Back to Journals » Clinical Interventions in Aging » Volume 15
Medication Reconciliation Associated with Comprehensive Geriatric Assessment in Older Patients with Cancer: ChimioAge Study
Authors Couderc AL, Boisseranc C, Rey D, Nouguerede E, Greillier L, Barlesi F, Duffaud F, Deville L, Honoré S, Villani P, Correard F
Received 14 May 2020
Accepted for publication 30 July 2020
Published 8 September 2020 Volume 2020:15 Pages 1587—1598
DOI https://doi.org/10.2147/CIA.S262209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Anne-Laure Couderc,1,2 Celia Boisseranc,3 Dominique Rey,1 Emilie Nouguerede,1 Laurent Greillier,4,5 Fabrice Barlesi,4,5 Florence Duffaud,4,6 Jean-Laurent Deville,6 Stéphane Honoré,3,4 Patrick Villani,1,2 Florian Correard3,4
1Internal Medicine, Geriatry and Therapeutic Unit, AP-HM, Marseille, France;Coordination Unit for Geriatric Oncology (UCOG), PACA West, Marseille, France; 2Aix-Marseille Université, CNRS, EFS, ADES, Marseille, France; 3Pharmacology Department, AP-HM, Marseille, France; 4Aix-Marseille University, Marseille, France; 5Multidisciplinary Oncology and Therapeutic Innovations Unit, AP-HM, Marseille, France; 6Oncology Unit, AP-HM, Marseille, France
Correspondence: Anne-Laure Couderc
Coordination Unit for Geriatric Oncology (UCOG), PACA West, University Hospital of Marseille (AP-HM), 270 Boulevard De Sainte Marguerite, Marseille 13009, France
Tel +33 491744530
Fax +33 491744833
Email [email protected]
Background: Polymorbidity induces polypharmacy in older patients may lead to potential drug–drug interactions (DDI) which can modify the tolerance and safety of oncological treatments and alter the intended therapeutic effect. The objective of our study was to describe the decision-making process for oncological treatment and related outcomes, in a population of older adults undergoing a comprehensive geriatric assessment (CGA) associated to a comprehensive medication reconciliation (CMR) prior to initiating oncological treatment.
Methods: ChimioAge is a prospective observational study conducted between 01/2017 and 07/2018 at Marseille University Hospital and approved by the French National Ethics Committee. It comprised all consecutive patients aged 70 years and over who were referred for a CGA as part of CMR, before initiating systemic treatment.
Results: One hundred and seventy-one cancer patients were included. Mean age was 79.2 years, over half had metastatic cancers, 75% had an ECOG performance status zero or one, and two-thirds were independent in daily activities. Two-thirds of the patients had polypharmacy and the CMR identified potential DDI with systemic treatment in 43.3% of patients. Following the CGA, the CMR and the hospital oncologists decision, 30% of the patients received adapted systemic treatment with reduced doses at initiation. They presented fewer toxicities – irrespective of grade and type – than patients who received standard treatment (p< 0.001) and had comparable overall survival (Log rank p=0.21).
Conclusion: This is one of the first studies to highlight the value in conducting CMR and a CGA simultaneously before initiating systemic treatment in older patients with cancer. These two evaluations could give oncologists decisive information to personalize cancer treatment of older patients and optimize treatment dose to offer the best efficacy and minimize toxicity.
Keywords: aged, antineoplastic protocols, geriatric assessment, medication reconciliation, treatment failure
Introduction
Aging and cancer are closely linked, as aging leads to complex cellular, molecular, and physiological changes associated with accumulation of genetic changes, which can result in the development of cancer.1 Cancer affects nearly 50% of people over 65 years worldwide according to Globocan data,2–4 in the USA, and nearly 60% of people aged 65 years and over in Europe.5,6 Although older patients are the most affected by cancer, they are still under-represented in clinical trials, especially in an oncological setting.7 However, it is known that drug pharmacokinetics change substantially with aging and vary according to the patient’s history. For example, malnutrition is common in older patients with cancer, and results in a decrease in albumin which modifies the pharmacokinetics of drugs that bind strongly to plasma proteins, and hence their efficacy and toxicity.8 Clinical features of older people are heterogeneous, with frequent comorbidities and associated polypharmacy (5 or more drugs per day). When managing older adults with cancer, potential drug interactions (DDI) between these drugs and the chemotherapy delivered should be considered, as these interactions may modify the tolerance of the cancer treatment and alter the intended therapeutic effect.9,10 Recent studies have shown that major DDI are very prevalent in older adults with cancer and are a risk factor for early and unplanned hospitalizations.11,12 In this particular context, the International Society of Geriatric Oncology (SIOG) recently recommended establishing close cooperation with pharmacists as part of the Comprehensive Geriatric Assessment (CGA)13 in order to review prescriptions of older patients with cancer and avoid adverse side effects of treatment.14 This pharmaceutical intervention is called comprehensive medication reconciliation (CMR)15,16 and the clinical pharmacist is fully integrated into the multidisciplinary team.17 The ChimioAge study was implemented in our hospital in January 2017, to evaluate the impact of the association CGA-CMR on the oncological management of older cancer patients. The aims of the following analysis were to describe the potential impact of the geriatric and pharmaceutical advice provided on dose reduction of oncological treatment, early discontinuation and toxicities.
Methods
Study Design
The ChimioAge study is a prospective observational study.
Study Duration, Site and Sample Size
Between January 2017 and July 2018, 171 patients were enrolled at Marseille University Hospital (AP-HM).
Participants
All consecutive patients, aged 70 years or over referred for geriatric advice before initiation of systemic treatment.
Inclusion Criteria
Patients included were 70 years and older, who agreed to participate in the ChimioAge Study, underwent both CGA and CMR, and received systemic treatment. Systemic treatment included cytotoxic therapy and/or targeted therapy and/or immunotherapy.
Exclusion Criteria
Patients under guardianship or curatorship who were currently enrolled in another clinical study were excluded from the study.
Ethical Approval
In accordance with the declaration of Helsinki, the study protocol was submitted and approved by an Ethics Committee (CPP Ouest IV – Nantes registered 61/18_3) and registered in ClinicalTrials.gov (NCT03960593).
Data Collection and Measurements at Baseline
A multidisciplinary team comprising a geriatrician, pharmacists, nutritionists, and nurses collected the data. A hospital pharmacist first conducted a systematic review of all the medications each patient was taking in order to detect drugs that can cause interactions with oncologic systemic treatment. Drugs informations were collected from the patient and/or caregiver, the most recent medical prescription, and the patient’s medical record. The CMR included indications and doses of the prescribed drugs, as well as an evaluation of self-administration of non-prescribed medication and consumption of medicinal products (phytotherapy, herbs and spices).
All the medications were classified according to the Anatomical Therapeutic Chemical (ATC) classification, as recommended by the World Health Organization. The pharmaceutical analysis was performed using Vidal Hoptimal® and Drugs.com® and DDI was performed using STOPP criteria.18 Polypharmacy was defined as the simultaneous use of a minimum of five prescribed medications.
A geriatrician collected the different components of the CGA: G8 screening tool (impaired ≤ 14/17),19 vulnerability score (ECOG-PS) (impaired ≥ 2),20 Activities of Daily Living (ADL) (impaired < 6/6),21 Instrumental Activities of Daily Living (IADL) scales (impaired < 4/4).22 Cognitive disorders and depressive mood were respectively assessed by the Mini Mental State Examination scale (MMSE) (impaired MMSE < 24),23 and the short Geriatric Depression scale (impaired GDS≤1/4).24 Body Mass Index (BMI), albumin levels, and Mini Nutritional Assessment scale (MNA)25 were used to determine the nutritional status as defined by the French Department of Health (malnutrition = BMI < 21 and/or albumin levels < 35 g/l and/or MNA < 17)). Patients’ mobility was assessed using gait speed (impaired < 0.8m/s),26 Timed Up and Go Test (impaired TUG > 20s),27 One Leg Balance test (impaired OLBT < 5s),28 fall history over the past three months, and handgrip strength (impaired < 27 kg for men; < 16 kg for women)29). Patients were asked about their demographic characteristics and lifestyle (age, living place, and presence of a caregiver). Severe comorbidities were identified using the geriatric Cumulative Illness Rating Scale (CIRS-G).30 Primary medical information was obtained from the medical records: cancer site and stage, detailed treatment, and biological data. Renal function was assessed using the Cockcroft creatinine clearance (renal failure if clearance < 30 µmol/L), anemia was defined by a level of hemoglobin ≤ 11.5 g/dl, thrombopenia was defined by a platelets level <150 G/l and lymphopenia by a lymphocytes level <1.26 G/l.
At the end of the CGA, the geriatrician adapted the patient’s treatment according to the CMR results and gave recommendations to the patient to avoid self-medication, herbals and spice that could interfere with oncological treatment.
Follow-Up Data and Measurements
Data on cancer progression and treatment were obtained from medical records: number of systemic treatment cycles, toxicities, oncologic treatment adaptation (ie, dose reduction) and premature discontinuation, as well as causes for treatment adaptation and discontinuation.
A total number of frailties (from 0 to 6) was computed by giving 1 point to each of the following frailties: CIRS-G severe comorbidities, malnutrition, polypharmacy, cognitive disorders, impaired mobility and/or handgrip strength decrease, impaired autonomy for the instrumental activities of daily living. These particular frailties were selected by the geriatrician as the main domains used to determine systemic treatment dose adaptation. The hospital pharmacist conducted follow-up calls with the patients at 30, 60, and 90 days after enrollment to collect information about unplanned hospitalizations and overall survival (OS) (collected up to January 2019).
Premature systemic treatment discontinuation was defined as treatment discontinuation before the fourth systemic treatment cycle related to cancer progression, toxicity, other reasons or death. OS was defined as the time between date of CGA and date of death or last known follow-up.
Statistical Analysis
A descriptive analysis was performed to describe the main demographic, oncological, geriatric, and treatment characteristics of our population using headcounts and percentages for discrete data as well as mean values plus or minus the standard error and the interval between the minimum and maximum values for continuous data. Comparative analysis were performed to compare patients according to initial doses of systemic therapy (reduced doses vs standard doses), premature systemic treatment discontinuation (yes vs no), and presence of toxicities grade 3–5 (yes vs no). The Chi-squared test was used to analyze discrete data whereas Student’s t-test was used to analyze continuous variables. A Kaplan-Meier analysis was used to compare the overall survival rates in two groups of patients: those who received reduced doses at systemic therapy initiation, and those who received standard doses. All the statistical analyses were performed using SPSS software (version 17.0).
Results
Descriptive Analysis
A total of 171 older patients with cancer who received systemic treatment after a CGA and a CMR were included in the survey.
Socio-demographic and baseline medical characteristics of the study population are detailed in Table 1. The mean age was 79.2 years (SD 5.2). Only 10 patients had hematologic malignancies, and nearly one-third had lung cancer. A majority of patients with solid tumors had metastatic cancer (53.2%). Table 2 displays the results of the CGA. Most patients had good performance status (74.9% patients with ECOG-PS score 0 or 1) and 66.1% of patients were independent in daily activities. The mean number of frailties per patient was 2.3 ±1.4 (from 0 to 6).
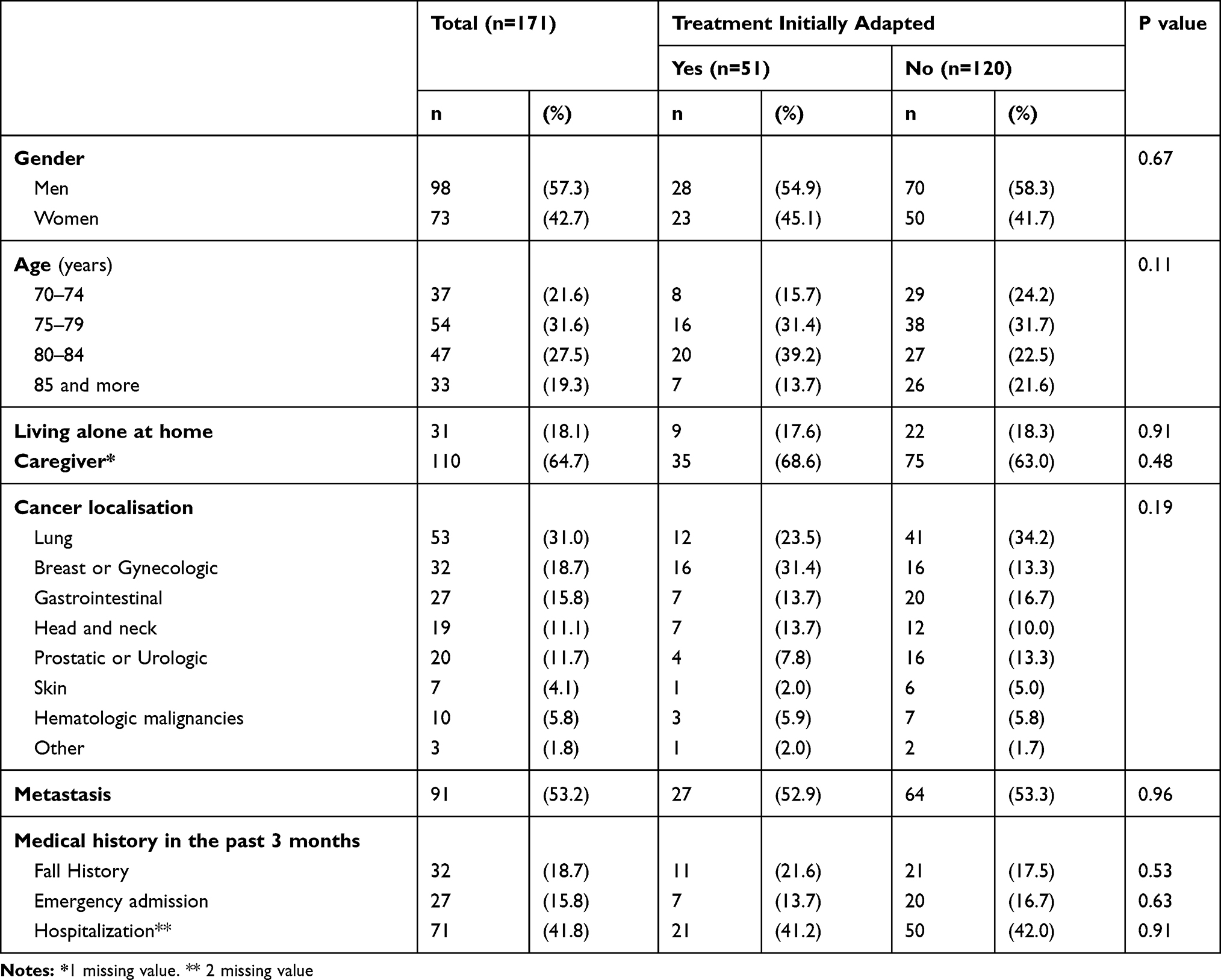 |
Table 1 Socio-Demographic and Medical Characteristics at Baseline According to Systemic Therapy (Standard Doses vs Reduced Doses at Initiation) (n=171) |
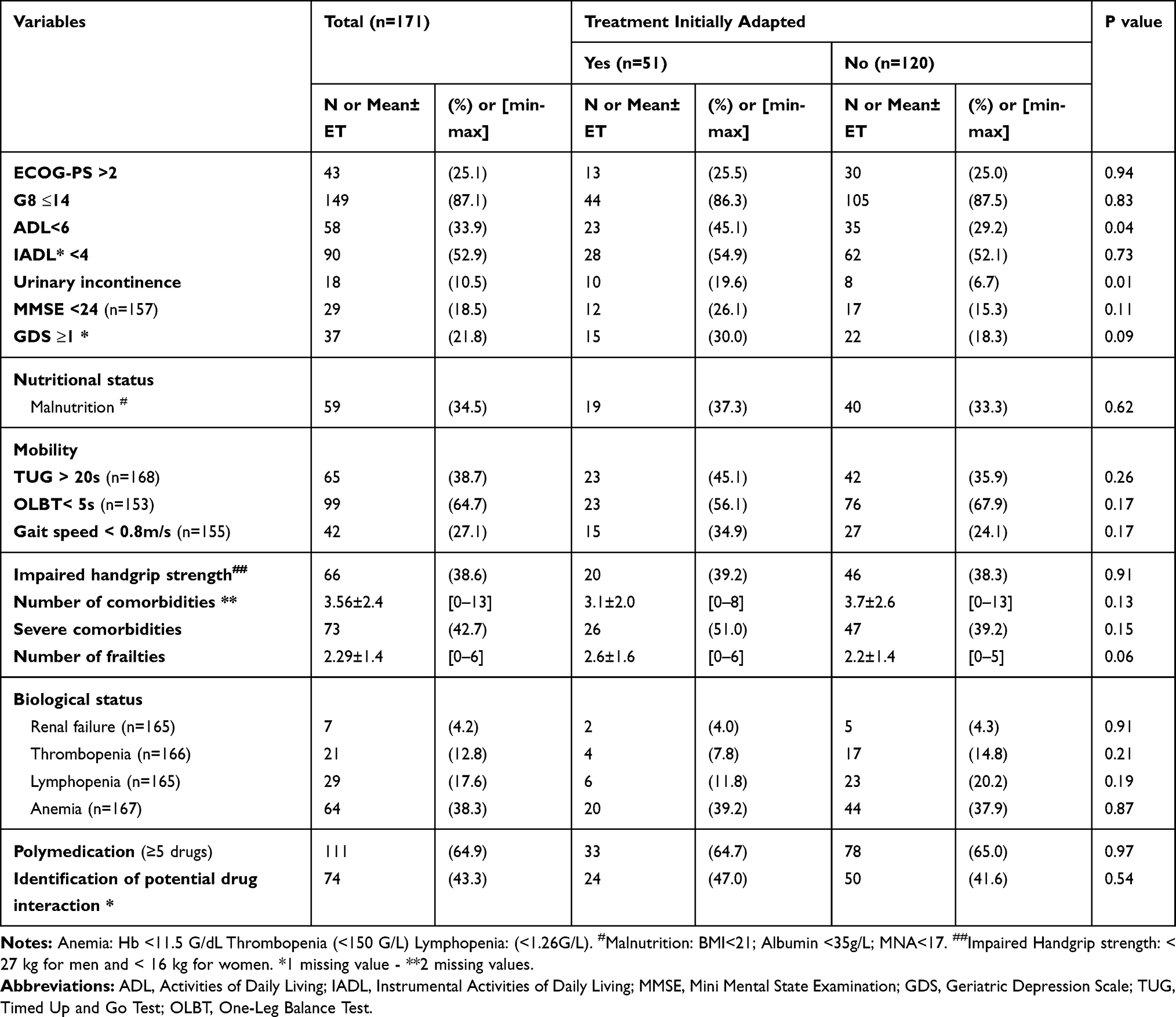 |
Table 2 Geriatric and Pharmacological Characteristics at Baseline According to Systemic Therapy (Standard Doses vs Reduced Doses at Initiation) (n=171) |
Nearly two-thirds of the patients were prescribed more than five drugs (64.9%), and the medication reconciliation identified potential interactions with oncologic treatment in 74 patients (43.3%). Personal drugs were adapted in accordance with General Practitioners (GPs) to take into account the potential DDI.
All patients received cancer systemic treatment; the majority received chemotherapy (74.1%) (Table 3).
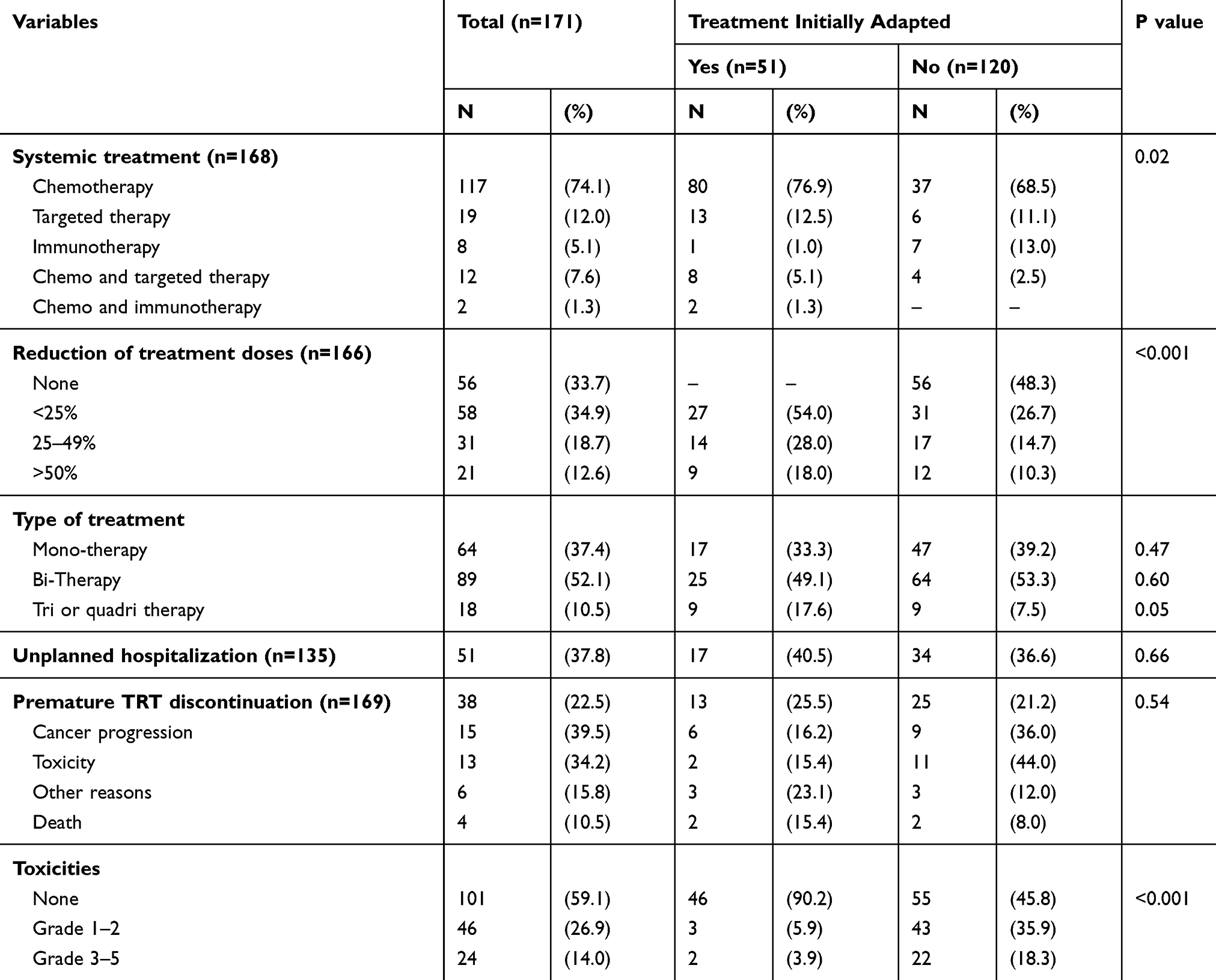 |
Table 3 Clinical Follow-Up Data 3 Months After Treatment Initiation According to Systemic Therapy (Standard Doses vs Reduced Doses at Initiation) (n=171) |
Dose Reduction at Treatment Initiation
A total of 51 patients (29.8%) received reduced doses of systemic treatment at initiation. In the majority of cases (75%), reduction of doses at treatment initiation was made according to the recommendations of both CGA and CMR. Decision of treatment reduction was more often observed in patients dependent on activities for daily living (Table 2).
Only 33.7% of the whole sample received full standard treatment, 29.8% received adapted treatment and 35% had further dose reduction during the treatment course. Toxicities were much more frequent in patients who benefited from standard treatment than patients whose treatment was initially adapted (54.2% vs 9.8% - p<0.001) (Table 3).
Figure 1 depicts the 2-year OS by treatment modality (initially adapted treatment vs standard treatment). Median OS was higher in patients who received standard doses of systemic treatment at initiation, but the difference did not reach statistical significance (Log rank p=0.21).
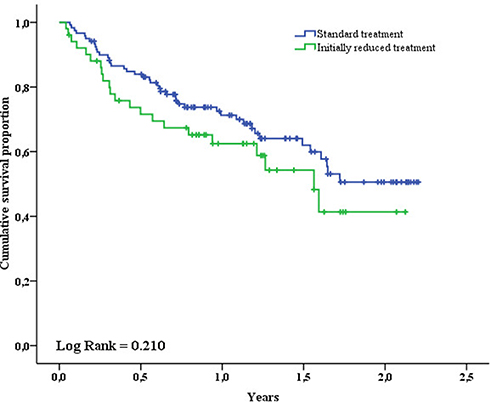 |
Figure 1 Overall survival standard treatment versus adapted treatment. |
Premature Discontinuation of Systemic Treatment
Systemic treatment was prematurely discontinued in 38 patients (22.5%). Causes for discontinuation were disease progression (n=15), toxicity (n=13), other reasons (n=6), and death (n=4) (Table 3). A univariate comparative analysis showed that early oncological treatment discontinuation was more often observed in men, aged 80 to 84 years, and in patients suffering from lung or gastrointestinal cancer. No geriatric characteristic was associated with premature systemic treatment discontinuation (Table 4).
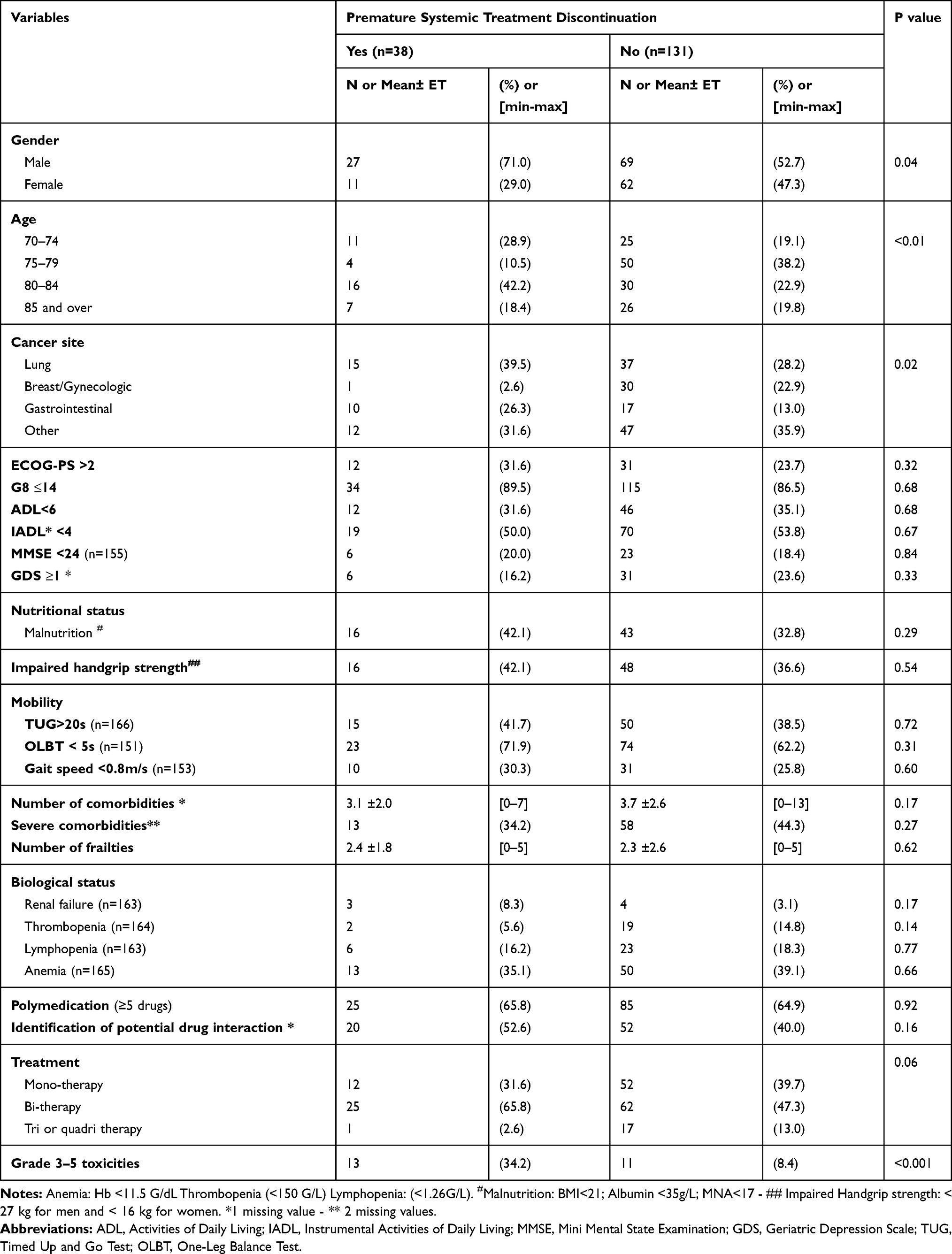 |
Table 4 Patient’s Characteristics at Baseline According to Premature Systemic Treatment Discontinuation (n=169) |
Toxicities
A total of 70 patients (40.9%) suffered from toxicities, and 24 of these from severe toxicities (10/24 hematological toxicities, 5/24 digestive toxicities and 9/24 other toxicities (including neuropathy, skin toxicities and asthenia)). Grade 3–5 toxicities were mostly observed in patient who benefited from standard treatment and were the major cause of premature treatment discontinuation (Tables 3 and 4). The occurrence of toxicities was independent of patients’ geriatric characteristics (Table 5).
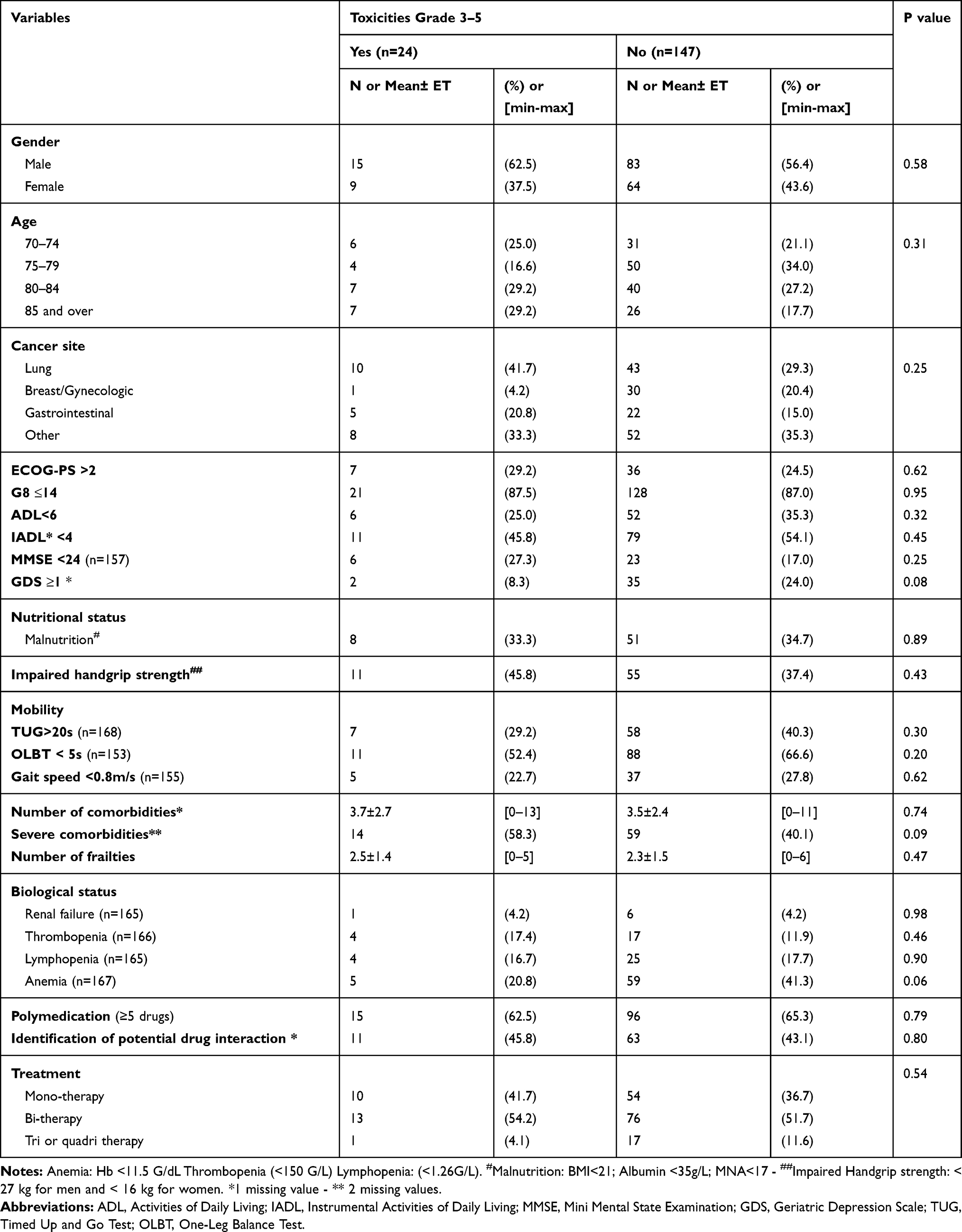 |
Table 5 Patient’s Characteristics at Baseline According to Presence of Toxicities Grade 3–5 (n=171) |
Discussion
This is one of the first studies to show the potential benefits of a close collaboration between oncologists, geriatrician and pharmacists for older patients with cancer before initiation of systemic treatment. Our results showed the high frequency of polypharmacy (65%) and potential DDI (43%) among older cancer patients, and confirmed the major utility of using CGA to assess frailties and to detect potential DDI and oncological treatment interactions in older adults before the initiation of cancer management. In our study, the dose reduction at oncological treatment initiation after CGA and CMR association reduced grade 3–5 toxicities in older adults treated for cancer and had no significant impact on their overall survival.
In our survey, systemic treatment was initially adapted for 29.8% of the patients. In a review by Hamaker et al,31 after CGA, oncological treatment was changed by oncologists for a median of 28% of patients (range 8–54%), and these modifications resulted in the decision to adopt a less intensive treatment in the majority of cases. Moreover, further dose reduction during the course of systemic treatment concerned 35% of our patients, in accordance with literature. Kotzerke et al, showed that the dose reduction rate during systemic treatment reached 38% in a cohort of 104 older patients treated with chemotherapy,32 and 31% in a sample population of 494 patients treated with chemotherapy in Aaldriks et al.33 Chemotherapy dose reduction is controversial because it may lead to a reduction in relative dose intensity and compromise treatment efficacy. Some studies have shown that chemotherapy toxicity in older adults was probably counterbalanced by the positive effect of oncological standard systemic treatment.34 However, as already reported in the literature,31 we found that initial treatment reduction had no negative impact on the overall survival of older patients with cancer.
In practice, many reasons may lead oncologists to modify chemotherapy doses in older adults. Nevertheless, in the literature, the respective impact of CGA and clinical judgement in these modifications is unclear. CGA domains or tumor type have never been proven to be associated with dose reduction, particularly at treatment initiation.35–39 In our work, two thirds of initial dose reductions were secondary to CGA and CMR advice, and we found that two geriatric factors were associated with initial dose reduction: autonomy impairment in the activities of daily living and urinary incontinence. This confirms findings of a previous study, where we showed that functional impairment was decisive for cancer management in older patients.40 Even when the geriatric characteristics of the patients (assessed by the CGA) do not contra-indicate systemic treatment for their cancer, a minor loss of autonomy or the presence of minor frailties may lead the geriatrician to recommend an adaptation of cancer treatment.
In our study, the use of a systemic treatment based on tri or quadri-therapy was another factor associated with initial dose reduction in older adults treated for cancer. Polychemotherapy and systemic therapy associations are known to be associated with toxicity.39,41,42 In particular polychemotherapy carries a higher risk of toxicity than monotherapy,39,41,43 which may lead the oncologists to decrease initial polychemotherapy doses. Two scores have recently been developed to predict severe chemotherapy toxicity in older patients: the CARG score (Cancer and Aging Research Group score)41 and the CRASH score (Chemotherapy Risk Assessment Scale for High-Age Patients).42 They are not yet used in routine practice by oncologists and they could be recommended to guide chemotherapy management32 as part of multidisciplinary care of older patients.
Toxicity rates found in our study were lower than those previously described, irrespective of toxicity grade. Fourteen percent of the sample population presented grade 3–5 toxicities, although around 57–64% severe grade of toxicities are usually reported in the literature.32,44,45 The percentage of severe toxicities was even lower in patients with initially reduced treatment (4%) than in patients with standard treatment (18%). The difference observed in frequency of grade 3–5 toxicity in our study compared to others may also be imputable to the multidisciplinary management set up after CGA and CMR. CMR recommendations, associated with geriatricians’ interventions have been effective at identifying and managing geriatric frailties and medication-related risks,46,47 and at decreasing severe chemotherapy toxicity.48 This decrease of toxicity rate, including grade 1–2 toxicities, is important to preserve functional status and quality of life of older patients. Indeed, decreasing the frequency of lower-grade toxicities has been shown to be as important as decreasing the frequency of higher-grade toxicities for optimizing quality of life domains.49 Consequently, oncologists may choose to modify or stop systemic treatment to protect older patients from lower-grade toxicities and preserve their quality of life.44 In this regard, appropriate adaptation of the treatment is an important step to decrease both lower- and higher-grade toxicities as shown in our data (Table 3). Management of high-grade toxicities encompass hospital care, as recommended by ASCO and ESMO, and is responsible for unplanned hospitalizations. By decreasing the incidence of severe toxicities, CMR associated with CGA could also help to reduce healthcare costs.50
In the literature, chemotherapy toxicity was associated with age,51 geriatric factors as cognitive troubles39 or comorbid conditions.45 Geriatric factors were not associated with systemic therapy toxicity in our work, showing that adequate geriatric management may reduce or even eliminate frailties linked toxicities.
The systemic treatment discontinuation rate of 22.5% found in our study is consistent with literature findings that report treatment discontinuation rates between 24 and 40%.32,52 According to our results, toxicity was the second most common cause of systemic treatment discontinuation after disease progression, concurring with literature32,33,52 and geriatric factors were not associated to chemotherapy discontinuation, controversially with other studies.33,52–54 This important finding confirms the benefits of performing a CGA before deciding on oncological treatment in older patients, as recommended at international level.13 A majority of the patients of our study sample had a G8 ≤ 14 but few had impaired functional status, cognitive disorders, malnutrition or mobility impairment, and all were considered as “not frail” and apt to receive oncological treatment after the CGA and the implementation of CGA interventions. This is in line with the results of Kalsi et al47 who showed an association between CGA interventions and improvement of chemotherapy tolerance in older cancer patients. Carrying out the CMR at the same time with CGA by a multidisciplinary team including a clinical pharmacist,55 in order to search potential DDI and avoid iatrogenia, can explain the lack of observed association between polypharmacy and systemic therapy discontinuation in our survey, as previously shown elsewhere.56,57
Associations between chemotherapy discontinuation and tumor site or chemotherapy regimen have already been reported.45,52,58 In older cancer patients, lung and digestive cancers have worse prognoses than other cancers.5 This may be one explanation for the highest frequency of chemotherapy discontinuation with these specific cancer localizations. Systemic treatment discontinuation is important in determining outcome of older patients treated for cancer as it is strongly associated with mortality in literature (in Fairfield et al58).
The present study has limitations. It was monocentric in design, including patients with all types of cancer and all types of systemic treatment. The heterogeneity of our study sample resulted in a lack of power for statistical analyses in subgroups of patients. Another difficulty was to perform CMR with the usual DDI tools (2012 Beers criteria and STOPP criteria), which are not designed for older people treated for cancer, and to take into account oncological systemic treatment. Finally, this is an observational study with no controlled group, and our results have to be confirmed in larger randomized studies.
The strengths of our study include new findings on outcomes in a population of older patients with initially adapted oncological treatment. Furthermore, few studies to date have incorporated concurrent CGA and CMR and evaluated the impact of these two assessments on oncological treatment decision-making and on older patients’ outcomes. This multidisciplinary cooperation (oncologists, geriatricians and pharmacists) reflects the routine practice of the Coordination Unit for Geriatric Oncology in PACA West since 2017. Our findings highlight that this collaboration should be more largely considered in future clinical practice.
Conclusion
Older patients have frequent comorbidities, frailties and associated polypharmacy, exposing them to a high medication risk. This risk is even higher in older adults with cancer receiving chemotherapy or targeted therapy and it may lead to interruptions in cancer treatment with negative consequences on patient survival. The systematic collaboration between oncologists, geriatricians and pharmacists is essential to implement a personalized care plan in geriatric oncology. In our survey, initial treatment dose adaptation following CGA and CMR had no significant impact on overall survival and reduced grade 3–5 toxicities in older adults treated for cancer. All grades of toxicity were lowered, and discontinuation rate was comparable to those reported in the literature among older cancer patients. This CGA and CMR association is a plus to avoid DDI and improve oncological treatment initial dose decision-making, leading to better tolerance of systemic treatment in older adults.
Data Sharing Statement
Patient consent did not allow public data to be shared. To abide by French law, all requests for data, whether for analysis verification or meta-analyses, must be addressed to the corresponding author.
Acknowledgments
This work is supported by French Ministry of Health: Appel à projet pharmacie Clinique (DGOS/PF2/2016-49). The funding body had no role in design of the study, the collection and analysis of data or in the writing of the manuscript. The authors would like to thank all patients and GPs who agreed to participate in this work. The authors would like to thank Jude Sweeney for his proofreading.
Author Contributions
All authors made substantial contributions to the study’s conception and design, acquisition of data, and analysis and interpretation of data. All participated in drafting the article or revising it critically for important intellectual content. All gave final approval for the version to be published and agreed to be accountable for all aspects of the work.
Disclosure
Laurent Greillier reports personal fees and non-financial support from ABBVIE, ASTRA-ZENECA, BOEHRINGER INGELHEIM, BMS, MSD, and ROCHE and personal fees from TAKEDA, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Di Silvestro K, Pautex S, Pugliesi A. [Cancer and aging: an epidemiological fact]. Rev Med Suisse. 2011;7(296):
2. Estimated number of new cases in 2018, worldwide both sexes, all ages. Accessed April 22, 2020. https://gco.iarc.fr/today/online-analysis-pie?v=2018&mode=cancer&mode_population=who&population=900&populations=900&key=total&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17items=7&group_cancer=1&include_nmsc=1&include_nmsc_other=1&half_pie=0&donut=0&population_group_globocan_id=#collapse-others.
3. Estimated number of new cases in 2018, worldwide both sexes, age 65+. Accessed April 22, 2020. https://gco.iarc.fr/today/online-analysis-pie?v=2018&mode=cancer&mode_population=who&population=900&populations=900&key=total&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=13&ages_group%5B%5D=17items=7&group_cancer=1&include_nmsc=1&include_nmsc_other=1&half_pie=0&donut=0&population_group_globocan_id=.
4. Estimated number of new cases in 2018, worldwide both sexes, age 0-64.
5. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. doi:10.1016/j.ejca.2018.07.005
6. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. doi:10.3322/caac.21332
7. Ruiter R, Burggraaf J, Rissmann R. Under-representation of elderly in clinical trials: an analysis of the initial approval documents in the Food and Drug Administration database. Br J Clin Pharmacol. 2019;85(4):838–844. doi:10.1111/bcp.13876
8. Walter-Sack I, Klotz U. Influence of diet and nutritional status on drug metabolism. Clin Pharmacokinet. 1996;31(1):47–64. doi:10.2165/00003088-199631010-00004
9. Balducci L. Frailty: a common pathway in aging and cancer. Interdiscip Top Gerontol. 2013;38:61–72. doi:10.1159/000343586
10. Popa MA, Wallace KJ, Brunello A, Extermann M, Balducci L. Potential drug interactions and chemotoxicity in older patients with cancer receiving chemotherapy. J Geriatr Oncol. 2014;5(3):307–314. doi:10.1016/j.jgo.2014.04.002
11. Nightingale G, Pizzi LT, Barlow A, et al. The prevalence of major drug-drug interactions in older adults with cancer and the role of clinical decision support software. J Geriatr Oncol. 2018;9(5):526–533. doi:10.1016/j.jgo.2018.02.001
12. Beinse G, Reitter D, Segaux L, et al. Potential drug-drug interactions and risk of unplanned hospitalization in older patients with cancer: A survey of the prospective ELCAPA (ELderly CAncer PAtients) cohort. J Geriatr Oncol. 2019. doi:10.1016/j.jgo.2019.07.023
13. Mohile SG, Dale W, Somerfield MR, et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J Clin Oncol. 2018;36(22):2326–2347. doi:10.1200/JCO.2018.78.8687
14. Scotte F, Bossi P, Carola E, et al. Addressing the quality of life needs of older patients with cancer: a SIOG consensus paper and practical guide. Ann Oncol. 2018;29(8):1718–1726. doi:10.1093/annonc/mdy228
15. Son H, Kim J, Kim C, Ju J, Lee Y, Rhie SJ. Pharmacist-led interdisciplinary medication reconciliation using comprehensive medication review in gynaecological oncology patients: a prospective study. Eur J Hosp Pharm. 2018;25(1):21–25. doi:10.1136/ejhpharm-2016-000937
16. Mekonnen AB, McLachlan AJ, Brien J-AE. Pharmacy-led medication reconciliation programmes at hospital transitions: a systematic review and meta-analysis. J Clin Pharm Ther. 2016;41(2):128–144. doi:10.1111/jcpt.12364
17. Shrestha S, Shrestha S, Khanal S. Polypharmacy in elderly cancer patients: challenges and the way clinical pharmacists can contribute in resource‐limited settings. Aging Med. 2019;2(1):42–49. doi:10.1002/agm2.12051
18. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. doi:10.1093/ageing/afu145
19. Soubeyran P, Bellera C, Goyard J, et al. Screening for vulnerability in older cancer patients: the ONCODAGE Prospective Multicenter Cohort Study. PLoS One. 2014;9(12):e115060. doi:10.1371/journal.pone.0115060
20. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655. doi:10.1097/00000421-198212000-00014
21. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. STUDIES OF ILLNESS IN THE AGED. THE INDEX OF ADL: A STANDARDIZED MEASURE OF BIOLOGICAL AND PSYCHOSOCIAL FUNCTION. JAMA. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
22. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. doi:10.1093/geront/9.3_Part_1.179
23. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
24. Yesavage JA. Geriatric Depression Scale. Psychopharmacol Bull. 1988;24(4):709–711.
25. Guigoz Y, Vellas B, Garry PJ. Mini Nutritional Assessment: a practical assessment tool for grading the nutritional state of elderly patients. Facts Res Gerontol. 1994;12–13.
26. Friedman PJ, Richmond DE, Baskett JJ. A prospective trial of serial gait speed as a measure of rehabilitation in the elderly. Age Ageing. 1988;17(4):227–235. doi:10.1093/ageing/17.4.227
27. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
28. Vellas BJ, Wayne SJ, Romero L, Baumgartner RN, Rubenstein LZ, Garry PJ. One-leg balance is an important predictor of injurious falls in older persons. J Am Geriatr Soc. 1997;45(6):735–738. doi:10.1111/j.1532-5415.1997.tb01479.x
29. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601. doi:10.1093/ageing/afz046
30. Miller MD, Paradis CF, Houck PR, et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992;41(3):237–248. doi:10.1016/0165-1781(92)90005-n
31. Hamaker ME, Te Molder M, Thielen N, van Munster BC, Schiphorst AH, van Huis LH. The effect of a geriatric evaluation on treatment decisions and outcome for older cancer patients - A systematic review. J Geriatr Oncol. 2018;9(5):430–440. doi:10.1016/j.jgo.2018.03.014
32. Kotzerke D, Moritz F, Mantovani L, et al. The performance of three oncogeriatric screening tools - G8, optimised G8 and CARG - in predicting chemotherapy-related toxicity in older patients with cancer. A prospective clinical study. J Geriatr Oncol. 2019;10(6):937–943. doi:10.1016/j.jgo.2019.04.004
33. Aaldriks AA, Maartense E, Nortier HJWR, et al. Prognostic factors for the feasibility of chemotherapy and the Geriatric Prognostic Index (GPI) as risk profile for mortality before chemotherapy in the elderly. Acta Oncol. 2016;55(1):15–23. doi:10.3109/0284186X.2015.1068446
34. Hurria A, Hurria A, Zuckerman E, et al. A prospective, longitudinal study of the functional status and quality of life of older patients with breast cancer receiving adjuvant chemotherapy. J Am Geriatr Soc. 2006;54(7):1119–1124. doi:10.1111/j.1532-5415.2006.00789.x
35. Basso U, Tonti S, Bassi C, et al. Management of Frail and Not-Frail elderly cancer patients in a hospital-based geriatric oncology program. Crit Rev Oncol Hematol. 2008;66(2):163–170. doi:10.1016/j.critrevonc.2007.12.006
36. Lai P, Sud S, Zhang T, Asmis T, Wheatley-Price P. Palliative chemotherapy in advanced colorectal cancer patients 80 years of age and older. Curr Oncol. 2016;23(3):144–153. doi:10.3747/co.23.2996
37. Garg P, Rana F, Gupta R, Buzaianu EM, Guthrie TH. Predictors of toxicity and toxicity profile of adjuvant chemotherapy in elderly breast cancer patients. Breast J. 2009;15(4):404–408. doi:10.1111/j.1524-4741.2009.00745.x
38. Zauderer MG, Sima CS, Korc-Grodzicki B, Kris MG, Krug LM. Toxicity of initial chemotherapy in older patients with lung cancers. J Geriatr Oncol. 2013;4(1):64–70. doi:10.1016/j.jgo.2012.09.003
39. Aparicio T, Jouve J-L, Teillet L, et al. Geriatric factors predict chemotherapy feasibility: ancillary results of FFCD 2001-02 Phase III study in first-line chemotherapy for metastatic colorectal cancer in elderly patients. J Clin Oncol. 2013;31(11):1464–1470. doi:10.1200/JCO.2012.42.9894
40. Couderc A-L, Boulahssass R, Nouguerède E, et al. Functional status in a geriatric oncology setting: A review. J Geriatr Oncol. 2019;10(6):884–894. doi:10.1016/j.jgo.2019.02.004
41. Hurria A, Cirrincione CT, Muss HB, et al. Implementing a geriatric assessment in cooperative group clinical cancer trials: CALGB 360401. J Clin Oncol. 2011;29(10):1290–1296. doi:10.1200/JCO.2010.30.6985
42. Extermann M, Boler I, Reich RR, et al. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer. 2012;118(13):3377–3386. doi:10.1002/cncr.26646
43. Marinello R, Marenco D, Roglia D, et al. Predictors of treatment failures during chemotherapy: A prospective study on 110 older cancer patients. Arch Gerontol Geriatr. 2009;48(2):222–226. doi:10.1016/j.archger.2008.01.011
44. Kalsi T, Babic-Illman G, Fields P, et al. The impact of low-grade toxicity in older people with cancer undergoing chemotherapy. Br J Cancer. 2014;111(12):2224–2228. doi:10.1038/bjc.2014.496
45. Wildes TM, Ruwe AP, Fournier C, et al. Geriatric assessment is associated with completion of chemotherapy, toxicity, and survival in older adults with cancer. J Geriatr Oncol. 2013;4(3):227–234. doi:10.1016/j.jgo.2013.02.002
46. Nightingale G, Skonecki E, Boparai MK. The Impact of Polypharmacy on Patient Outcomes in Older Adults With Cancer. Cancer J. 2017;23(4):211–218. doi:10.1097/PPO.0000000000000277
47. Kalsi T, Babic-Illman G, Ross PJ, et al. The impact of comprehensive geriatric assessment interventions on tolerance to chemotherapy in older people. Br J Cancer. 2015;112(9):1435–1444. doi:10.1038/bjc.2015.120
48. Corre R, Greillier L, Le Caër H, et al. Use of a Comprehensive Geriatric Assessment for the Management of Elderly Patients With Advanced Non-Small-Cell Lung Cancer: the Phase III Randomized ESOGIA-GFPC-GECP 08-02 Study. J Clin Oncol. 2016;34(13):1476–1483. doi:10.1200/JCO.2015.63.5839
49. Schuurhuizen CS, Verheul HM, Braamse AM, et al. The predictive value of cumulative toxicity for quality of life in patients with metastatic colorectal cancer during first-line palliative chemotherapy. Cancer Manag Res. 2018;10:3015–3021. doi:10.2147/CMAR.S166468
50. Niraula S, Amir E, Vera-Badillo F, Seruga B, Ocana A, Tannock IF. Risk of incremental toxicities and associated costs of new anticancer drugs: a meta-analysis. J Clin Oncol. 2014;32(32):3634–3642. doi:10.1200/JCO.2014.55.8437
51. Falandry C, Weber B, Savoye A-M, et al. Development of a geriatric vulnerability score in elderly patients with advanced ovarian cancer treated with first-line carboplatin: a GINECO prospective trial. Ann Oncol. 2013;24(11):2808–2813. doi:10.1093/annonc/mdt360
52. Laurent M, Paillaud E, Tournigand C, et al. Assessment of solid cancer treatment feasibility in older patients: a prospective cohort study. Oncologist. 2014;19(3):275–282. doi:10.1634/theoncologist.2013-0351
53. Soubeyran P, Fonck M, Blanc-Bisson C, et al. Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J Clin Oncol. 2012;30(15):1829–1834. doi:10.1200/JCO.2011.35.7442
54. Honecker F, Wedding U, Kallischnigg G, et al. Risk factors for unplanned discontinuation of scheduled treatment in elderly patients with castration-resistant prostate cancer: results of the IBuTu study. J Cancer Res Clin Oncol. 2018;144(3):571–577. doi:10.1007/s00432-017-2577-1
55. Shrestha S, Shrestha S, Palaian S. Can clinical pharmacists bridge a gap between medical oncologists and patients in resource-limited oncology settings? An experience in Nepal. J Oncol Pharm Pract. 2019;25(3):765–768. doi:10.1177/1078155218784734
56. LeBlanc TW, McNeil MJ, Kamal AH, Currow DC, Abernethy AP. Polypharmacy in patients with advanced cancer and the role of medication discontinuation. Lancet Oncol. 2015;16(7):e333–e341. doi:10.1016/S1470-2045(15)00080-7
57. Colombo LRP, Aguiar PM, Lima TM, Storpirtis S. The effects of pharmacist interventions on adult outpatients with cancer: A systematic review. J Clin Pharm Ther. 2017;42(4):414–424. doi:10.1111/jcpt.12562
58. Fairfield KM, Murray K, Lucas FL, et al. Completion of adjuvant chemotherapy and use of health services for older women with epithelial ovarian cancer. J Clin Oncol. 2011;29(29):3921–3926. doi:10.1200/JCO.2010.34.1552
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.