Back to Journals » Psychology Research and Behavior Management » Volume 10
Mental disorders, functional impairment, and nerve growth factor
Authors Salles FHM, Soares PSM, Wiener CD, Mondin TC, da Silva PM, Jansen K, de Mattos Souza LD ![]() , da Silva RA
, da Silva RA ![]() , Oses JP
, Oses JP
Received 22 January 2016
Accepted for publication 13 May 2016
Published 22 December 2016 Volume 2017:10 Pages 9—15
DOI https://doi.org/10.2147/PRBM.S104814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Fanny Helena Martins Salles,1 Pedro San Martin Soares,1 Carolina David Wiener,1 Thaise Campos Mondin,1 Paula Moraes da Silva,1 Karen Jansen,1–3 Luciano Dias de Mattos Souza,1 Ricardo Azevedo da Silva,1 Jean Pierre Oses1–3
1Translational Science on Brain Disorders, Department of Health and Behavior, Catholic University of Pelotas, Pelotas, Rio Grande do Sul, Brazil; 2Translational Psychiatry Program, 3Center of Excellence on Mood Disorders, Department of Psychiatry and Behavioral Sciences, The University of Texas Health Science Center at Houston (UTHealth) Medical School, Houston, TX, USA
Abstract: Nerve growth factor (NGF) is an important member of the neurotrophin family and its alteration has been associated with psychiatric disorders. Functionality consists of the activities that an individual can perform, as well as their social participation, which is an important factor in analyzing the carrier living conditions of subjects with psychiatric suffering. Several studies have evaluated functionality in bipolar disorder; however, no studies have evaluated the functionality in other mental disorders. There are also few studies investigating the association between functionality and the biological bases of mental disorders. This study aimed to evaluate the serum NGF levels in psychiatric patients and to verify a possible association between the serum neurotrophic levels and functionality. This was a cross-sectional study with a convenient sample obtained from the Public Mental Health Service from the south of Brazil. The final sample was composed of 286 patients enrolled from July 2013 to October 2014. Data was collected using a sociodemographic questionnaire, and the diagnosis was confirmed using the Mini International Neuropsychiatric Interview (M.I.N.I) and a Functioning Assessment Short Test. The serum NGF levels were determined using the enzyme-linked immunosorbent assay method. Statistical analyses were performed using IBM SPSS Statistic 21.0 software. NGF serum levels were increased significantly in patients with obsessive–compulsive disorder compared with patients with no obsessive–compulsive disorder (P=0.015). An increase in serum NGF levels in generalized anxiety disorder patients was observed compared with patients with no generalized anxiety disorder (P=0.047). NGF was negatively associated with autonomy (P=0.024, r=–0.136), work (P=0.040, r=–0.124), and cognition (P=0.024, r=–0.137), thereby showing that changes in serum levels of NGF are associated with functionality in mental disorders.
Keywords: NGF, mental disorders, functional impairment
Introduction
Nerve growth factor (NGF) is an important member of the neurotrophin family and is produced mainly in the cortex, hippocampus, and hypothalamus. It has a role in the survival of sympathetic and some sensory and central cholinergic neurons. Additionally, NGF acts outside of the nervous system, particularly within the neuroendocrine and immune system. Previous studies have evaluated the role of altered NGF in animal and human models and found reduced levels of NGF mainly in subjects with major depression.1–7 NGF has an important role in neuronal survival, differentiation, connectivity, and plasticity during development and adulthood, and when affected by stress, are good candidates for the transduction of the effects of adverse events to changes in brain function.1,8,9 Since NGFs have a relevant role in the maintenance of neuronal homeostasis, changes in their levels have been implicated in diverse neuropsychiatric disorders.4 Thus, it has been recently suggested that NGF is involved in the pathophysiology of psychiatric disorders.2,3 In mice, NGF release was associated with an increase in behavioral stress.3 In human studies, Diniz et al4 found reduced levels of NGF in subjects with late-life depression. Moreover, treatment with antidepressants has restored NGF levels in both clinical and experimental studies.5 Recently, our group has shown that NGF and brain-derived neurotrophic factor (BDNF), but not glial cell-drived neurotrophic factor, were associated with the clinical features of major depressive disorder (MDD) in patients.10 The management of psychiatric disorders is evaluated by clinical assessments and does not consider the related biological basis of brain functions. Moreover, more useful biomarkers in the psychiatry field are needed to be explored in order to better understand mental disorders. Thus, the identification of biological parameters could improve the diagnosis and treatment of these disorders.
Functionality consists of activities that an individual can perform, as well as their social participation. Functional impairment in mental disorders is a well-known fact. Furthermore, the concept of functional impairment is complex, involving different domains of functioning and areas of life. Functionality is an important factor to evaluate the patient to understand the living conditions of psychiatric suffering.11,12 Several studies have evaluated functionality in bipolar disorder;13–19 however, to the best of our knowledge, no studies have evaluated the functionality in other mental disorders. There are also few studies investigating the association between functionality and biological bases of mental disorders. The most common mental disorders present in the general population are associated with functioning deficits, interfering with the management of one’s life; however, they are not considered as biological parameters. Therefore, this study aimed to evaluate the serum NGF levels in psychiatric patients and to verify a possible association between serum NGF levels and functionality in patients from the Brazilian Public Mental Health Service.
Methods
Participants
This was a cross-sectional study with a convenient sample obtained from the Public Mental Health Service (Bage, Brazil). Subjects were 19 years of age or above, of either sex, and in their first psychiatry and/or psychological care. The total sample was composed of 286 subjects who participated between July 2013 and October 2014. The project was approved by the ethical committee of the Catholic University of Pelotas (16429713.9.0000.5339), and all subjects signed an informed consent.
Data collection
For data collection, a sociodemographic questionnaire was used to obtain information, such as age, education, economic status, and marital status. The economic classification was performed using the criteria of the Brazilian Association of Research Companies, which is based on the accumulation of material goods and education of the household head. This classification fits people into Classes A, B, C, D, or E from the scores achieved, in which the letter “A” refers to the highest socioeconomic status and “E” refers to the lowest.20 There were no participants belonging to the Class E in this sample. Body mass index (BMI) was calculated by using the following formula: weight (kg)/height (m2). Participants were asked about current psychiatric medication use. The diagnosis was conducted by trained psychologists of the Mental Health Service using the structured diagnostic interview – Mini International Neuropsychiatric Interview, according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition diagnostic criteria.21 The mental disorders evaluated were major depression, bipolar disorder, obsessive–compulsive disorder (OCD), panic disorder, generalized anxiety disorder (GAD), and schizophrenia. Moreover, suicide risk was evaluated. To measure the individual functionality, we used the Functioning Assessment Short Test (FAST). FAST is a 24-item interview designed to assess the damaged areas of everyday functioning, which included the objective evaluation of six specific areas of functionality: autonomy, work, cognition, interpersonal skills, finance, and leisure.16 Scores were determined by the sum of items, ranging from 0 (indicating no problems) to 3 (indicating a severe limitation) over a period of 15 days prior to the application of the scale.13 Therefore, the higher the scores, the higher the functional impairment. Comorbidity was calculated through diagnosis groups: anxiety disorder (GAD, OCD, and panic disorder [PD]), mood disorder (major depression and bipolar disorder), and psychotic disorders (schizophrenia and presence of psychotic symptoms) and after the sum of each group separated.
Biochemical analyses
For the biochemical analyses, 10 mL of blood were drawn from each subject by venipuncture into an anticoagulant-free vacuum tube at baseline and postintervention. All venous blood samples were taken in the morning (between 9 am and 11 am). The blood was at room temperature for 30 minutes for coagulation, after which the blood was immediately centrifuged at 4000× g for 10 minutes, and serum was kept frozen at −80°C until analysis. Serum NGF levels were measured using a commercial immunoassay kit (DuoSet ELISA Development, R&D Systems, Inc., Minneapolis, MN, USA). Serum NGF levels were expressed in pg/mL. The kits have a minimum detectable dose of 9.46 pg/mL for NGF. NGF levels ranged from 7.39 to 198.37 pg/mL, with values below 9.46 pg/mL considered as the reference number (n=12).
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistic 21.0 (IBM Corporation, Armonk, NY, USA) software. Sociodemographic characteristics and serum NGF levels are shown by the absolute and relative frequencies, mean ± standard deviation, or by the median and interquartile range (IQR). The serum levels of NGF had non-Gaussian distributions. To verify the association between sociodemographic and clinical characteristics and NGF serum levels, the Mann–Whitney U test, Kruskal–Wallis test, and Spearman correlation were used. Differences between FAST scale and diagnosis groups were analyzed using Student t-test for independent sample and Pearson’s correlation. A multivariate linear regression was performed to verify the relation between NGF levels and functioning. NGF outliers were considered in the analyses. The results with P≤0.05 were considered statistically significant.
Results
The sample demographic and clinical characteristics according to NGF levels are presented in Table 1. We recruited 276 subjects with a mean ± standard deviation age of 38.79±12.98 years, of which 75.3% were female, 57.1% belonged to C and D socioeconomic classes, 53.8% were married, and the mean BMI was 26.43 kg/m2 (±5.15 kg/m2). Regarding clinical characteristics, 30.4% (n=84) were using psychiatric medication; the prevalence of depression was 53.3% (n=147), bipolar disorder 18.8% (n=52), suicide risk 55.8% (n=154), schizophrenia 11.6% (n=32), OCD 24.7% (n=67), GAD 12.3% (n=33), and panic disorder 26.4% (n=73). The mean age of onset of the disease was 27.28 (±12.37) years, and the mean duration of the disease was 10.46 years (±10.93 years). The median NGF levels in the total sample was 21.81 pg/mL (15.72–32.28 pg/mL). The total mean of the FAST score was 31.05 (±16.83). Serum NGF levels were increased significantly in OCD patients compared with patients with no OCD: 24.25 pg/mL (IQR =18.31–34.58) and 21.25 pg/mL (IQR =18.31–34.58) (P=0.017), respectively. We also observed an increase in serum NGF levels in GAD patients compared with patients with no GAD: 22.25 pg/mL (IQR =15.97–32.40) and 17.81 pg/mL (IQR =13.43–23.54) (P=0.047), respectively.
 | Table 1 Sample distribution and median (IQR) of serum NGF levels according to demographic and clinical characteristics Notes: aMann–Whitney U test. bKruskal–Wallis test. cSpearman correlation. ”—” = no data. Abbreviations: IQR, interquartile range; NGF, nerve growth factor; BMI, body mass index; OCD, obsessive–compulsive disorder; GAD, generalized anxiety disorder; FAST, Functioning Assessment Short Test. |
Table 2 shows the functioning scores according to clinical characteristics. FAST scores were significantly increased in all the disorders and there was a trend toward significance for GAD (P=0.062). No correlation was observed between the FAST score and age of onset and duration of disease. Sex, age, marital status, and BMI were not associated with OCD and GAD (data not shown).
 | Table 2 Functioning scores according to clinical characteristics Note: “—” = no data. Abbreviations: FAST, Functioning Assessment Short Test; OCD, obsessive–compulsive disorder; GAD, generalized anxiety disorder. |
A multivariate linear regression was calculated to predict serum NGF levels based on FAST total score and domains. After adjustments for GAD and OCD, participant’s NGF levels decreased: –0.21 pg/mL for each increase in the FAST total score (P=0.035) and –1.20 pg/mL for the autonomy domain for each increase in the FAST total score (P=0.011). A trend toward significance was observed in the work (P=0.084) and cognition domain (P=0.096; Table 3).
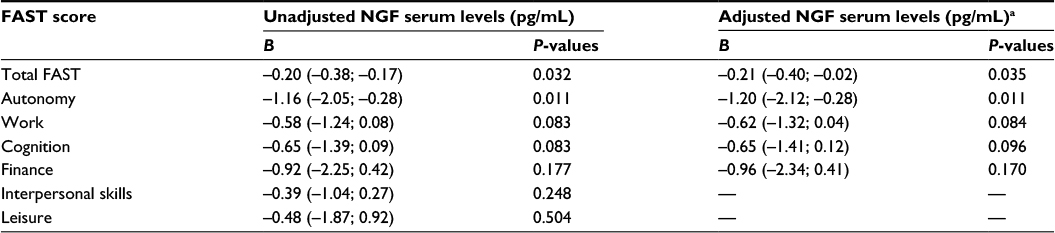 | Table 3 Multivariate linear regression of the relation between NGF and functioning scores and domains Notes: aAdjusted for OCD and GAD. “—” = no data. Abbreviations: NGF, nerve growth factor; FAST, Functioning Assessment Short Test; OCD, obsessive–compulsive disorder; GAD, generalized anxiety disorder. |
Discussion
In this study, OCD and GAD were associated with serum NGF levels, and higher functional impairment was observed in all mental disorders. After adjustments, we found a negative association in the total scores of the FAST and NGF, as well as autonomy domain and NGF. Epidemiological studies in Brazil show a degree of functional impairment of psychiatric patients. Upon analyzing the domains, “work and income”, we found that 35% had never worked and 55% do not have their own income.22,23 The occupational dysfunction is not only bad per se but also has been reported as a predictor of relapse.24
NGF has a significant role in neurite outgrowth, thereby promoting neuronal integrity.25,26 Furthermore, NGF supported the activity-dependent neuronal plasticity underlying cognitive processes, such as learning and memory, thereby having an important role in anxiety, emotions, and behavioral changes.27–31 A wide variety of studies show that reduced serum levels for the neurotrophic factors are associated with reduced neuronal complexity and impaired learning, and many of these effects can be restored with increased neurotrophic factor levels.32–36 According to this perspective, studies have speculated a significant role of NGF and BDNF levels in complex social interactions, which shows that higher levels of these neurotrophic levels are associated with more aggression and reduced social interactions, while decreased NGF and BDNF levels are associated with socially submissive behaviors and increased social bonding.37 In a psychosocial stress model, agonistic encounters induce NGF release, and the circulating levels of this protein reflect the number of aggressive episodes and hierarchical status.38 Moreover, similar results were found in humans.27 Interestingly, the serum NGF levels precede the increase of cortisol and adrenocorticotropic hormone, thereby suggesting, as a sort of early alert mechanism, that these levels are associated with a homeostatic adaptation. In subjects with chronic stress, such as withdrawal in alcoholics and being a caregiver, there was an association between stress and elevated peripheral NGF.3 Regarding psychiatric disorders, in animal models of depression, changes in NGF levels in rats have been observed.39 In a recent clinical study, reduced NGF levels were found in bipolar disorder patients during manic episodes, in schizophrenia patients with impaired cognitive performance, and in unmedicated patients in first psychosis episode.40
Our results agree with a previous study that NGF levels increase in OCD, and the authors found a statistically significant positive correlation between both NGF levels and the symptoms severity. Fontenelle et al41 suggested two hypotheses: 1) increased NGF levels could represent a coping response involved in preparing the organism to face a highly stressful situation or 2) OCD washing may be associated with some sort of cholinergic dysfunction, since the highest brain levels of NGF are found in targets for basal forebrain cholinergic neurons. We suppose that this increase is according to some cholinergic dysfunction since the patients involved in this study are patients in serious state of mental health and many of them do not use medicines. GAD patients presented an increase in NGF levels compared to non-GAD patients. A previous study by Jockers-Scherübl et al42 did not observe differences between GAD patients and healthy subjects. However, our sample have no control group to compare with mental disorders. Moreover, we cannot discard a possible highly stressful situation together with the NGF changes in the other group as a bias in these results.
Banerjee et al1 and Dwivedi43 found that NGF levels in the hippocampus and serum of suicide victims decreased considerably. We found no association between suicide risk and NGF levels; one possible explanation might be the characteristics of our sample, in which almost no one was taking any medication and probably was seeking attendance for the first time. However, treatment with antidepressants and electroconvulsive therapy increased NGF levels in both clinical and experimental studies.44,45 The psychopathology that was more prevalent included MDD, and the pathogenesis of these disorders is related to the regulation of multiple neurotrophic factors and associated NGF levels decreased in the early stages.46 These results together corroborate that NGF is effective in the pathophysiology of schizophrenia.2 Recently, our group has reported an increase in NGF in some other mental disorders, such as MDD, suicide risk, and alcohol abuse disorder,7 thereby presupposing a relevant role of NGF in mental disorders. In this way, our results agree with previous literature data. Furthermore, these changes in serum NGF levels are associated with functionality in mental disorders.
Limitations
The limitations of this study are related to the control group, which was not diagnosed, and heterogeneity of the sample in relation to the stages of disorders. The design of the cross-sectional study limits the established causal relation between clinical characteristics and neurotrophin. Peripheral NGF levels do not represent the central environment fully, but changes in the circulant NGF can reflect the central nervous system. Moreover, the correlation between peripheral and central NGF levels would have interaction in some specific situations; however, more studies are necessary for a better understanding of this field.47
Conclusion
Understanding the physiological changes related to mental disorders can provide a better understanding of the genesis and mechanisms involved in the progression of these conditions. In this work, we observed an association between functionality and serum levels of NGF in patients from a Public Mental Health Service suggesting a relevant role of NGF in GAD and OCD and its association in functionality.
Acknowledgments
This study was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Capes; 23038.001671/2012-16), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ), and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS; 10/0055-0) Brazil.
Disclosure
The authors report no conflicts of interest in this work.
References
Banerjee R, Ghosh A, Ghosh B, Bhattacharyya S, Mondal A. Decreased mRNA and protein expression of BDNF, NGF, and their receptors in the hippocampus from suicide: an analysis in human postmortem brain. Clin Med Insights Pathol. 2013;6:1–11. | ||
Xiong P, Zeng Y, Wan J, et al. The role of NGF and IL-2 serum level in assisting the diagnosis in first episode schizophrenia. Psychiatry Res. 2011; | ||
Gioiosa L, Iannitelli A, Aloe L. Stress, anxiety schizophrenia and neurotrophic factors: the pioneer studies with nerve growth factor. Riv Psichiatr. 2009;44(2):88–94. | ||
Diniz BS, Teixeira AL, Machado-Vieira R, Talib LL, Gattaz WF, Forlenza OV. Reduced serum nerve growth factor in patients with late-life depression. Am J Geriatr Psychiatry. 2013;21(5):493–496. | ||
Martino M, Rocchi G, Escelsior A, et al. NGF serum levels variations in major depressed patients receiving duloxetine. Psychoneuroendocrinology. 2013;38(9):1824–1828. | ||
Lhullier AC, Moreira FP, da Silva RA, et al. Increased serum neurotrophin levels related to alcohol use disorder in a young population sample. Alcohol Clin Exp Res. 2015;39(1):30–35. | ||
Wiener CD, de Mello Ferreira S, Pedrotti Moreira F, et al. Serum levels of nerve growth factor (NGF) in patients with major depression disorder and suicide risk. J Affect Disord. 2015;184:245–248. | ||
Thoenen H. Neurotrophins and activity-dependent plasticity. Prog Brain Res. 2000;128:183–191. | ||
Dwivedi Y. Brain-derived neurotrophic factor and suicide pathogenesis. Ann Med. 2010;42(2):87–96. | ||
de Azevedo Cardoso T, Mondin TC, Wiener CD, et al. Neurotrophic factors, clinical features and gender differences in depression. Neurochem Res. 2014;39(8):1571–1578. | ||
Zarate C, Tohen M, Land M, Cavanagh S. Functional impairment and cognition in bipolar disorder. Psychiatr Q. 2000;71(4):309–329. | ||
Ustün B, Kennedy C. What is “functional impairment”? Disentangling disability from clinical significance. World Psychiatry. 2009;8(2):82–85. | ||
Salamero M, Torrent C, Reinares M, et al. Validity and reliability of the Functioning Assessment Short Test (FAST) in bipolar disorder. Clin Pract Epidemiol Ment Heal. 2007;3:5. | ||
Vieta E, Cieza A, Stucki G, et al. Developing core sets for persons with bipolar disorder based on the International Classification of Functioning, Disability and Health. Bipolar Disord. 2007;9(1–2):16–24. | ||
Rosa AR, Franco C, Martínez-Aran A, et al. Functional impairment in patients with remitted bipolar disorder. Psychother Psychosom. 2008;77(6):390–392. | ||
Cacilhas AA, Magalhães PV, Ceresér KM, et al. Validity of a short functioning test (FAST) in Brazilian outpatients with bipolar disorder. Value Health. 2009;12(4):624–627. | ||
Demant KM, Almer GM, Vinberg M, Kessing LV, Miskowiak KW. Effects of cognitive remediation on cognitive dysfunction in partially or fully remitted patients with bipolar disorder: study protocol for a randomized controlled trial. Trials. 2013;14(1):378. | ||
Rosa AR, Magalhães PV, Czepielewski L, et al. Clinical staging in bipolar disorder: focus on cognition and functioning. J Clin Psychiatry. 2014;75(5):e450–e456. | ||
Grande I, Magalhães PV, Chendo I, et al. Staging bipolar disorder: clinical, biochemical, and functional correlates. Acta Psychiatr Scand. 2014;129(6):437–444. | ||
ABEP. Critério de Classificação Econômica do Brasil. Sao Paulo: Assoc Bras Empres Pesqui; 2012: 1–4. Available from: www.abep.org – [email protected]. Accessed February 10, 2016. | ||
Amorin P. Mini International Neuropsychiatric Interview (MINI): validation of a short structured diagnostic psychiatric interview. Rev Bras Psiquiatr. 2000;22(3):106–115. | ||
Paula CTC. [Epidemiological profile of patients treated in a Center for Psychosocial Care] Perfil epidemiológico dos usuários de um centro de Atenção Psicossocial na cidade de recife. Cad Bras Saúde Mental. 2010;2(4–5):94–106. | ||
Santos G, Nascimento Y, Veríssimo R, Cavalcante J, Brêda M, Holanda J. [Epidemiological profile of intensive users of a psychosocial care center] O perfil epidemiológicodos usuários de um Centro de Atenção Psicossocial. Revista de enfermagem UFPE online 2013;7(3):679–687. | ||
Fagiolini A, Kupfer D, Masalehdan A, Scott J, Houck P, Frank E. Functional impairment in the remission phase of bipolar disorder. Bipolar Disord. 2005;7(3):281–285. | ||
Sofroniew M, Howe C, Mobley W. Nerve growth factor signaling, neuroprotection and neural repair. Annu Rev Neurosci. 2001;24: | ||
Kimata H. Kissing reduces allergic skin wheal responses and plasma neurotrophin levels. Physiol Behav. 2003;80(2–3):395–398. | ||
Aloe L, Bracci-Laudiero L, Alleva E, Lambiase A, Micera A, Tirassa P. Emotional stress induced by parachute jumping enhances blood nerve growth factor levels and the distribution of nerve growth factor receptors in lymphocytes. Proc Natl Acad Sci USA. 1994;91(22): | ||
Alleva E, Santucci D. Psychosocial vs. “physical” stress situations in rodents and humans: Role of neurotrophins. Physiol Behav. 2001; | ||
Hadjiconstantinou M, McGuire L, Duchemin AM, Laskowski B, Kiecolt-Glaser J, Glaser R. Changes in plasma nerve growth factor levels in older adults associated with chronic stress. J Neuroimmunol. 2001; | ||
Branchi I, Francia N, Alleva E. Epigenetic control of neurobehavioural plasticity: the role of neurotrophins. Behav Pharmacol. 2004; | ||
Emanuele E. NGF and romantic love. Arch Ital Biol. 2011;149(2):265–268. | ||
Schaevitz LR, Moriuchi JM, Nag N, Mellot TJ, Berger-Sweeney J. Cognitive and social functions and growth factors in a mouse model of Rett syndrome. Physiol Behav. 2010;100(3):255–263. | ||
Hellweg R. Trophic factors during normal brain aging and after functional damage. J Neural Transm Suppl. 1994;44:209–217. | ||
Ari C, Borysov SI, Wu J, Padmanabhan J, Potter H. Alzheimer amyloid beta inhibition of Eg5/kinesin 5 reduces neurotrophin and/or transmitter receptor function. Neurobiol Aging. 2014;35(8):1839–1849. | ||
Yegla B, Parikh V. Effects of sustained proNGF blockade on attentional capacities in aged rats with compromised cholinergic system. Neuroscience. 2014;261:118–132. | ||
Conner JM, Franks KM, Titterness AK, et al. NGF is essential for hippocampal plasticity and learning. J Neurosci. 2009;29(35): | ||
Alleva E, Francia N. Psychiatric vulnerability: suggestions from animal models and role of neurotrophins. Neurosci Biobehav Rev. 2009;33(4):525–536. | ||
Axelrod J, Reisine TD. Stress hormones: their interaction and regulation. Science. 1984;224(4648):452–459. | ||
Angelucci F, Aloe L, Vasquez PJ, Mathé AA. Mapping the differences in the brain concentration of brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF) in an animal model of depression. Neuroreport. 2000;11(6):1369–1373. | ||
Barbosa IG, Huguet RB, Sousa LP, et al. Circulating levels of GDNF in bipolar disorder. Neurosci Lett. 2011;502(2):103–106. | ||
Fontenelle LF, Barbosa IG, Luna JV, Rocha NP, Silva Miranda A, Teixeira AL. Neurotrophic factors in obsessive-compulsive disorder. Psychiatry Res. 2012;199(3):195–200. | ||
Jockers-Scherübl MC, Zubraegel D, Baer T, et al. Nerve growth factor serum concentrations rise after successful cognitive-behavioural therapy of generalized anxiety disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(1):200–204. | ||
Kheirouri S, Noorazar SG, Alizadeh M, Dana-Alamdari L. Elevated brainderived neurotrophic factor correlates negatively with severity and duration of major depressive episodes. Cogn Behav Neurol. 2016;29(1):24–31. | ||
Fink M. Neuroendocrinology and ECT: a review of recent developments. Compr Psychiatry. 1980;21(6):450–459. | ||
Hassanzadeh P, Rahimpour S. The cannabinergic system is implicated in the upregulation of central NGF protein by psychotropic drugs. Psychopharmacology (Berl). 2011;215(1):129–141. | ||
Gümrü S, Arıcıo-lu F. Neurotrophic Factors and Depression: Pathophysiology and Beyond. J Marmara Univ Inst Heal Sci. 2012;2(2):53–56. | ||
Chen YW, Lin PY, Tu KY, Cheng YS, Wu CK, Tseng PT. Significantly lower nerve growth factor levels in patients with major depressive disorder than in healthy subjects: a meta-analysis and systematic review. Neuropsychiatr Dis Treat. 2015;11:925–933. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.