Back to Journals » Substance Abuse and Rehabilitation » Volume 6
Parenthood and opioid dependence
Authors Pihkala H, Sandlund M
Received 14 October 2014
Accepted for publication 18 December 2014
Published 10 February 2015 Volume 2015:6 Pages 33—40
DOI https://doi.org/10.2147/SAR.S75796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Li-Tzy Wu
Heljä Pihkala, Mikael Sandlund
Institution of Clinical Sciences/Psychiatry, Umeå University, Umeå, Sweden
Introduction: Many patients in maintenance treatment programs for opioid dependence are parents to underage children.
Objective: The aim of this study was to explore how parents who are regular patients in maintenance treatment perceive their parenthood.
Methods: The study used a qualitative approach. The informants were recruited by staff at a substance abuse clinic in Sweden. Criteria for inclusion were participation in the local maintenance treatment program, having a child or children younger than 18 years, and being in contact with the child or children. Data were collected in 2012–2013 by in-depth interviews of seven fathers and five mothers and analyzed using concepts and procedures of qualitative content analysis.
Results: The central findings of the study were: 1) the parents’ concerns about possible future discrimination against their children, ie, stigma by association; and 2) the patients’ own parents’ role as the most important support in parenthood.
Conclusion: The issue of anticipated discrimination against the children of parents undergoing maintenance treatment might be an aspect to consider in the development of interventions and support. Considering the role of the patients' own parents also seems important.
Keywords: parenthood, opiod dependence, maintenance treatment, qualitative analysis, anticipated stigma, stigma by association
Introduction
Rehabilitation programs for persons with severe opioid dependence, including maintenance treatment (MT) with buprenorphine or methadone, are common in most high-income countries. The results of such programs are generally considered good: decreased drug use and mortality, patients remaining in the programs, and improved quality of life.1,2 On the other hand, social control and institutional stigma are also felt by many patients in such programs.3
Many of the patients are parents. A number of studies have examined issues concerning the children of opioid-dependent patients in MT: prenatal exposure to methadone or buprenorphine, their potential developmental effects on the child, and the mother–child relationship. Such children have been highlighted as a risk group for developmental and behavioral deviations from early years to adolescence.4–6 It is known that substance abuse/dependence is a risk factor for problems in parental functioning.7 Persons in MT always have a history of heavy substance abuse, and criminality and comorbidity with mental illness are common. Consequently, it is likely that parenthood is a challenging task for such patients. Those in MT have often achieved significantly improved social and psychological adaptation compared to the period prior to MT.2 Nevertheless, MT patients remain dependent on a legal drug and tied to the health care system that prescribes it, although many of them wish to end the medication.8
Previous studies on MT and parenthood have mainly focused on mothers and on the perinatal period, parental strategies for harm minimizing drug use to their children, provided/needed support in parenting, and stigmatization of the parent.9–12 Skinner et al5 showed that parent–child ties are often sustained into young adulthood, highlighting the importance of parenthood. The aim of this study was to explore how parents who are regular patients in MT perceive their parenthood.
Methods
We used a qualitative approach with in-depth interviews and qualitative analysis of the data.
Settings and informants
Informants were recruited by staff at a substance abuse clinic in northern Sweden. The catchment area consisted of about 80,000 inhabitants. The unit had 79 patients (19 females) in the MT program, of whom 42 (12 females) had children under 18 years of age. The criteria for inclusion were participation in the local MT program, having a child or children younger than 18 years, and being in contact with the child or children. A selection was made to obtain variation in informant age, sex, and family circumstances. The staff members at the clinic invited patients to interviews according to these factors. Twelve patients were invited, and all agreed to be interviewed (see Table 1 for background data on the informants). All but one of the informants had suffered from substance abuse since adolescence. All had been subjects to compulsory addiction care. According to Swedish legislation, the Social Services may initiate compulsory care when a person’s health or life is in danger because of substance abuse.
 | Table 1 The informants |
The children and families
The informants had in total 18 children, 1–16 years of age, with a mean age of 7.4 years. Two of the female patients were pregnant, as was the partner of one of the male patients. Two of the seven men lived with their children; both men were living on social benefits and one lived with the mother of the children. The remaining five men spent time with their children to varying extents. All of the women lived with their children: two were single parents, one lived with the father of three of her five children, one lived with the father of their unborn baby, and one lived with the father of her children. The family constellations were complex, eg, two ex-partners had died from drug overdose or suicide.
Data collection and analysis
Data were collected by individual qualitative interviews conducted by the first author (HP) in 2012–2013.13 HP is a consultant psychiatrist and her focus of research is communication in families with parental mental illness. The second author (MS) is a consultant psychiatrist in drug abuse services and works with mental health systems research. The interviews took place at the outpatient clinic where the informants received their medication. The interviews were made as open-ended as possible. The informants were first invited to talk about their experiences as parents. Subjects covered included, for example, pregnancy and the period after the birth of the child, the support the parent can call on, concerns about their child or children, experiences of discrimination, and views on drugs and parenthood. An interview guide covering topics of interest was used as a support during the interviews (Figure S1). The topics were based on earlier research on the area: substance dependence is a risk factor for problems in parental functioning and the children run a high risk of developmental and behavioral deviations,4–7and parents in MT face judgmental attitudes from the health care system.9–11 The interviews lasted for 30 to 75 minutes. They were recorded and subsequently transcribed by an assistant.
Qualitative content analysis of the data was made using concepts and procedures suggested by Graneheim and Lundman.14 The authors read each interview transcript several times and conducted a line-to-line examination and divided the text into meaning units, ie, sentences, or paragraphs relating to a topic. The meaning units were condensed and labeled with codes identifying similar content. The codes were then compared, discussed, and sorted into six categories.
Ethics
The study was approved by the regional Ethics Committee of Umeå University, Umeå, Sweden (Dnr 2012-70-31M).
Results
Six categories were identified: 1) pregnancy – surprise and shock; 2) substance abuse and being a parent – bad conscience; 3) support – one’s own parents; 4) anticipated stigma by association; 5) longing for a child; and 6) a normal life. These categories are mainly descriptive and cover all information relevant to the aim of the study. See Table 2 for a summary of the results.
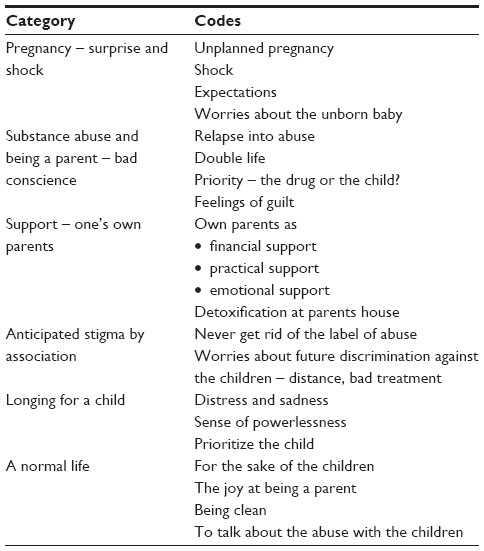 | Table 2 Summary of the results: the categories and codes |
Pregnancy – surprise and shock
Almost all of the pregnancies were unplanned. The pregnancy had often come as a “shock”, especially for the men, but gradually they had accepted it and adapted to the new situation. Positive expectations were common during pregnancy, although the men were uncertain whether they would be able to meet all the practical and financial demands on a parent, as most were in an active period of abuse. They had intended to get clean but were unable to achieve this before they entered MT, which could be many years later. Severe problems in their relationship and cooperation with the child’s mother started, continuing for several years in a number of cases.
Some of the women had not expected to get pregnant, because they had never become pregnant before entering MT, despite not using contraception. After the initial shock or confusion, the women were content during pregnancy, with most of them feeling good. Some were concerned about the possible harmful effects of buprenorphine on their baby, and tried but could not stop their medication: “It’s not funny to think that your baby has to be detoxicated just after being born.”
Substance abuse and being a parent – bad conscience
The mothers had been able to be mostly clean during pregnancies, even during pregnancies before they entered MT, but relapsed, for example, after the end of breastfeeding: “I just wanted to have a party one time, like everyone else.” Almost all the informants had abused drugs while a parent at some time. Discussing what their priority was – their child or the drug – was a complex issue. The informants took the drugs to feel well and to be able to do things with their children:
You feel good when you take the drug and when you are on it; you’ll be in a bad mood if you don’t take it. So I thought … if I take it, I’ll feel better; I will have a better conscience in the evening because I know he has had a good day; I have had the energy to play and be the mother I wanted to be.
However, during periods of abuse the drug was the first priority. A father put it like this: “When you have the drug, the children are number one; but when you don’t have it, the drug is number one.” The informants described many feelings of guilt about these periods – what children had had to witness, what they had lost, or what they had never had because of the drugs. In some cases, there were really dramatic episodes such as police interventions at their home with the children present; there was also remorse about the fact that the child had not had an emotionally engaged parent.
Some of the informants had been “successful” at maintaining a double life for long periods: they had regular work, daily routines, self-discipline, and backup with the children. They took the drug, in controlled doses, when the child was asleep, and always bought the drug from reliable suppliers and in large quantities to minimize contact with other addicts. This required quite advanced strategies for concealing things from their family, employer, children’s daycare, and Social Services: “I’ve been an expert … it’s not good … I’ve been so good at hiding, I’ve lived a real double life … I can’t believe they didn’t notice.” Finally, the situation in the families fell apart and they were found out, and many of the children were taken into custody of Social Services for a period.
The informants also worried about the heredity of drug dependence, but thought that their children had seen so much of the negative side of drugs that they were “immune” or “scared” and therefore not susceptible. One of the adult children of the informants was also a drug abuser, which was very painful for the parent, who blamed himself. Mostly the children seemed to feel and do quite well according to the informants. Only one of the informants living with their children told about specific problems at school or their child’s health problems.
Support – one’s own parents
The most important support in parenthood was the informants’ own parents. They took care of their grandchildren when the informants were in treatment or when an informant had relapsed and needed backup with the children for a while. It was common for Social Services to place the children in the custody of the grandparents for a certain period. Some of the fathers met their children at their parents’ home, often with the grandmother. Instead of seeking help at the hospital, several informants had gone through detoxification at their parents’ home in order to avoid discovery of their abuse. The parents provided emotional, practical, and financial support relating to the grandchildren: “They have always been there for me; they have helped me with everything.”
Most of the informants felt they received some support from the MT program. They had had conversations about their children, and two had been offered family intervention or family conversations. Their opinions of Social Services varied – from hostile to experiences of good support. A program for early attachment was appreciated by all the women who had participated in it. The informants who lived with their children had no contact with the Social Services by the time of the interview.
Anticipated stigma by association
Almost all the informants were concerned that their children might be stigmatized in the future because of their parents’ history of drug abuse. They supposed that their past abuse was known by the teachers and the other parents in the children’s school or daycare. They were worried that their children might not be accepted by other parents or as friends, and whether their children’s friends would be allowed to visit their home:
When he will be a little bit older, after a couple of years, his friends in daycare he has now may not be allowed to come home to us because the parents know that I have taken drugs, you know they still … “but oh my God, she has been a junkie”… maybe we should move from this area … but I am still here and they know. I hope he will not suffer because of my abuse.
There were also concerns about how the children’s friends would react if they find out that their friend’s parent has been a drug addict. The informants were observant regarding their children’s friendships and schooling. One parent reflected on if her own way of being among the other parents could affect her child. She was withdrawn and shy and did not take initiatives to contact the other parents. She suspected that her son made fewer friends because she was different. Feelings of sorrow and anger were associated with this category:
They always talk, I don’t care, but when it affects my child I feel mad. When he was not allowed to play with the other kids, it was not okay. That I have done stupid things doesn’t mean that he is a bad or dangerous person!
The informants did not state that their children suffered from discrimination at the moment, but they were nevertheless anxious about the future, on the basis of their own experiences:
We try to give them as a normal childhood as possible, but I think about when they are teenagers. How will that turn out? I know what it can be like … how will they be treated? That’s why it would be nice to move and make a fresh start.
All of the informants had experienced stigmatization in one way or another at some time, and this sense was still present for many. It was experienced in subtle ways in society in general, in the form of gossip, in looks, or in shops. Maternity care was experienced as supportive and nonjudgmental by most of the mothers, but one parent in particular had been treated in a discriminating manner at the hospital emergency department. Informants had varying experiences of Social Services, too. Staff at the children’s school or daycare had mostly treated the parents and the children in a fair manner.
Longing for a child
Five of the fathers met their children only 1 day or for only a few hours every 2 weeks, or irregularly. They felt distress and sadness, and longing for their children took a lot of energy out of them. They had a sense of powerlessness in relation to the child’s mother and were uncertain about their rights as a parent. However, they wished to avoid a legal process for custody, considering the child’s loyalty to the mother. They preferred to wait until the child was older and could decide for him- or herself. Although the men had no intention of assuming custody of the child, they wanted to have regular, scheduled access to their child, given that they were clean, which they all had been for quite a long period. Although these fathers could not spend much time with their children, fatherhood was nevertheless a reason to stay clean: “To be part of it and be able to be a father … that’s a strong argument for being clean.” There was pressure to have fun with the child in those short moments when they met, suggesting a fear of being forgotten. The fathers were also worried about the child’s well-being in periods of conflict with the mother.
A normal life
All the informants struggled for a “normal life” – a decent place to live and work and daily routines – for the sake of their children. Some had come a long way in their efforts. All the informants expressed joy at being a parent. Everyday activities like brushing teeth with the children could be experienced deeply and gave meaning to all their efforts. Being clean (drug-free) was a condition for normal life, ie, to be able to be a parent with custody of the children. Further, MT was the condition for being clean. Some of the informants felt imprisoned by the system and the medication, while others said that the medication was “a godsend”.
To talk with their child about their past drug abuse was a major issue for many of the informants. They considered it important to do so because honesty with the child was regarded as the basis of parenthood: “We’re okay, but we’re not an ordinary family. Recovering as a parent means talking about everything that’s happened.” It was difficult for many because of their feelings of shame and guilt, but almost all of the parents had talked with their older children (older than 7 years) and aimed to do so with their younger children later on.
Discussion
The interviewed patients who lived with their children were generally quite satisfied with their situation as parents. The main concern regarding their children was future bad treatment and discrimination – anticipated stigma by association. The informants’ own parents had been and remained the most significant support in parenthood. The priority setting between the child and the drug in periods of abuse was a complex issue, giving rise to feelings of guilt and shame, and making it difficult to discuss the abuse with their children, even after a long time. MT seemed to be the only way to maintain a parental role and custody for many informants, but some felt imprisoned in the system. The men who only occasionally met with their children prioritized the children’s welfare.
Limitations
As the number of interviewed parents was relatively small, the transferability, ie, the external validity, of the results is limited. Findings from 12 informants cannot be generalized to the population at large, but are rather descriptions within a specified setting. A large number of informants could strengthen, although not guarantee, transferability. The description of the context makes it possible for the reader to judge if our findings are applicable or not to other situations.15
Another issue regarding qualitative research is the question of subjectivity. A researcher’s background and position will always affect his/her interpretations of the material. Researchers need to identify and be aware of their preconceptions in order to be reflexive at every step of the research process and thereby counteract subjectivity.15 Our point of departure is long experience from clinical practice including frequent contact with patients and relatives in different situations. This contributes to openness to the fact that people live their lives in many different ways. We may tend to see many phenomena as normal rather than conspicuous. Thus, an analysis close to the informants’ accounts was preferred.
Anticipated stigma of the children
Persons suffering from drug dependence are heavily burdened by stigmatization. The public attitudes against drug misusers are dominated by a wish for social distance.16 Patients in MT do not get rid of the stigma associated with drug dependence.3 Further, according to Chandler et al and Radcliffe, judgmental attitudes to drug-dependent parents, including those in MT, have a negative impact on the parents’ efforts to reach “good-enough” parental functioning and their access to services during the perinatal period.9–11 However, the parents in our study were more concerned about how the stigma would affect their children. This concern is not unfounded: it has been shown that stigma may affect all family members when there is mental illness in a family.17 Some of the informants had concrete strategies in mind to avoid stigmatization of their children. On the other hand, the patients had neither experienced significant discrimination as a parent – in many instances they felt they received fair treatment – nor did they state that their children were discriminated against. According to a new Swedish study of persons with mental illness, parenthood was not the domain where discrimination was most often perceived.18 Thus, a process of self-stigmatization, with internalized stereotypes leading to anticipated discrimination of the children, seems to explain the parents’ worries about their children’s future. Anticipated stigma has harmful effects, limiting an individual’s life in many domains.19 It is possible that anticipated discrimination of their children could affect patients’ functioning as a parent and therefore possibly affect their children negatively, too. Interventions addressing self-stigma have been introduced.20 Consequently, the issue of anticipated discrimination of children should be included in such interventions.
The topic of anticipated stigma of the children relates to the parents’ feelings of shame and guilt and how to talk with the children about their past drug abuse – the heart of the matter being the parents’ inability to give up drugs despite being a parent, thereby risking loss of custody of the children. Supporting the parents in talking about parenthood and their children’s situation, and in discussing these topics with their children, may help some patients overcome their feelings of shame and guilt in relation to their children and as parents. Beardslee’s family intervention21 – a structured, family-focused psychoeducative intervention – has been shown to decrease parents’ feelings of shame and guilt toward their children in families with parental mental illness.22 It would therefore be of interest to offer parents in MT interventions like Beardslees and study the effectiveness regarding children’s well-being as well as parents’ self-stigma and anticipated discrimination of the children.
Patients’ own parents as support
The role of the patients’ own parents as the most important source of support is worth noting. The informants described their own parents with warmth and appreciation. This contrasts with findings of Earnshaw et al, who described how many patients in MT experienced stereotyping and discriminating attitudes from their parents.23 A possible explanation may be that the situation with grandchildren changes the relations in the family. It was common that the grandparents took care of their grandchildren and had custody of them in periods. This corresponds to international studies showing that parental drug abuse is the most common reason for grandparents having custody of the children.24 On the other hand, sometimes the help from parents seemed to enable the drug abuse to continue. This shows the power and the complexity of family bonds – as an important support but also as a codependence with double-edged effects.
Conclusion
Support of parents and their children in substance abuse care is an important task from a preventive perspective and is legally obligated in some Nordic countries. Work to develop methods and policies is ongoing in many clinics and districts. The issues of self-stigmatization as a parent and anticipated discrimination against the children might be aspects to consider in the development of interventions and support for parents in MT and their children, as well as the role of the patients’ own parents.
Acknowledgment
We would like to thank CEPI, University of Lund, Sweden, for research grants for Heljä Pihkala.
Disclosure
The authors report no conflicts of interest in this work.
References
Connock M, Juarez-Garcia A, Jowett S, et al. Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation. Health Technol Assess. 2007;11(9):1–171. | |
De Maeyer J, Vanderplasschen W, Camfield L, Vanheule S, Sabbe B, Broekaert E. A good quality of life under the influence of methadone: a qualitative study among opiate-dependent individuals. Int J Nurs Stud. 2011;48(10):1244–1257. | |
Harris J, McElrath K. Methadone as social control: institutionalized stigma and the prospect of recovery. Qual Health Res. 2012;22(6):810–824. | |
Sarfi M, Smith L, Waal H, Sundet JM. Risks and realities: dyadic interaction between 6-month-old infants and their mothers in opioid maintenance treatment. Infant Behav Dev. 2011;34(4):578–589. | |
Skinner ML, Haggerty GP, Fleming CB, Catalano RF, Gainey RR. Opiate-addicted parents in methadone treatment: long-term recovery, health, and family relationships. J Addict Dis. 2011;30(1):17–26. | |
Sundelin Wahlsten V, Sarman I. Neurobehavioural development of preschool-age children born to addicted mothers given opiate maintenance treatment with buprenorphine during pregnancy. Acta Paediatr. 2013;102(5):544–549. | |
Wells KM. Substance abuse and child maltreatment. In: Brittain CR, editor. Understanding the Medical Diagnosis of Child Maltreatment: A Guide for Nonmedical Professionals. Oxford: Oxford University Press. 2006:179–189. | |
Gutwinski S, Bald LK, Gallinat J, Heinz A, Bermpohl F. Why do patients stay in opioid maintenance treatment? Subst Use Misuse. 2014;49(6):694–699. | |
Chandler A, Whittaker A, Cunningham-Burley S, Williams N, McGorm K, Mathews G. Substance, structure and stigma: parents in the UK accounting for opioid substitution therapy during the antenatal and postnatal periods. Int J Drug Policy. 2013;24(6):e35–e42. | |
Radcliffe P. Substance-misusing women: stigma in the maternity setting. Br J Midwifery. 2011;19(8):497–506. | |
Radcliffe P. Motherhood, pregnancy, and the negotiation of identity: the moral career of drug treatment. Soc Sci Med. 2011;72(6):984–991. | |
Rhodes T, Bernays S, Houmoller K. Parents who use drugs: accounting for damage and its limitation. Soc Sci Med. 2010;71(8):1489–1497. | |
Kvale S. InterViews: An Introduction to Qualitative Research Interviewing. 1st ed. Thousands Oaks, CA: Sage Publications; 1996. | |
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | |
Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358:483–488. | |
Link BG, Phelan JC, Bresnahan M, Stueve A, Pescosolido BA. Public conceptions of mental illness: labels, causes, dangerousness, and social distance. Am J Public Health. 1999;89(9):1328–1333. | |
Ostman M, Kjellin L. Stigma by association: psychological factors in relatives of people with mental illness. Br J Psychiatry. 2002;181: 494–498. | |
Hansson L, Stjernswärd S, Svensson B. Perceived and anticipated discrimination in people with mental illness – an interview study. Nord J Psychiatry. 2014;68(2):100–106. | |
Watson AC, Corrigan P, Larson JE, Sells M. Self-stigma in people with mental illness. Schizophr Bull. 2007;33(6):1312–1318. | |
Livingston JD, Milne T, Fang ML, Amari E. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction. 2011;107(1):39–50. | |
Beardslee WR, Wright EJ, Gladstone TR, Forbes P. Long-term effects from a randomized trial of two public health preventive interventions for parental depression. J Fam Psychol. 2007;21(4):703–713. | |
Solantaus T, Toikka S, Alasuutari M, Beardslee WR, Paavonen EJ. Safety, feasibility and family experiences of preventive interventions for children and families with parental depression. Int J Ment Health Promot. 2009;11(4):15–24. | |
Earnshaw V, Smith L, Copenhaver M. Drug addiction stigma in the context of methadone maintenance therapy: an investigation into understudied sources of stigma. Int J Ment Health Addict. 2013;11:110–122. | |
Worrall J. When grandparents take custody–changing intergenerational relationships: the New Zealand experience. J Intergener Relatsh. 2009;7(2–3):259–273. |
Supplementary material
 | Figure S1 Interview guide – parents in maintenance treatment. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.