Back to Journals » Patient Preference and Adherence » Volume 8
Non-pharmaceutical factors for poor glycemic control in 13,970 Chinese women with drug-treated type 2 diabetes: a cross-sectional survey in 77 tertiary hospitals in four Chinese cities
Authors Lu JL, Weng J, Gu W, Guo X, Yang W, Zou D, Zhou Z, Zhu D, Ji Q, Ji L, Yang X ![]()
Received 28 April 2014
Accepted for publication 27 June 2014
Published 30 August 2014 Volume 2014:8 Pages 1161—1167
DOI https://doi.org/10.2147/PPA.S66915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Juming Lu,1,* Jianping Weng,2,* Weijun Gu,1 Xiaohui Guo,3 Wenying Yang,4 Dajin Zou,5 Zhiguang Zhou,6 Dalong Zhu,7 Qiuhe Ji,8 Linong Ji,9 Xilin Yang10
1Department of Endocrinology, Chinese PLA General Hospital, Beijing, 2Department of Endocrinology, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, 3Department of Endocrinology, First Hospital of Peking University, Beijing, 4Department of Endocrinology, Sino-Japan Friendship Hospital, Beijing, 5Department of Endocrinology, Changhai Hospital of Shanghai, Shanghai, 6Department of Endocrinology, The Second Xiangya Hospital of Central South University, Changsha, 7Department of Endocrinology, Nanjing Drum Tower Hospital, Nanjing, Jiansu, 8Department of Endocrinology, Xijing Hospital affiliated to 4th Military Medical University, Xi’an, 9Department of Endocrinology, Peking University People’s Hospital, Beijing, 10Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China
*These authors contributed equally to the manuscript
Background: Achieving good glycemic control improves clinical outcomes among patients with type 2 diabetes (T2D). This study aimed to explore non-pharmaceutical factors for poor glycemic control in Chinese women with T2D who used antidiabetic drug(s).
Methods: A cross-sectional survey was conducted in March to June 2011 in 77 top tertiary hospitals in Beijing, Shanghai, Tianjin, and Guangzhou, People’s Republic of China (the coverage rates of the 3A hospitals: 74.4%, 76%, 55%, and 29.3%, respectively). Of 29,502 patients with T2D who used oral antidiabetic drugs (OADs) alone or combined with insulin, 13,970 were women and used in the analysis. Logistic regression analysis was used to obtain odds ratios (ORs) and 95% confidence intervals (CIs) of factors for hyperglycemia defined as HbA1c (glycated hemoglobin) ≥77 mmol/mol (7.0%).
Results: The mean age was 60.3 (standard deviation 11.0) years, with a median of 4 (interquartile range 2–9) years of duration of diabetes, and 65.1% had hyperglycemia. In multivariable analysis, body height of ≥164 cm (OR 1.26, 95% CI 1.15–1.37) and obesity (OR 1.16, 95% CI 1.04–1.31) was associated with increased risk of hyperglycemia, while self-monitoring blood glucose (SMBG) decreased the risk of hyperglycemia (OR 0.78, 95% CI 0.73–0.84). Duration of diabetes ≥3 years (≥3 to <6 years, OR 1.46, 95% CI 1.32–1.62; ≥6 to <10 years, OR 1.65, 95% CI 1.44–1.89), especially ≥10 years (OR 1.95, 95% CI 1.73–2.19), was associated with higher risks of hyperglycemia.
Conclusion: Body height ≥164 cm, obesity, and duration of diabetes ≥3 years increased while SMBG decreased risk of hyperglycemia in Chinese women with OAD-treated T2D.
Keywords: HbA1c goal, hyperglycemia, oral antidiabetic drugs
Introduction
The prevalence of diabetes has been increasing worldwide, especially in the People’s Republic of China.1 Type 2 diabetes (T2D) increases the risk of micro- and macrovascular diseases2,3 and shortens life expectancy by 10–12 years.4 It is established that hyperglycemia increases the risk of diabetes complications, including microvascular diseases and macrovascular diseases, while hyperglycemia control decreases their risk. The United Kingdom Prospective Diabetes Study (UKPDS) showed that maintaining glycated hemoglobin (HbA1c) around 77 mmol/mol (7.0%) by intensive blood-glucose control with sulfonylureas and/or insulin was able to reduce a 25% risk of microvascular endpoints over a 10-year period as compared with a conventional group whose HbA1c was around 86 mmol/mol (7.9%),5 and achieved a 9% risk reduction in any diabetes-related endpoint, 24% risk reduction in the microvascular endpoint, a 15% risk reduction in myocardial infarction over 10 years of further follow-up after the original trial.6 Although the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial found that further tight control of HbA1c below 66 mmol/mol (6.0%) increased mortality risk,7 both the ACCORD trial and the Veterans Affairs Diabetes Trial found that tight control of HbA1c below 66 mmol/mol (6.0%) did not achieve additional reduction in the risk of cardiovascular disease,7,8 the Action in Diabetes and Vascular Disease Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE)9 did demonstrate that achievement of HbA1c by intensive management below 71 mmol/mol (6.5%) was able to further reduce nephropathy by about 20%, which may be translated into cardiovascular disease (CVD) risk reduction in the long run.10 Nevertheless, achieving low HbA1c targets by pharmaceutical intervention itself brings harm to patients. Such interventions may lead to more frequent hypoglycemia,7,8 which is related with high risk of CVD and all-cause mortality.11
Thus, a research question should be asked: whether factors other than drug treatments also contribute to good glycemic control in T2D. In this regard, a study showed that women with T2D were at higher risk of poor glycemic control and abnormal lipid metabolism than men.12 Obesity, insulin resistance, and metabolic syndrome are well established risk factors for diabetes13,14 but it is less certain whether obesity still plays a role in hyperglycemia control in drug-treated T2D. Low body height has been found associated with gestational diabetes mellitus (GDM) in Asian women,25,26 while no studies have attempted to examine the association between body height and glycemic control. Understanding associations of these factors with good glycemic control may help achieve better glycemic control and reduce the diabetes complications in the long run. Therefore, the current study aimed to explore non-drug factors for failure to achieve good glycemic control in Chinese women with T2D who used oral antidiabetic drugs (OADs) alone or combined with insulin.
Materials and methods
Patients
The Chinese Diabetes Society launched an HbA1c surveillance system among patients with T2D in mainland China in 2009. A total of 400 hospitals from 75 cities in 20 provinces, three autonomous regions, and four municipalities (Beijing, Shanghai, Tianjin, and Chongqing) directly under the central government agreed and participated in the surveillance system. The number of participating hospitals was increased to 414, with 81 cities in 30 provincial administrative regions of the People’s Republic of China in 2011, from all the provincial administrative regions in the People’s Republic of China except for Tibet. The ethics approval was obtained from People’s Liberation Army (PLA) General Hospital, and informed consent was obtained before collecting data from the patients.
The survey in 2011 was conducted from March to June 2011. The inclusion criteria were 1) being an outpatient with T2D mellitus being treated with OADs alone, OADs combined with insulin, or OADs combined with glucagon-like peptide (GLP)-1 receptor agonists; 2) aged 18 years and more; 3) with at least one previous outpatient medical record pertaining to diabetes; and 4) being a local resident for at least 6 consecutive months prior to participation in the study. The exclusion criteria included 1) diabetes secondary to other diseases; 2) type 1 diabetes; 3) on diet and other lifestyle therapy and/or Chinese herbal medicine only; 4) being pregnant or breast-feeding an infant; and 5) being unable to complete the survey due to mental diseases, unconsciousness, or inability to communicate.
During the recruitment period, health professionals (junior doctors, nurses or postgraduate medical students) sequentially screened patients with T2D for their eligibility. Those who met the inclusion criteria and did not have any of the exclusion criteria were invited to participate in the survey. The process continued until seven patients were successfully recruited in a consecutive way in each day and until 400 patients were recruited in the pre-specified period. After obtaining informed consent, the health professional(s) reviewed the medical notes, including the results of laboratory assays, and recorded the related data in a form. The retrieved data included sex, height, weight, blood pressure, and date of diagnosis of diabetes. Laboratory data on HbA1c and lipid profile were recorded. Specific information about the treatments used for the management of their T2D was documented, including the use of OADs (including dipeptidyl-peptidase (DPP) inhibitors and GLP-1 receptor agonists), and different types of insulin, as well as combinations of these antidiabetic drugs. Prior history of coronary heart disease, cerebrovascular disease, diabetic retinopathy, diabetic neuropathy, diabetic nephropathy, diabetes-related foot ulcers, and other complications diagnosed by secondary-care hospitals or tertiary hospitals were retrieved from medical notes, including dates of diagnosis of these medical conditions. A special staff member entered all the data and uploaded the entered data to the central database.
This analysis chose to analyze data of subjects recruited from the accredited 3A hospitals in four well-developed cities in the People’s Republic of China: Beijing, Shanghai, Tianjin, and Guangzhou. The 3A hospitals were the best hospitals that are assumed to provide quality care to patients with T2D. The reason to select 3A hospitals in four cities was that the coverage rates of the 3A hospitals were high and may be assumed to be representative of the population of patients with T2D cared by the top hospitals in the cities concerned. The coverage rates of the 3A hospitals were 74.4% for Beijing (n=32), 76% for Shanghai (n=22), 55% for Tianjin (n=11), and 29.3% for Guangzhou (n=12) after excluding those 3A hospitals that recruited less than 30 patients during the pre-specified recruitment period (n=2 for Beijing, n=2 for Tianjin, n=3 for Shanghai, and n=4 for Guangzhou). The recruitment goal was 400 patients by each hospital. A total of 13,970 women with T2D out of 29,502 patients recruited from the participating 3A hospitals from the four cities were used in the final analysis.
Statistical analysis
The Statistical Analysis System (SAS) release 9.3 (SAS Institute Inc., Cary, NC, USA) was used in all the data analysis. Data were expressed as mean (standard deviation [SD]) if normal distribution could not be rejected or median (25th to 75th percentile) if normal distribution was rejected by checking the Q-Q plot of the variable concerned. Chi-square test or Fisher’s exact test where appropriate was used to compare categorical variables, and Student’s t-test or Wilcoxon two-sample test where appropriate was used to compare continuous variables between two groups. Body mass index (BMI) was calculated as body weight in kilograms divided by squared body height in meters. Overweight and obesity were defined based on recommendations of the Chinese Diabetes Association (ie, BMI ≥24.0 but <28.0 kg/m2 being used to defined overweight, and ≥28.0 kg/m2 being used to define obesity).15 Duration of diabetes was calculated as the period from the date of diagnosis of diabetes to that of measurement of HbA1c. Quintiles of duration of diabetes and body height were used to check their V-shaped or J-shaped relations, if any, with hyperglycemia. The American Diabetes Association (ADA) recommended that the treatment target of HbA1c was <77 mmol/mol (7.0%),16 and HbA1c ≥77 mmol/mol (7.0%) was used to define hyperglycemia or poor glycemic control.
Logistic regression analysis on cities and 3A hospitals was used to obtain odds ratio (OR) of factors of interest for hyperglycemia in univariable and multivariable analysis. P-values <0.05 were considered to be statistically significant.
Results
The mean age of the women surveyed was 60.3 (SD 11.0) years, and they had a median duration of diabetes of 4 (25th to 75th percentiles: 2 to 9) years. The percentage of patients with poor glycemic control was 65.1% in the four cities combined, and also varied from city to city, with the highest percentage in Tianjin (76.3%), followed by Shanghai (69.2%), Beijing (62.4%), and Guangzhou (54.7%) (P<0.0001). Women with hyperglycemia had higher body height, higher BMI, longer duration of diabetes, and higher blood pressure, higher lipids (total cholesterol, triglyceride, and low-density lipoprotein (LDL)-cholesterol) and were less likely to use self-monitoring blood glucose (SMBG) (Table 1).
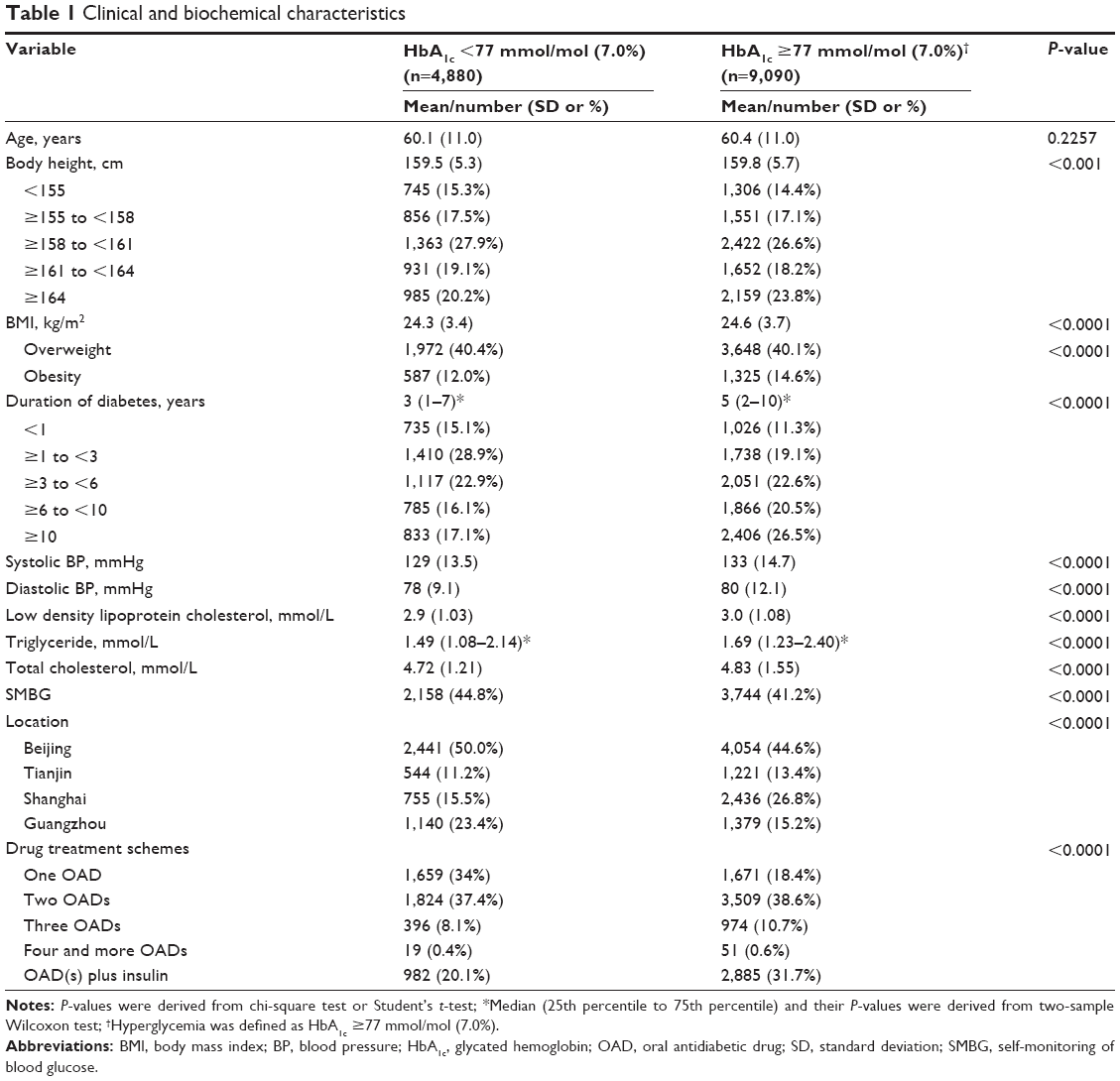 | Table 1 Clinical and biochemical characteristics |
In univariable analysis, obesity and body height ≥164 cm were associated with a higher risk of poor glycemic control, while SMBG in the last week was associated with lower risk of poor glycemic control. Duration of diabetes was associated with poor glycemic control in a J-shaped relation. Below 1 year and above 3 years of disease duration were all associated with increased risk of hyperglycemic control, with a marked increase for 10 and more years of duration of diabetes (Table 2).
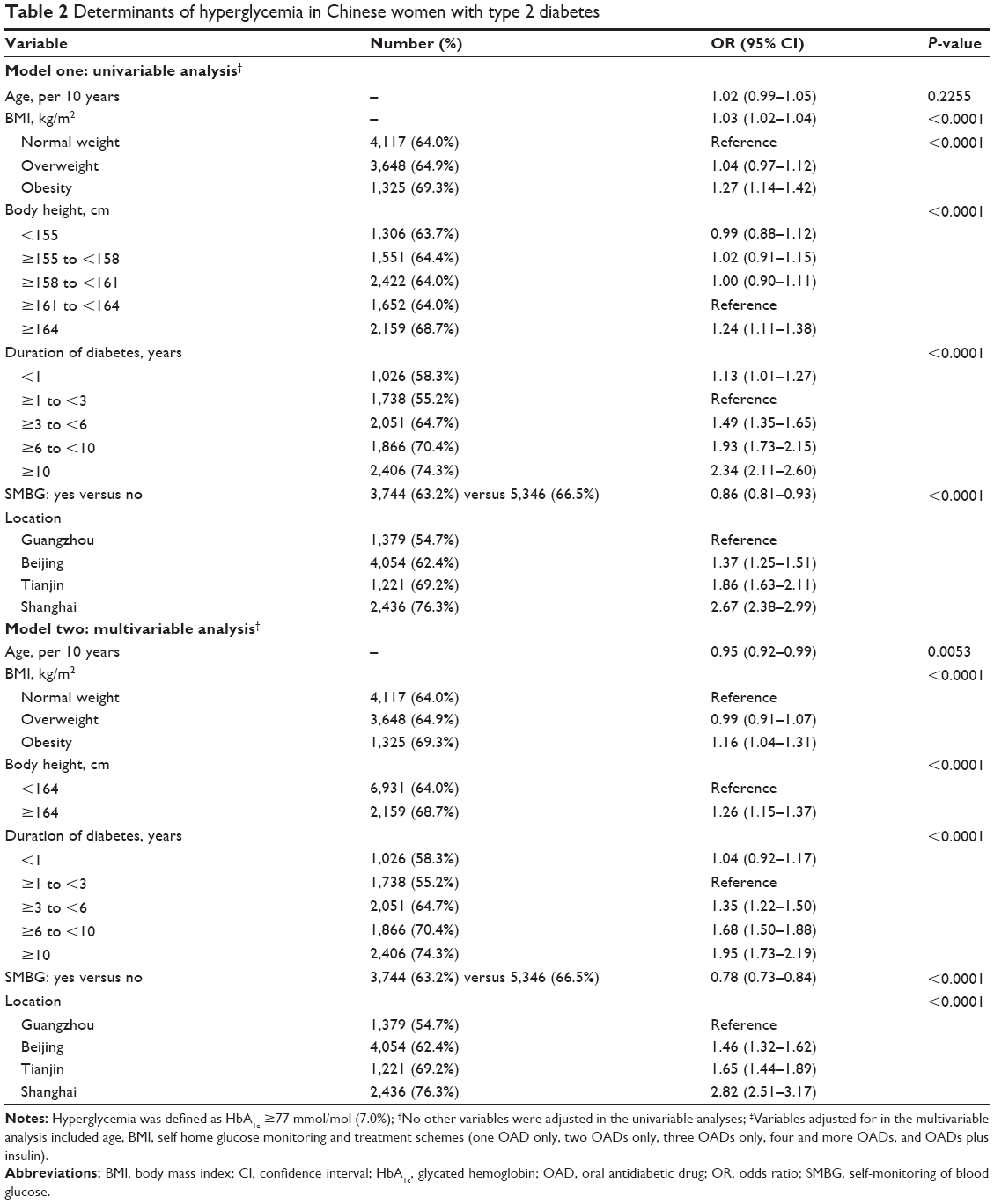 | Table 2 Determinants of hyperglycemia in Chinese women with type 2 diabetes |
After adjusting for covariates, the statistical significance for the association between obesity and poor glycemic control persisted, with an OR of 1.16 (95% confidence interval [CI] 1.04–1.31). Body height of ≥164 cm was also significantly associated with poor glycemic control (OR 1.26, 95% CI 1.15–1.37). Duration of diabetes ≥3 years but not <1 year increased the risk of poor hyperglycemia control, while SMBG was associated with lower risk of hyperglycemia (OR 0.78, 95% CI 0.73–0.84) (Table 2).
Age was not significant in univariable analysis, but in multivariable analysis, older age tended to reduce the risk of poor glycemic control. As compared with patients residing in Guangzhou, those patients residing in other cities were all at higher risk of poor glycemic control (Table 2).
Discussion
Although pharmaceutical treatment is the cornerstone in hyperglycemia control, we found that obesity, a body height of ≥164 cm and long duration of diabetes in OAD-treated T2D were independently associated with hyperglycemia, and use of SMBG helped achieve good glycemic control, highlighting the importance of obesity control and use of SMBG in the management of T2D.
Recent mega-trials caused concerns over the safety of intensive pharmaceutical intervention to achieve the further tight glycemic control, including increased risk of death and hypoglycemia, which itself may increase the risk of CVD and death.7–9,17 Epidemiological analysis of the ADVANCE trial data18 reconfirms the benefit to control HbA1c below 77 mmol/mol (7.0%) for macrovascular events and death, and below 71 mmol/mol (6.5%) for microvascular events. The ADA recommendation endorsed maintenance of the HbA1c target of 77 mmol/mol (7.0%).16 Pharmaceutical intervention plays an essential role in achieving the glycemic control target in T2D. Although tighter glycemic control was achievable in clinical trial settings,9 it is very difficult to achieve and maintain HbA1c <77 mmol/mol (7.0%) in real practice,19 as reflected by up to 65.1% of women with T2D in the survey not reaching the HbA1c target. These figures are consistent with a report that showed that 62.7% in Asia, 64% in Eastern Europe, and 64% in Latin America of patients with T2D failed to reach the HbA1c target.20 In that multi-region survey,20 old age, obesity (defined as BMI >30 kg/m2), longer duration of diabetes, and nonuse of SMBG were determinants of poor glycemic control as defined as HbA1c ≥77 mmol/mol (7.0%). The association between age and hyperglycemia appeared after the adjustment suggests that old age seemed to be a protective factor, probably through increased awareness with age. Obesity is associated with insulin resistance. Large diabetes prevention trials have shown that lifestyle intervention aiming at normalizing obesity reduces incidence of diabetes, establishing a causal role of obesity in T2D occurrence.21–23 In our study, obesity was associated with poor glycemic control in Chinese women with OAD-treated T2D, highlighting importance of maintaining normal body weight for achieving good glycemic control in T2D. Our study also quantified duration of diabetes for the risk of poor glycemic control and reported that hyperglycemia worsened from the third year of diagnosis of diabetes and deteriorated over time. Similar with the findings from UKPDS,24 the small increased risk of poor glycemic control in the first year of diagnosis of diabetes was likely to be confounded by other factors. On the other hand, gradual increase in the risk of hyperglycemia with increasing duration of diabetes since the third year of diagnosis of diabetes may reflect deterioration of beta-cell function.
Our study was the first reporting that body height of ≥164 cm was associated with poor glycemic control among women with T2D. Shorter body height, eg, <159 cm for Chinese pregnant women25 and <157 cm for Korean pregnant women,26 was associated with increased risk of GDM. Other studies reported that short leg length was related to insulin resistance and diabetes in multiple adult populations,27,28 suggesting a role of prepubertal growth in the etiology of diabetes.27 Differently from the relationship between body height and diabetes or GDM reported in other studies, we found that higher rather than shorter body height was associated with poor glycemic control. This group of women needs special attention, and more diabetes education is needed to help them to achieve the glycemic control target given to its benefits for micro- and macrovascular outcomes.5,6,9 The importance of SMBG for good glycemic control has been demonstrated by several observational29 and randomized controlled trials,30 which itself may be associated with reduced risk of morbidity and mortality.31 Our study reaffirmed that SMBG was useful for achieving good glycemic control among Chinese women with OAD-treated T2D.
Our study has strengths and limitations. The strength of the study is that the sample size was large and could detect factors for poor glycemic control with high sensitivity and accuracy. The OR reported in this study ranged from 1.35 to 1.95 for duration of diabetes and 0.78 for SMBG and 1.26 for body height, which may not be detectable by small sample sized studies. The first limitation was that the patients were outpatient female subjects with T2D who were seeking care from top tertiary hospitals in the four well-developed cities in the People’s Republic of China. They were not representative of all the women with T2D in the People’s Republic of China, especially those women under the care of community or primary-care hospitals. The findings cannot be extrapolated to patients with T2D under care by primary-care hospitals. The second limitation was that this study was a cross-sectional survey; time-relationships and causal relationships between these factors and hyperglycemia could not be established. Further cohort studies and trials are needed to verify our findings. The third limitation was that physical activity and diet data were not collected. It is unknown whether physical activity and diet mediated these associations.
In conclusion, the study found that obesity, body height of ≥164 cm, and duration of diabetes ≥3 years, especially ≥10 years, were associated with hyperglycemia, while use of SMBG decreased the risk of poor glycemic control. Our study highlights the importance of maintaining normal body weight and use of SMBG, and special attention needs to be given to patients with a longer duration of disease and/or a higher body height. Given the epidemic of diabetes in the world and a huge number of patients with T2D in the People’s Republic of China,1 understanding these non-drug treatment factors related with poor glycemic control may help control hyperglycemia and reduce the burden of T2D.
Acknowledgments
The authors thank those who were involved in the surveillance system for their efforts in data collection and quality control. This study was supported by a research grant from Novo Nordisk, People’s Republic of China.
Disclosure
All the authors except for XY received a grant from Novo Nordisk, People’s Republic of China. The authors have no other conflicts of interest in this work.
References
Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–321. | ||
Fioretto P, Dodson PM, Ziegler D, Rosenson RS. Residual microvascular risk in diabetes: unmet needs and future directions. Nat Rev Endocrinol. 2010;6(1):19–25. | ||
Laakso M. Cardiovascular disease in type 2 diabetes: challenge for treatment and prevention. J Intern Med. 2001;249(3):225–235. | ||
Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care. 2005;28(9):2130–2135. | ||
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–853. | ||
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. | ||
Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–2559. | ||
Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–139. | ||
Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–2572. | ||
Heller SR. A summary of the ADVANCE Trial. Diabetes Care. 2009;32(Suppl 2):S357–S361. | ||
Zoungas S, Patel A, Chalmers J, et al. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410–1418. | ||
Franzini L, Ardigo D, Cavalot F, et al. Women show worse control of type 2 diabetes and cardiovascular disease risk factors than men: results from the MIND. IT Study Group of the Italian Society of Diabetology. Nutr Metab Cardiovasc Dis. 2013;23(3):235–241. | ||
Ford ES, Schulze MB, Pischon T, Bergmann MM, Joost HG, Boeing H. Metabolic syndrome and risk of incident diabetes: findings from the European Prospective Investigation into Cancer and Nutrition-Potsdam Study. Cardiovasc Diabetol. 2008;7:35. | ||
He Y, Zhai F, Ma G, et al. Abdominal obesity and the prevalence of diabetes and intermediate hyperglycaemia in Chinese adults. Public Health Nutr. 2009;12(8):1078–1084. | ||
Chen C, Lu FC. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed Environ Sci. 2004;(Suppl 17): 1–36. | ||
American Diabetes Association. Standards of medical care in diabetes – 2013. Diabetes Care. 2013;36(Suppl 1):S11–S66. | ||
Riddle MC, Karl DM. Individualizing targets and tactics for high-risk patients with type 2 diabetes: practical lessons from ACCORD and other cardiovascular trials. Diabetes Care. 2012;35(10):2100–2107. | ||
Zoungas S, Chalmers J, Ninomiya T, et al. Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia. 2012;55(3): 636–643. | ||
Rosenthal ES, Bashan E, Herman WH, Hodish I. The effort required to achieve and maintain optimal glycemic control. J Diabetes Complications. 2011;25(5):283–288. | ||
Chan JC, Gagliardino JJ, Baik SH, et al. Multifaceted determinants for achieving glycemic control: the International Diabetes Management Practice Study (IDMPS). Diabetes Care. 2009;32(2):227–233. | ||
Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20(4):537–544. | ||
Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–1350. | ||
Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403. | ||
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853. | ||
Yang X, Hsu-Hage B, Zhang H, et al. Gestational diabetes mellitus in women of single gravidity in Tianjin City, China. Diabetes Care. 2002; 25(5):847–851. | ||
Jang HC, Min HK, Lee HK, Cho NH, Metzger BE. Short stature in Korean women: a contribution to the multifactorial predisposition to gestational diabetes mellitus. Diabetologia. 1998;41(7):778–783. | ||
Asao K, Kao WH, Baptiste-Roberts K, Bandeen-Roche K, Erlinger TP, Brancati FL. Short stature and the risk of adiposity, insulin resistance, and type 2 diabetes in middle age: the Third National Health and Nutrition Examination Survey (NHANES III), 1988–1994. Diabetes Care. 2006;29(7):1632–1637. | ||
Smith GD, Greenwood R, Gunnell D, Sweetnam P, Yarnell J, Elwood P. Leg length, insulin resistance, and coronary heart disease risk: the Caerphilly Study. J Epidemiol Community Health. 2001;55(12):867–872. | ||
Blonde L, Karter AJ. Current evidence regarding the value of self-monitored blood glucose testing. Am J Med. 2005;118(Suppl 9A): 20S–26S. | ||
Chen HS, Wu TE, Jap TS, Lin SH, Hsiao LC, Lin HD. Improvement of glycaemia control in subjects with type 2 diabetes by self-monitoring of blood glucose: comparison of two management programs adjusting bedtime insulin dosage. Diabetes Obes Metab. 2008;10(1):34–40. | ||
Martin S, Schneider B, Heinemann L, et al. Self-monitoring of blood glucose in type 2 diabetes and long-term outcome: an epidemiological cohort study. Diabetologia. 2006;49(2):271–278. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.