Back to Journals » Open Access Emergency Medicine » Volume 10
Medical issues in flight and updating the emergency medical kit
Authors Verjee MA ![]() , Crone R
, Crone R ![]() , Ostrovskiy G
, Ostrovskiy G ![]()
Received 28 September 2017
Accepted for publication 15 February 2018
Published 30 April 2018 Volume 2018:10 Pages 47—51
DOI https://doi.org/10.2147/OAEM.S152777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Video abstract presented by Mohamud A Verjee.
Views: 447
Mohamud A Verjee,1 Robert Crone,2 Grigory Ostrovskiy3
1Primary Care Clerkship, Family Medicine in Clinical Medicine, 2Clinical and Faculty Affairs, Clinical Pediatrics and Anesthesiology, 3Emergency Medicine, Weill Cornell Medicine – Qatar, Qatar Foundation – Education City, Doha, Qatar
Abstract: Airline travel is more affordable than ever and likely safer than ever too. Within half a day, a passenger can be on the other side of the world. However, medical care in-flight has been an issue for those with medical conditions and for those who fall sick during a journey. While airlines have the advice of multiple recognized organizations on needs and standards of care, in-flight emergencies occur at various levels. An emergency medical kit (EMK) together with trained cabin crew can be very effective at resolving the minor problems that arise and reducing the risk of escalation. On occasion, an overhead plea may be announced for additional medical expertise. Having the right content in a medical kit is more important in modern day travel, coupled with advances in equipment and passenger expectations. The authors address current issues of illness and other relevant conditions and suggest a content enhancement for an onboard EMK.
Keywords: emergency medical kit, in-flight medical emergency, arterial oxygen partial pressure, pulse oximeter, automated external defibrillator, Federal Aviation Authority, International Civil Aviation Organization
Introduction
An emergency medical kit (EMK) for commercial passenger flights is well established as a supportive health principle. Multiple publications discuss the EMK content, but inconsistencies still abound according to airline policies, geographic routes, and in-flight staff training levels. There is a consensus by the International Air Transport Association (IATA)1,2,25 and the Aerospace Medical Association,3–5 both of whom publish recommendations for the content of onboard EMKs on international flights. The International Academy of Aviation and Space Medicine,6 the American Osteopathic Association,7 and the American College of Emergency Physicians,8 all approved content in collaboration with the American Medical Association9 in 2003 and 2004.1–3.Health care advances and changing philosophies necessitate urgent updates.
Materials and methods
The authors reviewed IATA1 publicly available onboard EMK content for international flights to identify potential areas for improvement, particularly for pediatric passengers in need of arising supportive care. Diagnostic and critical management considerations took precedence. In the authors’ opinion, the modified list (Table 1) would be safer, feasible, and practical to implement. (Recommended changes are printed in bold italic with the original contents left in place for comparison.) In 2004, the Federal Aviation Authority mandated all US commercial airlines should include on-board automated external defibrillators (AEDs) “on passenger flights that are large enough to have at least one flight attendant and to train cabin crew in their use”. No such mandate exists for European airlines to carry AEDs, although many now comply with a recommendation (Resuscitation Council [UK], 2014–2018).10 The authors recommend the inclusion of pulse oximetry for all flights, and this is not a new item for the IATA to consider for widespread implementation.
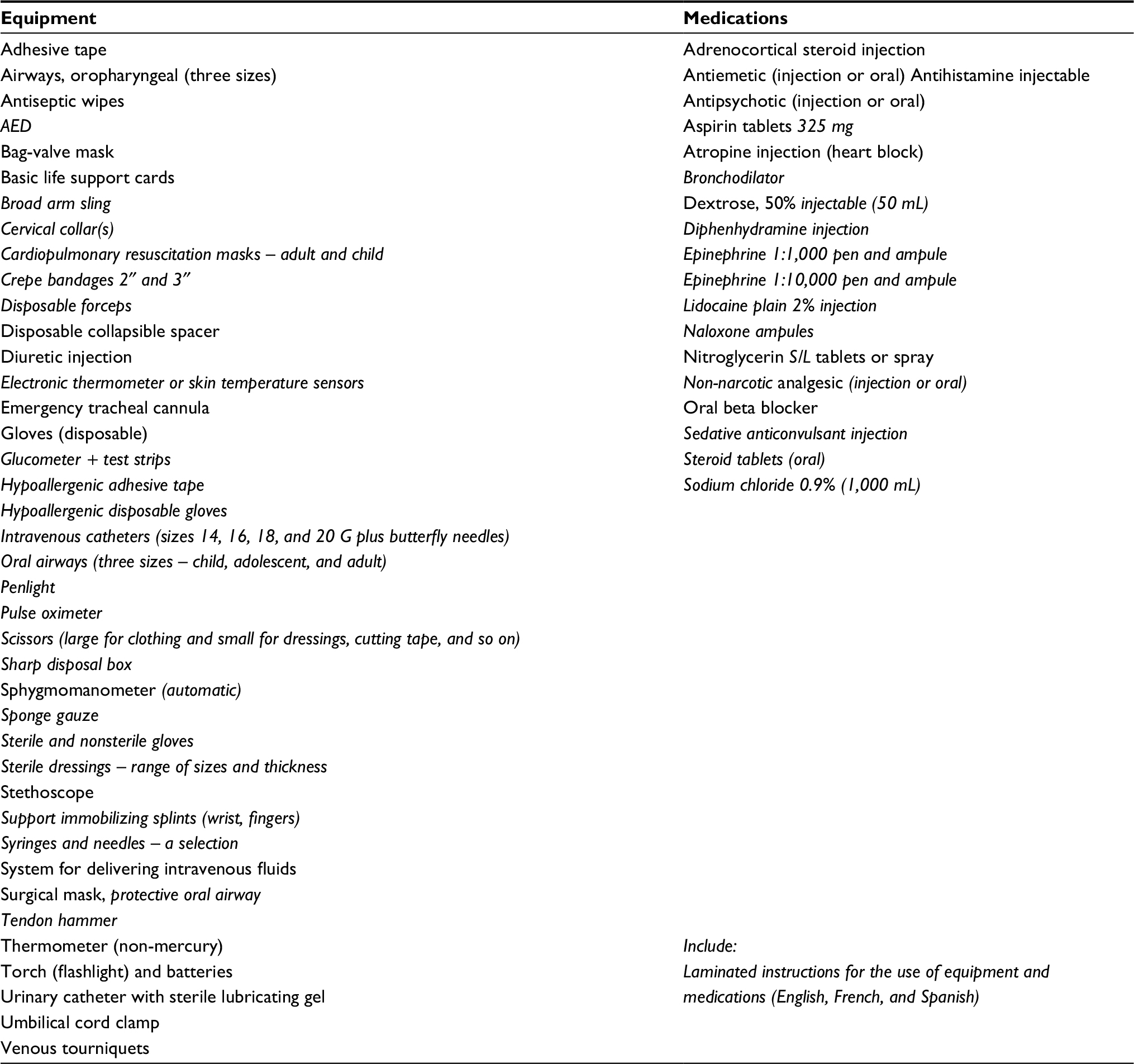 | Table 1 Proposal for modified EMKs fashioned after a list published by the IATAa Note: All ‘new’ items are written in italics. Abbreviations: AED, automated external defibrillator; EMK, emergency medical kit; IATA, International Air Transport Association. |
In 2009, Silverman and Gendreau11 stated that “Environmental and physiological changes that occur during routine commercial flights lead to mild hypoxia and gas expansion, which can exacerbate chronic medical conditions or incite acute in-flight medical events.” The advent of long-haul flights lasting 12–14 hours can cause a more significant adverse effect on vulnerable passengers. Aircraft cruising heights can vary between 7,010 and 12,498 m (23,100–41,000 ft) above sea level. The passenger cabin pressure is equivalent to an altitude of between 1,524 and 2,438 m (5,000–8,000 ft). Arterial oxygen partial pressure (PaO2) can fall from 95 mmHg to as low as 60 mmHg at the highest level of cabin pressure.12
Support for monitoring oxygen levels arose in 2015 from Kesapli et al,13 but routine pulse oximetry is not yet included. In 2011, Ahmedzai et al14 suggested pre-flight screening for passengers with respiratory disorders because of the decrease in PaO2 compromise. Cabin pressure can cause a 10% fall in PaO2, even for entirely healthy passengers. Pulse oximeters would be invaluable in monitoring any compromised passenger. Supplementary oxygen is available for short periods. The Resuscitation Council (UK)10 gives an estimate of ~1,000 passengers dying during commercial flights annually. In-flight medical emergencies (IMEs) appear to be more frequent today because of increased numbers of passengers, especially older people with chronic diseases traveling. The frequency of reporting significant IMEs is 1:10,000–40,000.
The US House of Representatives introduced legislation in 201515 “to require airlines to update their emergency kits to better protect kids in-flight”. The issue centered on the lack of emergency epinephrine treatment by pen injection for an acute and severe allergic reaction in flight. This medication has not yet been universally implemented. The lack of research information about pediatric care in flight is apparent. Some families may prepare for a journey, but specific items such as an epinephrine pen will have to accompany them in checked baggage as such items are not permissible in carry-ons. Other common pediatric conditions that could arise include febrile convulsions, epileptic seizures, acute asthmatic attacks, and an acute epistaxis. The danger of airway obstruction and inhaling a foreign body such as part of a toy, a piece of Lego, a lump of ice or bolus of food, or a free-floating plastic object are additional IME hazards. Physical assessment rather than an EMK item, except for nasal balloons or nasal tampons for protracted nosebleeds, is required. Nasal gauze packing should not be performed by an untrained person.
Current considerations
With the current trend of more nonstop, long-distance intercontinental flights, pediatric and elderly passengers are more likely to experience a more extensive IME. In 2016, Badawy et al16 implied that neonatal patients may be more vulnerable to an IME and that kits remained non-customized for such passengers. Mattison and Zeidel17 commented on the inadequacies of EMKs over 13 years earlier in 2004, considering the type of an IME and the rationale for a more complete kit to avoid possible flight diversion or emergency landings. The consequences are self-evident with considerable additional costs to the airline and logistic issues of aircraft and passenger displacement. Prioritization of ethical health care should be foremost. An unscheduled landing of an international flight could incur fees between US $70,000 and $230,000, not to mention the airlines’ logistic problems and ongoing passenger travel. It would take an average time of between 30 and 45 minutes for a commercial airliner to land from the time of a severe IME such as a cardiac arrest.18
Trained cabin crew might well enhance medical management and improve outcomes of passenger incidents, if not achieving full resolution. Support and primary care may be all that is required, without any need for equipment or medication. Declaration of being an active practicing physician by a boarding passenger should also be considered commendable. Not all physicians may feel adequately prepared or possess certified proof of status. Medical assistance is still not precluded in dire emergencies, manifested by onboard overhead announcements. The longstanding “Good Samaritan” law provided legal protection to all volunteer medical assistance on the ground before 1988. After that, the Aviation Medical Assistant Act, passed by the US Congress, extended further reassurance to passenger medical professionals in flight.19
Stethoscopes are effectively useless due to background noise, as are hand-operated sphygmomanometers. Automated blood pressure machines are preferable, but with onboard pressurized conditions, they only provide a guide. After 2009, a small number of airlines equipped their aircraft with the Tempus IC,20 a state-of-the-art telemedicine monitor that can transmit information, including video, to a ground-based medical center. The storage of drugs in an onboard EMK may be an issue according to specific country regulations. While the IATA recommends a “major analgesic” implying the use of an opiate, such a class of medicines is not routinely included as part of an onboard EMK at this time.
Pre-boarding alcohol intake and subsequent additional onboard consumption can lead to behavioral and medical issues. Most airlines can discreetly observe fitness to board at several stages before and at the aircraft door and may decline embarkation. Once on board, the only pre-emptive action is to deny any further alcohol supply. Alcohol excess can also precipitate epilepsy. A complete smoking ban on all flights can lead to nicotine withdrawal symptoms. The safety video or demonstrations articulate the nonsmoking rule. Abrogation of the policy is emphasized as punishable by law. Confined spaces and prolonged flights for regular alcohol imbibers and smokers can invoke air rage in rare circumstances. Narcotic drug abuse before or during flight justifies the carriage of naloxone injection. Airlines may have previous records of disruptive behavior on flights and have the right to deny boarding.
Certain medical or physiological conditions are particularly important for any air travel, especially for long-distance flights, and should be declared to the transporting airline at the time of booking.14,21,22 There is no routine health questionnaire or declaration used by any airline at this time. Costs and altered itineraries for diverted flights are considerable with extra landing fees liable to receiving countries. Health and travel liability insurance may be required for emergency care on the ground, or for any delay or contraindication in taking an original flight. They include the following:
- Recent post-intracranial or abdominal surgery within 14 days
- Recent chest or pulmonary surgery within 14 days
- Pneumothorax 21 days before flight; 7–14 days allowed with medical escort
- Any ear, nose, and throat procedure within the preceding 14 days
- Cerebrovascular accident within the preceding 10 days
- Acute psychotic mental illness
- Gestation >36 weeks (<4 hours in flight); 32 weeks with twins
- Post-delivery within the previous 7 days
- Neonates under 1 week of age
- Myocardial infarction within the previous 10 days
- Unstable angina
- Cardiac surgery within the previous 14 days (coronary artery bypass grafting)
- Uncontrolled daytime epilepsy
- Acutely infectious or communicable disease
- Decompression syndrome 3–7 days before flight
There is an assumption that all travelers will be responsible and reveal any pertinent, active medical issues. The declaration of pre-existing conditions is not a regular requirement before flight ticket purchase. Airlines concentrate more on the bioprofile and passport details rather than conducting any inquiry into chronic ailments or disability. Some elderly passengers may declare a condition that necessitates a wheelchair or buggy cart help to reach an aircraft, but chronic diseases affecting the cardiovascular, pulmonary, or metabolic systems are rarely apparent.
One earlier estimate of chronic diseases in passengers showed 5%.23 This figure is quite likely an underestimate for 2017 and can be predicted to rise further as more aging people travel globally. Most minor disorders are undeclared. Post-surgical conditions are also frequently unreported, only becoming known with specific requests for better seating accommodation.
Some airlines provide health documentation forms. Sand et al24 analyzed 10 airlines willing to participate and found a total of 199 different items to complete. When asked in 2009 for IME data, only 4 out of 32 European airlines could produce fully documented data. The IATA recommends an accurate recording of an IME.25 The International Civil Aviation Organization states that an incident record form is an essential part of an EMK.26
Conclusion
Commercial airlines primarily intend to transport healthy individuals. Onboard, it is neither possible nor desirable to replicate a diagnostic or therapeutic environment comparable to an Emergency Room setting. EMKs should be customized for adults, children, and infants and undergo periodic content review. Oxygen saturation readings in flight are useful for compromised pulmonary conditions. A pulse oximetry device, an AED, and autoinjectable epinephrine should be included in all international commercial airline flights.
A multilingual set of instructions should be included with an onboard EMK. The authors have suggested English, French, and Spanish as being useful, and Mandarin, Hindi, and Arabic could be added according to global journeys.
Onboard medical professionals who volunteer assistance and are unlikely to have aviation medicine training should not fear retribution. However, the ethical principle of “Primum Non Nocere – First, do no harm”27 must be borne in mind by any physician at all times.
Disclosure
The authors report no conflicts of interest in this work which received no funding.
References
IATA Medical Manual. AsMA Guidance Document, Medical Emergencies: Managing In-Flight Medical Events 2017; July 2016 edition. | ||
International Air Transport Association (IATA). International Air Transport Association Medical Manual. 1st ed. Montreal, QC: International Air Transport Association; 2004. | ||
Aerospace Medical Association (AsMA) Medical Guidelines Task Force. Medical guidelines for airline travel, 2nd edition. Aviat Space Environ Med. 2003;74(5):A1–A19. | ||
Aerospace Medical Association (AsMA), Managing In-Flight Medical Events, 2018. Available from: https://www.asma.org/publications/medical-publications-for-airline-travel/managing-in-flight-medical-events. Accessed January 20, 2018. | ||
Aerospace Medical Association (AsMA), Medical Guidelines for Airline Travel, 2018. Available from: https://www.asma.org/publications/medical-publications-for-airline-travel/medical-considerations-for-airline-travel. Accessed January 20, 2018. | ||
International Academy of Aviation and Space Medicine, 2009. Definition. Available from: https://www.iaasm.org/aboutus.cfm. Accessed January 20, 2018. | ||
American Osteopathic Association, 2018. Summer travel: are you ready to answer the call for a doctor on the plane? Available from: https://thedo.osteopathic.org/2017/07/summer-travel-ready-answer-call-doctor-plane/. Accessed January 18, 2018. | ||
American College of Emergency Physicians, 2018, Be Prepared for In-Flight Medical Emergencies. Available from: https://www.acep.org/Clinical-Practice-Management/Be-Prepared-for-In-Flight-Medical-Emergencies/#sm.00000nk3h27f2rem8ti0p7382c1ab. Accessed January 18, 2018. | ||
American Medical Association, Criteria for CPT® Category I and Category III Codes, 2018. Available from: https://www.ama-assn.org/practice-management/criteria-cpt-category-i-and-category-iii-codes. Accessed January 18, 2018. | ||
Resuscitation Council (UK), Automated External Defibrillators on Aircraft, 2018. Available from: https://www.resus.org.uk/media/statements/automated-external-defibrillators-on-aircraft/. Accessed January 19, 2018. | ||
Silverman D, Gendreau M. Medical issues associated with commercial flights. Lancet. 2009;373(9680):2067–2077. | ||
Toff WD, Jones CI, Ford I, et al. Effect of hypobaric hypoxia, simulating conditions during long-haul air travel, on coagulation, fibrinolysis, platelet function, and endothelial activation. JAMA. 2006;295(19):2251–2261. | ||
Kesapli M, Akyol C, Gungor F, Akyol AJ, Guven DS, Kaya G. Inflight emergencies during eurasian flights. J Travel Med. 2015;22(6):361–367. | ||
Ahmedzai S, Balfour-Lynn IM, Bewick T, et al. British thoracic society standards of care committee. Thorax. 2011;66(Supp 1):i1–i30. | ||
Wheeler L. House bill would mandate emergency supplies for kids on planes. 2015. Available from: http://thehill.com/regulation/healthcare/249602-house-bill-would-update-emergency-medical-kits-on-airplanes. Accessed December 29, 2017. | ||
Badawy SM, Thompson AA, Sand M. In-flight emergencies: medical kits are not good enough for kids. J Paediatr Child Health. 2016; 52(4):363–365. | ||
Mattison ML, Zeidel M. Navigating the challenges of in-flight emergencies. JAMA. 2011;305(19):2003–2004. | ||
Gounder C. Medical emergencies at 40,000 feet. 2013. Available from: https://www.theatlantic.com/health/archive/2013/04/medical-emergencies-at-40-000-feet/274623/. Accessed December 29, 2017. | ||
House of Representatives 105th Congress, 2nd session. Report 105–456. Aviation Medical Assistance Act, 1988. | ||
Tempus IC User/Operator Manual 2009. Available from: https://fccid.io/ROSTEMPUSIC-1/User-Manual/User-manual-1250092. Accessed October 20, 2017. | ||
Zahger D, Leibowitz D, Tabb IK, Weiss AT. Long-distance air travel soon after an acute coronary syndrome: a prospective evaluation of a triage protocol. Am Heart J. 2000;140(2):241–242. | ||
Roby H, Lee A, Hopkins A. Safety of air travel following acute myocardial infarction. Aviat Space Environ Med. 2002;73 (2):91–96. | ||
Rodenberg H. Medical emergencies aboard commercial aircraft. Ann Emerg Med. 1987;16(12):1373–1377. | ||
Sand M, Morrosch S, Sand D, Altmeyer P, Bechara FG. Medical emergencies on board commercial airlines: is documentation as expected? Crit Care. 2012;16(2):R42. | ||
International Air Transport Association (IATA), Montreal-Geneva: Medical Manual; 2004;3:66–67, Appendix D. | ||
International Civil Aviation Organization. Annex 6, Operation of Aircraft Part I, International Commercial Air Transport, Aeroplanes, Chapter 6 Aeroplane Instruments, Equipment and Flight Documents Attachment B. 8th ed. First Aid Medical Supplies. 2001:4. | ||
Smith CM. Origin and uses of primum non nocere – above all, do no harm! J Clin Pharmacol. 2005;45(4):371–377. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.