Back to Archived Journals » Open Access Surgery » Volume 10
Magnitude and patterns of injuries among patients in Gondar University Hospital, northwest Ethiopia: an institutional-based study
Authors Ayele TA, Zeleke BM, Tessema GA, Melak MF
Received 29 October 2016
Accepted for publication 16 February 2017
Published 5 April 2017 Volume 2017:10 Pages 25—31
DOI https://doi.org/10.2147/OAS.S126043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Tadesse Awoke Ayele,1 Berihun Megabiaw Zeleke,1 Gizachew Assefa Tessema,2 Melkitu Fentie Melak3
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health sciences, University of Gondar, Gondar, Ethiopia; 2Department of Reproductive Health, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Human Nutrition, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: The World Health Organization (WHO) estimates that injuries constitute 16% of the global burden of disease. This translates into 5.8 million injury-related deaths annually, worldwide. The aim of this study was to determine the magnitude and pattern of injury in the Gondar University Hospital (GUH) in the year 2013.
Methods: A retrospective study was conducted in GUH from March to April 2013. All charts of injured patients who visited the hospital from January 1 to December 30, 2012 were included in this study. A total of 616 patients’ charts were included in this study. Data were entered and cleaned using Epi Info and exported to Stata version 11 for analysis. Binary logistic regression was used, and odds ratios with 95% confidence interval were reported.
Results: During the study period, a total of 84,254 patients visited the hospital, of whom 16,611 (19.7%) were surgical cases. Injury accounted for 25% of surgical emergency cases. Patients were predominantly young males (82%). Three in five (59.4%) of the injured patients were within the age range of 15–30 years. Approximately one in three, 187 (32.2%), and one in four, 141 (24.3%), of those injured patients were students and farmers, respectively. The injury mechanism for nearly half (48.9%) of students was assault, followed by 45.2% of road traffic accidents. Intentional injuries occurred among 291 (47.24%) cases, of whom 84.5% were males. Fracture (22.9%) and head injury (17.2%) were the leading outcomes of injuries. Severe injuries accounted for ~13% of all cases. Residence, physical nature of injury and place of work were found to be significantly associated with the outcome of injury.
Conclusion and recommendation: The magnitude of injury in this hospital was found to be high when compared with other similar settings. Assault and road traffic accidents were the two common mechanisms of injury. Appropriate prevention strategies should be designed and implemented against assault and road traffic accidents.
Keywords: road traffic accident, surgical department, University Hospital, Ethiopia
Introduction
The World Health Organization (WHO) estimates that injuries constitute 16% of the global burden of disease. This translates into 5.8 million injury-related deaths at a rate of 97.9/100,000 worldwide.1,2 Injury has been defined as damage to the body caused by an exchange with environmental energy that is beyond the body’s resilience.3 Whatever the conceptual ambiguities may be, violence and injuries are among the leading health challenges of our times. They are a major threat to health in every country in the world and are responsible for >5 million deaths and millions of injuries annually. A total of 8 of the 15 leading causes of death for people aged 15–29 years are violence or injury related.4 Injury is the leading cause of death for children aged 1–19 years in Canada.5 The WHO reported that, on a daily basis, >2000 children die worldwide from unintentional injuries and at least half of these deaths are preventable if appropriate prevention measures are used.6
Injury is one of the commonest causes of death and disability in the African region, particularly among those aged 5–29 years. Three of the top five causes of death for this age group are injury related.7 Every day in Africa, ~2,400 people die from injuries. Injury-related deaths in Africa among people aged 15–44 years rank second after HIV/AIDS. For every person who dies of injuries aged >35 years, others suffer from nonfatal injuries.8
The number of people injured in road traffic crashes was as high as 50 million worldwide. The number of people killed each year was estimated to be almost 1.2 million. The tragedy behind these figures regularly attracts less media attention than others, less frequent but more unusual types of tragedy.9 In Ethiopia, traffic accident resulted in ~2.3 deaths/100,000 population, which can be taken as a mid value as compared to other countries (Rwanda, Senegal, Uganda, Namibia, Swaziland, South Africa, Morocco, Tunisia). The death rate per 10,000 vehicles, however, is the second highest in the world (134.3/10,000 vehicles).10 A cross-sectional survey conducted in Northern Ethiopia found the prevalence of burn injury to be 1.2%, of which children <5 years accounted for the highest incidence of 4.8%.11 A retrospective study conducted in Addis Ababa showed of all emergency cases, injury accounts for 27%.12
Injuries are major health problems that commonly appear on the morbidity and mortality reports of the health institutions in Ethiopia. Despite this prevailing phenomenon, limited attention has been given to injuries as health problems. Therefore, the present study attempted to contribute to determining the magnitude and pattern of injury among patients who visited Gondar University Hospital (GUH), Gondar, northwest Ethiopia.
Methods
Study design and period
A retrospective study was conducted in GUH from March to April 2013. All charts of injured patients who visited the hospital from January 1 to December 30, 2012 were included in the study.
Study area and setting
This study was conducted in GUH. The hospital provides health care to ~5 million people coming from Amhara National Regional State and partly from neighboring regions. It has ~700 beds in different wards. About 320 patients daily visit the hospital, of whom 10 visit due to injury.
Source and study population
The source population of this study was individuals who had been injured with all kinds of injury during the past 1 year. The study population was all injured individuals who visited the hospital during the study period.
Inclusion criteria
Injured patients’ charts with complete clinical information, which can address where, when, by what and how the injury happened, were included (Figure 1).
 | Figure 1 Flowchart for the sampling procedure. |
Sampling technique and sample size
There were a total of 734 injury cases from January 1 to December 30, 2012, of which 616 cases satisfied all the inclusion criteria and were included in this study.
Variables of the study
The following were the variables for this study:
- Outcome variable: degree of injury
- Independent variables: age, sex, marital status, religion, occupation, residence, intent, physical nature of injury, object that causes injury, place, activity, mechanism, disability, and action taken.
Operational definitions
The degree of injury is defined as superficial injuries such as bruises and lacerations as minor injury; injuries beyond subcutaneous tissue but not including visceral organs, which require some skilled treatment as moderate injury and injuries affecting visceral organs, which required intensive surgical and/or medical treatment as severe injury. Major injuries include both moderate and severe injuries.
Data collection instrument
A pretested and structured checklist was used to retrieve the data from hospital records. The checklist was adapted from the WHO standard questionnaire for institute-based injury survey.13 Data were collected from the patients’ charts about injury and possible factors. Data on basic sociodemographics and types of injury were collected from each individual’s chart. Data collectors were three nurses who were working at the surgical ward: 1 day training was given to them on the content of the checklist. The data extraction checklist was pretested on 20 patients’ charts, and modifications were made accordingly. The supervisor rechecked the checklist daily and submitted to the principal investigator to maintain data quality.
Data analysis procedure
Data were entered and cleaned using Epi Info 2002 and exported to Stata version 11 statistical package for further analysis. Then, descriptive statistics were used to summarize the data and graphs, and statistical summary measures were used for presentation. After getting the overview about the data, simple binary logistic regression was fitted for each explanatory variable, and those variables with a p-value of <0.2 were fitted in multiple logistic regressions to get odds ratio with 95% confidence interval (CI) to identify associated factors with injury outcomes. A p-value of <0.05 was considered as a cutoff value for statistical significant association.
Ethical considerations
A human subject research approval for this study was received from the institutional review board (IRB) of the University of Gondar. As the study was retrospective, the IRB waived that the research could be done based on record review without contacting the patients. A support letter was obtained from the medical director office of the hospital for retrieving retrospective data from the database and records. All the information was kept confidential, and no individual identifiers were collected.
Results
A total of 84,254 patients visited GUH during the 12-month period, from January 1 to December 30, 2012, of whom 16,611 (19.7%) were surgical cases. Of the total surgical cases, 2934 (17.7%) were surgical emergency cases, of which 734 (25.0%) were injury cases. A total of 616 patients had complete information and were included in this study. Of the 616 injured patients, a high proportion of males, 502 (81.5%), were injured, with a male to female ratio of 5:1. Three in five (59.35%) of the injured patients were within the age range of 15–30 years. The average age was found to be 29 years (±14.4 SD). Nearly half of those who were injured were single in their status. With regard to residence, almost an equal proportion were injured in the study period. In relation to occupation, 187 (32.24%) and 141 (24.31%) of those injured were students and farmers, respectively. Most of the injury cases were orthodox, 567 (95.1%), in religion and Amhara, 562 (93.98%), in ethnicity. From the total 465 cases who had information about the time of injury, 288 (60.22%) had occurred during ante meridiem. Of the total cases, 25 (4.06%) were occupational injuries (Table 1).
 | Table 1 Sociodemographic characteristics of injured patients who visited GUH from January to December 2012 Abbreviation: GUH, Gondar University Hospital. |
The three leading outcomes of injury were bruise or superficial, 215 (34.9%); fracture, 141 (22.9%); and head injury, 106 (17.2%). Nearly one in three of the head injuries (34.65%) were among students, while 37 (26.8%) farmers had fracture as a result of injury.
This finding revealed that the common mechanism of injury was blunt assault, 316 (51.3%), followed by road traffic accidents, 334 (30.3%). The injury mechanism for nearly half (48.9%) of students was assault, followed by 45.2% of road traffic accidents.
Intentional injuries occurred among 291 (47.24%) cases, of whom 246 were males and only 46 were females. With regard to occupation, most students, 104 (55.9%), were injured unintentionally, while a high number of farmers, 89 (64.5%), were injured intentionally. With regard to place of injury, two in three, 405 (65.75%) and 134 (21.75%), injuries took place on the street and around home, respectively. Approximately three-fourth of the injuries that happened on the street, 132 (35.8%) and 84 (22.8%), were among students and farmers, respectively. When the injury had happened, 342 (55.52%) people were traveling, 135 (21.92%) were playing, and 75 (12.18%) were working. Of the 245 traffic injuries, nearly half, 114 (47.3%), were passengers, 89 (36.93%) were pedestrians, and 20 (8.3%) were drivers (Table 2).
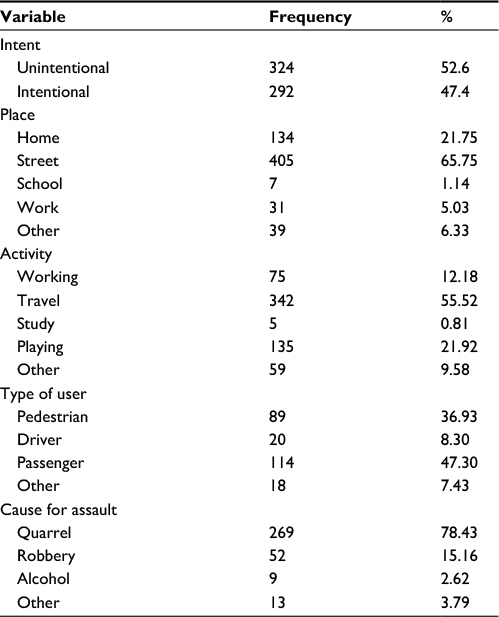 | Table 2 Profile of injury among patients who visited GUH from January to December 2012 Abbreviation: GUH, Gondar University Hospital. |
Of 343 injuries that happened due to assault, almost four in five, 269 (78.43%), were because of quarrel and 52 (15.16%) were due to robbery. A total of 105 (33.2%) people used stick during the assault (Figure 2).
 | Figure 2 Types of objects used to execute injury among injured patients who visited GUH from January to December 2012. Abbreviation: GUH, Gondar University Hospital. |
The degree of injury had characterized according to the severity. Almost half, 322 (52.27%), of the injuries were moderate, 179 (29.06%) injuries were minor, and 80 (12.99%) of the patients were severely injured. Of the 316 patients injured due to assault, 154 (48.7%) and 44 (13.9%) had moderate and severe injuries, respectively. Of all severe cases, 55% and 30% were due to assault and traffic accidents, respectively. Nearly two out of three (68.02%) injured patients had been treated, and 182 (29.55%) were admitted and treated in the hospital. Of all injured patients, 13 (2.11%) were reported to die because of injury. With regard to disability, 78 (12.66%) people experienced disability. Of the total who had information about the status of disability, 27 (42.2%) people walked with a limp and 8 (12.5%) were unable to walk at all (Table 3).
 | Table 3 Clinical information of injury among injured patients who visited GUH surgical ward from January to December 2012 Abbreviation: GUH, Gondar University Hospital. |
It seems that there is a difference in the number of injuries during months of the year. As can be seen from Figure 3, the total number of injuries was high in January, February, March, and April. The number of injuries reached high during January and March (Figure 3).
 | Figure 3 Months of the year when the injury happened among injured patients who visited GUH from January to December 2012. Abbreviation: GUH, Gondar University Hospital. |
Bivariable logistic regression was fitted to identify the possible factors to be used for multiple logistic regressions. Sex, residence, intent, age group, physical nature of injury, place, and occupation were the variables that had p-value <0.2 and were considered for multiple logistic regression. Being from rural area disregarding the kinds of injury had a risk of approximately twofold (adjusted odds ratio [AOR]=2.11, 95% CI=[1.37, 3.25]) for moderate or severe injury than their counterparts. With regard to the physical nature of injury, those with open wound and head injury were 91% and 70% (AOR=0.09, 95% CI=[0.05, 0.16]; AOR=0.30, 95% CI=[0.15, 0.61]) less likely to have moderate or severe injury, respectively, compared with those having fracture. The place where the patients got injured was also another associated factor of the degree of injury. Those who were injured at home and on the street were approximately two times (AOR=2.31, 95% CI=[1.18, 4.55]; AOR=2.19, 95% CI=[1.22, 3.92]) more likely to have moderate or severe injury than those injured at school or work (Table 4).
 | Table 4 Factors associated with the degree of injury among injured patients in GUH from January 1 to December 30, 2012 Notes: *Other includes: burn, dislocation, bits, open wound or bruise. **Other includes: house wife, merchant or daily laborer. Bold values refer to statistically significant confidence intervals. Abbreviations: GUH, Gondar University Hospital; COR, crude odds ratio; CI, confidence interval; AOR, adjusted odds ratio. |
Discussion
This study showed that surgical admissions contributed to 19.7% of all total admissions at GUH. It was lower than the study conducted at the Tikur Anbessa Hospital in Addis Ababa (34.6%).14 This might be due to the difference in the study area. As Tikur Anbessa Hospital is the hospital at the capital city of the country, it serves largely urban population in whom surgical cases may be higher. The study also revealed that the magnitude of injury was 5.4%. This finding is similar to the study done in the North Gondar zone15 but smaller than the study conducted in the Jimma University Hospital (8.2%).2 This difference might be attributed to the difference in the accessibility of other health facilities in the current study area than in the previous study area. A high proportion of males, 513 (82%), were injured than females with a male to female ratio of 5:1, which was similar to other studies.16,17 This might be due to a high exposure of males due to their sex role to outdoor activities than females. Of all injured patients, students took the highest proportion, followed by farmers. This finding is similar to the study conducted in the Viet Duc Hospital, Vietnam.18 This could be explained as students are exposed with different causes of injury due to their age and activity. With regard to intent, intentional injury accounted for approximately half of the cases in this study. This is similar to the study done in the Jimma University Hospital2 but very high compared with a community-based study conducted in the Jimma zone.19 The discrepancy may be due to the difference in the study area. The current study is hospital based, which may include more intentional cases due to the need of witness for judiciary issue. A high proportion of students were injured unintentionally; however, intentional injury was high among farmers than other occupations. The occurrence of injury was higher during January–April in the given year. It reached the peak in the months of January and March. This is because this period is the harvesting period for farmers in which most people moved from home to field and market places and vice versa to sell their products. This movement may give them an opportunity for drinking and expose them to car accidents and assault. In addition, as most public holidays are celebrated during these months, people move from place to place, which might again expose them to different accidents.
The leading causes of injury were assault and road traffic accidents. Of the total people with traffic injuries, nearly half were passengers, three in eight were pedestrians and ~8% were drivers. This finding was similar to the study done in the North Gondar zone15 and the Jimma University Hospital.2 Two of three injuries occurred on the street, followed by one of five around home, which is consistent with a study carried out in Jimma2 and Vietnam.18 Approximately three-fourth of the injuries that happened on the street, 35.8% and 22.8% were among students and farmers, respectively.
In this study, occupational injury accounted for 4.06%, which is smaller than a study conducted in the Gondar town (38.7%)20 and Addis Ababa city (43.7%).21 This difference might be explained by the difference in the study area. This study was conducted at a tertiary hospital in which almost all cases were referral occupational injuries that required hospital admission, which made the magnitude smaller; however, the earlier studies were community-based studies that included all types of occupational injuries. With regard to the degree of injury, almost half and 13% of the patients had moderate and severe injury, respectively. Of all severe cases, 55% and 30% were due to assault and traffic accidents, respectively. A study conducted in the Jimma University Hospital put road traffic accident for almost half of the severe injuries, 179 (49.7%), followed by stab injury, 45 (12.5%).2 Unlike a study conducted in the Jimma University Hospital, this study indicated that 78 (12.66%) of injured patients had experienced disability. Of the total where information about the status of disability was available, 8 (12.5%) were unable to walk at all. This might be due to differences in the extent of injury and the quality of the care given, which determined the treatment outcome and the final fate of a patient.
Of all injured patients, 13 (2.11%) were reported dead. This finding was lower than that reported in the study conducted in Addis Ababa.12 This could be defined by the difference in the study area and degree of injury. This study showed injury-related deaths that occurred at a hospital level only, but the study that was conducted in Addis Ababa was a community-based study that assessed all injury-related deaths that occurred other than in hospitals. Differences in degree of injury might also affect the death rate. As this is a hospital-based study, the data we used were secondary data. This could be considered as the main limitation of this study.
Conclusion
The magnitude of injury in this hospital was found to be high, and mostly males and people within the age range of 15–30 years were affected. Blunt assault and road traffic accidents were the two common mechanisms of injury. The leading outcomes were bruise, fracture, and head injury. Most students were injured unintentionally, while farmers were injured intentionally. Injury cases reached high during January and March. It is better to design and implement appropriate prevention strategies against assault and road traffic accidents. Finally, we recommend a more representative community-based study.
Disclosure
The authors report no conflicts of interest in this work.
References
WHO. World Report on Violence and Health. Geneva: World Health Organization; 2002. | ||
Woldemichael K, Berhanu N. Magnitude and pattern of injury in Jimma University Specialized Hospital, South West Ethiopia. Ethiop J Health Sci. 2011;21(3):155–165. | ||
Holder Y, Peden M, Krug E, et al. Injury Surveillance Guidelines. Geneva: World Health Organization; 2001. | ||
Brunicardi F, Andersen D, Billiar T, Dunn D, Hunter J, Matthews J. Schwartz’s Principles of Surgery. New York: McGraw-Hill; 2005:129–188. | ||
WHO. Violence, Injuries and Disability 2006-2007. Geneva: World Health Organization; 2008. | ||
Public Health Agency of Canada. Leading Causes of Death and Hospitalization in Canada. Toronto, Canada; 2015. | ||
Peden M, Oyegbite K, Ozanne-Smith J, et al. World Report on Child Injury Prevention. Geneva: World Health Organization; 2008. | ||
Peden M, Scurfield R, Sleet D, et al. World Report on Road Traffic Injury Prevention. Geneva: World health organization; 2004. | ||
WHO. The African Regional Health Report: The Health of the People. Geneva: World Health Organization; 2006. | ||
Berhane Y, Mariam DH, Kloos H. Epidemiology and Ecology of Health and Disease in Ethiopia. Addis Ababa: USAID; 2006. | ||
Lagarde E. Road traffic injury is an escalating burden in Africa and deserves proportionate research efforts. PLoS Med. 2007;4(6):e170. | ||
Nega KE, Lindtjørn B. Epidemiology of burn injuries in Mekele town, Northern Ethiopia: a community based study. Ethiop J Health Dev. 2002;16(1):1–7. | ||
Adem A, Abebe A, Abdurahman M. Pattern of Surgical Admissions to Tikur Anbessa Hospital, Addis Ababa, Ethiopia. East Cent Afr J Surg. 2001;6(1). | ||
Osman M, Kebede Y, Anberbir S. Magnitude and pattern of injuries in North Gondar Administrative Zone, Northwest Ethiopia. Ethiop Med J. 2003;41(3):213–220. | ||
Ray K, Bhattacherjee S, Akbar F, Biswas R, Banerjee R, Chakraborty M. Physical injury: a profile among the municipal primary school children of Siliguri, Darjeeling District. Indian J Public Health. 2012;56(1):49–52. | ||
Kyungsu K, Dejan O, Donald CV. Differences in incidence of injury between rural and urban children in Canada and the USA: a systematic review. Inj Prev. 2012;18(4):264–271. | ||
Nguyen D, Cao D, Nguyen DH. Preliminary results of injury surveillance at Viet Duc hospital. Thai J Surg. 2007;28:83–89. | ||
Woldemichael K, Tessema F, Sena L. Community based survey of injury in Jimma Zone, Southwest Ethiopia. Ethiop J Health Sci. 2008;17(4):179–188. | ||
Adane MM, Gelaye KA, Beyera GK, Sharma HR, Yalew WW. Occupational injuries among building construction workers in Gondar City, Ethiopia. Occup Med Health Aff. 2013;1:125. | ||
Bogale D, kumie A, Tefera W. Assessment of occupational injuries among Addis Ababa city municipal solid waste collectors: a cross-sectional study. BMC Public Health. 2014;14:169. | ||
Wolde A, Abdella K, Ahmed E, et al. Pattern of injuries in Addis Ababa, Ethiopia: a one-year descriptive study. East Cent Afr J Surg. 2008;13:14–22. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.