Back to Journals » Eye and Brain » Volume 11
Orbital Apex Syndrome: A Review
Authors Badakere A, Patil-Chhablani P
Received 16 April 2019
Accepted for publication 8 November 2019
Published 12 December 2019 Volume 2019:11 Pages 63—72
DOI https://doi.org/10.2147/EB.S180190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Margaret Wong-Riley
Akshay Badakere,1 Preeti Patil-Chhablani2
1Jasti V Ramanamma Children’s Eye Care Centre, Pediatric Ophthalmology And Neuro-ophthalmology Services, L V Prasad Eye Institute, Hyderabad 500034, India; 2Department of Ophthalmology, Children’s Hospital of Pittsburgh, University of Pittsburgh Medical Center, UPMC Eye Center, Pittsburgh, PA 15224, USA
Correspondence: Preeti Patil-Chhablani
Department of Ophthalmology, Children’s Hospital of Pittsburgh, University of Pittsburgh Medical Center, UPMC Eye Center, Pittsburgh, PA 15224, USA
Email [email protected]
Abstract: Orbital apex syndrome is characterized by vision loss from optic neuropathy and ophthalmoplegia due to the involvement of ocular motor nerves in the anatomical region of the orbital apex. Patients could present with signs and symptoms deriving from the involvement of structures within the orbital apex, the superior orbital fissure or the cavernous sinus. The primary focus of the ophthalmologist should be to locate the lesion and then identify its etiology. Clinical evaluation holds key to diagnosis which is aided then by certain serological and lab investigations and neuro-imaging modalities including brain and orbital MRI (Magnetic Resonance Imaging) with contrast, CT (Computed Tomography) scans. In rare instances, a biopsy may be needed to aid in diagnosis. Treatment depends on what the nature of the lesion is with inflammatory conditions usually responding to steroids and infections to anti-microbial agents. Through this review, the authors attempt to decode the approach to localizing the lesion, the etiopathology and the management of cases of orbital apex syndrome
Keywords: orbital apex syndrome, Tolosa Hunt syndrome, orbital mucormycosis, orbital imaging
Introduction
The human orbit is shaped like a pyramid with the apex directed posteriorly. This region is anatomically complex due to interactions between bony, vascular and neural structures as is seen in Figure 1.
 |
Figure 1 Diagram representing the anatomy of the orbital apex. Notes: Adapted from Hacking C. Orbital apex (diagram). © 2017 Craig Hacking; CC-BY-SA-NC. Radiopedia.org. Available from: https://radiopaedia.org/cases/orbital-apex-diagram-1?lang=us. Accessed 28 November 2019.31 |
“Orbital apex syndrome” – refers to a constellation of symptoms and signs which result from the involvement of various structures in the region of the orbital apex by a disease process. These structures include the four rectus muscles taking their origin from the tendinous annulus of Zinn, the optic nerve and ophthalmic artery through the optic canal. The superior and inferior branches of the oculomotor nerve, the abducens nerve and the naso-ciliary nerve pass through the annulus of Zinn through the middle portion of the superior orbital fissure.
Orbital Apex syndrome constitutes a syndrome characterized by involvement of the following cranial nerves (C.N)1
- Optic nerve (II C.N)
- Oculomotor nerve (III C.N)
- Trochlear nerve (IV C.N)
- Abducens nerve (VI C.N)
- The first division of the trigeminal nerve (ophthalmic division of V C.N)
Due to anatomical proximity, two other syndromes that can have overlapping features are the Superior orbital fissure syndrome and the cavernous sinus syndrome.
In cavernous sinus syndrome, clinical features result from the combination of orbital apex syndrome and involvement of the sympathetic fibers and the maxillary division of the trigeminal nerve.2 The superior orbital fissure syndrome, also known as Rochon -Duvigneaud syndrome is caused by lesions anterior to the orbital apex and those in close proximity to the annulus of Zinn. It is characterized by multiple cranial nerve involvement but generally spares the optic nerve.
Clinical Features
Due to the large variety of disease conditions that can affect the orbital apex, the prominent clinical symptoms and severity can be quite variable.
The most common clinical features of a disease process in the orbital apex are vision loss and painful and limited eye movements. In addition to these, certain symptoms and signs can help in localizing the lesion, for example, pain around the orbit or the skin around the orbit would likely indicate the involvement of the ophthalmic division whereas facial pain would point towards the maxillary division of the trigeminal nerve. Involvement of the oculomotor, abducens, trochlear nerves in any combination can lead to ophthalmoplegia and patients can present with vertical, horizontal or torsional diplopia with or without compensatory abnormal head postures.
Other important clinical signs are
- Proptosis
- Presence/Absence of corneal sensations and corneal reflex – indicates the involvement of the fifth cranial nerve
- Pupillary abnormalities:
- Relative Afferent Pupillary Defect (RAPD) – indicating the involvement of the optic nerve
- Anisocoria – the side of dilated pupil indicating the involvement of the pupillary fibers of the third cranial nerve
- Optic disc edema or optic atrophy
- Choroidal folds
Differentiation between cavernous sinus syndrome and orbital apex might be difficult because of similar involvement of ocular motor nerves and trigeminal nerve; however, the main differentiator is the optic nerve involvement in orbital apex syndrome. This differentiation is important because the etiologies might be significantly different (eg inflammatory or infectious for the first versus sinus thrombosis).
Etiopathogenesis
A large variety of pathological processes can affect the region of the orbital apex, these may be inflammatory, infectious, or neoplastic in origin. Table 1 shows the main conditions that can lead to orbital apex syndrome.3,4
 |
Table 1 Etiology of Orbital Apex Syndrome syndrome |
Inflammatory Causes
Inflammatory causes for orbital apex syndrome are characterized by the following features1
- Symptoms have a rapid onset and typically progress over days
- Common symptoms include painful limitation of eye movements and may be associated with signs of optic neuropathy
Some of the known causes include ANCA (Anti-neutrophil cytoplasmic antibody) associated vasculitides, which are immune-mediated and tend to have a predilection for small and medium-sized vessels. This group of vasculitis includes 3 conditions which are known to cause orbital apex syndrome are5
- Granulomatosis with polyangiitis (known earlier as Wegener’s Granulomatosis)
- Microscopic polyangiitis
- Churg- Strauss syndrome
These conditions, in addition to affecting the eye, also affect multiple organs leading to Mono neuritis multiplex, granulomas and hemorrhages in the lungs, gastrointestinal tract and central nervous system. Ocular manifestations include (apart from orbital apex syndrome) dry eyes, peripheral corneal ulcer, episcleritis and scleritis, retinal vascular occlusion in young patients.
Tolosa Hunt syndrome (THS) is a common cause of orbital apex syndrome. It presents with painful and limited eye movements and although the exact cause remains unknown, it is believed to be due to an abnormal autoimmune response and granulomatous inflammation affecting the orbital apex and/or cavernous sinus.1 The characteristic feature of THS is periorbital pain, often described as a “gnawing” or “boring” pain, associated with ocular motor nerves paresis as is seen in Figure 2 and typically shows a dramatic response to steroid therapy, with most cases demonstrating clinical improvement within 48–72 hrs. The workup of a patient with suspected THS should include a complete white blood count and distribution, cerebrospinal fluid examination for cytology and microbiological workup and MRI Brain and orbits with gadolinium contrast which has typical findings as shown in Figure 3A and B. Other inflammatory causes and fungal infections must be ruled out before starting steroid therapy in THS. Despite a good response to steroids, THS can relapse,4 and a small percentage of patients may need other immunosuppressive agents in addition to/following steroid therapy.
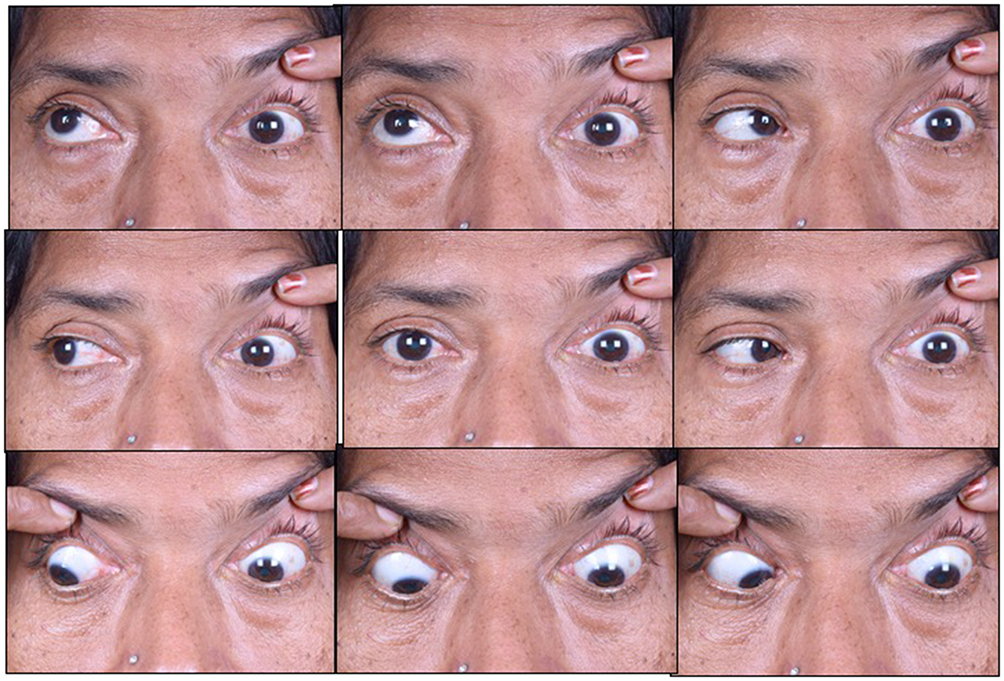 |
Figure 2 Nine gaze photo of a patient with orbital apex syndrome showing limitation of motility in all gazes in the left eye. This patient underwent a complete blood count and distribution, cerebrospinal fluid examination for cytology and microbiological work up, Mantoux test and serum ACE levels along with an MRI Brain and orbits with contrast. Since all the blood investigations were normal, she was diagnosed as Tolosa Hunt Syndrome. |
 |
Figure 3 (A and B) MRI brain and orbits with gadolinium contrast of the same patient mentioned in Figure 2. The yellow circle delineates a homogenously enhancing lesion extending from the left orbital apex to the cavernous sinus. |
IgG4-RD (Immunoglobulin G4- Related Disease) and IgG4-ROD (Immunoglobulin G4- Related Orbital Disease) are characterized by lesions rich in lymphoplasmacytic cells and IgG4 positive plasma cells.
The ocular features include6
- Dacryoadenitis
- Enlarged nerves especially the infraorbital branch of the trigeminal nerve
- Sclerosing orbital inflammation
- Enlargement and thickening of the extraocular muscles
Patients with IgG4-ROD can have systemic involvement in the form of enlarged salivary glands, lymphadenopathy, hydronephrosis due to retroperitoneal fibrosis, auto-immune pancreatitis as well as pulmonary disease. A complete systemic evaluation with the aid of a rheumatologist is ideal in these cases. Andrew et al,7 have used the comprehensive diagnostic criteria by Umehara et al and the consensus diagnostic criteria by Deshpande et al, and diagnosed cases of IgG4-ROD. CT scan or MRI scans of the orbit can help identify the structures involved. Initial response to steroids is good with most patients showing a decrease in inflammatory signs but can relapse on stopping steroids. This warrants a slow taper of steroids and may require patients to be kept on low dose steroids to prevent relapses. Immunosuppressive agents like Azathioprine, Mycophenolate Mofetil, Methotrexate, Rituximab, and radiotherapy, have also been used.6
Infections
Orbital apex syndrome can be caused by viral, bacterial, fungal and parasitic infections which result from contiguous infections of the paranasal sinuses (as is seen in Figure 4A and B) or other surrounding structures.
 |
Figure 4 (A) MRI orbit T2 weighted image (coronal section) shows a hyperintense lesion extending from the left sphenoid sinus (yellow arrow) into the left orbital apex compressing the optic nerve (green arrow). (B) MRI orbit T2 weighted image (coronal section) of the same patient post sphenoid sinus and optic nerve decompression. |
The organisms most commonly implicated in bacterial infections of paranasal sinuses belong to the staphylococcal species, Streptococcus pneumoniae, and gram-negative bacilli like Pseudomonas aeruginosa, Klebsiella and Proteus species.8 Patients with poorly controlled diabetes or immunocompromised patients are particularly susceptible to these infections Pseudomonas is known to produce toxins and osteoclastogenic lipopolysaccharides that can cause bone destruction and spread. This is in contrast to fungal infections which tend to have an angio-invasive nature.9 Early diagnosis and urgent treatment are vital to reducing mortality and morbidity.
Fungal infections are most commonly due to Aspergillus and Mucor.10 Individuals at risk of these infections are those who are immunocompromised due to uncontrolled diabetes, patients on immunosuppressive agents, patients with or being treated for lymphoid malignancies. Infections can spread from paranasal sinuses most commonly and there are reports of vertebral aspergillosis infections spreading to the orbital apex via the Batson’s plexus.11 Rhino-oculo-cerebral mucormycosis is the most common presentation and can be fatal if not identified and treated on time. Despite prompt treatment, the prognosis can be very guarded.9
Orbital apex syndrome is a rare complication of herpes zoster ophthalmicus and tends to have a predilection for immunocompromised patients.12 The possible pathogenic mechanisms are13,14
- Direct cytopathic effect of the virus
- Immune-mediated tissue damage
- Inflammatory edema causing compression and ischemia
Patients present with unilateral vesicular eruptions, vision loss, ophthalmoplegia and anisocoria along with signs of keratouveitis. Typically, ocular manifestations start 1–4 weeks after skin lesions. Treatment includes antivirals. The use of steroids as an add-on therapy is still controversial.
Parasitic infections include cysticercosis, which originates from an infestation with the cysts of Taenia solium and Taenia saginata.15 The most common sites for infestation are subcutaneous tissue followed by brain and eye. These lesions may affect the extraocular muscles or rarely even the optic nerve. The hypotheses for possible spread to the optic nerve are as follows15
- Possible hematogenous spread via the central retinal artery
- Via the pial vessels supplying the optic nerve
Clinical diagnosis depends on clinical examination aided with imaging. B scan (ophthalmic ultrasonography) can identify cysticercosis involving the anterior part of the optic nerve. Lesions close to the orbital apex need neuro-imaging with CT or MRI. Serological tests and immunological tests can be negative in endemic areas hence their role is doubtful. Treatment includes a combination of anthelminthic medications along with steroids. Treatment with antihelminthics alone is not recommended as it can lead to the death of the parasite and cause a severe inflammatory reaction.
Tumors (Neoplasms)
The various neoplastic causes for orbital apex syndrome include head and neck tumors, hematologic cancers and metastatic lesions. The various neoplastic causes for orbital apex syndrome include head and neck tumors, hematologic cancers and metastatic lesions. The loco-regional spread of head and neck cancers to the draining lymph nodes are the most common sites for metastases with lungs and bones being the most common distant sites. Ribeiro et al16 have reported a series of four cases with head and neck cancers who developed orbital apex syndrome. Two patients had nasopharyngeal carcinoma, one had squamous cell carcinoma of the tongue and one had squamous cell carcinoma of the larynx. The most common presenting complaint was diplopia and limitation of eye movements. In this series, all three patients died nine months after development of orbital apex syndrome and one patient died eleven months after development of orbital apex syndrome. According to this author, orbital apex syndrome in a patient with head and neck cancer is an indicator of poor prognosis.
Yuen et al report a case of a 75-year-old female patient who developed orbital apex syndrome as a presentation of ocular adnexal MALT lymphoma.17 Garala et al report a case of an 88-year-old female patient with chronic lymphoid leukemia who developed orbital apex syndrome.18 Nasopharyngeal rhabdomyosarcomas can also cause orbital apex syndrome in children.19
Orbital apex syndrome can also develop due to compression by neural tumors in the orbital apex. Meningiomas, schwannomas, and neurofibromas can cause compression of the contents of the orbital apex.
A rare case of orbital apex syndrome after initiating treatment of skin melanoma with Ipilimumab. Ipilimumab is an IgG1 antibody that targets cytotoxic T lymphocyte-associated protein 4 (CTLA-4). A range of side effects like aseptic meningitis, hypophysitis, Guillain-Barre syndrome, transverse myelitis, myasthenia gravis, and symptoms due to gastrointestinal and hepatic system involvement is known. The two possible causes for orbital apex syndrome hypothesized are20,21
- Orbital myositis due to direct T cell-mediated inflammation
- IgG4 related orbital myositis
Awareness of monoclonal antibodies possibly causing orbital myositis and orbital apex syndrome is crucial for timely management.
Trauma and Iatrogenic Causes
Cranio-maxillo-facial trauma and surgeries of the orbit and sinuses can lead to orbital apex syndrome as a result of the following mechanisms
- Direct compression by displaced bony fragments
- Foreign bodies
- Hematomas or inflammatory edema
There are reports of trauma resulting in Orbital apex syndrome and usually immediate surgical decompression of the orbital apex region is required along with simultaneous treatment with intravenous steroids.22
Surgeries for ethmoid artery ligation for recurrent epistaxis, septo-rhinoplasty and nasal polyps have been reported to result in orbital apex syndrome.23–25
Jarrahy et al, have reported a case of superior orbital fissure syndrome due to a retained foreign body in the orbit.26
Vascular Causes
The three main vascular lesions causing orbital apex syndrome are1,3
- Carotid cavernous fistulas
- Carotid cavernous aneurysms
- Carotid sinus thrombosis
Carotid cavernous fistula (CCF)- these are classified as traumatic or non-traumatic. Traumatic CCFs are most likely due to head trauma and are of the high flow type. Typically, patients present with pulsatile exophthalmos, chemosis and conjunctival congestion. They can also have raised intraocular pressure due to raised episcleral venous pressure.
Non-traumatic causes lead to low flow indirect CCFs. These can be seen in patients with hypertension, in patients with Ehler-Danlos syndrome.
CCFs need extensive investigations including ultrasounds, orbital Doppler studies, MRI studies with MRA (Magnetic Resonance Angiography), CT angiography, catheter angiography, depending upon the individual case the appropriate investigative modality followed by the treatment approach such as conservative management, balloon embolization, and direct or indirect surgery may be considered.27
Cavernous sinus thrombosis (CST) can be septic or aseptic. Septic causes of CST are seen following infections of paranasal sinuses, orbital cellulitis, tooth and ear infections. Aseptic causes are seen in hypercoagulable states as in patients on hormone replacement therapy particularly oral contraceptives, pregnancy, malignancies, congenital causes such as factor V, Leiden mutations, protein C and protein S mutations. While many carotid cavernous aneurysms may be asymptomatic and relatively “benign” in their course, some aneurysms may grow large enough to cause symptoms due to a mass effect on the adjacent cranial nerves resulting in Orbital apex syndrome like picture. Carotid cavernous aneurysms may also rupture, causing CCF and resultant clinical features.
Other causes- Neurofibromatosis, fibrous dysplasia, and dermoid and epidermoid cysts can also cause orbital apex syndrome.
In type 1 and type 2 Neurofibromatosis this syndrome may due to optic nerve gliomas, plexiform neurofibromas, sphenoid wing dysplasia, meningiomas, and schwannomas.
Congenital conditions like fibrous dysplasia can cause orbital apex syndrome by narrowing the optic canal.
Dermoid and epidermoid cysts and mucocele particularly of the ethmoid sinuses can compress the orbital apex. Dermoid cysts in the form of large suprasellar cysts can also lead to cavernous sinus syndrome. Rarely a dermoid cyst can rupture spontaneously and lead to inflammation in the surrounding tissues.28 Hence these developmental and congenital conditions cause features of orbital apex syndrome due to mass effect and in rare cases due to inflammation.
Diagnosis and Management
In neuro-ophthalmology, the primary focus of the physician should be to locate the lesion and then identify its etiology. Localization of the lesion based upon a complete and thorough clinical examination is of utmost importance. As we previously stated, differentiation between orbital apex, superior orbital fissure and cavernous sinus syndromes might be difficult. In general, it might be important to remember that optic nerve involved along with any of the combination of oculomotor, trochlear, abducens, ophthalmic division of trigeminal nerve with or without maxillary division involvement points to orbital apex syndrome, whereas a similar picture without involvement of the optic nerve should orientate towards a lesion in the superior orbital fissure. Finally, cavernous sinus syndrome is recognizable by all the features of superior orbital fissure syndrome along with the involvement of the maxillary division of the trigeminal nerve (Table 2)
 |
Table 2 Depicts a Simple Algorithm to Localize Lesions in and Around the Orbital Apex |
Neuro-imaging is mandatory in patients with orbital apex syndrome. Brain and orbit MRI are the imaging modality of choice and should be performed with gadolinium in case of suspected inflammatory conditions like sarcoidosis, Tolosa Hunt Syndrome, nonspecific orbital inflammatory disease, and vasculitides. MRI with fat suppression sequences is ideal for evaluating the orbital apex and cavernous sinus. Computed tomography (CT) can be done when MRI is contraindicated.1 When a tumor or metastasis are suspected, MRI with gadolinium is recommended to better evaluate:
- Soft tissue involvement
- Cavernous sinus and intracranial extension
- Bone marrow involvement
- Perineural spread of tumors which are characterized by focal or diffuse thickening of the cranial nerves involved
In carotid cavernous aneurysms, Magnetic resonance angiography (MRA) or angio-CT scans can be helpful but angiography remains the gold standard and is useful to plan intravascular treatment. Carotid cavernous fistula can be identified by an angio-CT scan with venous sequences, which can show proptosis, enlarged superior ophthalmic vein and cavernous sinus. These features can be supported by an MRI with contrast showing a dilated superior ophthalmic vein and post-contrast enhancement of the cavernous sinus. As in an aneurysm, digital subtraction angiography (DSA) is recommended if intervention is being planned. In fractures involving the base of the skull and in those where the zygomaticomaxillary or Naso-ethmoidal regions are involved thin-section CT scans with multiplanar reconstruction is advised. Three-dimensional reconstruction of CT images in such cases can help in planning surgeries. MRI has a limited role in these settings and would only be used for looking at intracranial injuries.
Blood investigations include a complete blood count, erythrocyte sedimentation rate peripheral blood smear, and those directed against a particular infectious agent if suspected should be done. A detailed vasculitis workup may be needed to diagnose systemic vasculitides. Tuberculosis and Sarcoidosis should also be kept in mind and targeted investigations such as chest X-ray, Mantoux testing, PCR for M. tuberculosis, Serum ACE levels must be carried out. Tests for HIV and additional investigations like lumbar puncture (LP) may be considered in selected cases – LP can aid diagnosis in infectious conditions and also in neoplastic diseases such as lymphomas, leukemias, meningeal infiltration.
In inflammatory conditions, the primary option of treatment is with corticosteroids under frequent and close observation of the patient. If vision loss or worsening of ophthalmoplegia is noted on steroids then repeat imaging should be considered and a biopsy of the lesion also is mandated.1
The key aspect to remember while dealing with orbital apex syndrome is that treatment is directed towards the underlying condition. The most crucial distinction is between an inflammatory cause and an infection especially fungal infections since they can worsen very quickly and can be fatal if steroid treatment is initiated for the latter. In some cases of Tolosa Hunt syndrome immunosuppressants like methotrexate and azathioprine have been added and in some refractory cases and cases of steroid dependence radiotherapy can be used.29,30
In cases of trauma, corticosteroids can be given while awaiting surgical treatment.
Conclusion
There are multiple causes of orbital apex syndromes varying from inflammatory disorders ion to trauma, tumor (and its treatment for example with immune check-point inhibitors), and infection. A careful clinical examination, paraclinical work-up (including biopsy of the lesion in selected cases) and imaging are essential to establish the
diagnosis and start adequate treatment. Establishing the underlying etiology of this syndrome is particularly important when considering that some specific treatments, such as corticosteroids, might be helpful in some disorders, such as inflammatory causes, but can be detrimental in others, such as infections.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yeh S, Foroozan R. Orbital apex syndrome. Curr Opin Ophthalmol. 2004;15(6):490–498. doi:10.1097/01.icu.0000144387.12739.9c
2. Kline LB. The Tolosa-Hunt syndrome. Surv Ophthalmol. 1982;27(2):79–95. doi:10.1016/0039-6257(82)90190-4
3. Goyal P, Lee S, Gupta N, et al. Orbital apex disorders: imaging findings and management. Neuroradiol J. 2018;31(2):104–125. doi:10.1177/1971400917740361
4. Kline LB, Hoyt WF. The Tolosa-Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71(5):577–582. doi:10.1136/jnnp.71.5.577
5. Schmidt J, Pulido JS, Matteson EL. Ocular manifestations of systemic disease: antineutrophil cytoplasmic antibody-associated vasculitis. Curr Opin Ophthalmol. 2011;22(6):489–495. doi:10.1097/ICU.0b013e32834bdfe2
6. McNab AA, McKelvie P. IgG4-related ophthalmic disease. Part II: clinical aspects. Ophthalmic Plast Reconstr Surg. 2015;31(3):167–178.
7. Andrew NH, Sladden N, Kearney DJ, Selva D. An analysis of IgG4-related disease (IgG4-RD) among idiopathic orbital inflammations and benign lymphoid hyperplasias using two consensus-based diagnostic criteria for IgG4-RD. Br J Ophthalmol. 2015;99(3):376–381. doi:10.1136/bjophthalmol-2014-305545
8. Kusunoki T, Kase K, Ikeda K. A case of orbital apex syndrome due to Pseudomonas aeruginosa infection. Clin Pract. 2011;1(4):e127. doi:10.4081/cp.2011.e127
9. Leung V, Dunn H, Newey A, O’Donnell B. Orbital apex syndrome in pseudomonas sinusitis after functional endoscopic sinus surgery. Ophthal Plast Reconstr Surg. 2018;34(5):e166–e8. doi:10.1097/IOP.0000000000001196
10. Jiang N, Zhao G, Yang S, et al. A retrospective analysis of eleven cases of invasive rhino-orbito-cerebral mucormycosis presented with orbital apex syndrome initially. BMC Ophthalmol. 2016;16:10. doi:10.1186/s12886-016-0189-1
11. Camargo JF, Seriburi V, Tenner M, El Khoury MY. Aspergillus osteomyelitis of the lumbar spine complicated with orbital apex syndrome: a potential role of the Batson’s plexus in disease propagation. Med Mycol Case Rep. 2012;1(1):9–12. doi:10.1016/j.mmcr.2012.02.004
12. Saxena R, Phuljhele S, Aalok L, et al. A rare case of orbital apex syndrome with herpes zoster ophthalmicus in a human immunodeficiency virus-positive patient. Indian J Ophthalmol. 2010;58(6):527–530. doi:10.4103/0301-4738.71708
13. Jun LH, Gupta A, Milea D, Jaufeerally FR. More than meets the eye: varicella zoster virus-related orbital apex syndrome. Indian J Ophthalmol. 2018;66(11):1647–1649. doi:10.4103/ijo.IJO_592_18
14. Merino-Iglesias A, Montero JA, Calabuig-Goena M, Giraldo-Agudelo LF. Orbital apex syndrome secondary to herpes zoster virus infection. BMJ Case Rep. 2014;2014:bcr2013203200.
15. Chaugule P, Varma DR, Patil Chhablani P. Orbital apex syndrome secondary to optic nerve cysticercosis. Int Ophthalmol. 2019;39(5):1151–1154. doi:10.1007/s10792-018-0910-6
16. Prado-Ribeiro AC, Luiz AC, Montezuma MA, Mak MP, Santos-Silva AR, Brandao TB. Orbital apex syndrome affecting head and neck cancer patients: a case series. Med Oral Patol Oral Cir Bucal. 2017;22(3):e354–e8. doi:10.4317/medoral.21506
17. Yuen CA, Pula JH, Mehta M. Primary ocular adnexal extranodal Marginal Zone Mucosa-Associated Lymphoid Tissue (MALT) lymphoma presenting as orbital apex syndrome. Neuroophthalmology. 2017;41(2):94–98. doi:10.1080/01658107.2016.1263343
18. Garala K, Jayaramachandran P, Knopp M, Critchley P. Orbital apex tumour caused by chronic lymphocytic leukaemia: an unlikely suspect. BMJ Case Rep. 2013;2013. doi:10.1136/bcr-2013-200166
19. Shindler KS, Liu GT, Womer RB. Long-term follow-up and prognosis of orbital apex syndrome resulting from nasopharyngeal rhabdomyosarcoma. Am J Ophthalmol. 2005;140(2):
20. Carrera W, Baartman BJ, Kosmorsky G. A case report of drug-induced myopathy involving extraocular muscles after combination therapy with tremelimumab and durvalumab for non-small cell lung cancer. Neuroophthalmology. 2017;41(3):140–143. doi:10.1080/01658107.2017.1291686
21. Hassanzadeh B, DeSanto J, Kattah JC. Ipilimumab-induced adenohypophysitis and orbital apex syndrome: importance of early diagnosis and management. Neuroophthalmology. 2018;42(3):176–181. doi:10.1080/01658107.2017.1368090
22. Imaizumi A, Ishida K, Ishikawa Y, Nakayoshi I. Successful treatment of the traumatic orbital apex syndrome due to direct bone compression. Craniomaxillofac Trauma Reconstr. 2014;7(4):318–322. doi:10.1055/s-00000151
23. Jaison SG, Bhatty SM, Chopra SK, Satija V. Orbital apex syndrome: a rare complication of septorhinoplasty. Indian J Ophthalmol. 1994;42(4):213–214.
24. Vassallo P, Tranfa F, Forte R, D’Aponte A, Strianese D, Bonavolonta G. Ophthalmic complications after surgery for nasal and sinus polyposis. Eur J Ophthalmol. 2001;11(3):218–222. doi:10.1177/112067210101100302
25. Yeh S, Yen MT, Foroozan R. Orbital apex syndrome after ethmoidal artery ligation for recurrent epistaxis. Ophthal Plast Reconstr Surg. 2004;20(5):392–394. doi:10.1097/01.IOP.0000139524.87938.18
26. Jarrahy R, Cha ST, Shahinian HK. Retained foreign body in the orbit and cavernous sinus with delayed presentation of superior orbital fissure syndrome: case report. J Craniofac Surg. 2001;12(1):82–86. doi:10.1097/00001665-200101000-00014
27. de Keizer R. Carotid-cavernous and orbital arteriovenous fistulas: ocular features, diagnostic and hemodynamic considerations in relation to visual impairment and morbidity. Orbit. 2003;22(2):121–142. doi:10.1076/orbi.22.2.121.14315
28. Orakcioglu B, Halatsch ME, Fortunati M, Unterberg A, Yonekawa Y. Intracranial dermoid cysts: variations of radiological and clinical features. Acta Neurochir (Wien). 2008;150(12):
29. Mormont E, Laloux P, Vauthier J, Ossemann M. Radiotherapy in a case of Tolosa-Hunt syndrome. Cephalalgia. 2000;20(10):931–933. doi:10.1046/j.1468-2982.2000.00147.x
30. Smith JR, Rosenbaum JT. A role for methotrexate in the management of non-infectious orbital inflammatory disease. Br J Ophthalmol. 2001;85(10):1220–1224. doi:10.1136/bjo.85.10.1220
31. Hacking C Orbital apex (diagram). Available from: https://radiopaedia.org/cases/orbital-apex-diagram-1?lang=us.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.