Back to Journals » Risk Management and Healthcare Policy » Volume 13
Mental Health Problems in Chinese Healthcare Workers Exposed to Workplace Violence During the COVID-19 Outbreak: A Cross-Sectional Study Using Propensity Score Matching Analysis
Authors Wang W ![]() , Lu L, Kelifa MM
, Lu L, Kelifa MM ![]() , Yu Y, He A, Cao N, Zheng S, Yan W, Yang Y
, Yu Y, He A, Cao N, Zheng S, Yan W, Yang Y
Received 2 September 2020
Accepted for publication 5 November 2020
Published 3 December 2020 Volume 2020:13 Pages 2827—2833
DOI https://doi.org/10.2147/RMHP.S279170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Wei Wang,1,* Lili Lu,2,* Mohammedhamid Mohammedosman Kelifa,3 Yan Yu,3 Anqi He,3 Na Cao,3 Si Zheng,3 Wenjun Yan,1 Yinmei Yang3
1School of Public Health, Xuzhou Medical University, Xuzhou, People’s Republic of China; 2Department of Gastroenterology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China; 3School of Health Sciences, Wuhan University, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Wang
School of Public Health, Xuzhou Medical University, Xuzhou, People’s Republic of China
Tel +86-15152118260
Email [email protected]
Yinmei Yang
School of Health Sciences, Wuhan University, Wuhan, People’s Republic of China
Tel +86-15071458786
Email [email protected]
Objective: This study aimed at examining the effect of medical workplace violence (MWV) on the mental health of Chinese healthcare workers during the outbreak of coronavirus disease 2019 (COVID-19).
Methods: An anonymous online survey was issued to Chinese healthcare workers (N=1063) from 31 provinces and autonomous regions between February 13th and February 20th. Mental health was measured by the Chinese Depression Anxiety Stress Scales-21 (DASS-21). Medical workplace violence was measured using a single item, whether any type of workplace violence was experienced during the COVID-19 outbreak. Propensity score matching was used to assess the impact of MWV on mental health.
Results: Out of 1063, 217 (20.4%) reported experiencing MWV during the COVID-19 outbreak. Before matching, MWV was correlated with elevated mental health problems (b=8.248, p< 0.001), after adjusting for other variables. After matching, Chinese healthcare workers who experienced MWV were more likely to suffer from mental health problems than those who did not.
Conclusion: MWV exerts a detrimental effect on mental health among Chinese healthcare workers during the COVID-19 outbreak. It is necessary to create a more supportive and safer work environment for healthcare workers at this special context of the COVID-19 outbreak.
Keywords: workplace violence, mental health, COVID-19, propensity score
Introduction
Medical workplace violence has been recognized as one of the biggest public health concerns that disproportionately affect the health of healthcare workers and the smooth delivery of health care services.1,2 The incidence rate of medical workplace violence (MWV) was repeatedly documented worldwide,3–6 and a recent meta-analysis study revealed that the prevalence of MWV reached as high as 61.9%, especially in Asian countries.7
The ongoing Coronavirus Disease 2019 (COVID-19) pandemic has become a threat to the psychological health (depression, anxiety) of many people around the world.8,9 Healthcare workers are at the frontline of the fight against COVID-19, which puts them at heightened risks of being infected. By the end of this investigation, nearly 3400 Chinese healthcare workers have contracted severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), along with 13 deaths.10 The surge of confirmed cases, longer waiting time-intervals, misinformation about SARS-CoV-2, and misplaced anger may be likely drivers of violence against healthcare workers.11–13 An Indian study also showed that the COVID-19 pandemic stirred an upsurge of MWV, and incognizance and anxiety exacerbated by the pandemic may explain this phenomenon.14
MWV relates to a wide range of physical problems, including physical impairment, temporary or permanent disability, or even death.15 On the other hand, the effects of MWV on the mental health of healthcare workers should not be ignored. Previous studies have consistently indicated positive links between workplace violence and mental health problems.16,17 For instance, employees exposed to work-related threats and violence had a higher risk of depression than non-exposed employees.18 Similarly, among healthcare workers, it exerted considerable negative impacts on their mental health, including anxiety, stress, and depression.19–21 A recent study in China also found that healthcare workers who experienced workplace violence were more likely to suffer from depression and anxiety.22
The mental health problems not only affect the healthcare workers’ decision-making capacity, but it may also have a lasting effect on their overall well-being.23 Therefore, providing a safer workplace for healthcare workers is crucial for the continuity of their service and long-term health. Despite considerable exploration of the associations between MWV and mental health, no research to date has examined the effects of MWV on the mental health of healthcare workers in the context of the COVID-19 outbreak.
Most previous studies regarding MWV and mental health were observational. Their methodological limitations like selection bias would hinder the understanding of the relationship between MWV and mental health problems. Propensity score matching (PSM) is a useful analytic approach that can provide less biased findings when randomization fails or is impossible.24 Therefore, this study aims to investigate the prevalence and the influence of MWV on mental health using PSM among Chinese healthcare workers during the COVID-19 outbreak.
Methods
Participants
A cross-sectional study was conducted among Chinese healthcare workers between February 13th and 20th, 2020, through electronic questionnaires from 31 provinces, municipalities, and autonomous regions in mainland China. Relying on the authors’ networks, a link or a quick response (QR) code of an online questionnaire was sent to Chinese healthcare workers through WeChat (similar to WhatsApp). Electronic informed consent was also obtained from all participants via WeChat.
Ethical approval for this study was obtained from the Medical Ethics Committee of Xuzhou Medical University.
Measures
Medical Workplace Violence
Medical workplace violence was measured using a single item (yes or no): “have you experienced any type of workplace violence during the COVID-19 pandemic, including physical, mental and verbal violence?”
Mental Health
The Chinese Depression Anxiety Stress Scales-21 (DASS-21)25 was used to measure the symptoms of depression, anxiety, and stress. Each item was scored on a 4-point Likert scale (0 = did not apply to me at all, 3 = applied to me very much or most of the time). The composite score was multiplied by 2 to make it comparable to the DASS-42.26 The total possible score ranges from 0 to 126, with higher scores representing more negative emotional states in the past week. The Cronbach’s α coefficient of the scale in the current study was 0.94.
Control Variables
Control variables contained demographic information (age, gender, and education), job-related factors (job type, working time, working at a designated hospital for COVID-19, and adequacy of preventive medical equipment), interpersonal factors (experience discrimination for working in hospitals and household transmission-related fears) and social support. The 12-item perceived social support (PSS) scale27 was applied to evaluate perceived social support from families, friends and significant others. Each item was rated on a 7-point Likert scale (1 = very strongly disagree, 7 = very strongly agree), with higher scores denoting greater perceived social support. The Cronbach’s α coefficient of the scale in the current study was 0.94.
Statistical Analysis
Firstly, we compared control variables and mental health across workplace violence and non-workplace violence groups using Pearson’s Chi-squared or t-test. Next, the ordinary least squares (OLS) model was applied to examine the association between MWV and mental health problems, after adjusting for other covariates. Finally, to eliminate observed differences between the workplace violence and non-workplace violence groups, control variables were utilized to estimate the propensity score using 1:1 nearest neighbor matching (with replacement), 1:4 nearest neighbor matching (with replacement), caliper matching (width= 0.01), 1:4 caliper matching (width= 0.01), and kernel matching (width= 0.06). The average treatment effect on the treated (ATT) was estimated and reported in the current study. All statistical analyses were performed using Stata (version 12.0).
Results
In total, 1063 healthcare workers completed the questionnaire. 20.4% (217/1063) reported having experienced MWV during the COVID-19 pandemic. Healthcare workers who experienced MWV were significantly different from those who were not exposed to MWV in mental health problems and nearly all control variables, except education and job type (Table 1).
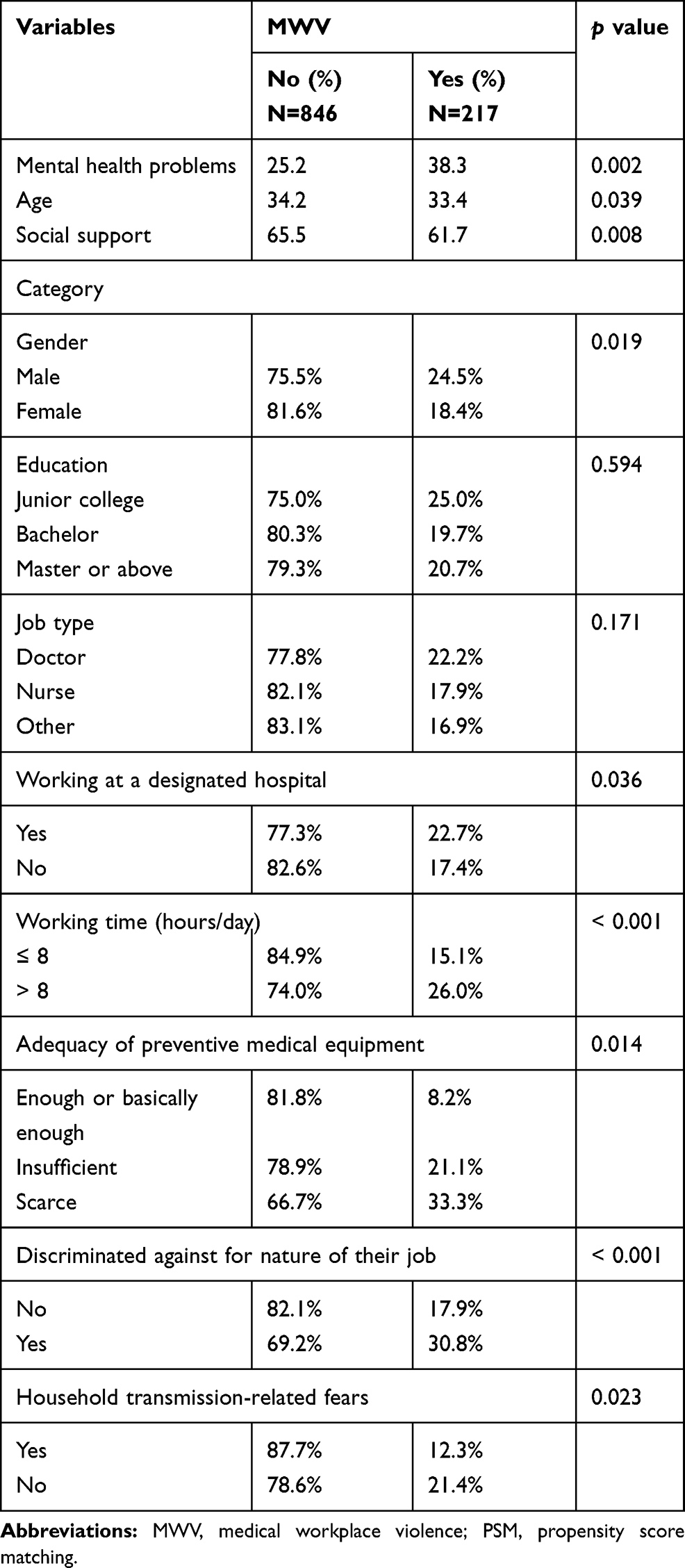 |
Table 1 Characteristics of Healthcare Workers Exposed to MWV Before PSM (N = 1063) |
As shown in Table 2, MWV was correlated with elevated mental health problems (b = 8.248, p<0.001), after adjusting for other variables.
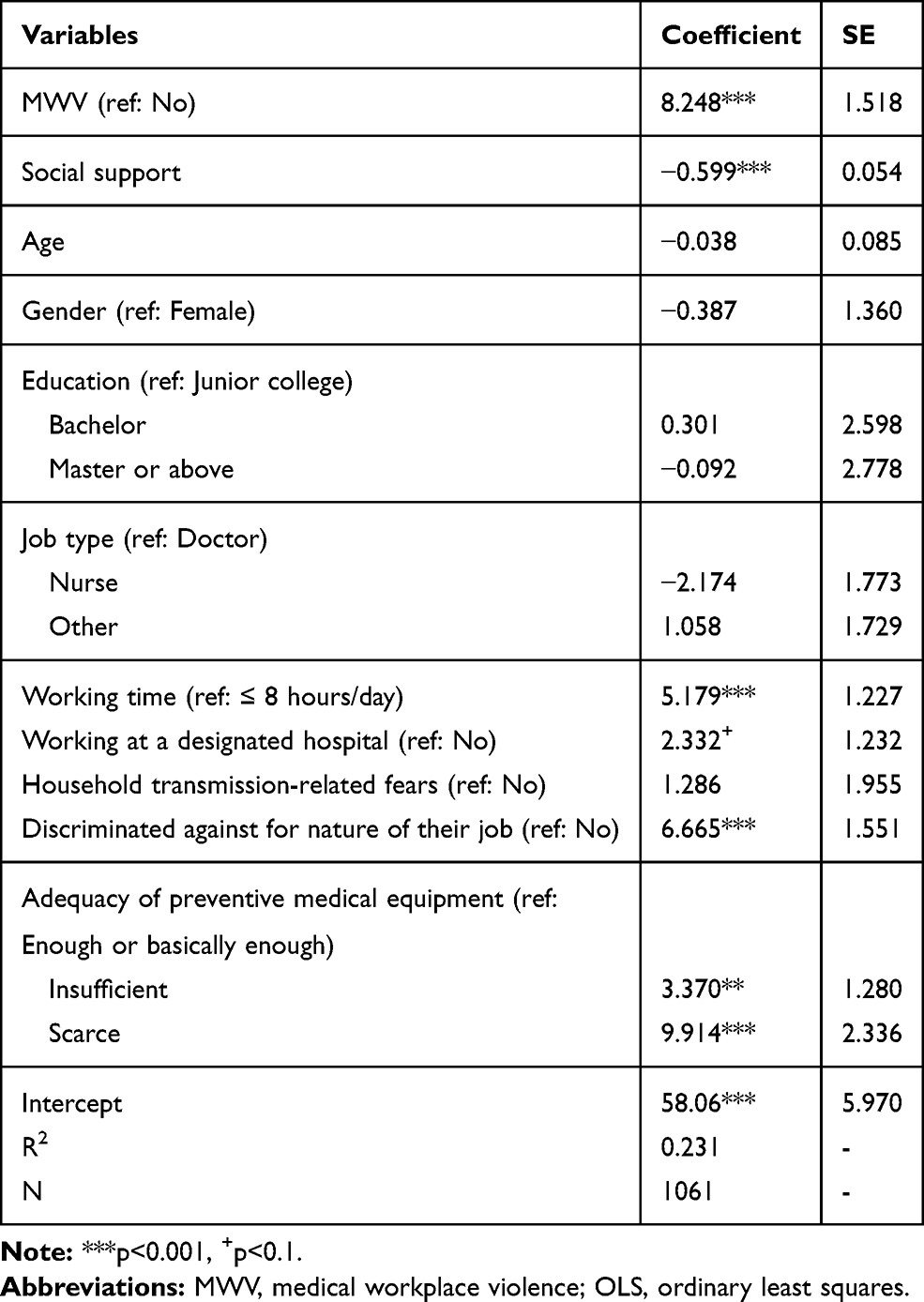 |
Table 2 Association Between MWV and Mental Health Problems: Based on OLS |
After matching, the standard bias of all control variables was less than 10.0%, and the p-value of LR Chi2 was larger than 0.05, suggesting a good balance of all matching (Table 3). Other details of balance check are summarized in Table 4. The post-matching comparisons using different methods revealed that none of the control variables remained statistically significant after the application of PSM. Sensitivity analysis indicated that the study becomes sensitive to hidden bias at Γ = 1.5 or 1.6 (Table 3); hence, further analysis controlling for additional biases is warranted.
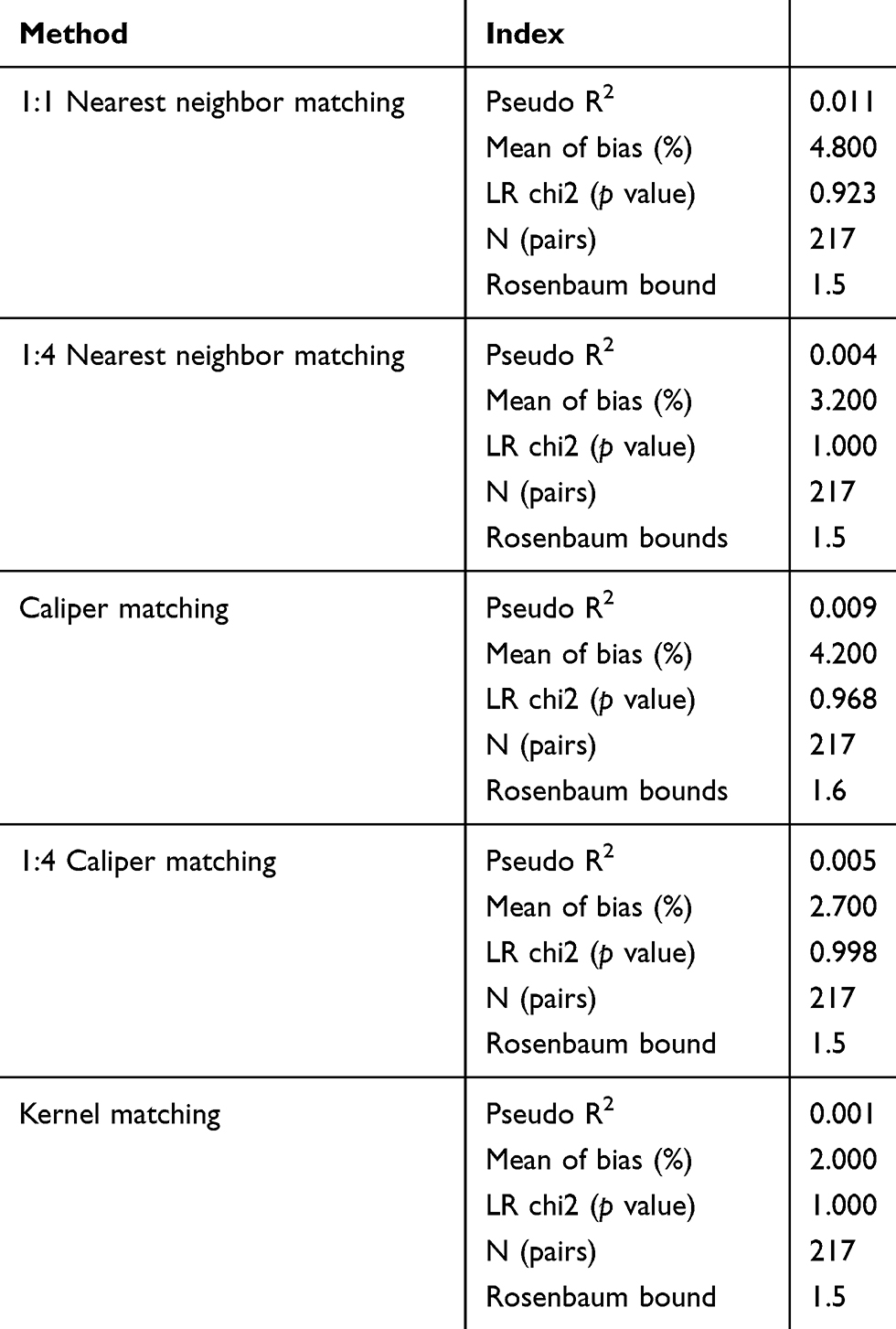 |
Table 3 Results of Balance Check and Sensitivity Analysis |
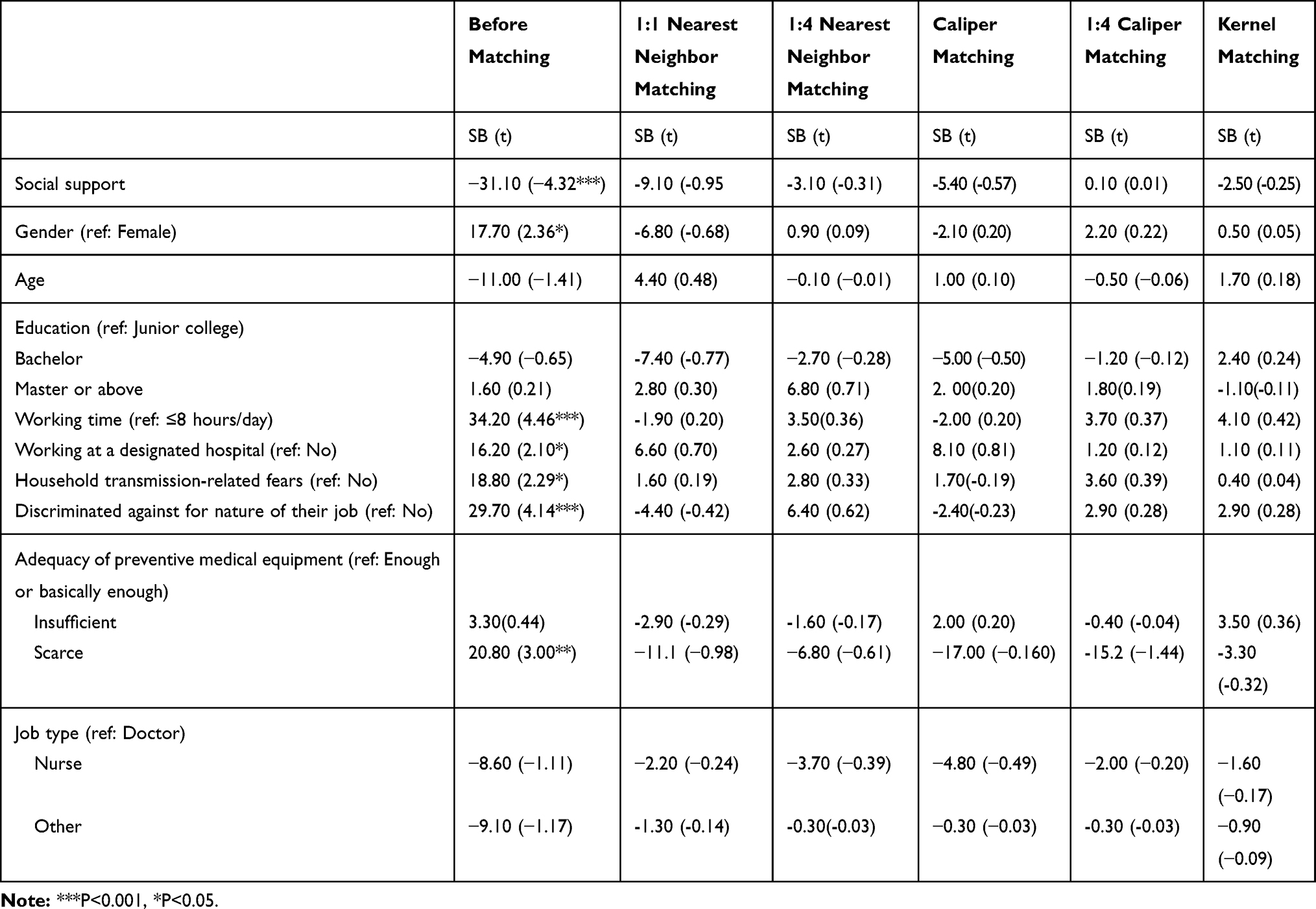 |
Table 4 Results of Balance Check |
As shown in Table 5, after matching, healthcare workers who reported MWV had higher levels of mental health problem (ATT =7.097–8.193, p<0.05) than those who did not.
 |
Table 5 The Effect of MWV on Mental Health Problems |
Discussion
A review suggested that the COVID-19 pandemic resulted in unprecedented mental health hazards in the general population.28 To our knowledge, this is the first study to examine the impact of MWV on the mental health of healthcare workers during the COVID-19 outbreak using PSM. Our findings indicated that Chinese healthcare workers exposed to MWV were more likely to have high levels of mental health problems (including depression, anxiety and stress symptoms).
Our study found that the prevalence of workplace violence toward healthcare workers (mainly doctors and nurses) was relatively lower (20.4%) than rates reported by previous studies in China (ranging from 59.64% to 76.2%)29,30 and other countries, such as Israel (58.4%)31 and Australia (71.0%).32 The extant research typically investigated the experience of exposure to MWV in the past year, but we only surveyed MWV experience during an approximately one-month period of the outbreak, which may provide some explanations for the difference.
Both OLS and PSM revealed that MWV was an independent risk factor for mental health problems among Chinese healthcare workers. Healthcare workers reporting MWV experience were more likely to suffer from depression, anxiety and stress symptoms than those who did not. Similarly, a substantial part of the literature has found that workplace violence may increase the prevalence of anxiety and depression among healthcare workers.17,33–35 In the context of the COVID-19 outbreak, exposure to violence may further exacerbate the already unprecedented COVID-19-related stress and burnout that healthcare workers are experiencing.13 Consequently, exposure to violence has detrimental effects on healthcare workers’ mental health. Hence, it must be prevented and condemned, and creating a more supportive and safer working environment for healthcare workers at this time is particularly helpful.
Effective interventions at a national, hospital and individual levels should be taken to address MWV. For example, the government should issue strict, permanent, and strongly enforce legislation to protect healthcare workers from violence, signals the government’s “zero tolerance” concerning MWV.36 Hospital administration should invest in health security measures, like improving an orderly medical system, optimizing the process of consultation, classifying the management of disease, establishing security patrols, and installing cameras.22 In addition, telemedicine has been critical during the COVID-19 pandemic, as it has the potential to continue a “normal” job for healthcare workers and avoid MWV.37 In terms of healthcare workers, staff training for improving communication skills can improve empathetic care and patient-healthcare worker relationship which in turn may minimize MWV.
Our results also revealed that low levels of social support, long working time, working at a designated hospital, discrimination experience, and scarcity of preventive medical equipment were related to increased mental health problems among healthcare workers during the COVID-19 outbreak. With the surge of confirmed and suspected cases, healthcare workers are obliged to overwork to meet health requirements, which may result in mental exhaustion.23,38 Providing social support, as well as creating a safe working environment through logistical support, nondiscrimination, an arrangement of adequate rest would appear to alleviate their psychological pressure.
Limitations
Several limitations should be noted in the current study. First, this was a cross-sectional study. Hence, the causal relationship between MWV and mental health cannot be established. Second, despite the efforts to recruit participants from 31 provinces, municipalities, and autonomous regions in mainland China, non-random sampling of healthcare workers limits generalizability of our findings. Third, MWV was measured as a binary variable using unvalidated scales. Additionally, data on different types of violence should be collected in future research. Fourth, PSM cannot control unobserved confounders. Last, sensitivity analysis indicated that the study was sensitive to hidden bias; hence, further research should include other important variables.
Conclusions
In summary, despite the relatively low occurrence of MWV among Chinese healthcare workers during the COVID-19 outbreak, healthcare workers who experienced MWV were more likely to suffer from mental health problems than those who did not. Providing safer workplace for healthcare workers should be urgently prioritized. Once healthcare workers experience violence, it is vital to focus on their emotional reactions to attenuate the detrimental effects of MWV on their mental health. Future longitudinal studies with a nationally representative sample would verify the causal relationship between MWV and the mental health of healthcare workers.
Data Sharing Statement
Data obtained for the study will not be made available to others.
Funding
This study was supported by The Postdoctoral research fund of Jiangsu Province [grant number 2020Z177] and China Association for Science and Technology [20200608CG080611].
Disclosure
Wei Wang and Lili Lu are co-first authors for this study. No potential conflict of interest was reported by the authors.
References
1. Hsieh HF, Hung YT, Wang HH, Ma SC, Chang SC. Factors of resilience in emergency department nurses who have experienced workplace violence in Taiwan. J Nurs Scholarsh. 2016;48(1):23–30. doi:10.1111/jnu.12177
2. Li Z, Yan CM, Shi L, et al. Workplace violence against medical staff of Chinese children’s hospitals: a cross-sectional study. PLoS One. 2017;12(6):e0179373. doi:10.1371/journal.pone.0179373
3. Zeng JY, An FR, Xiang YT, et al. Frequency and risk factors of workplace violence on psychiatric nurses and its impact on their quality of life in China. Psychiatry Res. 2013;210(2):510–514. doi:10.1016/j.psychres.2013.06.013
4. Raveesh BN, Lepping P, Lanka SV, Turner J, Krishna M. Patient and visitor violence towards staff on medical and psychiatric wards in India. Asian J Psychiatr. 2015;13:52–55. doi:10.1016/j.ajp.2014.10.003
5. Talas MS, Kocaöz S, Akgüç S. A survey of violence against staff working in the emergency department in ankara, Turkey. Asian Nurs Res (Korean Soc Nurs Sci). 2011;5(4):197–203. doi:10.1016/j.anr.2011.11.001
6. Lanza ML, Zeiss RA, Rierdan J. Non-physical violence: a risk factor for physical violence in health care settings. AAOHN J. 2006;54(9):397–402. doi:10.1177/216507990605400903
7. Liu J, Gan Y, Jiang H, et al. Prevalence of workplace violence against healthcare workers: a systematic review and meta-analysis. Occup Environ Med. 2019;76(12):927–937. doi:10.1136/oemed-2019-105849
8. Yan L, Gan Y, Ding X, Wu J, Duan H. The relationship between perceived stress and emotional distress during the COVID-19 outbreak: Effects of boredom proneness and coping style. J Anxiety Disord. 2020;77:102328. doi:10.1016/j.janxdis.2020.102328
9. Khan S, Siddique R, Bai Q, et al. Coronaviruses disease 2019 (COVID-19): causative agent, mental health concerns, and potential management options. J Infect Public Health. 2020:
10. The Novel Coronavirus infected pneumonia report National Health Commission of the People’s Republic of China; 2020. Available from: http://www.nhc.gov.cn/xcs/xxgzbd/gzbd_index.shtml.
11. Rodríguez-Bolaños R, Cartujano-Barrera F, Cartujano B, Flores YN, Cupertino AP, Gallegos-Carrillo K. The urgent need to address violence against health workers during the COVID-19 pandemic. Med Care. 2020;58(7):663. doi:10.1097/mlr.0000000000001365
12. Lancet T. Violence against doctors: why China? Why now? What next? Lancet. 2014;383(9922):1013. doi:10.1016/s0140-6736(14)60501-8
13. McKay D, Heisler M, Mishori R, Catton H, Kloiber O. Attacks against health-care personnel must stop, especially as the world fights COVID-19. Lancet. 2020;395(10239):1743–1745. doi:10.1016/s0140-6736(20)31191-0
14. Covid-19: Indian government vows to protect healthcare workers from violence amid rising cases. BMJ. 2020;369:m1631. doi:10.1136/bmj.m1631
15. Alexy EM, Hutchins JA. Workplace violence: a primer for critical care nurses. Crit Care Nurs Clin North Am. 2006;18(3):305–312. doi:10.1016/j.ccell.2006.05.014
16. Lipscomb JA, London M, Chen YM, et al. Safety climate and workplace violence prevention in state-run residential addiction treatment centers. Work (Reading, Mass). 2012;42(1):47–56. doi:10.3233/wor-2012-1330
17. Fang H, Zhao X, Yang H, et al. Depressive symptoms and workplace-violence-related risk factors among otorhinolaryngology nurses and physicians in Northern China: a cross-sectional study. BMJ Open. 2018;8(1):e019514. doi:10.1136/bmjopen-2017-019514
18. Andersen LPS, Hogh A, Andersen JH, Biering K. Depressive symptoms following work-related violence and threats and the modifying effect of organizational justice, social support, and safety perceptions. J Interpers Violence. 2019:886260519831386. doi:10.1177/0886260519831386
19. Cheung T, Yip PS. Workplace violence towards nurses in Hong Kong: prevalence and correlates. BMC Public Health. 2017;17(1):196. doi:10.1186/s12889-017-4112-3
20. Zhang SE, Liu W, Wang J, et al. Impact of workplace violence and compassionate behaviour in hospitals on stress, sleep quality and subjective health status among Chinese nurses: a cross-sectional survey. BMJ Open. 2018;8(10):e019373. doi:10.1136/bmjopen-2017-019373
21. Zhao S, Xie F, Wang J, et al. Prevalence of workplace violence against Chinese nurses and its association with mental health: a cross-sectional survey. Arch Psychiatr Nurs. 2018;32(2):242–247. doi:10.1016/j.apnu.2017.11.009
22. Shi L, Li G, Hao J, et al. Psychological depletion in physicians and nurses exposed to workplace violence: a cross-sectional study using propensity score analysis. Int J Nurs Stud. 2020;103:103493. doi:10.1016/j.ijnurstu.2019.103493
23. Xiang YT, Yang Y, Li W, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020;7(3):228–229. doi:10.1016/s2215-0366(20)30046-8
24. Guo SY, Fraser MW. Propensity Score Analysis: Statistical Methods and Applications.
25. Taouk M, Lovibond P, Laube R. Psychometric Properties of a Chinese Version of the 21-Item Depression Anxiety Stress Scales (DASS21). Sydney: Cumberland Hospital; 2001.
26. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
27. Sinclair SJ, Siefert CJ, Slavin-Mulford JM, Stein MB, Renna M, Blais MA. Psychometric evaluation and normative data for the depression, anxiety, and stress scales-21 (DASS-21) in a nonclinical sample of U.S. adults. Eval Health Prof. 2012;35(3):259–279. doi:10.1177/0163278711424282
28. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
29. Liu W, Zhao S, Shi L, et al. Workplace violence, job satisfaction, burnout, perceived organisational support and their effects on turnover intention among Chinese nurses in tertiary hospitals: a cross-sectional study. BMJ Open. 2018;8(6):e019525. doi:10.1136/bmjopen-2017-019525
30. Sun T, Gao L, Li F, et al. Workplace violence, psychological stress, sleep quality and subjective health in Chinese doctors: a large cross-sectional study. BMJ Open. 2017;7(12):e017182. doi:10.1136/bmjopen-2017-017182
31. Itzhaki M, Peles-Bortz A, Kostistky H, Barnoy D, Filshtinsky V, Bluvstein I. Exposure of mental health nurses to violence associated with job stress, life satisfaction, staff resilience, and post-traumatic growth. Int J Ment Health Nurs. 2015;24(5):403–412. doi:10.1111/inm.12151
32. Cashmore AW, Indig D, Hampton SE, Hegney DG, Jalaludin BB. Workplace violence in a large correctional health service in New South Wales, Australia: a retrospective review of incident management records. BMC Health Serv Res. 2012;12:245. doi:10.1186/1472-6963-12-245
33. Hsieh HF, Wang HH, Shen SH, Li YC. Predictors of depressive symptoms among psychiatric nurses who suffered from workplace violence. J Adv Nurs. 2018;74(2):425–432. doi:10.1111/jan.13451
34. Kim JH, Lee N, Kim JY, Kim SJ, Okechukwu C, Kim SS. Organizational response to workplace violence, and its association with depressive symptoms: a nationwide survey of 1966 Korean EMS providers. J Occup Health. 2019;61(1):101–109. doi:10.1002/1348-9585.12025
35. Lindwall M, Gerber M, Jonsdottir IH, Börjesson M, Ahlborg G
36. Lu S, Ren S, Xu Y, et al. China legislates against violence to medical workers. Lancet Psychiatry. 2020;7(3):e9. doi:10.1016/s2215-0366(20)30005-5
37. Tolone S, Gambardella C, Brusciano L, Del Genio G, Lucido FS, Docimo L. Telephonic triage before surgical ward admission and telemedicine during COVID-19 outbreak in Italy. Effective and easy procedures to reduce in-hospital positivity. Int J Surg. 2020;78:123–125. doi:10.1016/j.ijsu.2020.04.060
38. Ranney ML, Griffeth V, Jha AK. Critical supply shortages - the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.