Back to Journals » Clinical Ophthalmology » Volume 12
Outcomes of undercorrection in surgical management and binocular vision gained of adult intermittent exotropia
Authors Lekskul A ![]() , Supakitvilekarn T, Padungkiatsagul T
, Supakitvilekarn T, Padungkiatsagul T ![]()
Received 19 May 2018
Accepted for publication 23 July 2018
Published 11 September 2018 Volume 2018:12 Pages 1763—1767
DOI https://doi.org/10.2147/OPTH.S174695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Apatsa Lekskul, Tatha Supakitvilekarn, Tanyatuth Padungkiatsagul
Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Purpose: To study the surgical outcomes of intended undercorrection on adult intermittent exotropia (X(T)) performed to avoid postopertively overcorrected diplopia.
Patients and methods: A retrospective chart review was conducted for adult patients (age ≥18 years) with X(T) ≥15 prism diopter (PD) who underwent strabismus surgery by a single surgeon. Inclusion criteria were 1) corrected VA ≥20/40 in either eye; 2) monocular occlusion at least 30 minutes before deviation measurement; 3) difference of ≤10 PD between near and distance deviation; 4) absence of significant A or V pattern or vertical deviation; 5) lateral rectus recession and medial rectus resection procedure were performed unilaterally; and 6) intended surgical number for deviation correction was aimed at 5 PD undercorrection.
Results: Of 234 patients who met the inclusion criteria, 122 were women (52.14%). Average age at the time of surgery was 27.56 years (range, 18–42 years). A total number of 197 patients (84.19%) had postoperative exodeviation under 10 PD. Twenty five (10.68%) and 12 patients (5.13%) had postoperative exodeviation within 10–15 PD and >15 PD, respectively. All patients who had postoperative exodeviation >15 PD exhibited initial deviation of ≥40 PD and had undergone re-operation. In 74 patients (46.25%) out of 160 who had no binocular vision in orthoptic examination before surgery, fusion or stereopsis was gained after good alignment. No postoperative diplopia was found in this study.
Conclusion: Intended undercorrection in surgical management of adult X(T) showed good functional and cosmetic outcomes. No procedure resulted in consecutive esodeviation or persistent diplopia. Fusion or stereopsis could be gained after successful surgical alignment. Our recommendations are as follows: 5 PD undercorrection if deviation is <40 PD and regular correction if deviation is ≥40 PD.
Keywords: diplopia, intermittent exotropia, stereopsis, fusion, recession, resection
Introduction
Strabismus, a condition in which the eyes are misaligned, has an estimated prevalence of 1%–3%.1 Exodeviations are more frequent in females than males and have a higher prevalence in sunnier lattitudes,2 comprising approximately 25% of the cases of strabismus in the Western world and 72% in Asia.3 Intermittent exotropia (X(T)) is the most common form of childhood exotropia. Although, the characteristics of X(T) include better maintained ocular alignment and superior binocular sensory function, the eyes may adopt a divergent alignment with an accompanying loss of stereopsis when in states of tiredness, inattention or distance fixation.4 Exuberant convergence in childhood can mask exotropia. As convergence weakens with age, an increasingly divergent position of the eyes manifests,5 which eventually becomes constantly divergent with loss of stereopsis. For this reason, most of the patients with X(T) are asymptomatic until exodeviation becomes increasingly evident; then, symptoms of headache, asthenopia or unsatisfactory cosmesis may develop. Despite incongruities among ophthalmologists in management of X(T), treatment typically involves surgical correction to improve ocular alignment and binocular sensory function. A highly variable success rate has been reported in published literature, ranging from 61%–92%.6–11
Postoperative diplopia may vary among age groups although it can stimulate development of fusional vergences and stabilize postoperative alignment.12 In adults, diplopia follows overcorrected strabismus surgery – even slightly – and tends to persist because the adult nervous system is not relatively plastic as it is in children; in contrast, children have the ability to suppress diplopia.13 This study was undertaken to measure outcomes of intended undercorrection to avoid postoperative overcorrected diplopia in surgical management of adult X(T).
Patients and methods
Approval for this study was obtained from the Institutional Review Board (IRB) of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, and was conducted according to the tenets of the Declaration of Helsinki. Patients’ consent to review their medical records was not required by the IRB because of the retrospective nature of the study and because the medical records are stored such that the patients cannot be identified by the research team; moreover, the authors had routine access to this information by virtue of his/her patient care responsibilities. A retrospective chart review of adult patients age ≥18 years with X(T) ≥15 PD who underwent strabismus surgery at Ramathibodi Hospital between January 2002 and January 2017 was conducted. The inclusion criteria were 1) corrected VA ≥20/40 in either eye; 2) monocular occlusion at least 30 minutes before deviation measurement; 3) difference of ≤10 PD between near and distance deviation; 4) absence of significant A or V pattern or vertical deviation; 5) lateral rectus (LR) recession and medial rectus (MR) resection procedure were performed unilaterally; and 6) intended surgical deviation was 5 PD undercorrection. A total number of 234 patients met these criteria; all underwent preoperative slit lamp biomicroscopy, refraction, fundus examination and orthoptic measurement. Total manifest exodeviation, combining exotropia and exophoria, was measured after patching one eye of the patient for at least 30 minutes to break fusional convergence. Refractive error was corrected with glasses or contact lenses at the time of deviation measurement. Near deviation was measured immediately after the eye patch was removed; it was followed by distance deviation, using the prism and alternate cover test technique, which measures both exophoria and exotropia for overall deviation (Figure 1). Intended surgical undercorrection was 5 PD for distance deviation angle. This intended undercorrection protocol was followed regularly for adult X(T) correction at Ramathibodi Hospital to avoid postoperative overcorrected diplopia. All subjects underwent LR recession and MR resection procedures unilaterally by a single pediatric and strabismus ophthalmologist (AL).
 | Figure 1 Adult intermittent exotropia, pre and postoperative examination. |
Ethics approval and consent to participate
Approval for this study was obtained from the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, and was conducted according to the tenets of the Declaration of Helsinki. A waiver of patient consent was given by the IRB because of the retrospective nature of the study.
Results
Of 234 patients with X(T) who met the inclusion criteria, 122 were women (52.14%) and 112 were men (47.86%). Mean age at the time of surgery was 27.56 years (range, 18–42 years) (Table 1). Mean follow-up duration was 42.84 months (range, 6–87 months).
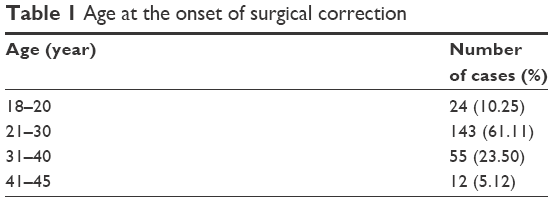 | Table 1 Age at the onset of surgical correction |
The majority of patients had preoperative total exodeviation of ≤30 PD (range, 15–45 PD) (Table 2).
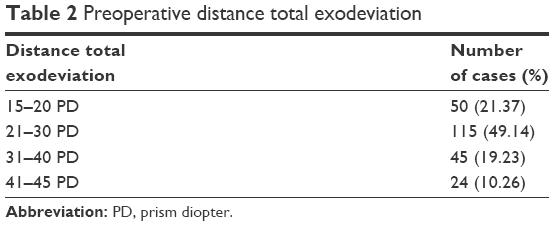 | Table 2 Preoperative distance total exodeviation |
Postoperative orthoptic measurements revealed that 197 patients (84.19%) had successful surgical alignment, with total exodeviation <10 PD. 25 patients (10.68%) and 12 patients (5.13%) had postoperative exodeviation within 10–15 PD and >15 PD, respectively. No procedures resulted in overcorrection (Table 3). Regarding patients with postoperative exodeviation within 15 PD, all had satisfactory cosmesis and relief from symptoms, including headache and asthenopia. However, all patients who had postoperative exodeviation >15 PD had initial deviation of ≥40 PD; re-operation was required in all cases.
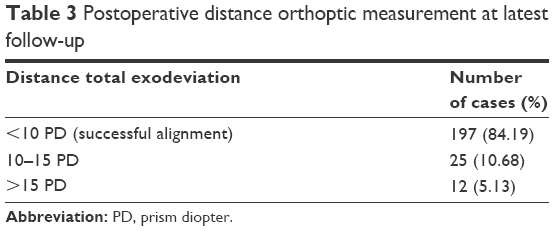 | Table 3 Postoperative distance orthoptic measurement at latest follow-up |
Regarding sensory binocular vision, no binocular vision, fusion and stereopsis were respectively measured in 160 (68.38%), 42 (17.95%) and 32 (13.67%) patients during preoperative examination and in 86 (36.75%), 72 (30.77%) and 76 (32.48%) patients during postoperative examination (Table 4). Postoperative binocular vision gain was reported in 92 patients (45.54%). Nearly half of the patients who had no binocular vision preoperatively, ie, 74 of 160 patients, gained fusion or stereopsis. Eighteen (42.86%) of 42 patients with preoperative fusion demonstrated improved binocular vision to stereopsis after good alignment.
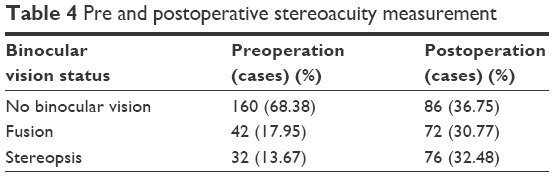 | Table 4 Pre and postoperative stereoacuity measurement |
Discussion
Initial overcorrection is an accepted protocol worldwide for desirable long-term surgical outcomes in X(T).6,7 However, studies reporting desirable surgical outcomes with initial overcorrection protocol primarily include children as subjects; notably, cases of exotropia in children greatly differ from those in adults. When early postoperative esotropia occurs in children, they typically prevent diplopia by suppression of the deviating eye. In contrast, most of adult patients with postoperative esotropia – even small deviations – typically experience persistent postoperative diplopia. Re-operation is often required to correct this consecutive esotropia. In this study, we aimed to avoid postoperative diplopia in adult X(T) by slight initial surgical undercorrection.
This study reviewed 234 cases series of adult X(T) that were operated by a single surgeon, with an average follow up time of 42.84 months. Unilateral LR recession and MR resection were performed with 5 PD initial undercorrection in all cases. Binocularity was measured by amblyoscope and was defined as no binocular vision, fusion, and stereopsis. The criterion for successful surgical alignment is defined as an alignment with objective motor deviation <10 PD.
In our study, surgical management of adult X(T) by slightly intended undercorrection showed promising outcomes. We demonstrated that 197 patients (84.19%) had successful surgical alignment, resulting in postoperative exodeviation <10 PD. Only 12 patients (5.12%) had postoperative exodeviation >15 PD, requiring reoperation. No consecutive esotropia or postoperative diplopia was found in this study. Jung et al14 reported 39 adults with X(T) who underwent LR recession and MR resection with initial overcorrection <10 PD. Although 28 patients (72%) achieved surgical success and only four (10%) had recurrence, seven (18%) exhibited overcorrection, 64% continued to show consecutive esotropia at the final follow-up. Their result suggests that exodrift in adults differs from that in children, and that overcorrection of >10 PD affects the incidence of consecutive esotropia. In our study, no patient experienced consecutive esotropia fulfilling our goal of avoiding this sequelae.
Other studies have reported lower success rate than our series: Ruttum: 63%,6 Kushner: 64%,8 Flax and Selenow: 61.8%,9 and Pineles et al: 64%.10 Several reasons could explain these differences. First, the inclusion of children as subjects in those studies may have contributed to increased postoperative recurrence of manifested exodeviation due to age-related deterioration in the fusional convergence mechanism. Moreover, Kushner reported a lower success rate of bilateral LR recession, which was a preferred procedure for children in those studies, compared with combined MR resection with LR recession procedures because of the tethering effect from MR resection.15 An additional factor that may have contributed to satisfactory outcomes in our study was preoperative orthoptic measurement with monocular occlusion for at least 30 minutes to manifest total exodeviation, including both exophoria and exotropia (Figure 1). Because we aimed our surgical correction at distance total exodeviation – the largest deviation in basic X(T) – none of our patients had residual exotropia, but some postoperative exophoria was measured. These reasons contributed to successful surgical alignment and improved binocular vision.
Of 234 patients, 25 (10.16%) had postoperative exodeviation within 10–15 PD. They all had satisfactory cosmesis and relieved symptoms. Twelve patients (5.13%) had postoperative exodeviation >15 PD; re-operation was required in all 12 because of unsatisfactory cosmesis. These patients had preoperative deviation ≥40 PD.
Patients with X(T) who had successful surgical alignment postoperatively could gain binocular vision, such as fusion or stereopsis, even though some were as old as 42 years. The primary reason might have been good alignment of the eyes in early infancy, when critical binocular cortical connections are established and deviation is intermittent, allowing fusion to be developed. Our study showed favorable results in recovery of binocularity in 92 patients (45.54%). Recovery of binocularity was varied in previous studies.16–18 Nonetheless, there was evidence of a persistent imbalance between the two eyes after successful surgical alignment with normal stereoacuity. Quantitative assessment of the binocular vision using binocular phase paradigm demonstrated significant interocular imbalance compared with control subjects.
Although carefully designed, there are several limitations to our study. First, our study is limited by its retrospective design, which includes missing data, selection bias and inaccurate data recording. Second, the minimal follow-up period of 6 months is considerably short compared with other long-term studies.10 This short follow-up period may lead our study to overestimate the successful surgical alignment. Additionally, our interpretation of sensory outcome was limited by non-quantified measurement and did not include the distance stereoacuity measurement. Finally, comparisons with other studies are restricted by the surgical technique and variable definition of success.
Conclusion
In summary, intended undercorrection as surgical management of adult X(T) showed good functional and cosmetic outcomes. There was no consecutive esodeviation, which tends to result in postoperative persistent diplopia. Our recommendations from this study are as follows: 5 PD undercorrection if deviation is <40 PD, and regular correction if deviation is ≥40 PD.
Acknowledgments
We thank Ryan Chastain-Gross, Ph.D., from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Author contributions
All authors made substantial contributions to the conception (AL, TS, and TP) or design (AL, TS, and TP) of the work or the acquisition (AL, TS), analysis (AL, TS and TP), or interpretation (AL, TS, and TP) of data. AL, TS and TP drafted the manuscript and revised it critically. AL, TS, and TP provided final approval for submission. AL, TS, and TP are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
Donnelly UM, Stewart NM, Hollinger M. Prevalence and outcomes of childhood visual disorders. Ophthalmic Epidemiol. 2005;12(4):243–250. | ||
Jenkins RH. Demographics: Geographic Variations in the Prevalence and Management of Exotropia. Am Orthopt J. 1992;42(1):82–87. | ||
Govindan M, Mohney B, Diehl N, et al. Incidence and types of childhood exotropia. Ophthalmology. 2005;112:104–108. | ||
Clarke MP. Intermittent exotropia. J Pediatr Ophthalmol Strabismus. 2007;44(3):153–157. | ||
Burian HM, Spivey BE. THE SURGICAL MANAGEMENT OF EXODEVIATIONS. Am J Ophthalmol. 1965;59:603–620. | ||
Ruttum MS. Initial versus subsequent postoperative motor alignment in intermittent exotropia. J Aapos. 1997;1(2):88–91. | ||
Scott WE, Keech R, Mash AJ. The postoperative results and stability of exodeviations. Arch Ophthalmol. 1981;99(10):1814–1818. | ||
Kushner BJ. Exotropic Deviations: A Functional Classification and Approach to Treatment. Am Orthopt J. 1988;38(1):81–93. | ||
Flax N, Selenow A. Results of surgical treatment of intermittent divergent strabismus. Am J Optom Physiol Opt. 1985;62(2):100–104. | ||
Pineles SL, Ela-Dalman N, Zvansky AG, Yu F, Rosenbaum AL. Long-term results of the surgical management of intermittent exotropia. J Aapos. 2010;14(4):298–304. | ||
Kh K, Min BM. Factors related to surgical results of intermittent exotropia. J Korean Ophthalmol Soc. 1996;37:179–184. | ||
Von Noorden GK. Exodeviations. In: Von Noorden GK, Campos E, editors. Binocular Vision and Ocular Motility: Theory and Management of Strabismus. 6th ed. St. Louis; Sydney: Mosby; 2002:356–372. | ||
Posner A, Schlossman A. Relation of diplopia to binocular vision in concomitant strabismus. AMA Arch Ophthalmol. 1951;45(6):615–622. | ||
Jung EH, Kim SJ, Yu YS, Ys Y. Factors associated with surgical success in adult patients with exotropia. J Aapos. 2016;20(6):511–514. | ||
Kushner BJ. Selective surgery for intermittent exotropia based on distance/near differences. Arch Ophthalmol. 1998;116(3):324–328. | ||
Lal G, Holmes JM. Postoperative stereoacuity following realignment for chronic acquired strabismus in adults. J Aapos. 2002;6(4):233–237. | ||
Fawcett SL, Felius J, Stager DR. Predictive factors underlying the restoration of macular binocular vision in adults with acquired strabismus. J Aapos. 2004;8(5):439–444. | ||
Fatima T, Amitava AK, Siddiqui S, Ashraf M. Gains beyond cosmesis: Recovery of fusion and stereopsis in adults with longstanding strabismus following successful surgical realignment. Indian J Ophthalmol. 2009;57(2):141–143. | ||
Feng L, Zhou J, Chen L, Hess RF. Sensory eye balance in surgically corrected intermittent exotropes with normal stereopsis. Sci Rep. 2015;5:13075. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.