Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 10
Minimal recovery time needed to return to social engagement following nasolabial fold correction with hyaluronic acid fillers produced with XpresHAn technology
Authors Swift A, von Grote E, Jonas B ![]() , Nogueira A
, Nogueira A
Received 28 March 2017
Accepted for publication 5 May 2017
Published 14 June 2017 Volume 2017:10 Pages 229—238
DOI https://doi.org/10.2147/CCID.S138155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Arthur Swift,1 Erika von Grote,2 Brandie Jonas,2 Alessandra Nogueira2
1Arthur Swift Research Inc., Montreal, QC, Canada; 2Medical Affairs, Galderma Laboratories, L.P., Fort Worth, TX, USA
Introduction: The appeal of hyaluronic acid fillers for facial soft tissue augmentation is attributable to both an immediate aesthetic effect and relatively short recovery time. Although recovery time is an important posttreatment variable, as it impacts comfort with appearance and perceived treatment benefit, it is not routinely evaluated. Natural-looking aesthetic outcomes are also a primary concern for many patients.
Materials and methods: A single-center, noncomparative study evaluated the time (in hours) until subjects return to social engagement (RtSE) following correction of moderate and severe nasolabial folds (NLFs) with RR (Restylane® Refyne) and RD (Restylane® Defyne), respectively. Twenty subjects (aged 35–57 years) who received bilateral NLF correction documented their RtSE and injection-related events posttreatment. Treatment efficacy was evaluated by improvements in Wrinkle Severity Rating Scale (WSRS) and subject satisfaction questionnaire at days 14 and 30, and by Global Aesthetic Improvement Scale (GAIS) at day 30. Safety was evaluated by injection-related events and treatment-emergent adverse events.
Results: Fifty percent of subjects reported RtSE within 2 hours posttreatment. WSRS for the RR group improved significantly from baseline at day 14 (–1.45±0.42) and day 30 (–1.68±0.46) (P<0.001), respectively. WSRS for the RD group improved significantly from baseline at day 14 (–2.22±0.44) and day 30 (–2.50±0.50) (P<0.004), respectively. All GAIS improvements were clinically significant at day 30. The majority of injection-related events were mild or moderate. Two subjects experienced 3 related treatment-emergent adverse events; 1 RR subject experienced severe bruising, and 1 RD subject experienced severe erythema and mild telangiectasia. Subject satisfaction was high regarding aesthetic outcomes and natural-looking results.
Conclusion: Optimal correction of moderate NLFs with RR and severe NLFs with RD involved minimal time to RtSE for most subjects. Treatments that significantly improved WSRS and GAIS, were generally well-tolerated, and provided natural-looking aesthetic outcomes.
Keywords: hyaluronic acid, dermal filler, nasolabial fold, recovery time, naturalness
Introduction
Facial rejuvenation with nonpermanent hyaluronic acid (HA) fillers is a safe and effective aesthetic procedure for patients seeking to maintain a youthful appearance. The number of minimally invasive (nonsurgical) procedures using HA fillers has surged from 1,670,650 to 2,865,086 worldwide within the past 5 years.1 The appeal of these procedures is due to the immediate aesthetic effect and the relatively short recovery time involved.2,3 Treatment-related recovery time is an important factor for patients considering treatment and likely impacts their decision in scheduling treatment. Although typically short-term, common injection site reactions can potentially include bruising, itching, pain/tenderness, redness, and swelling and may impact the duration of posttreatment recovery time.4 It is speculated, that return to social engagement (RtSE) is affected by the appearance of common injection site reactions, some of which have been directly linked to injection speed and injection volume.5
Patients also want discrete treatment results that do not alter the natural character or individuality of their facial expressions.6 A recent patient survey revealed that a fear of losing natural expressiveness and loss of facial mobility were among the concerns regarding facial treatment outcomes.6 Although HA fillers can improve the static appearance of wrinkles and furrows, there is no guarantee that the product’s benefit will accommodate natural facial movements.
In the past decade, HA filler product innovation has greatly increased the range of HA products with respect to the manufacturing processes which impact their physicochemical properties and clinical performance.7,8 By varying the degree of HA cross-linking, gel firmness can be fine-tuned to suit a specific indication, provide firmer volume in deep dermis, or provide softer volume in the papillary/reticular dermis.9
The RR (Restylane® Refyne) and RD (Restylane® Defyne) (Galderma S.A., Lausanne, Switzerland) products are 20 mg/mL HA dermal fillers which received CE mark in Europe in 2008. The products are produced with the XpresHAn Technology™ (known as OBT™ outside the US) with a range of HA cross-linking and gel calibration (particle size), differentiating the products by softness and flexibility to provide a product option more tailored for each indication.10 Both RR and RD are approved for injection into the mid-to-deep dermis for the correction of moderate-to-severe wrinkles and folds, such as nasolabial folds (NLFs). The RR gel is calibrated to provide a softer gel with smaller particles in comparison with RD, for less severe wrinkles and folds. The firmer texture and larger particle size of RD make it well-suited for the correction of more prominent wrinkles and folds.
Two large randomized, evaluator-blinded, active comparator-controlled, multicenter studies, were conducted to assess the safety and efficacy of RR and RD in the treatment of NLFs.11,12 Both studies compared RR and RD with dermal fillers of similar indications and demonstrated product safety and efficacy results in 18- and 12-month follow-up periods, respectively. A survey spanning a 10-month period was conducted with 58 clinicians to evaluate the immediate (and up to 15 months posttreatment) injection site reactions and adverse events (AEs) of 1,806 patients treated for correction of mild-to-moderate NLFs, 47% of whom received RR or RD, or a combination of both. The average baseline wrinkle severity for the total patient population was 2.4±1.1 and was based on an ascending severity score of 1–5).13 The survey results showed that patients were treated with a bilateral injection volume of 1.0±0.6 mL using a linear retrograde technique in 89.3% of patients, a combined technique (linear retrograde + multipuncture) in 5.4% of patients, and a multipuncture technique alone in 5.3% of patients.
Ninety percent of all patients in the survey had a score of less than “1” (based on an ascending severity scale of 0–4) for erythema, bruising, edema, and pain, and more than 60% had a score of “0” for these criteria, and no serious adverse events were reported for up to 15 months posttreatment.
The RR and RD products are designed to provide the degree of softness and flexibility appropriate to their indications and are well-tolerated when used for the treatment of facial wrinkles and folds such as NLFs, an important factor for patients considering facial soft tissue augmentation. The primary aim of the present open-label, single-center study was to evaluate the posttreatment recovery time duration until subjects reported feeling comfortable RtSE following optimal bilateral correction (≥1-grade improvement) of moderate NLFs with RR or severe NLFs with RD.
Materials and methods
Subjects and inclusion/exclusion criteria
All subjects who provided written consent to participate were enrolled in the study based on the following inclusion and exclusion criteria. Inclusion criteria was men and women aged 35–60 years with bilateral NLFs rated as 3 (moderate) or 4 (severe), as assessed by the treating investigator, and based on the Wrinkle Severity Rating Scale (WSRS).
A brief list of exclusion criteria included subjects who
- had severe midface volume loss or a wrinkle/fold severity that required other treatments (laser treatment or chemical peeling) to achieve optimal correction;
- had previous tissue-revitalization treatment with neurotoxin, laser or light, mesotherapy, chemical peeling, or dermabrasion below the zygomatic arch within 6 months;
- had tissue-augmenting therapy with nonpermanent filler or fat injection in the facial area to be treated within 12 months;
- had previous tissue augmenting therapy or contouring with a permanent filler-type injectable product (ie, polymethyl methacrylate);
- had a known hypersensitivity to lidocaine, hyaluronic acid, gram-positive bacterial proteins, a history of porphyria, or severe or multiple allergies manifested by anaphylaxis;
- had a tendency to develop keloids, hypertrophic scars, or any healing disorders; and
- had a history of social anxiety disorder or other psychiatric disorder that may affect study participation.
Treatments
Subjects received optimal bilateral correction of NLFs with up to 2 mL per NLF per treatment session (total volume up to 4 mL) of either RR or RD using a 30G × ½″ or 27G × ½″ needle, respectively.
Study design
This single-center, noncomparative, pilot study was approved by Quorum Review Institutional Review Board, a central institutional review board, and conducted in accordance with the guidelines for standard clinical practice and the Declaration of Helsinki (Clinical Trial #02672644). The study’s primary objective was to evaluate the duration of subject-reported time (in hours) until their RtSE following optimal bilateral correction of NLFs using RR or RD. The definition of RtSE was described as making public and social appearances, such as returning to a public place of work, having dinner in a public restaurant, attending a social event or gathering, etc. Subjects were instructed that RtSE was based on when they felt comfortable resuming social interactions, and not necessarily the time of the first social engagement after treatment.
Secondary study objectives included evaluation of NLF severity by the treating investigator using the WSRS, investigator and subject assessment of NLF improvement using the Global Aesthetic Improvement Scale (GAIS), subject satisfaction with treatment outcomes by questionnaire, the RtSE following optional touch-up treatments; local tolerability of injection-related events (IREs) documented by safety assessments and subject diary entries, and treatment-emergent adverse events (TEAEs) documented throughout the study.
The study consisted of up to 4 visits: screening (visit 1), baseline/day 1 (visit 2, initial treatment), day 14/optional touch-up (visit 3), and day 30/study exit (visit 4). The screening visit and first treatment visit could be combined as 1 visit. Prior to initial treatment, full-face photographs of subjects’ neutral expressions (frontal and left/right oblique views) were captured and baseline investigator-assessed WSRS and subject satisfaction were assessed prior to treatment. Following treatment, 14-day diaries were dispensed to the subjects. Subjects were asked to maintain the diary documenting local tolerability symptoms, and the earliest time they felt comfortable (with or without covering makeup) to RtSE.
On day 14, subjects returned for safety monitoring, investigator-assessed WSRS, and completion of a satisfaction questionnaire. Optional touch-up injections were administered to those subjects who did not achieve optimal correction with the initial treatment. Subjects receiving touch-ups were asked to complete an additional 14-day diary documenting local tolerability symptoms and time until RtSE. On day 30/study exit, subjects returned to the site for safety monitoring, facial photographs, investigator-assessed WSRS, investigator- and subject-assessed GAIS, and completion of a subject satisfaction questionnaire. Throughout the study (days 1, 14, and 30), IREs and any potential TEAEs were monitored by observation and diary entries.
Treatment procedures were conducted as follows: all subjects were treated to optimal correction, which consisted of at least a 1-grade bilateral NLF improvement (reduction) in wrinkle severity with either RR (for moderate NLFs, WSRS =3) or RD (for severe NLFs, WSRS =4). Only 1 product was used per subject, which was injected into the mid-to-deep dermis (on-label) using a linear threading or serial puncture technique. For this study, the use of cannulas and layered injection technique was not permitted. Following treatment, injection sites were gently massaged by the treating investigator to conform to the contour of the surrounding tissues. Topical cooling was applied to reduce initial swelling, and subjects were asked to avoid exposing the treated area to heat or extreme cold until any signs of local inflammation had subsided. Subjects were also asked to avoid covering the injection sites with makeup for 24 hours posttreatment to minimize any possibility of infection.
All injections were completed by noon on the day of treatment to standardize the reporting window for the time to RtSE across subjects and to facilitate the opportunity for RtSE throughout the remainder of the day.
Efficacy and safety assessment
The primary efficacy analysis was based on the time in hours from the end of the initial treatment procedure on day 1 until the earliest time subjects felt comfortable with RtSE and included all subjects who received bilateral treatment and completed at least 1 posttreatment assessment. Also, the number and percent of subjects who felt comfortable with RtSE were categorized within specified time frames (≤2, ≤8, ≤24, ≤48, and >48 hours) following the initial treatment procedure on day 1 and summarized by product and overall.
Secondary efficacy analyses included: 1) investigator-assessed WSRS by live evaluation of the length and depth of each NLF using the validated WSRS photonumeric grading scale (1= absent; 2= mild; 3= moderate; 4= severe; 5= extreme),14 with a change of at least 1-grade improvement (reduction) from the live evaluation performed at baseline, representing a clinically significant improvement; 2) investigator- and subject-assessed GAIS using a 5-grade scale (“worse,” “no change,” “somewhat improved,” “much improved,” or “very much improved”)15 with a score of “somewhat improved,” “much improved,” or “very much improved” representing a clinically significant improvement; 3) a 9-item subject satisfaction questionnaire using a 5-point Likert scale (1= strongly disagree; 2= disagree; 3= neutral; 4= agree; 5= strongly agree); and 4) the time in hours to RtSE following optional touch-up treatment. Exploratory endpoints included evaluation of RtSE and total injection volume relationship.
Safety assessments included AEs, TEAEs, serious AEs, AEs leading to withdrawal, any deaths, pregnancies, use of concomitant medications, and IREs. The IREs were evaluated by observation and by subject diary entries regarding the presence and severity of predefined expected injection-related events (redness, swelling, pain, itching, bruising, and tenderness) at the injection sites. The following 3-point scale was used: 1= mild, “awareness of symptoms or signs, but easily tolerated (acceptable)”; 2= moderate, “enough discomfort to interfere with usual activity (disturbing)”; or 3= severe, “incapacity to work or to do usual activity (unacceptable).” TEAEs were collected throughout the study.
Statistical analysis
The full analysis set was the primary population for all efficacy analyses and included all subjects treated in both NLFs and who had at least 1 posttreatment assessment performed. The per-protocol population included all subjects in the full analysis set who did not have any major protocol violations. The safety population included all subjects treated with any amount of product.
Results
A total of 20 subjects (aged 35–57 years) were included in the full analysis set and safety population. The majority of subjects were females (95.0%) with a mean age of 49.4 (±5.6) years. At baseline, all subjects had bilaterally symmetrical NLFs with a mean WSRS score of 3 in the RR group and 4 in the RD group. The subject demographics and baseline WSRS characteristics are summarized in Table 1.
 | Table 1 Subject demographics and BL NLF wrinkle rating severity scores Notes: aAverage WSRS was calculated from the individual left and right scores. If the WSRS was only available for 1 side, then the average WSRS was the score for 1 side. Abbreviations: BL, baseline; n, number of subjects; NLF, nasolabial fold; RR, Restylane® Refyne; RD, Restylane® Defyne; SD, standard deviation; WSRS, Wrinkle Severity Rating Scale. |
Overall, 50.0% of the total subject population reported RtSE within 2 hours and 55.0% within 8 hours following treatment (Figure 1A). In less than 4 days posttreatment, 90.0% of subjects reported RtSE. In the RR group, 8 subjects (72.7%) reported RtSE within 2 hours of treatment, which increased to 10 subjects (90.9%) by 2 days posttreatment (Figure 1B). The RtSE timeframes for the 10 subjects who received a touch-up treatment at day 14 ranged from 0 to 2 hours for 6 subjects to more than 48 hours for 1 subject. In the RR group, a greater majority of subjects (4/6) reported RtSE within 2 hours compared to subjects in the RD group (2/4) (Figure 2).
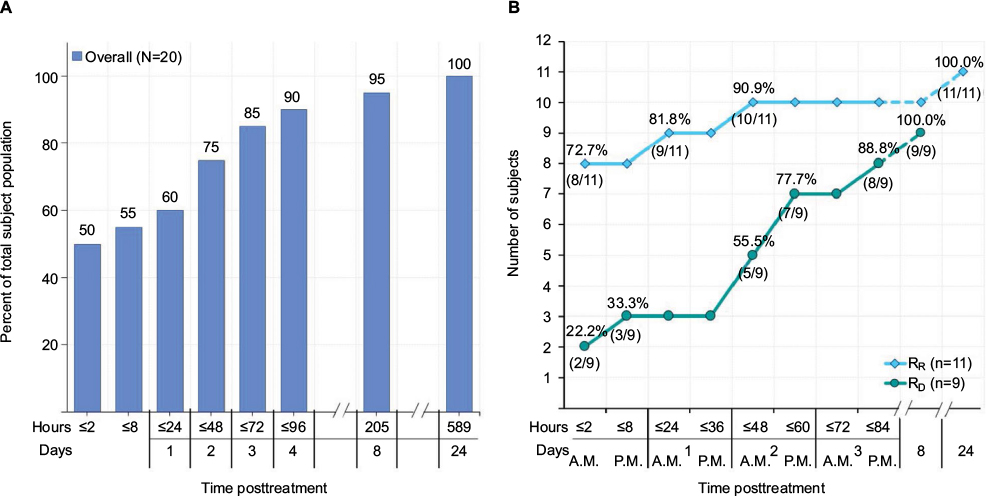 | Figure 1 Timeframes to RtSE after initial treatment. Notes: (A) Overall RtSE in hours and days posttreatment. (B) RtSE by product in hours and days posttreatment. Abbreviations: n, number of subjects; RR, Restylane® Refyne; RD, Restylane® Defyne; RtSE, Return to Social Engagement. |
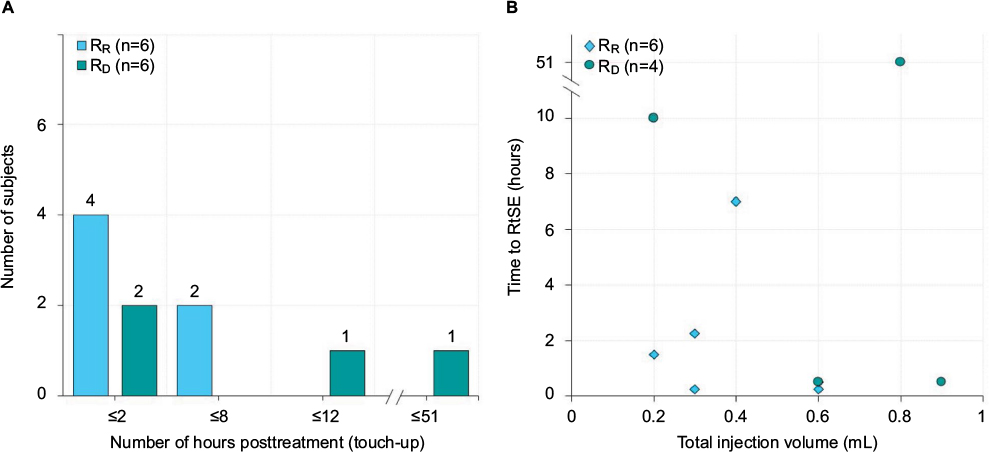 | Figure 2 Timeframes for RtSE and corresponding injection volumes following touch-up treatment on day 14. Notes: (A) Timeframes for RtSE; (B) RtSE times corresponding with injection volumes. Volume of injection is the sum of the injected volume in both right and left NLF, with a maximum volume of 2 mL per NLF, per treatment session (ie, a total of 4 mL per injection session). Abbreviations: n, number of subjects; NLF, nasolabial fold; RR, Restylane® Refyne; RD, Restylane® Defyne; RtSE, return to social engagement. |
One subject in the RR group with a TEAE (severe bruising) did not report RtSE until 24 days posttreatment. In the RD group, 7 subjects (77.7%) reported RtSE by the evening of the 2nd-day posttreatment, which increased to 8 subjects (88.8%) by the evening of the 3rd-day posttreatment (Figure 1B). One subject in the RD group with 2 TEAEs (severe erythema and mild telangiectasia) did not report RtSE until 8 days posttreatment. The single subject in the RR group, with RtSE of 24 days (589.3 hours), drove the mean values higher for the RR group and the overall RtSE average (Table 2). The group mean results for both the RR and RD subjects were similar, with a mean time of 60.4 and 56.9 hours, respectively. The mean RtSE for the overall population (all subjects) was 58.8 hours.
 | Table 2 Mean (SD) time to RtSE after initial treatment Notes: aP-value comparing the mean RtSE between treatment groups calculated using a two-sample t-test. Abbreviations: CI, confidence interval; max, maximum; min, minimum; n, number of subjects; RR, Restylane® Refyne; RD, Restylane® Defyne; RtSE, return to social engagement; SD, standard deviation. |
The overall proportion of subjects with a WSRS score reflecting a ≥2-grade improvement at day 30, relative to baseline, was 75.0% (Figure 3A). Relative to baseline, the overall mean (SD) reduction in WSRS scores at days 14 and 30 were –1.80 (0.57) (P<0.001) and –2.05 (0.62) (P<0.001), respectively (Figure 3B). Seven subjects (63.6%) in the RR group and 8 subjects (88.9%) in the RD group had a ≥2-grade improvement at day 30, relative to baseline. In the RR group, the mean (SD) WSRS scores decreased from baseline by –1.45 (0.42) (P<0.001) at day 14 and by –1.68 (0.46) (P<0.001) at day 30. In the RD group, the mean (SD) WSRS scores decreased from baseline by –2.22 (0.44) at day 14 (P<0.004) and by –2.50 (0.50) (P<0.004) at day 30 (Figure 3B).
 | Figure 3 Proportion of subjects with 1- and 2-grade improvements in bilateral WSRS scores at day 14 and day 30, relative to baseline. Notes: (A) Number of subjects with 1- and 2-grade improvement. aDefined as both NLFs at least a 1-grade reduction from baseline; bDefined as both NLFs at least a 2-grade reduction from baseline. (B) Mean (SD) reduction in WSRS by visit. *P-value calculated for mean reductions within each treatment group using the Wilcoxon signed-rank test. Abbreviations: NLF, nasolabial fold; n, number of subjects; RR, Restylane® Refyne; RD, Restylane® Defyne; SD, standard deviation; WSRS, Wrinkle Severity Rating Scale. |
All 20 subjects were rated with a clinically significant improvement in GAIS at day 30, relative to baseline, as reported by treating investigator and subjects (Figure 4). The treating investigator rated 15 subjects (75.0%) as “very much improved,” and 5 subjects (25.0%) as “much improved.” Half of all subjects (50.0%) rated their NLFs as “very much improved,” 7 subjects (35.0%) as “much improved,” and 3 subjects (15.0%) as “somewhat improved.” The majority of subjects “agree” or “strongly agree” to all questionnaire statements regarding satisfaction with the aesthetic outcome at day 14 and day 30 (Figure 5). At day 30, subjects agreed with the statement that their face had a pleasing appearance overall (85.0%), that they felt attractive (75.0%), and that they looked more like the way they felt (70.0%). The majority of subjects (90.0%) at day 30 also agreed that their face looked natural when smiling and when relaxed.
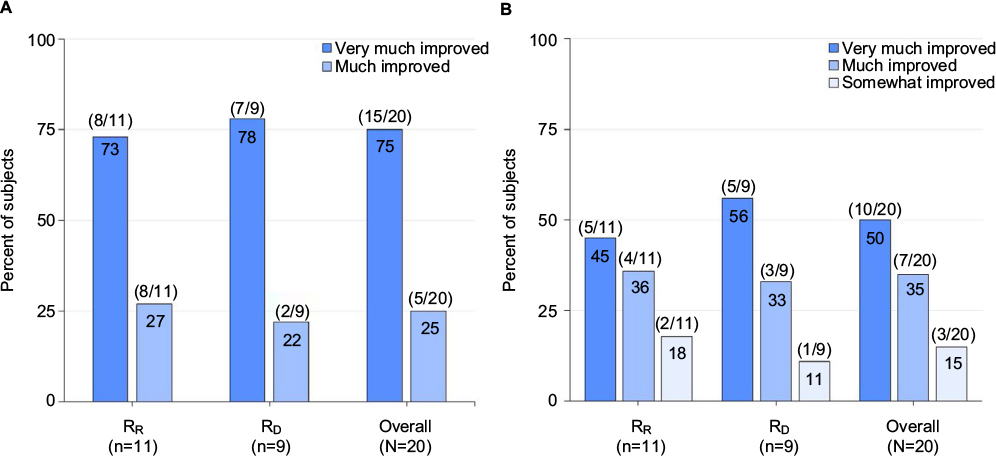 | Figure 4 Proportion of clinically significant improvement on the GAIS at day 30, relative to baseline. Note: (A) Treating investigator-accessed GAIS; (B) Subject-accessed GAIS. Clinically significant improvement defined as “very much improved”, “much improved”, or “somewhat improved”. Abbreviations: n, number of subjects; GAIS, Global Aesthetic Improvement Scale; RR, Restylane® Refyne; RD, Restylane® Defyne. |
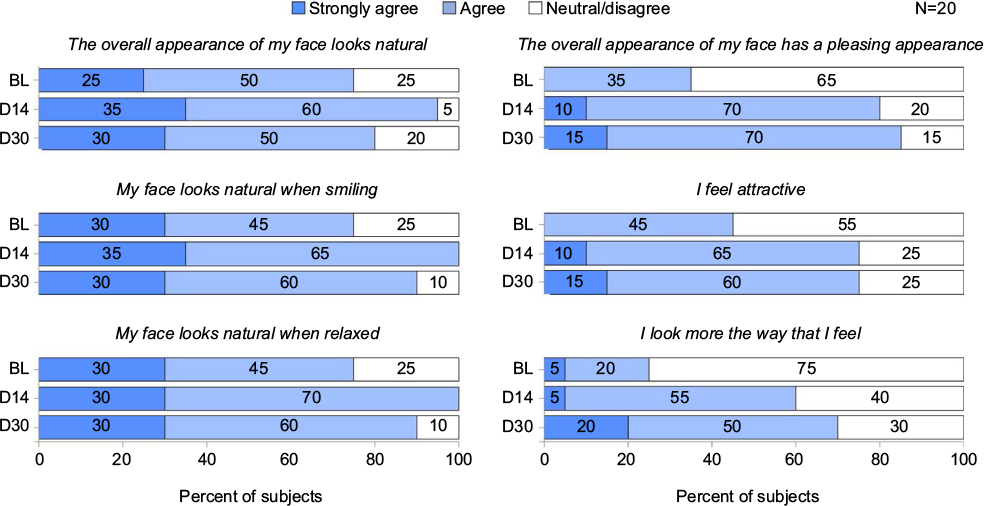 | Figure 5 Overall subject satisfaction with aesthetic outcomes at day 14 and day 30, relative to baseline. Abbreviations: BL, baseline; D14, day 14; D30, day 30. |
Nineteen subjects experienced at least 1 of the predefined IREs (Table 3). The most frequent IRE overall was redness (80.0%), followed by bruising and swelling (both 75.0%), tenderness (60.0%), itching (55.0%), and pain (35.0%). Overall, 65.0% of all IREs were mild, 27.0% were moderate, and 8.0% were severe. Four TEAEs were reported in 3 subjects, 1 of which was considered unrelated to treatment. One subject in the RR group experienced severe implant site bruising, and 1 subject in the RD group experienced severe erythema and mild telangiectasia.
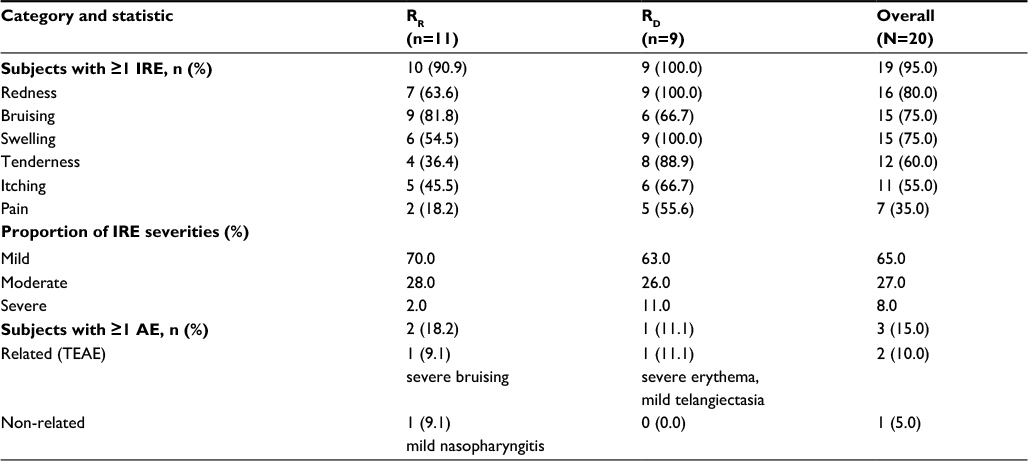 | Table 3 IREs and TEAEs Note: Adverse events are coded using MedDRA version 18.1. Abbreviations: AE, adverse event; IREs, injection-related events; n, number of subjects; RR, Restylane® Refyne; RD, Restylane® Defyne; TEAEs, treatment-emergent adverse events. |
The RtSE times corresponding with total injection volumes after initial treatment indicated a greater time duration for those subjects treated with RD, as well as for those subjects receiving ≥2 mL as a total injection volume (Figure 6).
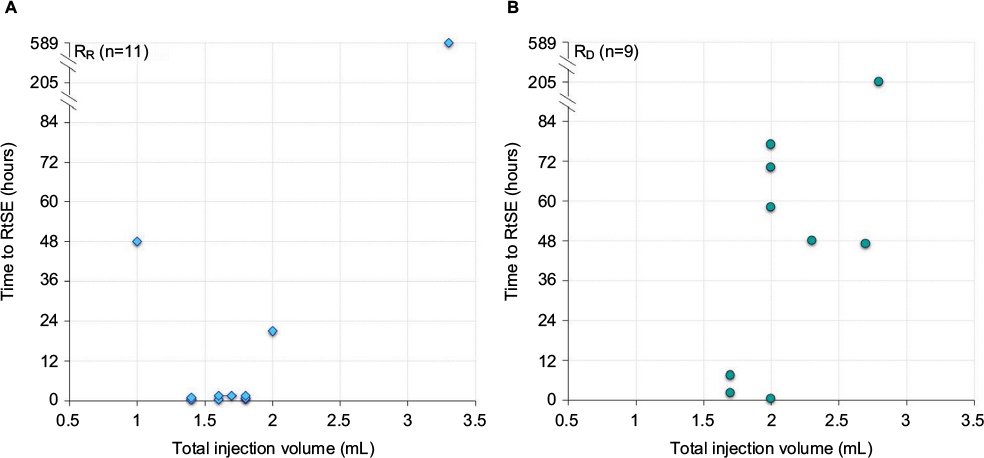 | Figure 6 Timeframes for RtSE and corresponding injection volumes after initial treatment on day 1, by product and total injection volume. Note: (A) RtSE and Injection Volumes for RR subjects; (B) RtSE and Injection Volumes for RD subjects. Volume of injection is the sum of the injected volume in both right and left NLF during initial injection, with a maximum volume of injected 2 mL per NLF, per injection session (ie, a total of 4 mL per injection session). Abbreviations: n, number of subjects; NLF, nasolabial fold; RR, Restylane® Refyne; RD, Restylane® Defyne; RtSE, return to social engagement. |
Discussion
The primary purpose of this study was to evaluate the earliest time (in hours) a subject reported feeling comfortable RtSE following optimal bilateral correction of NLFs with up to 2 mL per NLF (up to 4 mL per treatment session) with RR or RD. The baseline WSRS characteristics of the RR and RD subjects were rated as 3/3 and 4/4, respectively. The distribution of the RtSE data by time points showed subjects treated with RR required less recovery time and had a shorter duration to RtSE than those subjects treated with RD. The majority of subjects (8/11) treated with RR reported RtSE within the same day of treatment, while only 3 of 9 subjects treated with RD reported RtSE in that same timeframe.
A RtSE of greater than 24 hours was reported by 2 RR and 6 RD subjects. Notably, 2 of the 11 RR and 7 of the 9 RD subjects had received injection volumes of ≥2 mL, a factor which seemed to be associated with a longer duration of time prior to RtSE (Figure 2). Although 1 RR subject who received >2 mL had a baseline WSRS of 3 for both left and right NLF, a total injection volume of 3.3 mL was ultimately required to achieve optimal results during initial treatment. Of all study subjects, 3.3 mL was the greatest volume administered during a single treatment session during the study. Consequently, this subject reported the longest time duration to RtSE (24 days). The remaining 10 subjects in the RR group were all treated with ≤2 mL during their initial treatment. Overall, 19 subjects experienced at least 1 IREs, though the majority of IREs were reported as mild in severity. Treatment with RR and RD was generally found to be well-tolerated, which was consistent with findings of previous studies.
For subjects treated with RD, optimal correction of NLFs required a volume of ≥2 mL by 7 out of 9 subjects. All subjects achieved optimal NLF correction by day 30, demonstrated by 7 RR subjects and 8 RD subjects achieving a bilateral 2-point reduction, and 4 RR subjects and 1 RD subject achieving a bilateral 1-point reduction in WSRS by day 30. The treating investigator also reported 100% of subjects had a clinically significant improvement per the GAIS assessment.
A high level of patient satisfaction with treatment outcomes is the goal in aesthetic dermatology, and the concern to maintain a natural look is a crucial factor in the pursuit of treatment for many patients. The concept of facial appearance as “natural” is multidimensional (ie, youthful, rested, happy) and may be a difficult objective around which to tailor a treatment approach. There are several unifying themes of facial aging that are relevant to how facial naturalness may be perceived. As the midface ages, the underlying volume is gradually lost due to atrophy of the fat pads (deep and superficial) and the retaining connective tissues that hold them in place.16 The malposition of the remaining cheek volume no longer resists the dynamic movements of the muscles in the same way, which leads to more exaggerated expression folds and lines, and may appear to some as more of a caricature than a natural look. By restoring underlying volume, and thereby the skin’s resistance to deformation, the skin may move in a more synchronized manner with surrounding muscle strain and may be key in what constitutes a natural look at rest and during movement.
Interestingly, in comparison with baseline responses, a higher percentage of overall subjects “strongly agreed” or “agreed” that their face not only looked more natural overall (95% at day 14 and 80% at day 30, vs 75% at baseline) but also looked more natural when smiling (100% at day 14 and 90% at day 30, vs 75% at baseline) and when relaxed (100% at day 14 and 90% at day 30, vs 75% at baseline) (Figure 2). The majority of subjects also reported that they looked more like the way they felt (60% at day 14 and 70% at day 30, vs 25% at baseline).
The results of this study demonstrate that optimal correction of NLFs with RR and RD can provide clinically significant aesthetic improvement and RtSE within the same day for treatment of less severe NLFs. For the purposes of this study, subjects were required to avoid wearing covering makeup at the injection sites for 24 hours posttreatment to minimize any possibility of infection. The contributing authors believe that this posttreatment provision may have contributed to a longer delay in subject’s RtSE, and this does not reflect real-life situations where patients do apply foundation posttreatment in order to return to normal social activities immediately. In this light, the study results may be even more reassuring, since 10 of the 20 subjects indicated that they were comfortable with RtSE within 2 hours posttreatment without covering makeup.
The particular limitations of this study are attributable to its design, which was limited to a small number of subjects in each treatment group and use of an open-label and nonblinded evaluator. Additional studies designed with a greater number of subjects, a greater range of products (physicochemical properties), and additional exploration into the effect of injection volume may enhance the understanding of the factors that may affect a patient’s RtSE. A more in-depth evaluation of a subject’s comfort with RtSE vs their actual RtSE may also help clarify the factors affecting recovery times and help clinicians manage patient expectations.
Conclusion
Treatment with any filler is associated with a risk of IREs and TEAEs, the severity of which may impact the time duration to RtSE. Understanding the posttreatment recovery time associated with different injection techniques and fillers is essential for injectors to reduce the risk of IREs and improve patient outcomes. The results of this study demonstrate that treatment of moderate NLFs with RR and severe NLFs with RD involves minimal recovery time (ie, RtSE within same day of treatment) for the majority of subjects, significant improvement in WSRS, provides a high degree of clinician and subject satisfaction as demonstrated by GAIS, and provides the natural-looking aesthetic outcome that is a primary concern for many patients.
Disclosure
Drs Erika von Grote and Alessandra Nogueira are employees of Galderma Laboratories, L.P., Fort Worth, TX; Dr Arthur Swift is a paid investigator and speaker for Galderma Laboratories, L.P. The authors report no other conflicts of interest in this work.
References
ISAPS [homepage on the Internet]. ISAPS global statistics. Available from: www.isaps.org/news/isaps-global-statistics. Accessed September 9, 2016. | ||
Carruthers A, Carruthers J. Non-animal-based hyaluronic acid fillers: scientific and technical considerations. Plast Reconstr Surg. 2007;120(Suppl 6):33S–40S. | ||
Carruthers J, Cohen SR, Joseph JH, Narins RS, Rubin M. The science and art of dermal fillers for soft-tissue augmentation. J Drugs Dermatol. 2009;8(4):335–350. | ||
Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Plast Surg Nurs. 2015;35(1):13–32. | ||
Glogau RG, Kane MA. Effect of injection techniques on the rate of local adverse events in patients implanted with nonanimal hyaluronic acid gel dermal fillers. Dermatol Surg. 2008;34(Suppl 1):S105–S109. | ||
Michaud T, Gassia V, Belhaouari L. Facial dynamics and emotional expressions in facial aging treatments. J Cosmet Dermatol. 2015;14(1):9–21. | ||
Micheels P, Sarazin D, Tran C, Salomon D. Effect of different crosslinking technologies on hyaluronic acid behavior: a visual and microscopic study of seven hyaluronic acid gels. J Drugs Dermatol. 2016;15(5):600–606. | ||
Kablik J, Monheit GD, Yu L, Chang G, Gershkovich J. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol Surg. 2009;35(Suppl 1):302–312. | ||
Molliard GS, Albert S, Mondon K. Key importance of compression properties in the biophysical characteristics of hyaluronic acid soft-tissue fillers. J Mech Behav Biomed Mater. 2016;61:290–298. | ||
Segura S, Anthonioz L, Fuchez F, Herbage B. A complete range of hyaluronic acid filler with distinctive physical properties specifically designed for optimal tissue adaptations. J Drugs Dermatol. 2012;11(Suppl 1):S5–S8. | ||
Rzany B, Bayerl C, Bodokh I, et al. An 18-month follow-up, randomized comparison of effectiveness and safety of two hyaluronic acid fillers for treatment of moderate nasolabial folds. Dermatol Surg. 2017;43(1):58–65. | ||
Ascher B, Bayerl C, Kestemont P, Rzany B, Edwartz C, Podda M. A 12-month follow-up, randomized comparison of effectiveness and safety of two hyaluronic acid fillers for treatment of severe nasolabial folds. Dermatol Surg. 2017;43(3):389–395. | ||
Farhi D, Trevidic P, Kestemont P, et al. The Emervel French survey: a prospective real-practice descriptive study of 1,822 patients treated for facial rejuvenation with a new hyaluronic acid filler. J Drugs Dermatol. 2013;12(5):e88–e93. | ||
Day DJ, Littler CM, Swift RW, Gottlieb S. The wrinkle severity rating scale. Am J Clin Dermatol. 2004;5(1):49–52. | ||
Narins RS, Brandt F, Leyden J, Lorenc ZP, Rubin M, Smith S. A randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane versus Zyplast for the correction of nasolabial folds. Dermatol Surg. 2003;29(6):588–595. | ||
Rohrich, RJ, Pessa, JE, Ristow, B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008:121:2107–2112. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.