011;118(8):1594–1602. | ||
Campochiaro PA, Sophie R, Pearlman J, et al; RETAIN Study Group. Long-term outcomes in patients with retinal vein occlusion treated with ranibizumab: the RETAIN study. Ophthalmology. 2014;121(1):209–219. | ||
Tachi N, Hashimoto Y, Ogino N. Vitrectomy for macular edema combined with retinal vein occlusion. Doc Ophthalmol. 1999;97(3–4):465–469. | ||
Takahashi MK, Hikichi T, Akiba J, Yoshida A, Trempe CL. Role of the vitreous and macular edema in branch retinal vein occlusion. Ophthalmic Surg Lasers. 1997;28(4):294–299. | ||
Tsujikawa A, Sakamoto A, Ota M, et al. Serous retinal detachment associated with retinal vein occlusion. Am J Ophthalmol. 2010;149(2):291–301.e295. | ||
Ohashi H, Oh H, Nishiwaki H, Nonaka A, Takagi H. Delayed absorption of macular edema accompanying serous retinal detachment after grid laser treatment in patients with branch retinal vein occlusion. Ophthalmology. 2004;111(11):2050–2056. | ||
Muraoka Y, Tsujikawa A, Murakami T, Ogino K, Miyamoto K, Yoshimura N. Branch retinal vein occlusion-associated subretinal hemorrhage. Jpn J Ophthalmol. 2013;57(3):275–282. | ||
Ota M, Tsujikawa A, Miyamoto K, Sakamoto A, Murakami T, Yoshimura N. Visual acuity following intravitreal bevacizumab for macular edema associated with retinal vein occlusion. Jpn J Ophthalmol. 2010;54(6):555–564. | ||
Kakinoki M, Sawada O, Sawada T, Saishin Y, Kawamura H, Ohji M. Effect of vitrectomy on aqueous VEGF concentration and pharmacokinetics of bevacizumab in macaque monkeys. Invest Ophthalmol Vis Sci. 2012;53(9):5877–5880. | ||
Marticorena J, Romano MR, Heimann H, et al. Intravitreal bevacizumab for retinal vein occlusion and early growth of epiretinal membrane: a possible secondary effect? Br J Ophthalmol. 2011;95(3):391–395. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.