Back to Journals » Clinical Interventions in Aging » Volume 10
One-site versus two-site phacotrabeculectomy: a prospective randomized study
Authors Moschos M, Chatziralli I ![]() , Tsatsos M
, Tsatsos M
Received 28 May 2015
Accepted for publication 7 July 2015
Published 24 August 2015 Volume 2015:10 Pages 1393—1399
DOI https://doi.org/10.2147/CIA.S89401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Marilita M Moschos,1 Irini P Chatziralli,2 Michael Tsatsos3
1First Department of Ophthalmology, University of Athens, 2Second Department of Ophthalmology, Ophthalmiatrion Athinon, Athens, Greece; 3Department of Ophthalmology, Cambridge University Hospital NHS, Cambridge, UK
Purpose: The purpose of this study is to compare the efficacy and safety of one-site and two-site combined phacotrabeculectomy with foldable posterior chamber intraocular lens implantation.
Methods: Thirty-four patients (41 eyes) with glaucoma and cataract were randomly assigned to undergo either a one-site (22 eyes) or a two-site (19 eyes) combined procedure. One-site approach consisted of a standard superior phacotrabeculectomy with a limbus-based conjunctival flap, while two-site approach consisted of a clear cornea phacoemulsification and a separate superior trabeculectomy with a limbus-based conjunctival flap.
Results: Mean follow-up period was 54 months (standard deviation [SD] 2.3). Mean preoperative intraocular pressure (IOP) in the one-site group was 21.3 mmHg (SD 2.8) and in the two-site group was 21.8 mmHg (SD 3.0) (P>0.1). Mean postoperative IOP significantly decreased in both groups compared to the preoperative level and was 15.6 mmHg (SD 3.5) in the one-site group and 14.9 mmHg (SD 2.7) in the two-site group. Three months later, the difference between the two groups was not statistically significant (P=0.058). The one-site group required significantly more medications than the two-site group (P=0.03). Best-corrected visual acuity (BCVA) improved similarly in both groups, but there was less postoperative (induced) astigmatism in the two-site group in a marginal statistical level (P=0.058). Intra- and postoperative complications were comparable in the two groups.
Conclusion: Both techniques yielded similar results concerning final BCVA and IOP reduction. However, the two-site group had less induced astigmatism and a better postoperative IOP control with less required postoperative antiglaucoma medications compared to the one-site group.
Keywords: glaucoma, filtering surgery, intraocular pressure
Introduction
The use of phacoemulsification in cataract surgery has opened new dimensions in the management of patients with glaucoma and visually significant cataract. Small incision cataract surgery induces less inflammation, and therefore, less fibrosis at the site of the incision compared to extracapsular cataract extraction.1,2 A clear cornea approach leaves the conjunctiva intact and creates minimal distortion to the angle.3 The degree of postoperative intraocular inflammation is significantly lower with phacoemulsification, as the formation of peripheral anterior synechiae and the release of pigment cells in the anterior chamber are accordingly low. Therefore, in patients with visually significant cataract and glaucoma that is not adequately controlled with topical medication, the risk of failure of the glaucoma-filtering surgery is lower when phacoemulsification is preferred to extracapsular cataract extraction for the treatment of cataract.4
However, phacoemulsification may cause a significant short-term intraocular pressure (IOP) rise in the early postoperative period, and trabeculectomy is associated with progression of a preexisting cataract.5–8 Combined phacoemulsification and glaucoma-filtering surgery has the advantage of early visual rehabilitation, carries a lower risk of early postoperative IOP increase compared to phacoemulsification alone, and may result in adequate long-term control of glaucoma.9 Two main techniques of phacotrabeculectomy have been described: the one-site and the two-site approach.
In this prospective randomized study, our purpose was to compare the outcomes of one-site versus two-site combined phacoemulsification with a foldable intraocular lens (IOL) implantation and trabeculectomy and to report on the efficacy and safety of the two procedures.
Materials and methods
All patients with glaucoma and visually significant cataract who presented at the First University Department of Ophthalmology, University of Athens, Greece, during the period of 1 year were included in the study and were randomly assigned to undergo either one-site or two-site combined phacotrabeculectomy performed by one experienced anterior segment surgeon. Visually significant cataract was defined as a cataract that reduced the best-corrected visual acuity (BCVA) more than five lines in the Snellen chart. Exclusion criteria were the presence of lens subluxation, neovascular glaucoma, advanced visual field loss, and/or excessive cupping of the disk or history of previous intraocular surgery.
Forty-six eyes of 38 patients who met the inclusion criteria were included in the study. Five eyes of four patients were excluded from analysis because of loss at the follow-up. Therefore, we report on the findings of the remaining 41 eyes of 34 patients. This study is in accordance with the Declaration of Helsinki and has been approved by the Institutional Review Board of “G.Gennimatas” Hospital. Written informed consent was obtained from all patients.
Patients were randomized by the method of random numbers into two groups: 1) Group I (n=22 eyes), who underwent one-site phacotrabeculectomy and 2) Group II (n=19 eyes), who underwent two-site procedure. The technique in Group I involved fashioning a limbal-based conjunctival flap in the superior conjunctival quadrant and a scleral tunnel at the 12 o’clock position. The phacoemulsification was subsequently performed through the scleral tunnel, and a foldable acrylic posterior chamber IOL implant was inserted. The scleral tunnel was then converted to a scleral flap. No antimetabolites were used. A trabeculectomy was performed with a knife and Vannas scissors, followed by a peripheral iridectomy. The scleral flap was closed with two 10-0 nylon sutures, and the conjunctival flap was sutured with a mattress-type 10-0 nylon suture.
The two-site procedure was performed as follows: a limbal-based conjunctival flap and a 4 mm wide square scleral flap were fashioned superonasally, without the use of antimetabolites. A phacoemulsification through a temporal clear corneal incision was performed, and a foldable acrylic posterior chamber IOL implant was inserted. The trabeculectomy was subsequently performed with a knife and Vannas scissors, followed by a peripheral iridectomy. The scleral flap was then sutured with two 10-0 nylon sutures, and the conjunctival flap was closed with a running, two-layer 8-0 polyglycolic acid suture (BioSorb; Alcon Laboratories, Fort Worth, TX, USA).
All patients received the same postoperative regimen. Specifically, a topical combination of chloramphenicol and dexamethasone 1 mg/mL was used four times daily for 3 weeks postoperatively in both groups and then tapered over 2 weeks. No antimetabolites were used postoperatively in either group.
Preoperative data included patient’s age, sex, diagnostic type of glaucoma, BCVA measurement, the presence of any other ocular pathology (apart from cataract) that may reduce visual acuity, IOP measured by Goldmann applanation tonometry, and the number of preoperative glaucoma medications. It is worthy to mention that two patients (one of each group) were on no glaucoma medications preoperatively because of the absence of tolerance in all antiglaucoma treatments. Operative data included date of operation, surgical technique (one-site or two-site phacotrabeculectomy), and the presence of any operative complications.
BCVA was measured in Snellen charts and converted to logMAR scale for statistical purposes. BCVA and induced astigmatism were measured at 1 month and 3 months postoperatively and every year thereafter. In the early postoperative period, IOP measurements were made 24 hours after surgery, and then on the third day. Subsequently, a diurnal curve of IOP was performed (minimum of three measurements) 1 month and 3 months after surgery and thereafter every 6 months. A masked observer made all measurements. If IOP was found to be 20 mmHg or higher during follow-up, an antiglaucoma medication was introduced or added if necessary. The presence of any postoperative complications and the number of postoperative antiglaucoma medications at the last examination were also recorded. The mean follow-up time in both groups was 54 months (standard deviation [SD] 2.3).
Statistical methods
For comparisons between the two groups, the Mann–Whitney–Wilcoxon test for independent samples or the Wilcoxon signed-rank test was used for continuous variables, and the Pearson’s χ2 test was used for categorical variables, as appropriate. A P-value less than 0.05 was considered statistically significant. Statistical analysis was performed with SPSS 17.0 statistical software (SPSS Inc., Chicago, IL, USA).
Results
The study design, as well as the randomization of patients into the two groups, is depicted in the flowchart shown in Figure 1. The baseline characteristics (demographic and preoperative findings) of each group are summarized in Table 1. There was no statistically significant difference between the two groups in age, preoperative BCVA, preoperative IOP, and number of glaucoma medications used before the operation.
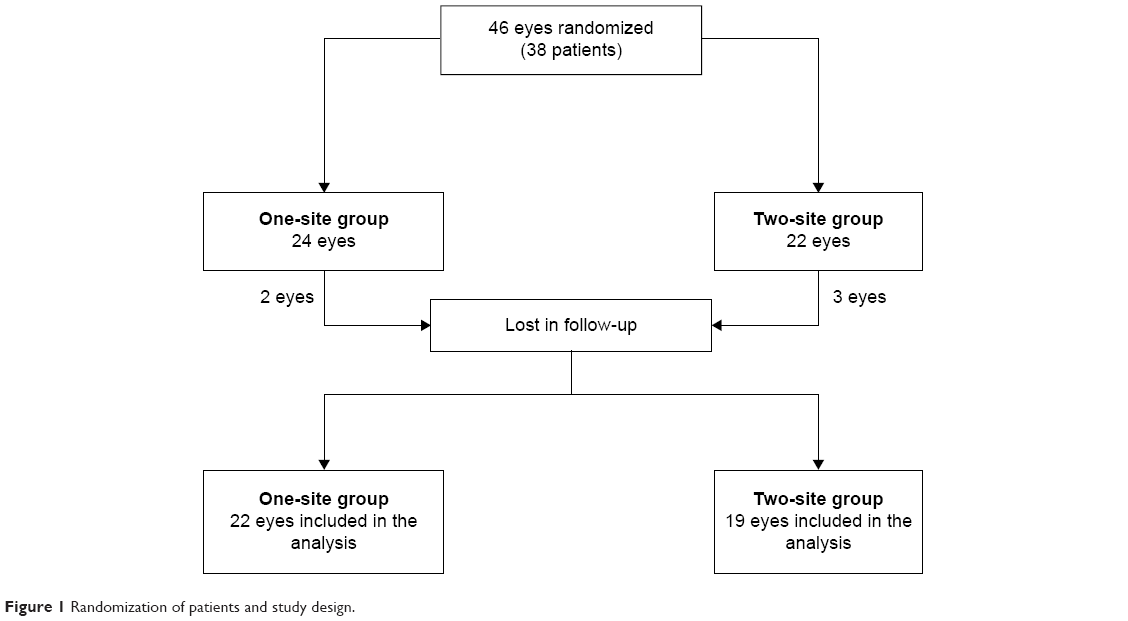 | Figure 1 Randomization of patients and study design. |
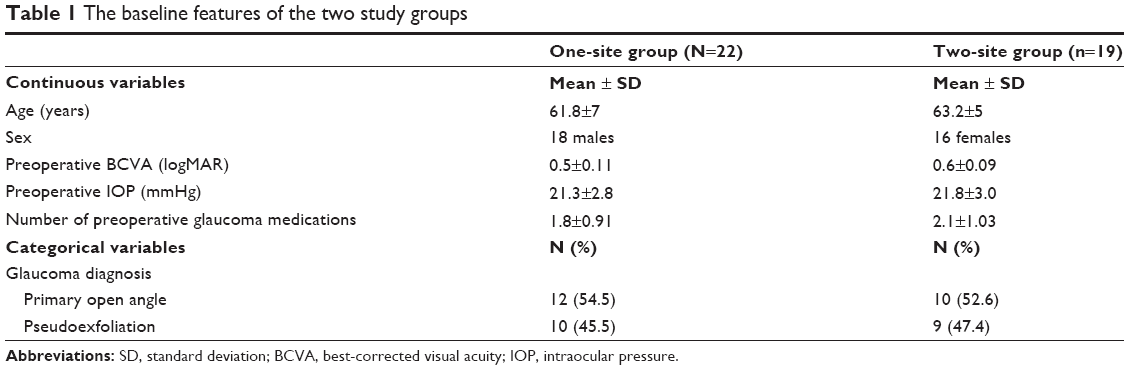 | Table 1 The baseline features of the two study groups |
The mean postoperative IOP was reduced after surgery in both groups and was 15.6 mmHg (SD 3.5) in the one-site group and 14.9 mmHg (SD 2.7) in the two-site group. Although the two-site group had lower IOP in the first 3 months after the operation compared to the one-site group, the difference between the two groups was not statistically significant (P=0.058, Mann–Whitney–Wilcoxon test) at the time of the last recorded measurement (Table 2).
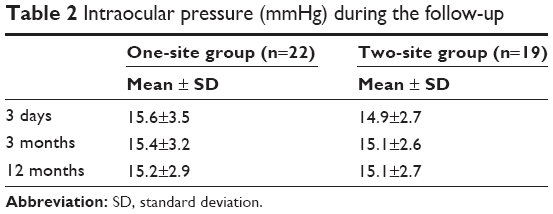 | Table 2 Intraocular pressure (mmHg) during the follow-up |
The number of glaucoma medications was reduced from 1.8 preoperatively to 0.6 postoperatively in the one-site group and from 2.1 preoperatively to 0.2 postoperatively in the two-site group. There is a statistically significant difference in favor of the two-site group in the number of glaucoma medications used postoperatively (P=0.03, Mann–Whitney–Wilcoxon test). No patient in the two-site group used more than one medication postoperatively in order to achieve adequate control of IOP. Three patients in the one-site group needed two glaucoma medications postoperatively. The percentage of patients who were on no medications postoperatively was lower in the two-site group (15; 78.95% of all patients in the group) compared to the one-site group (11; 50% of all patients in the group). All patients used fewer glaucoma medications after surgery. The number of glaucoma medications used pre- and postoperatively by patients in each of the two groups is illustrated in Figures 2 and 3.
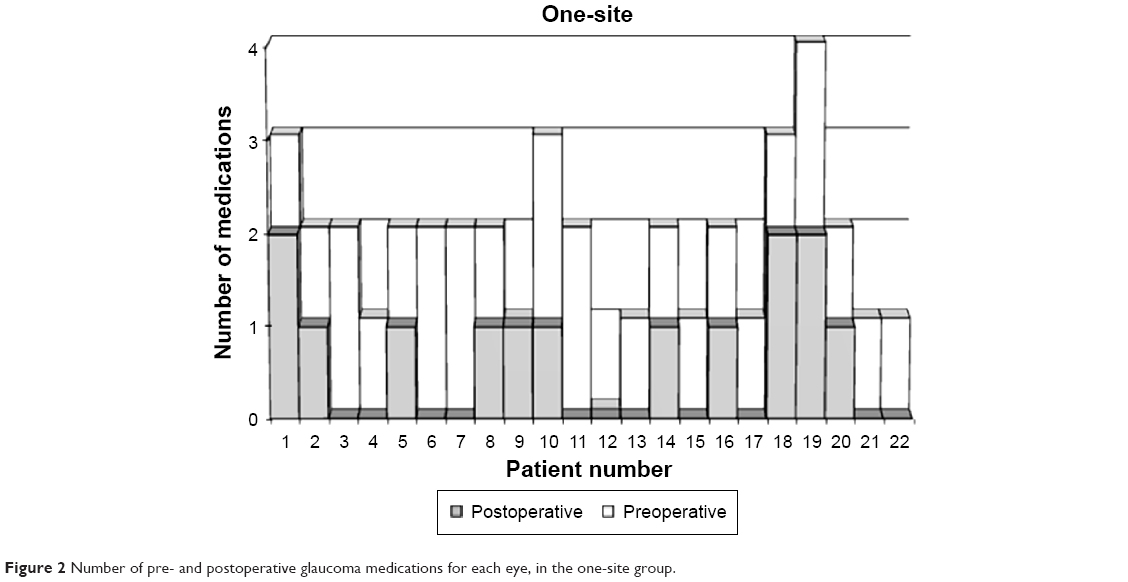 | Figure 2 Number of pre- and postoperative glaucoma medications for each eye, in the one-site group. |
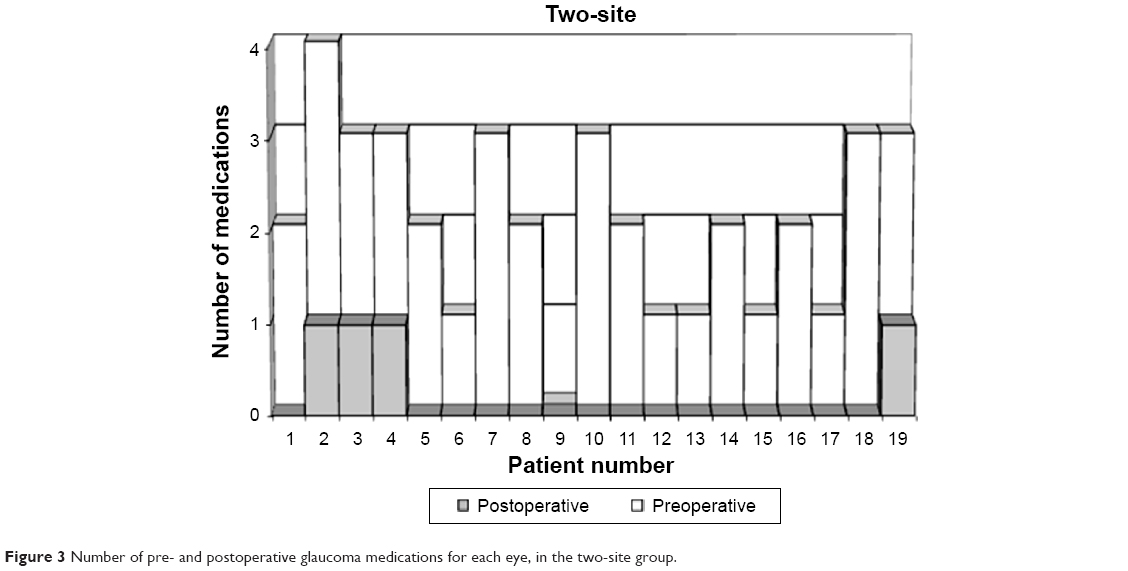 | Figure 3 Number of pre- and postoperative glaucoma medications for each eye, in the two-site group. |
Mean BCVA improved from 0.6 logMAR preoperatively to 0.15 logMAR postoperatively in the two-site group (P<0.001, Wilcoxon signed-rank test) and from 0.50 logMAR preoperatively to 0.2 logMAR postoperatively in the one-site group (P<0.001, Wilcoxon signed-rank test). There was no statistically significant difference between the two groups in mean postoperative BCVA (P>0.5, Mann–Whitney–Wilcoxon test).
The amount of induced astigmatism was 0.3 D (SD 0.11) in the two-site group and 0.4 D (SD 0.28) in the one-site group, and although it was lower in the two-site group, the two groups did not differ significantly (P=0.058, Mann–Whitney–Wilcoxon test). However, in no case was the induced astigmatism higher than 0.5 D in the two-site group, whereas astigmatism of 1.25 D was induced in one patient, 1 diopter in one patient, and 0.75 D in two patients in the one-site group.
No intra-operative complications occurred, and no major postoperative complications were encountered in either group. Hyphema occurred in one patient in the one-site group and was treated with irrigation of the anterior chamber. One eye in the one-site group presented with shallow anterior chamber. There were no postoperative complications in the two-site group. It is also worthy to say that no patient required a reoperation or a laser capsulotomy during the follow-up period.
Discussion
The management of coincident cataract and glaucoma is a clinical challenge, and in recent years, significant changes in surgical technique have been reported. The progress in small-size incision cataract surgery with IOL implantation has influenced the approach of management of an eye with glaucoma and cataract. The question is whether the one- or two-site combined phacotrabeculectomy is safer and more effective in improving vision and decreasing IOP.
Cataract and glaucoma are frequently coexisting ocular conditions in the elderly population. Recently, as the surgical techniques used to treat both cataracts and glaucoma have advanced, there has been an increased number of reports in the literature regarding the optimal management of these conditions. Evidence suggests that cataract surgery alone may be appropriate for some patients, although combining a trabeculectomy with the cataract extraction significantly increases the IOP-lowering effect.10
Several ophthalmologists advocate that the two-site approach, in which the phacoemulsification component is performed through a temporal approach followed by trabeculectomy, offers reduction in the conjunctival manipulation and technical ease of the cataract extraction.10–12 Other investigators have reported a very slight difference between the one- and two-site approaches.13–15
As far as the IOP is concerned, previous studies suggested that there was no statistically significant difference in postoperative IOP between one- and two-site phacotrabeculectomy,16–18 although a recent meta-analysis of randomized controlled trials supported that the two-site phacotrabeculectomy is superior to one-site phacotrabeculectomy in reducing IOP.19 Similar to previous studies, our results show that both techniques are effective in lowering the IOP, and at the end of the follow-up period, there was no significant difference between the two groups, although the mean IOP of the two-site group was lower (P=0.058). During the whole follow-up period after surgery, the two-site group had consistently lower IOP than the one-site group, something more pronounced in the early postoperative period. It is also interesting enough that a glaucoma reoperation was not required in all cases.
As more time elapsed since the operation, the difference in mean IOP between the two groups became smaller. This coincided with an increased use of antiglaucoma medications in the one-site group. Therefore, our findings of similar mean IOP in the two groups at the end of follow-up do not suggest that both techniques were equally effective in controlling the IOP. On the contrary, the one-site technique was less effective and necessitated the use of more medications in order to reach the same level of IOP as the two-site technique. This can be attributed to increased manipulation of the conjunctival and scleral flaps, and therefore, increased fibrosis.20 The topical increase in temperature at the trabeculectomy site and at the scleral flap caused by the production of heat by the phacoemulsification probe is another possible factor contributing to decreased efficacy of the one-site technique.
Furthermore, all patients in both groups required fewer antiglaucoma medications postoperatively. However, the number of postoperative medications was significantly lower in the two-site group than in the one-site group. A much higher percentage of patients in the two-site group needed no medications, and no patient in this group required more than one medication after surgery. Three patients in the one-site group needed two glaucoma medications postoperatively.
Visual acuity following surgery improved in all cases included in our study. This was due to the facts that no patient had a preoperative ocular pathology that could limit the final visual outcome and no major complications occurred with either technique. In addition, no significant difference in final visual outcome between the two techniques was observed.
Both methods were safe to perform, and we experienced no intra-operative complications. Moreover, no major postoperative complications occurred in either group. We only encountered two minor postoperative complications in two patients in the one-site group. One patient developed hyphema, which was treated with irrigation of the anterior chamber, and one patient presented with shallow anterior chamber. In a prospective randomized study of one-site versus two-site phacotrabeculectomy, Borggrefe et al found a 24% increase in postoperative fibrinous uveitis.21 According to Allan and Barrett, the incidence of postoperative uveitis increases to 33%. In our study, no patient presented postoperative uveitis.22
Previous studies have shown that a scleral tunnel induces less astigmatism compared to a clear corneal incision in cataract surgery.23 Other authors have concluded that an incision at the 12 o’clock position induces more astigmatism compared to a temporal incision.24 We found that the amount of induced astigmatism was lower in the two-site group, where we performed a clear corneal incision in a lateral location. The one-site group, with a scleral tunnel at the 12 o’clock position, resulted in greater induced astigmatism, and this is in accordance with the findings of other authors.13 The theoretical advantage of the scleral tunnel was outweighed by the astigmatism-inducing effect of an incision at the 12 o’clock position. This could be due to the fact that a combined procedure requires more manipulations through the scleral tunnel compared to phacoemulsification alone.
It is also worth to mention that different suture materials were used for the closure of the conjunctiva in the two groups. The 8-0 polyglycolic acid suture is more effective for the closure of large conjunctival gaps than 10-0 nylon suture used in the one-site group.
Potential limitation of our study pertains to the fact no subgroup analysis was performed concerning pseudoexfoliation glaucoma because of the small sample size of the two subgroups.
Conclusion
In conclusion, our study suggests that both the one-site and two-site combined phacotrabeculectomy techniques are safe and effective in improving vision and decreasing IOP. However, the two-site technique allows a better control of IOP, at a lower level and with fewer antiglaucoma medications.
Disclosure
The authors report no conflicts of interest in this work.
References
Handa J, Henry JC, Krupin T, Keates E. Extracapsular cataract extraction with posterior chamber lens implantation in patients with glaucoma. Arch Ophthalmol. 1987;105:765–769. | ||
Beckers HJM, de Kroon KE, Nuijts RMMA, Webers CAB. Phacotrabeculectomy. Doc Ophthalmol. 2000;100:43–47. | ||
Tennen DG, Masket S. Short- and long-term effect of clear corneal incisions on intraocular pressure. J Cataract Refract Surg. 1996;22:568–570. | ||
Tezel G, Kolker AE, Kass MA, Wax MB. Comparative results of combined procedures for glaucoma and cataract: I. Extracapsular cataract extraction versus phacoemulsification and foldable versus rigid intraocular lenses. Ophthalmic Surg Lasers. 1997;28:539–550. | ||
Krupin T, Feitl ME, Bishop KI. Postoperative intraocular pressure rise in open-angle glaucoma patients after cataract or combined cataract-filtration surgery. Ophthalmology. 1989;96:579–584. | ||
Obstbaum SA. Glaucoma and intraocular lens implantation. J Cataract Refract Surg. 1986;12:257–261. | ||
Gimbel HV, Meyer D, DeBroff BM, Roux CW, Ferensowicz M. Intraocular pressure response to combined phacoemulsification and trabeculectomy ab externo versus phacoemulsification alone in primary open-angle glaucoma. J Cataract Refract Surg. 1995;21:653–660. | ||
Suzuki R, Kuroki S, Fujiwara N. Ten-year follow-up of intraocular pressure after phacoemulsification and aspiration with intraocular lens implantation performed by the same surgeon. Ophthalmologica. 1997;211:79–83. | ||
Casson RJ, Salmon JF. Combined surgery in the treatment of patients with cataract and primary open-angle glaucome. J Cataract Refract Surg. 2001;27:1854–1863. | ||
Wyse T, Meyer M, Ruderman JM, et al. Combined phacotrabeculectomy and phacoemulsification: a one-site v two-site approach. Am J Ophthalmol. 1998;125:334–339. | ||
Park HJ, Weitzman M, Caprioli J. Temporal corneal phacoemulsification combined with superior trabeculectomy. A retrospective case-control study. Arch Ophthalmol. 1997;115:318–323. | ||
Shingleton BJ, Chaundhry IM, O’Donoghue MW. Phacotrabeculectomy; limbus-based versus fornix-based conjunctival flaps in fellow eyes. Ophthalmology. 1999;106:1152–1155. | ||
Rossetti L, Bucci L, Miglior S, Orzalesi N. Temporal corneal phacoemulsification combined with separate-incision superior phacotrabeculectomy; a comparative study. Acta Ophthalmol Scand Suppl. 1997;224:39–43. | ||
el Sayyad F, Helal M, el-Maghraby A, Khalil M, el-Hamzawey H. One-site versus 2-site phacotrabeculectomy: a randomized study. J Cataract Refract Surg. 1999;25:77–82. | ||
Gayton JL, Van Der Karr MA, Sanders V. Combined cataract and glaucoma procedures using temporal cataract surgery. J Cataract Refract Surg. 1996;22:1485–1491. | ||
Buys YM, Chipman ML, Zack B, Rootman DS, Slomovic AR, Trope GE. Prospective randomized comparison of one- versus two-site phacotrabeculectomy two-year results. Ophthalmology. 2008;115:1130–1133. | ||
Bagli E, Gartzios C, Asproudis I, Kitsos G. Comparison of one-site versus two-site phacotrabeculectomy without the use of antimetabolites intraoperatively in patients with pseudoexfoliation glaucoma and primary open-angle glaucoma. Clin Ophthalmol. 2009;3:297–305. | ||
Cotran PR, Roh S, McGwin G. Randomized comparison of 1-site and 2-site phacotrabeculectomy with 3-year follow-up. Ophthalmology. 2008;115:447–454. | ||
Liu HN, Chen XL, Li X, Nie QZ, Zhu Y. Efficacy and tolerability of one-site versus two-site phaco-trabeculectomy: a meta-analysis of randomized controlled clinical trials. Chin Med J. 2010;123:2111–2115. | ||
Weitzman M, Caprioli J. Temporal phacoemulsification combined with separate-incision trabeculectomy. Ophthalmic Surg Lasers. 1995;26:271–273. | ||
Borggrefe J, Lieb W, Grehn F. A prospective randomized comparison of two techniques of combined cataract-glaucoma surgery. Graefes Arch Clin Exp Ophthalmol. 1999;227:887–892. | ||
Allan BDS, Barrett GD. Combined small incision phacoemulsification and trabeculectomy. J Cataract Refract Surg. 1993;19:97–102. | ||
Vyas AV, Bacon PJ, Persival SP. Phacotrabeculectomy: comparison of results from 3.5- and 5.2-mm incisions. Ophthalmic Surg Lasers. 1998;29:227–233. | ||
Cagini C, Murdolo P, Gallai R. Long-term results of one-site phacotrabeculectomy. Acta Ophthalmol Scand. 2003;81:233–236. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.