Back to Archived Journals » Reports in Medical Imaging » Volume 7
Overview of 99mTc-anti-TNF-α scintigraphy: diagnostic applications
Authors Elboga U, Kalender E, Yalcin H
Received 2 October 2013
Accepted for publication 4 November 2013
Published 19 December 2013 Volume 2014:7 Pages 1—4
DOI https://doi.org/10.2147/RMI.S39098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Umut Elboga,1 Ebuzer Kalender,2 Hulya Yalcin2
1Department of Nuclear Medicine, Gaziantep University, Gaziantep, Turkey; 2Department of Nuclear Medicine, Mustafa Kemal University, Antioch, Turkey
Abstract: Tumor necrosis factor alpha (TNF-α) has a role in the pathogenesis of several inflammatory diseases such as rheumatoid arthritis, Crohn’s disease, and ulcerative colitis. As TNF-α plays a role in the pathogenesis of different inflammatory diseases, anti-TNF-α agents (monoclonal antibodies [mAbs]) such as infliximab, adalimumab, and certolizumab have been developed and investigated for the treatment of these conditions. In recent years, these mAbs also have been used for diagnosis, monitoring, follow-up of disease activity, and therapy decision-making for inflammatory diseases, especially rheumatoid arthritis, after labeling with 99mTc. However, 99mTc-anti-TNF-α imaging might have severe adverse effects and is expensive. In contrast, scintigraphic imaging before therapy with radiolabeled mAbs may be a cost-effective solution for therapy decisions.
Keywords: monoclonal antibodies, mAb, nuclear medicine, 99mTc tumor necrosis factor-α imaging
Introduction
Monoclonal antibody (mAb) targets are adhesion molecules, activation markers, antigens, or receptors. mAbs interact with some inflammation pathways at the molecular level. For diagnostic processes, mAbs can be labeled with radionuclides, using direct or indirect methods.
Anti-tumor necrosis factor alpha (TNF-α) antibodies such as infliximab, adalimumab, and certolizumab are used in the treatment of TNF-α-mediated inflammatory diseases.1 Infliximab, produced by a recombinant cell culture technique, has been approved by the US Food and Drug Administration for the treatment of moderate-to-severe active rheumatoid arthritis. Soluble and membrane-bound TNF-α are the targets of infliximab, which specifically binds to TNF-α.2 This complex inhibits the binding of TNF-α to its receptor, as well as inhibiting the biological activity of TNF-α.3 Infliximab does not have an effect on TNF-β (lymphotoxin α). The median terminal half-life of infliximab is 9.5 days.
TNF-α plays different roles: it induces some cytokines and acute-phase reactants; activates eosinophils and neutrophils; and enhances the endothelial layer permeability.4
Discussion
A study was performed by Conti et al in which they performed scintigraphy in a patient with arthritis to evaluate TNF-α-mediated inflammation degree in an affected knee.5 The researchers imaged the patient scintigraphically with infliximab before and 4 months after intraarticular therapy. Planar images of the inflamed joint were acquired at 6 and 24 hours after injection of 99mTc-infliximab. The researchers observed dense accumulation in the affected knee, and they determined that this accumulation was related to a high level of intralesional TNF-α. In the studies performed 4 months after intraarticular infliximab therapy, the authors evaluated the knee with disease and found no uptake in the inflamed joint. In addition, examination of the patients’ clinical features using clinical parameters, including erythrocyte sedimentation rate, C-reactive protein level, and visual analog scale, showed that complete remission was reached. Therefore, the researchers concluded that TNF-α scintigraphy could be a good guide in the evaluation and follow-up of intraarticular treatment.5
Another study was performed by Chianelli et al in rheumatoid arthritis, using scintigraphy with 99mTc-infliximab.6 Imaging with 99mTc-infliximab was performed before and 3 months after intraarticular infliximab therapy. In the follow-up imaging, radiopharmaceutical uptake of several amounts was seen in the affected joints. The authors concluded that inflamed joints demonstrated distinctive uptake compared with normal joints. They also emphasized that uptake in inflamed joints showed a correlation with clinical recovery and swelling reduction. They suggested that TNF-α scintigraphy might be important not only for evaluation of symptomatic joints but also for examining asymptomatic joint involvement.
D’Alessandria et al used 99mTc-infliximab scintigraphy in patients with Crohn’s disease.7 Their aim was to demonstrate the presence of TNF-α within the gut mucosa in patients with active Crohn’s disease. Ten patients with active Crohn’s disease refractory to conventional medical therapies were imaged 6 to 20 hours after intravenous injection of 10 mCi 99mTc-infliximab. One week after this imaging, the researchers performed a survey of 99mTc-hexamethylpropyleneamine-oxime-labeled autologous white blood cells. The authors found that 99mTc-infliximab uptake of the inflamed bowel was less than that of 99mTc-hexamethylpropyleneamine-oxime-labeled autologous white blood cells. However, when anti-TNF-α therapy was tried, there was a response to therapy in two of the patients, despite no uptake being seen in 99mTc-infliximab imaging. Thus, the authors concluded that the mechanism of anti-TNF-α therapy is related to peripheral blocking of TNF-α, rather than TNF-α downregulation in the bowel.7
Another 99mTc-anti-TNF-α mAb used in diagnosis and treatment is adalimumab. This antibody was approved by the US Food and Drug Administration in December 2002 as a therapeutic approach to rheumatoid arthritis and psoriatic arthritis. Labeling of adalimumab with 99mTc was done via indirect radiolabeling.8 Soluble and membrane-bound TNF-α are recognized by adalimulab.9 Adalimumab has fewer adverse effects than other antibodies.10
Barrera et al11 performed a study in patients with active rheumatoid arthritis. Their aim was to consider the susceptibility and biodistribution of radiolabeled adalimumab.11 They completed two scintigraphic imaging scans for each patient: one before treatment with 99mTc-adalimumab and another after treatment with nonradiolabeled anti-TNF-α mAb or an intramuscular injection of corticosteroid. The authors observed that same-time injection of nonradiolabeled TNF-α mAb reduced 99mTc-TNF-α mAB uptake by the joint. This retention demonstrated that the radiolabeled mAb target in arthritic joints is the TNF-α. In the group which received corticosteroids, the disease condition was reduced, which led to a decrease in uptake of the radiopharmaceutical. The authors concluded that 99mTc-adalimumab could be used to find clinical changes in disease progress and that this radiopharmaceutical is an advantage for specific evaluation of the inflamed joints.11
Malviya et al12 performed a study in patients with rheumatoid arthritis. Their aim was to conclude which radiopharmaceutical should be used for treatment and follow-up.12 They processed scintigraphic imaging with 99mTc-infliximab and 99mTc-adalimumab, respectively, in 12 and nine patients with active rheumatoid arthritis. Two imaging scans were done: one before and the second 3 months after local therapy with infliximab or systemic therapy with adalimumab. The authors found no differences in biodistribution between two radiopharmaceuticals. In addition, in two of the patients, the researchers performed 99mTc-human immunoglobulin (HIG) scintigraphy. In these two patients, the authors observed that although clinical response was seen, there was no decrease in the 99mTc-HIG uptake of the joints after the cold anti-TNF-α mAb treatment. In conclusion, the authors emphasized that for the evaluation of therapy, response in patients with active rheumatoid arthritis for unlabeled mAb 99mTc-TNF-α antibodies was superior to that for 99mTc-HIG scintigraphy.
In another study, performed in 2012 by Malviya et al, the researchers examined 20 patients with chronic inflammatory autoimmune disease. They imaged all patients with 99mTc rituximab before treatment with nonradioactive rituximab. The imaging was performed 6 and 20 hours after radiopharmaceutical treatment. The authors concluded that imaging with specifically labeled agents might be an advantage for cost-effectiveness and therapy evaluation in patients treated with biological agents.13
Finally, in a case published by Lopes et al,14 the authors emphasize that 99mTc-anti-TNF-α mAb could also be used in the diagnosis of Graves ophthalmopathy. For the diagnosis of Graves ophthalmopathy, different imaging methods can be used. However, 99mTc-anti-TNF-α scintigraphy could be a promising method for the diagnosis of active ocular disease. The researchers showed unilateral Graves ophthalmopathy by imaging with 99mTc-anti-TNF-α mAb because TNF-α is thought to be enrolled in the initial active phase of disease development.14 Thus, imaging with 99mTc-anti-TNF-α mAb might be the first step of new target-based modalities for the diagnosis and therapy of Graves ophthalmopathy (Table 1).14
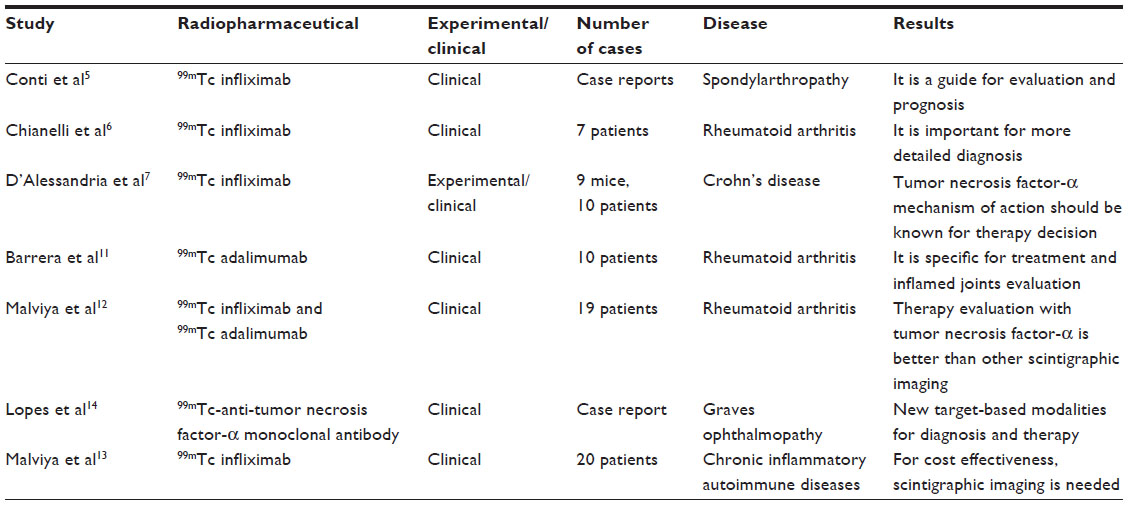 | Table 1 Summary of research performed with 99mTc-Anti-TNF-α scintigraphy |
Conclusion
All our research with mAbs guide us to the conclusion that more research should be carried out on the cost-effectiveness of 99mTc-anti-TNF-α mAb imaging.
Disclosure
The authors report no conflicts of interest in this work.
References
Tilg H, Moschen A, Kaser A. Mode of function of biological anti-TNF agents in the treatment of inflammatory bowel diseases. Expert Opin Biol Ther. 2007;7(7):1051–1059. | |
Knight DM, Trinh H, Le J, et al. Construction and initial characterization of a mouse-human chimeric anti-TNF antibody. Mol Immunol. 1993;30(16):1443–1453. | |
Scallon BJ, Moore MA, Trinh H, Knight DM, Ghrayeb J. Chimeric anti-TNF-alpha monoclonal antibody cA2 binds recombinant transmembrane TNF-alpha and activates immune effector functions. Cytokine. 1995;7(3):251–259. | |
Scott DL, Kingsley GH. Tumor necrosis factor inhibitors for rheumatoid arthritis. N Engl J Med. 2006;355(7):704–712. | |
Conti F, Priori R, Chimenti MS, et al. Successful treatment with intraarticular infliximab for resistant knee monarthritis in a patient with spondylarthropathy: a role for scintigraphy with 99mTc-infliximab. Arthritis Rheum. 2005;52(4):1224–1226. | |
Chianelli M, D’Alessandria C, Conti F, et al. New radiopharmaceuticals for imaging rheumatoid arthritis. Q J Nucl Med Mol Imaging. 2006;50(3):217–225. | |
D’Alessandria C, Malviya G, Viscido A, et al. Use of a 99mTc labeled anti-TNFalpha monoclonal antibody in Crohn’s disease: in vitro and in vivo studies. Q J Nucl Med Mol Imaging. 2007;51(4):334–342. | |
Abrams MJ, Juweid M, tenKate CI, et al. Technetium-99m-human polyclonal IgG radiolabeled via the hydrazino nicotinamide derivative for imaging focal sites of infection in rats. J Nucl Med. 1990;31(12):2022–2028. | |
Rau R. Adalimumab (a fully human anti-tumour necrosis factor alpha monoclonal antibody) in the treatment of active rheumatoid arthritis: the initial results of five trials. Ann Rheum Dis. 2002;61 Suppl 2:ii70–ii73. | |
European Medicines Agency. Humira: adalimumab. London: European Medicines Agency, 2013. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000481/human_med_000822.jsp&mid=WC0b01ac058001d124. Accessed November 26, 2013. | |
Barrera P, Oyen WJ, Boerman OC, van Riel PL. Scintigraphic detection of tumour necrosis factor in patients with rheumatoid arthritis. Ann Rheum Dis. 2003;62(9):825–828. | |
Malviya G, Conti F, Chianelli M, Scopinaro F, Dierckx RA, Signore A. Molecular imaging of rheumatoid arthritis by radiolabelled monoclonal antibodies: new imaging strategies to guide molecular therapies. Eur J Nucl Med Mol Imaging. 2010;37(2):386–398. | |
Malviya G, Anzola KL, Podestà E, et al. (99m)Tc-labeled rituximab for imaging B lymphocyte infiltration in inflammatory autoimmune disease patients. Mol Imaging Biol. 2012;14(5):637–646. | |
Lopes FP, de Souza SA, Dos Santos Teixeira Pde F, et al. 99mTc-Anti-TNF-α scintigraphy: a new perspective within different methods in the diagnostic approach of active Graves ophthalmopathy. Clin Nucl Med. 2012;37(11):1097–1101. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.