Back to Journals » Clinical Ophthalmology » Volume 14
Outcomes of Extraocular Muscle Surgery for Diplopia or Abnormal Head Posture After Treatment of Brain Disease
Authors Nishiguchi F ![]() , Kimura A
, Kimura A ![]() , Okamoto M, Okita Y, Gomi F
, Okamoto M, Okita Y, Gomi F ![]()
Received 18 May 2020
Accepted for publication 8 July 2020
Published 27 July 2020 Volume 2020:14 Pages 2151—2157
DOI https://doi.org/10.2147/OPTH.S263256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fumi Nishiguchi,1,2 Akiko Kimura,1 Mana Okamoto,1 Yoichi Okita,1 Fumi Gomi1
1Department of Ophthalmology, Hyogo College of Medicine, Nishinomiya, Hyogo, Japan; 2Nishiguchi Eye Clinic, Kobe, Hyogo, Japan
Correspondence: Akiko Kimura
Department of Ophthalmology, Hyogo College of Medicine, 1-1 Mukogawa-Cho, Nishinomiya, Hyogo, Japan
Tel +81 798 45 6462
Fax +81 798 45 6464
Email [email protected]
Purpose: To report the characteristics and outcomes of extraocular muscle (EOM) surgery for diplopia and abnormal head posture (AHP) after treatment of severe brain diseases such as brain tumor, severe cerebral bleeding and cerebral infarction.
Patients and Methods: Sixty-four patients (mean age 53.7 ± 16.0 years) who underwent EOM surgery to eliminate diplopia or AHP after treatment for brain disease at Hyogo College of Medicine Hospital from March 2006 through February 2018 were included. We divided the patients into two groups: a severe cerebrovascular disorder (SCVD) group and a brain tumor (BT) group. Backgrounds, surgical outcomes and satisfaction with treatment outcomes were examined retrospectively and compared between the two groups. The NEI-VFQ 25, Japanese version, was used to quantify postoperative satisfaction.
Results: There were 26 patients in the SCVD group and 38 patients in the BT group. The average age for the BT group was significantly younger than that for the SCVD group (P = 0.0236). The period from the onset of diplopia to EOM surgery was approximately 4 years for both groups. Abducens palsy was the most frequent disturbance (27% in the SCVD group and 52.6% in the BT group), and the numbers of operations were similar between the 2 groups (1.3 ± 0.7 and 1.3 ± 0.5 operations, respectively). In total, diplopia was eliminated in 82.8% of cases and AHP improved in 81.6% of cases. The BT group scored significantly higher than the SCVD group on 8 out of the 11 items on the VFQ 25.
Conclusion: EOM surgery was effective in eliminating diplopia and AHP. Therefore, we recommend that these patients visit an ophthalmologist as soon as possible and undergo EOM surgery.
Keywords: diplopia, abnormal head posture, strabismus surgery, brain disease, VFQ 25
Introduction
Visual impairment following severe brain disease such as brain tumor, bleeding or infarction may induce abnormalities of central and/or peripheral vision or ocular motility, and a variety of visual perception problems such as cognitive disorder and agnosia.1 These visual impairments can be complex, including ocular as well as cortical damage. Diplopia and abnormal head posture (AHP) are typical ocular complications in patients after severe brain disease, and include not only ocular motor nerve palsy but also central ocular motility disorders such as skew deviation, and vertical or horizontal gaze palsy.2,3 Hence, these ocular complications are generally considered to be refractory and tend to be left untreated.
As most patients suffer severe general complications such as disordered cognition, weakness, bowel/bladder dysfunction or hemiplegia,1,2,4,5 those complications are accorded priority for treatment and/or rehabilitation. Therefore, in patients with brain disease, ophthalmologic consultation tends to be delayed, even though visual system impairments including diplopia and AHP greatly reduce patients’ quality of life (QOL).
At our hospital, we have undertaken extraocular muscle (EOM) surgery to eliminate diplopia or AHP in these refractory patients after treatment for severe brain disease. Here, we report the characteristics and treatment outcomes for patients with diplopia and AHP after treatment of brain disease.
Patients and Methods
We conducted a retrospective, observational single-center study of patients who were seen in our Department of Ophthalmology, at Hyogo College of Medicine Hospital from March 2006 through February 2018. Inclusion criteria for the patients were as follows: strabismus caused by either severe cerebral vascular disease (SCVD), such as brainstem hemorrhage, subarachnoid hemorrhage, thalamic hemorrhage or brain infarction, or by a brain tumor (BT); stable strabismus deviation for more than 6 months; and first-time strabismus surgery. We focused on severe brain disease in this study; therefore, patients with ocular motor nerve palsy due to a microcirculatory disorder were excluded.
Ocular alignment was measured with the alternative prism cover test (APCT) for distance in the primary position, vertical deviation was measured by Hess red-green test, and cyclotorsion was measured by synoptophore with a cross slide for the primary position. Horizontal ocular motility disturbance was judged as severe if it did not move beyond the midline, and mild if it did. Vertical ocular motility disturbance was judged to be severe if it did not move beyond the line connecting inner and outer canthus, and mild if it did. AHP was measured with the prism adaptation test, in which AHP was eliminated.
Surgical treatment was performed on admission and, in cases in which diplopia remained after initial surgery, we performed adjustment surgery under topical anesthesia to eliminate the diplopia or AHP, and then discharged the patient. After discharge, if the diplopia or AHP recurred and further surgical treatment was needed, we performed a second surgery. When ocular movement was severely limited, muscle transposition procedures were performed. Surgical success was defined as the elimination of diplopia in the primary position or achievement of head posture within 5 degrees in the primary position, judged at 1 month after the patient’s first surgery. We documented the backgrounds of the patients, the surgical procedures, numbers of operations, surgical results and the results of a satisfaction survey for the SCVD and BT groups. The component 11 (Comp11) of the 25-Item National Eye Institute Visual Functioning Questionnaire (NEI-VFQ 25) Japanese version6,7 was used to quantify postoperative satisfaction. The Comp11 includes general vision, ocular pain, near vision, distant vision, social functioning, mental health, role limitations, dependency, driving, color vision and peripheral vision. Each item is scored from 0 to 100 points (the higher the score, the higher the satisfaction).
We mailed the NEI-VFQ 25 questionnaire and an informed consent form to all patients from December 2016 to March 2018 and analyzed the replies that were returned with a signed consent form. This study was approved by the Institutional Review Board of Hyogo College of Medicine Hospital.
All statistical analyses were performed by JMP software (Version pro 13, SAS, Cary, NC). Data were expressed as means ± standard deviations. The t-test, Kruskal–Wallis test, Tukey-Kramer test, and Wilcoxon signed-rank test were used for the statistical analyses, and p <0.05 was considered significant.
Results
Demographics of the Patients
Sixty-four patients who underwent EOM surgery to eliminate diplopia or AHP due to ocular motility disturbances after treatment of brain disease were enrolled (25 males, 39 females). The average age of patients at the time of their first EOM surgery was 53.6 ± 15.9 years (range: 11 to 85 years) and the average follow-up period was 19.3 ± 25.6 months.
The SCVD group included 26 patients (14 male and 12 female), and the average age was 58.6 ± 13.7 years (23 to 85 years), whereas the BT group included 38 patients (11 male and 27 female), and the average age was 50.1 ± 16.6 years (11 to 82 years). The average age for the BT group was significantly younger than that for the SCVD group (Mann–Whitney U-test, P = 0.0236).
The types of ocular motility disturbances are shown in Table 1. Ocular motor nerve palsy was the most common in both groups, accounting for 47 cases (73.4%) in total. Among the types of ocular motor nerve palsy, about half of the BT group showed abducens palsy (20 cases, 52.6%). In the SCVD group, abducens palsy was the most frequent (7 cases, 27.0%), but the percentage was almost the same as those for oculomotor palsy (5 cases, 19.2%), trochlear palsy (4 cases, 15.4%), compound ocular motor palsy (4 cases, 15.4%) and central ocular motility disorder (6 cases, 23.1%).
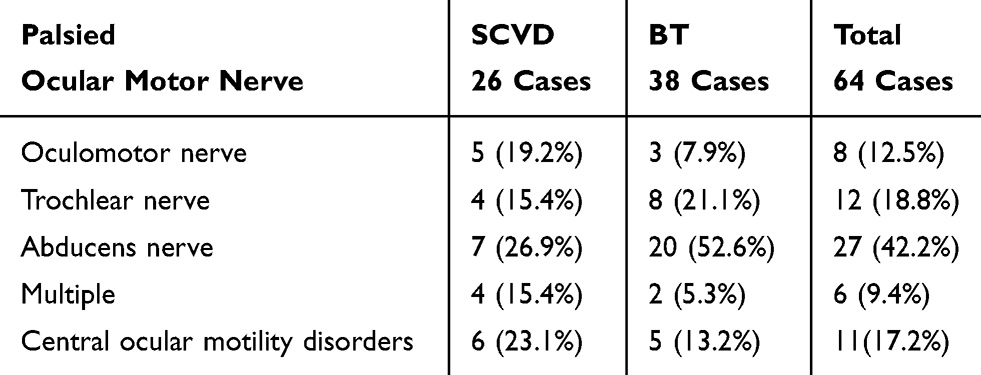 |
Table 1 Types of Ocular Motility Disturbance |
Overall, the period from the onset of diplopia or AHP to EOM surgery averaged 47.1 ± 64.4 months. The average was 45.8 ± 69.3 months (6 to 286 months) for the SCVD group and 48.0 ± 61.4 months (4 to 246 months) for the BT group. There was no significant difference between the two groups (Kruskal–Wallis test, P = 0.3869).
Surgical Procedures to Correct Strabismus Secondary to a SCVD or BT (Table 2)
Vertical muscle transposition for abducens palsy without tenotomy and muscle splitting (Nishida procedure)8 was performed in 17 cases (53.1%) out of the 32 with abducens palsy in horizontal deviation. In the other cases of horizontal deviation, recession and/or resection of the medial rectus muscle (MR) and the lateral rectus muscle (LR) were performed. Vertical transposition of the MR and LR to the position adjacent to the superior rectus muscle (SR) insertion following the spiral of Tillaux (Knapp procedure)9,10 was performed in three cases (33.3%) out of the nine cases with severe vertical deviation, and in the other cases of vertical deviation, recession and/or resection of the inferior rectus muscle (IR) and the SR were performed. Twenty-three cases (36.0%) were accompanied by cyclotorsion, and horizontal transposition of the SR or IR was performed in 16 cases (69.6%) out of the 23. General anesthesia was applied for patients who were to undergo a muscle transposition procedure or surgery for three or more muscles, but local anesthesia (sub-Tenon anesthesia) was used in other cases.
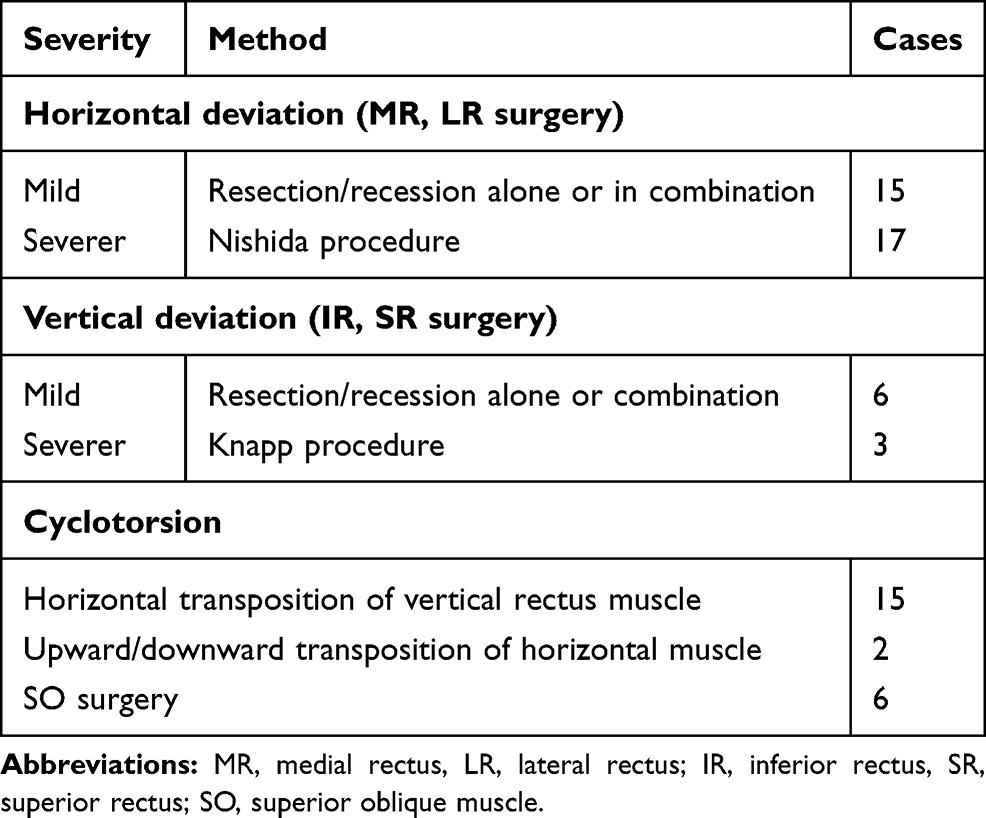 |
Table 2 Surgical Procedures |
Numbers of Operations
The mean number of operations was 1.3 ± 0.7 for the SCVD group and 1.3 ± 0.5 for the BT group. Adjustment surgery was performed for 38.5% of the patients in the SCVD group and 36.8% of those in the BT group, and reoperation was performed in 8 cases (30.8%) and 10 cases (26.3%), respectively. There were no significant differences between the two groups in terms of the numbers of operations, numbers of adjustment surgeries or the reoperation rates (Kruskal–Wallis test, P = 0.887; chi-square test, P = 0.896; chi-square test, P = 0.697).
Surgical results
In ocular alignment, preoperative exotropia improved 27.5±29.3PD to 8.5±10.3PD, preoperative esotropia improved 33.7±31.0PD to 6.7±10.1PD by APCT after surgery, vertical deviation from 7.6±6.9°to 3.9±4.4°by the Hess red-green test, and cyclotorsion improved 7.0±6.4°to 4.3±4.7°by synoptophore after surgery. The ocular alignment before and after surgery in SCVD group and BT group is shown in Table 3.
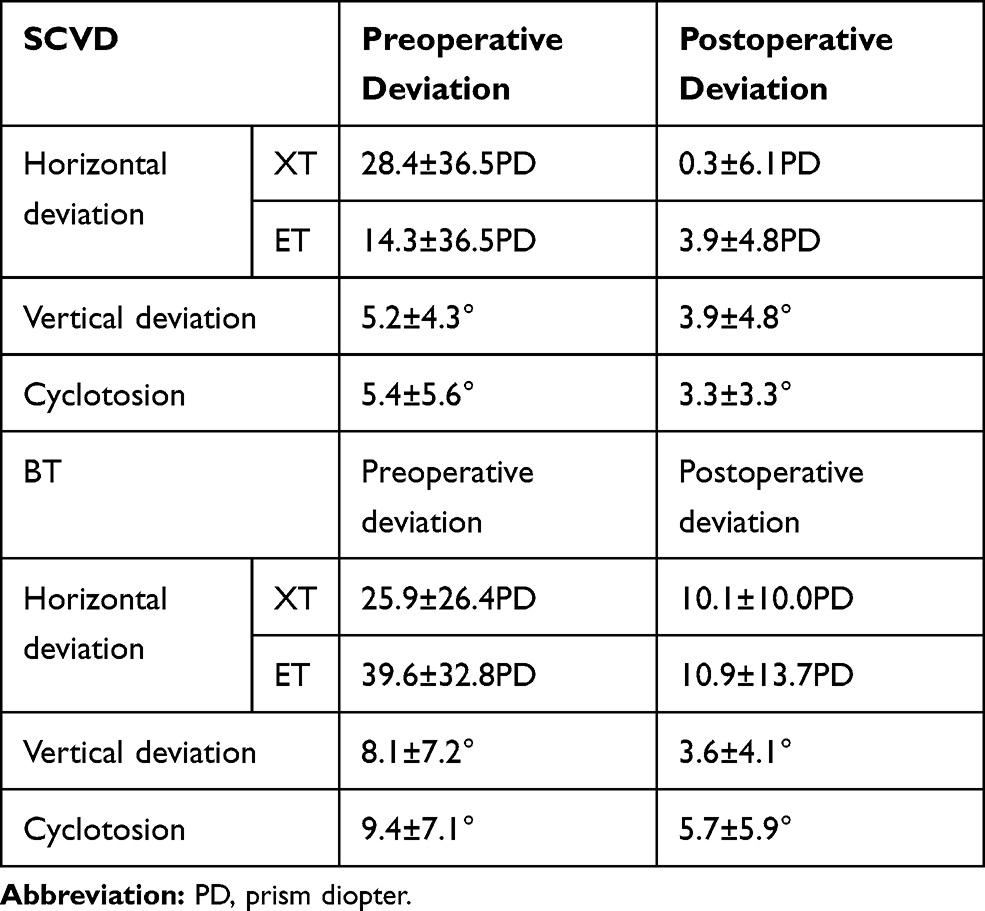 |
Table 3 Ocular Alignment Before and After Surgery |
Sixty of 64 patients (93.8%) complained of diplopia before EOM surgery, and the diplopia was eliminated by surgery, with or without prism therapy, in 50 of those cases (83.3%). Among the 25 patients with diplopia in the SCVD group before surgery, diplopia was eliminated in 12 cases (46.2%) by surgery alone and in 8 cases (30.8%) by surgery with prism therapy, for an elimination rate of 76.9% in the SCVD group. Of the 35 patients with diplopia in the BT group before surgery, diplopia was eliminated in 26 cases (74.3%) by surgery alone and in 4 cases (11.4%) by surgery with prism therapy, for an elimination rate of 85.7% in the BT group. There was no significant difference between the two groups in the rate of resolution of diplopia after surgery alone (46.2% versus 74.3%) or surgery with prism therapy (76.9% vs 85.7%) (chi-square test, P = 0.0749 and P = 0.8474, respectively). Of the 10 patients in whom diplopia remained after EOM surgery, ocular alignment was excellent in 3 cases of abducens palsy and 2 cases of central ocular motility disorders, with the patients showing less than 10 prism diopters (PD) base-in by APCT. The elimination rates for diplopia in each type of ocular motility disturbance are shown in Figure 1. For trochlear nerve palsy, the elimination rate was 100%, whereas the rate tended to be low for oculomotor nerve palsy (66.7%) and for central ocular motility disorders (66.7%).
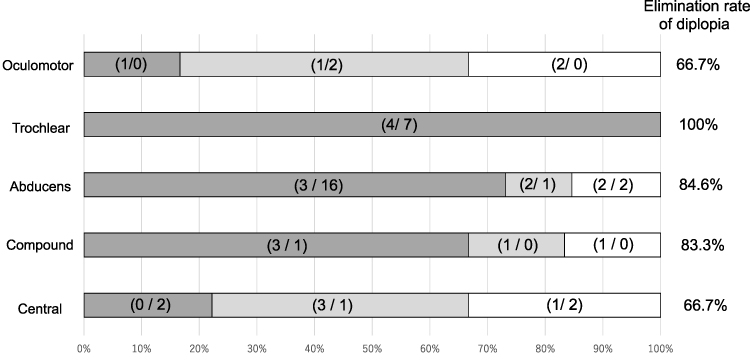 |
Figure 1 Rates at which diplopia was eliminated among different types of ocular motility disturbances. The bracketed numbers in each block indicate the number of patients in the severe cerebrovascular disorder (SCVD) group and the number in the brain tumor (BT) group (ie, SCVD/BT). The blocks of different shades illustrate the numbers of patients with the different disturbances for whom diplopia was eliminated by surgery alone or by surgery + prism therapy, and the numbers for whom diplopia remained. As listed on the left side of the figure, the types of motility disturbance were: Oculomotor = oculomotor nerve palsy; Trochlear = trochlear nerve palsy; Abducens = abducens nerve palsy; Compound = compound ocular motor palsy; and Central = central ocular motility disorders. |
AHP was observed in 38 cases (55.9%) overall and was eliminated in 31 cases (81.6%) through surgery with or without prism therapy. In the SCVD group, of 16 cases showing AHP preoperatively, this condition was improved in 13 cases (81.0%) by surgery alone, whereas of 22 cases in the BT groups showing AHP preoperatively, it was improved in 18 cases (81.8%): 14 cases (63.6%) by surgery alone and 4 cases (18.2%) by surgery with prism therapy. There was no significant difference between the two groups in the success rates for surgery alone (81.0% versus 63.6%) or surgery with prism therapy (81.0% versus 81.8%) (chi-square test, P= 0.2952, P = 0.8361).
Results of Satisfaction Survey
The return rate for the NEI-VFQ 25 questionnaire was 36 out of 64 (56.3%): 18 (69.2%) of 26 cases in the SCVD group and 18 (47.3%) of 38 cases in the BT group. In the comparison between groups, the scores for 8 out of 11 components were significantly higher for the BT group, but the total score was not significantly different between the two groups (SCVD = 69.7± 20.7, BT = 80.7 ± 15.2, P = 0.1675). The subscales that were significantly different between the groups were: near vision (SCVD = 49.8 ± 25.6, BT = 71.9 ± 26.3, Mann–Whitney U-test, P = 0.0165), distance vision (59.2 ± 16.6, 77.9 ± 16.8, P = 0.0023), social functioning (65.6 ± 22.9, 78.7 ± 17.0, P = 0.0347), mental health (47.1 ± 27.0, 68.4 ± 30.2, P = 0.0191), role limitations (49.4 ± 25.2, 75.0 ± 23.8, P = 0.0030), dependency (59.6 ± 27.7, 82.8 ± 24.0, P = 0.0053), color vision (68.1 ± 28.2, 89.1 ± 15.7, P = 0.0129) and peripheral vision (50.0 ± 18.6, 66.2 ± 24.9, P = 0.030)
Discussion
It is well known that most patients with isolated ocular motor nerve palsy (palsy of the oculomotor, trochlear or abducens cranial nerves) due to microvascular causes recover spontaneously within 6 months.11–13 In this study, as we focused on patients after treatment of severe brain disease with ocular complications such as diplopia or AHP, microvascular causes were excluded. Recently, advances in medical treatment have increased the survival rates for patients with severe brain disease, and a prospective, multicenter, observational case–cohort study, conducted by Rowe et al14 reported that 16.5% of post-stroke patients had ocular misalignment with diplopia. Therefore, treatment for diplopia and AHP, as well as general complications such as hemiparesis, should be demanded, to improve QOL. However, although surgical and conservative treatments were effective in eliminating diplopia and AHP in approximately 80% of patients, long periods (more than 4 years on average in this study) elapsed before EOM surgery in both groups (45.8 months for the SCVD group and 50.9 months for the BT group); therefore, we strongly believe that these patients should visit an ophthalmologist much sooner after their treatment for brain disease. Furthermore, eye-movement training for saccades and pursuit eye movements, and convergence insufficiency15,16 may be more effective after treatment for diplopia and AHP, because diplopia remained in 10 cases including oculomotor palsy and central ocular motility disorders; of those, 5 showed successful ocular alignment of less than 10 PD by APCT. In such cases, prism therapy was also unable to eliminate diplopia. We think that the remaining diplopia was closely related to the deterioration of fusion and/or accommodation, and perhaps to impaired visual-integration processing due to the brain damage.17
In previous reports,12,18 abducens palsy was the most frequent cause of acquired paralytic strabismus among adults, and abducens palsy was also the most frequent strabismus after severe brain disease in our study, reaching 53% in the BT group. A study of 81 cases by Peragallo et al19 demonstrated that patients with traumatic or neoplastic causes had a higher rate of complete abducens palsy, in comparison to other etiologies (58% versus 24%, respectively), and required more surgical procedures to achieve a successful outcome (48%). In this study, complete abducens palsy accounted for 53% of patients with abducens palsy who underwent muscle transposition, and, furthermore, severe vertical deviation was found in 33% and cyclotorsion was found in 36%, suggesting that strabismus after severe brain disease might be refractory. Nevertheless, the average number of operations (1.3) is not considered to be a high risk for reoperation, compared with other forms of incomitant strabismus.9,10
The success rate for Peragallo et al19 was 58% by surgery alone, but they did not use prism therapy. In an earlier report20 on abducens palsy, the surgical success rate was 52%, but when that same study allowed the use of prisms or small face turns to correct diplopia, the success rate reached 75%. We also believe that the surgical approach is effective in eliminating diplopia and AHP, but that applying prism therapy is essential for improving the treatment results.21 In the present study, prism therapy improved the success rate from 63.8% to 82.8% in eliminating diplopia and from 71.7% to 81.6% in eliminating AHP.
In their characteristics and surgical results, there were no significant differences between the two groups except for mean age, but differences were identified on the NEI-VFQ 25. The total scores were not significantly different between the two groups, but the scores for 8 out of 11 items were significantly higher for the BT group. In addition, compared with VFQ 25 results in other ocular diseases, as reported by Mangione et al22 the BT group was almost equivalent to glaucoma patients for vision (general, near, and distance), social function, mental health, and dependency, whereas the SCVD group was equivalent to patients with age-related macular degeneration (Figure 2). Thus, we show that the postoperative satisfaction in the SCVD group was worse than in the BT group. This might be associated with the sudden onset (stroke) of brain disorders in the SCVD group, with significantly older patients, so that it is presumed unacceptability of the stroke produces the low scores of VFQ 25.5 Some papers have pointed out that stroke not only causes enormous economic burdens but also triggers subsequent disability, including dementia, depression and difficulty in accepting disabilities.2,5 Conversely, the patients with BT (younger age may be involved) allow enough time to accept the disease and prepare for the surgical treatment because a brain tumor does not change its condition suddenly like a stroke.
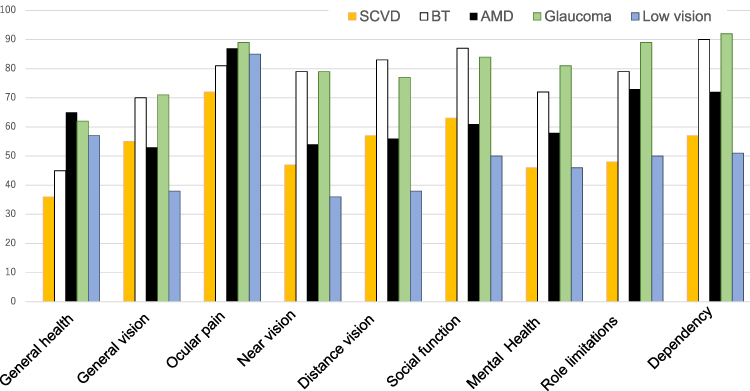 |
Figure 2 National Eye Institute Visual Functioning Questionnaire (NEI-VFQ 25), Japanese version, subscale scores compared between patients with severe cerebrovascular disorder (SCVD) or a brain tumor (BT), and those with other ocular conditions (age-related macular degeneration (AMD), glaucoma and low vision). Reproduced with permission from Arch Ophthalmol, 2001;119(7):1050–1058. doi:10.1001/archopht.119.7.1050, Mangione CM, Lee PP, Gutierrez PR, et al. National eye institute visual function questionnaire field test investigators. Development of the 25-item national eye institute visual function questionnaire.22 Copyright © (2001) American Medical Association. All rights reserved. |
This retrospective study has several limitations. First, we mailed out VFQ 25 and informed consent forms to all subjects regardless of the period after their EOM surgery, and the return rate was low for the VFQ 25 (69.2% for the SCVD group and 47.3% for the BT group). That may be due to the fact that many patients were in a care facility or in need of nursing care. Therefore, the lower response rate might have produced some response bias. One possibility is that those patients who were healthier might have been more likely to respond than those with long-lasting complications from their brain disease. In addition, our results are limited by the short follow-up time, as several patients were discharged from our service 3 months postoperatively; therefore, limited follow-up impeded the accurate assessment of the need for re-operation and the number of needed surgeries.
Although diplopia and AHP after treatment of severe brain disease tend to be regarded as intractable forms of strabismus, the surgical results here were better than expected (the elimination rates for diplopia and AHP were about 80%). We strongly recommend that these patients visit an ophthalmologist soon after their therapy for brain disease and that they receive appropriate treatment, including EOM surgery.
Conclusion
Ocular alignment in most patients after treatment of SCVD or BT showed not only horizontal strabismus but complicating vertical deviation and/or cyclotorsion; hence, these ocular motility disturbances were considered refractory to EOM surgery. However, EOM surgery was effective in eliminating diplopia and AHP. In addition, it became apparent that it took an average of 4 years from the onset of diplopia to first EOM surgery. Therefore, we recommend that these patients visit an ophthalmologist much sooner and undergo EOM surgery.
Abbreviations
EOM, extraocular muscle; AHP, abnormal head posture; SCVD, severe cerebrovascular disorder; BT, brain tumor; QOL, quality of life.
Disclosure
The authors report no conflicts of interest.
References
1. Mukand JA, Blackinton DD, Crincoli MG, Lee JJ, Santos BB. Incidence of neurologic deficits and rehabilitation of patients with brain tumors. Am J Phys Med Rehabil. 2001;80(5):346–350. doi:10.1097/00002060-200105000-00005
2. Pula JH, Yuen CA. Eyes and stroke: the visual aspects of cerebrovascular disease. Stroke Vasc Neurol. 2017;2(4):210–220. doi:10.1136/svn-2017-000079
3. Naoi T, Morita M, Kawakami T, Fujimoto S. Ipsiversive ocular torsion, skew deviation, and hearing loss as initial signs of anterior inferior cerebellar artery infarction. Intern Med. 2018;57(13):1925–1927. doi:10.2169/internalmedicine.0283-17
4. George S, Hayes A, Chen C, Crotty M. Are vision-specific quality of life questionnaires important in assessing rehabilitation for patients with hemianopia post stroke? Top Stroke Rehabil. 2011;18(4):394–401. doi:10.1310/tsr1804-394
5. Chiu SY, Livneh H, Tsao LL, Tsai TY. Acceptance of disability and its predictors among stroke patients in Taiwan. BMC Neurol. 2013;13:175–181. doi:10.1186/1471-2377-13-175
6. Oshika T, Sugita G, Hayashi K, et al. Influence of cataract and intraocular lens surgery on health-related quality of life. Nippon Ganka Gakkai Zasshi. 2005;109(11):753–760.
7. Emi K, Oyagi T, Ikeda T, et al. Influence of vitrectomy for diabetic retinopathy on health-related quality of life. Nippon Ganka Gakkai Zasshi. 2008;112(2):141–147.
8. Nishida Y, Hayashi O, Oda S, et al. A simple muscle transposition procedure for abducens palsy without tenotomy or splitting muscles. Jpn J Ophthalmol. 2005;49(2):179–180. doi:10.1007/s10384-004-0151-2
9. Rush JA, Younge BR. Paralysis of cranial nerves III, IV, and VI. Cause and prognosis in 1,000 cases. Arch Ophthalmol. 1981;99(1):76–79. doi:10.1001/archopht.1981.03930010078006
10. Richards BW, Jones FR, Younge BR. Causes and prognosis in 4,278 cases of paralysis of the oculomotor, trochlear, and abducens cranial nerves. Am J Ophthalmol. 1992;113(5):489–496. doi:10.1016/S0002-9394(14)74718-X
11. Watanabe K, Hagura R, Akanuma Y, et al. Characteristics of cranial nerve palsies in diabetic patients. Diabetes Res Clin Pract. 1990;10(1):19–27. doi:10.1016/0168-8227(90)90077-7
12. Akagi T, Miyamoto K, Kashii S, Yoshimura N. Cause and prognosis of neurologically isolated third, fourth, or sixth cranial nerve dysfunction in cases of oculomotor palsy. Jpn J Ophthalmol. 2008;52(1):32–35. doi:10.1007/s10384-007-0489-3
13. O’Colmain U, Gilmour C, MacEwen CJ. Acute-onset diplopia. Acta Ophthalmol. 2014;92(4):382–386. doi:10.1111/aos.12062
14. Rowe F. The profile of strabismus in stroke survivors. Eye. 2010;24(4):682–685. doi:10.1038/eye.2009.138
15. Pollock A, Hazelton C, Henderson CA, et al. Interventions for disorders of eye movement in patients with stroke. Cochrane Database Syst Rev. 2011;10:CD008389. doi:10.1002/14651858.CD008389.pub2
16. Winstein CJ, Stein J, Arena R, et al. American Heart association stroke council, council on cardiovascular and stroke nursing, council on clinical cardiology, and council on quality of care and outcomes research. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American heart association/american stroke association. Stroke. 2016;47(6):e98–e169. doi:10.1161/STR.0000000000000098
17. Margelisch K, Studer M, Ritter BC, et al. Cognitive dysfunction in children with brain tumors at diagnosis. Pediatr Blood Cancer. 2015;62(10):1805–1812. doi:10.1002/pbc.25596
18. Park UC, Kim SJ, Hwang JM, Yu YS. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye. 2008;22(5):691–696. doi:10.1038/sj.eye.6702720
19. Peragallo JH, Bruce BB, Hutchinson AK, et al. Functional and motor outcomes of strabismus surgery for chronic isolated adult sixth nerve palsy. Neuroophthalmology. 2014;38(6):320–325. doi:10.3109/01658107.2014.957780
20. Holmes JM, Leske DA. Long-term outcomes after surgical management of chronic sixth nerve palsy. J AAPOS. 2002;6(5):283–288. doi:10.1067/mpa.2002.127917
21. Tamhankar MA, Ying GS, Volpe NJ. Prisms are effective in resolving diplopia from incomitant, large, and combined strabismus. Eur J Ophthalmol. 2012;22(6):890–897. doi:10.5301/ejo.5000144
22. Mangione CM, Lee PP, Gutierrez PR, et al. National eye institute visual function questionnaire field test investigators. Development of the 25-item national eye institute visual function questionnaire. Arch Ophthalmol. 2001;119(7):1050–1058. doi:10.1001/archopht.119.7.1050
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.