Back to Journals » Clinical Ophthalmology » Volume 15
Maculopathy Secondary to Pentosan Polysulfate Use: A Single-Center Experience
Authors Kalbag NS, Maganti N, Lyon AT, Mirza RG ![]()
Received 5 October 2020
Accepted for publication 13 January 2021
Published 11 February 2021 Volume 2021:15 Pages 513—519
DOI https://doi.org/10.2147/OPTH.S285013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Neil S Kalbag, Nenita Maganti, Alice T Lyon, Rukhsana G Mirza
Department of Ophthalmology, Northwestern University, Chicago, IL, USA
Correspondence: Rukhsana G Mirza
Department of Ophthalmology, Northwestern University, Chicago, IL, USA
Email [email protected]
Aim: To investigate the prevalence of retinal pathology in patients with a history of exposure to pentosan polysulfate sodium (PPS).
Methods: Patients exposed to PPS and seen in the ophthalmology clinic at Northwestern University during 1/1/2002 to 1/1/2019 were identified from electronic health records (EHR) by an electronic data warehouse (EDW) search. Visual acuity (VA), reasons for clinic visit, ocular conditions, and duration of exposure to PPS were noted. Chart review was performed for fundus exam findings and ophthalmologic imaging, specifically fundus photography, fundus autofluorescence, and ocular coherence tomography (OCT) images. When OCT or fundus photography was available, studies were evaluated by two independent graders.
Results: A total of 131 patients who were exposed to PPS and seen at the Northwestern Ophthalmology clinic were identified in the EHR. Forty patients of 131 had imaging. Patients with imaging or fundus examination suspicious for PPS maculopathy were placed into the suspect group. Of the 40 patients that had imaging, 5 (12.5%) had features suspicious for PPS maculopathy. Of the remaining 91, 5 (5.4%) had macular pigmentary changes described on fundus exam. Among the 10 patients in the suspect group, the average duration of PPS use was 4.2 years (range 0.3– 11.6 years, interquartile range 5.5 years) and the average cumulative dose was 380g (range 29– 1092g, interquartile range 132g).
Conclusion: A novel drug-induced maculopathy has been associated with PPS use with a distinct clinical constellation that can be accurately identified with multimodal imaging.
Keywords: interstitial cystitis, IC, maculopathy, pentosan polysulfate sodium, PPS
Introduction
Interstitial cystitis (IC) or bladder pain syndrome is a chronic condition that causes pain or pressure in the bladder, predominantly in women.1 The pathophysiology of this disease is still unknown. In the US, 2.7–6.5% of the population is affected by IC.1 Antihistamines, tricyclic antidepressants, cyclosporine, bacille Calmette-Guérin, nitric oxide, and pentosane polysulfate (PPS) have all been used to treat IC.2 PPS is a sulfated polysaccharide, with a structure similar to heparin and glycosaminoglycan and is the only United States Food and Drug Administration (FDA)-approved drug for IC, typically dosed at 100mg three times per day.3 It works as a mucosal protecting agent in the bladder to provide symptomatic relief by binding to the uroepithelium and reducing permeability to decrease irritation from toxins.3
Long-term studies on PPS report nausea, diarrhea, and headache as the common adverse effects.3 Pearce et al recently described a unique pigmentary maculopathy associated with chronic exposure to PPS in which toxic changes to the retina in 6 out of 38 patients studied at a single center were described.4 They noted changes in the retinal pigment epithelium including parafoveal pigmented deposits, paracentral atrophy, and hyperreflective lesions.4 Further studies have shown that key features of PPS-associated maculopathy include a hypoautofluorescent peripapillary halo on imaging and early involvement of the central macula.5 Prior to understanding the new maculopathy, several patients were diagnosed as having macular dystrophies and hereditary maculopathies.5 Prospective studies by Wang et al and Vora et al have reported the prevalence of PPS-associated maculopathy to be 20% and 23.1% respectively.6,7 Theorized mechanisms include the antagonism of the fibroblastic growth factor pathway in the retina by PPS, specifically in the retinal pigmental epithelium layer (RPE), PPS being directly toxic to the retina, or interaction between PPS and the glycosaminoglycans in the photoreceptor layer of the retina.8,9 Although PPS was approved by the FDA in 1996, it was only recently in June of 2020 that the FDA released an updated label to include retinal pigmentary changes as a warning and adverse effect of the drug.
This study reports retinal changes noted in patients on PPS, for any duration of the drug, at a tertiary-care center to add to the previously reported single-center case series. The current state of identification of this disease, steps to understand the association versus causation between PPS and pigmentary maculopathy, and changes to improve identification of this condition are also discussed.
Methods
A retrospective study was performed on patients from the Northwestern Medicine EPIC electronic health records (EHR) by using an Electronic Data Warehouse (EDW) search. The study cohort included patients aged 18–95 years who had been exposed to PPS and seen in the Northwestern ophthalmology clinic from January 1, 2002 to January 1, 2019. An EDW query was performed to obtain visual acuities, duration of drug, dose of drug, other health conditions, and demographics for patients in the study group. Patient charts were reviewed by study team members for fundus findings documented in the examination and ophthalmologic imaging, specifically multimodal imaging including fundus photography, fundus autofluorescence, and ocular coherence tomography (OCT) images. When imaging was available, the images were evaluated by at least two independent ophthalmologists. In cases where imaging was not available, patient charts were reviewed for fundus examinations with clinical documentation of macular pigmentary changes such as pigmentary clumping or mottling. Subjective complaints were not utilized to identify suspicious findings. Patients with fundus exam or imaging findings suspicious for PPS-associated maculopathy as described by Pearce et al were separated into the suspect group for further evaluation.
This study was approved by the Institutional Review Board of Northwestern University. All data accessed complied with relevant data protection and privacy regulations. Descriptive statistics were used to summarize patient demographics. Continuous measures were summarized with means and standard deviations (SD), and categorical measures were summarized with frequencies and percentages. SAS version 9.4 (SAS Institute, Cary, NC) was used for all statistical analyses.
Results
The study cohort comprised a total of 262 eyes of 131 patients. One hundred and eleven (84.7%) patients were female, and the cohort’s average age was 59.5 (±16.1) years old (range: 21–90). Demographic data are shown in Table 1. Of the 131 patients, 40 patients (30.5%) had imaging while 91 (69.5%) did not. Of the 40 patients with imaging on file, 5 (12.5%) had findings suspicious for PPS-associated maculopathy and of the 91 patients without imaging, 82 patients had documented fundus examinations and 5 (6.1%) of such patients were noted to have macular pigmentary changes. The 5 patients with imaging findings suspicious for PPS maculopathy and the other 5 patients with macular pigmentary changes were separated into a suspect group.
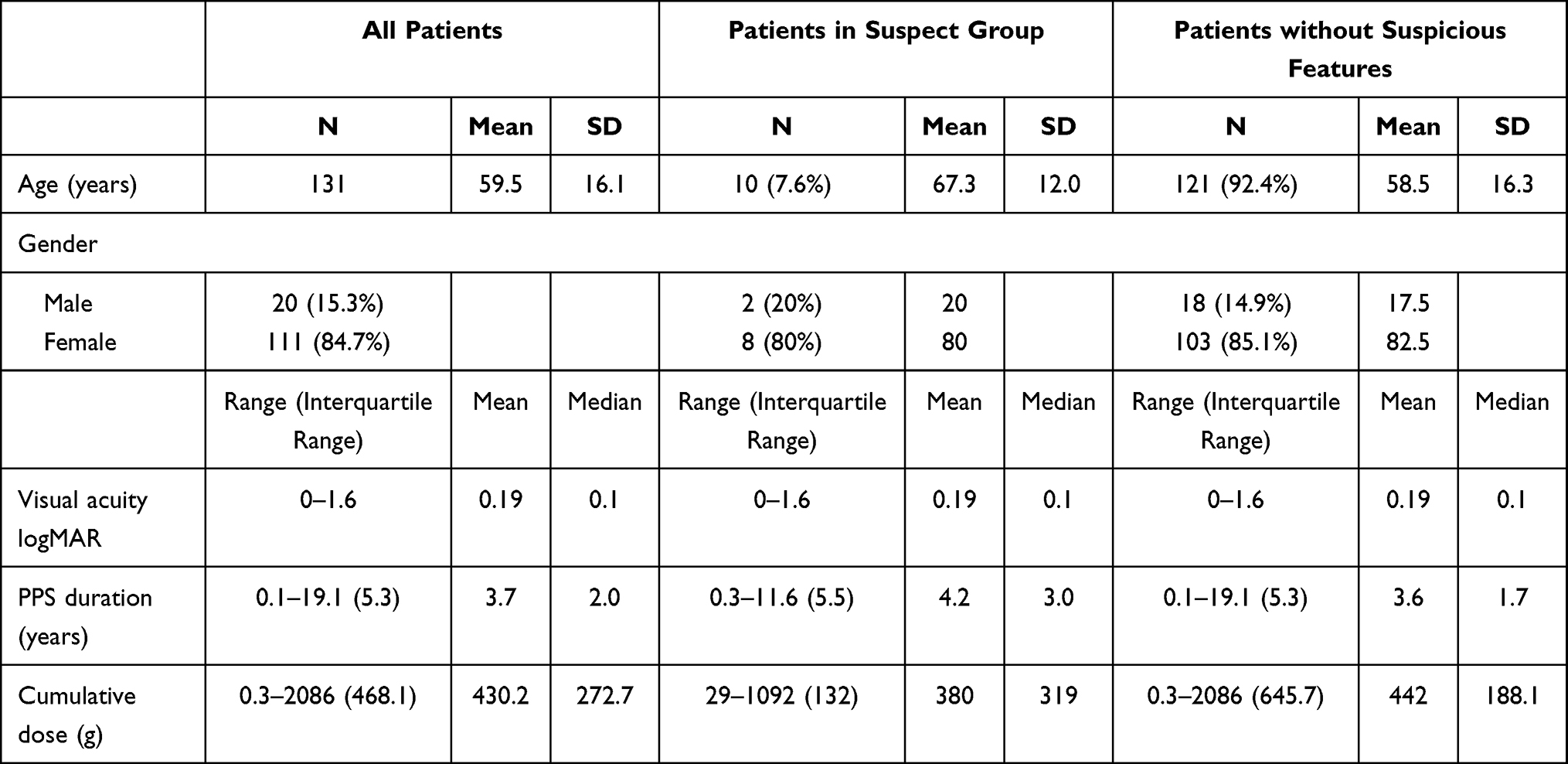 |
Table 1 Characteristics of Patients Taking Pentosan Polysulfate Sodium |
Individual examination and imaging findings for the suspect group and their classification based on degree of suspicion as described in a recent paper by Hanif et al are shown in Table 2.10 Patients 8 and 9 had the most striking findings including pigmentary changes around the fovea (Figures 1 and 2) with both hyper- and hypoautofluorescent pigmentary changes associated with vitelliform/hyperreflective lesions on OCT. Patient 8 had multiple studies over a 5 year period documenting progression of RPE atrophy in the late stage of the disease. (Figure 3).
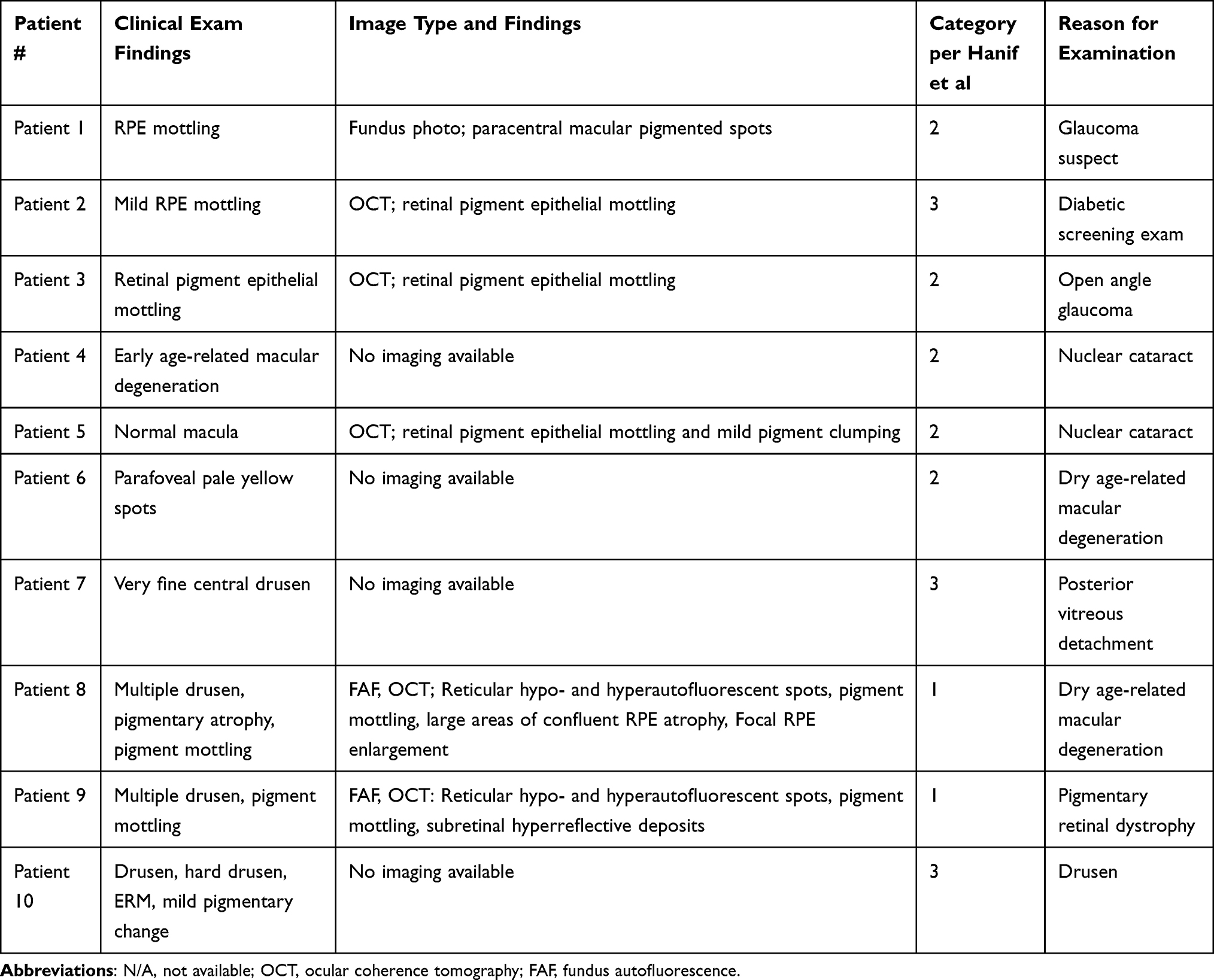 |
Table 2 Clinical Findings in Patients Suspicious for PPS-Associated Maculopathy |
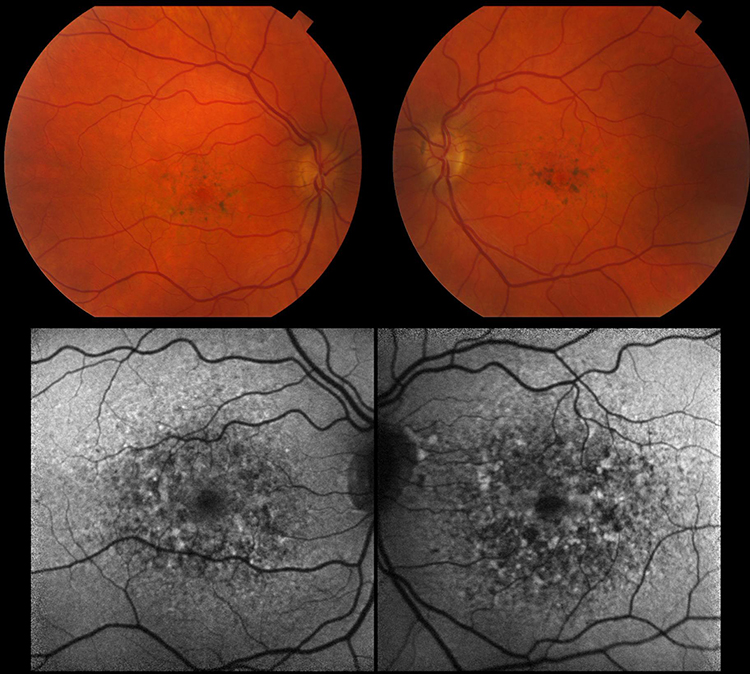 |
Figure 1 (Patient 9) Fundus photography: Fundus autofluorescence at early stage of disease showing pigment mottling, reticular hypoautofluorescent and hyperautofluorescent spots, and focal areas of RPE enlargement. |
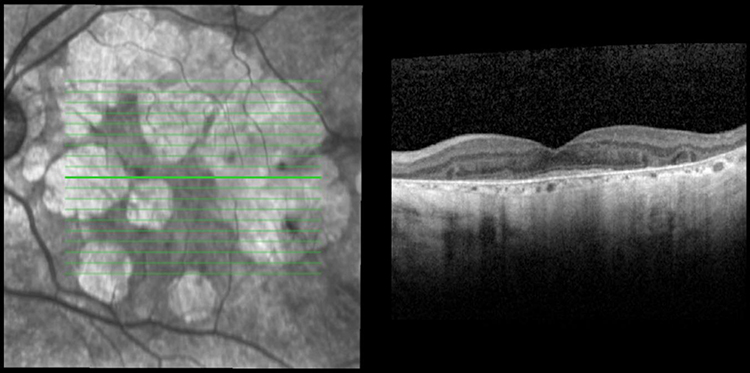 |
Figure 2 (Patient 8) OCT: Later stage of the disease shows large areas of confluent RPE atrophy. |
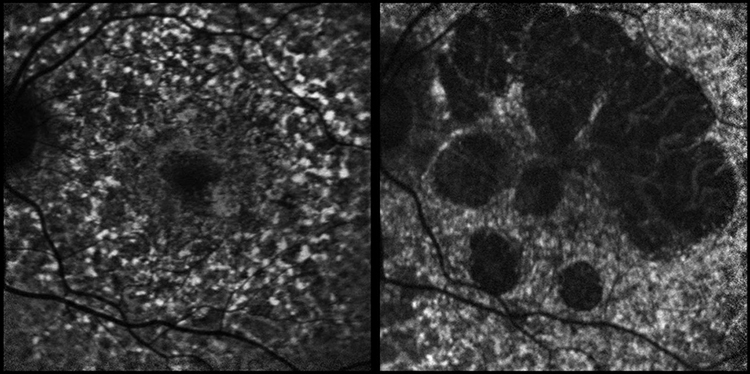 |
Figure 3 (Patient 8) Fundus autofluorescence at presentation and 4 years later, depicting the increase in areas of RPE atrophy. |
The average logMAR visual acuity (VA) for all 131 patients was 0.19. The mean duration of PPS use and mean cumulative dose in the suspect group were 4.2 years and 380g respectively and in the non-suspect group were 3.6 years and 442g (Table 1). Common other diagnoses for which patients were seen in the ophthalmology clinic included ocular surface issues (blepharitis, dry eye syndrome, meibomian gland dysfunction) (n=37), cataract: pre- or post-op (n=30), glaucoma/ocular hypertension (n=7), diabetic retinopathy surveillance (n=6), uveitis (n=8), and other issues including posterior vitreous detachment, retinal tear, esotropia, and migraine (n=23).
Discussion
Our study evaluated the prevalence of retinal pathology in a cohort of patients who had been exposed to PPS and examined in a tertiary care setting. Pearce et al described a potential association between chronic use of PPS and the development of a vision-threatening maculopathy,4 and Hanif et al recently reported a strong causal relationship between the two.4,9,10 An associated study with 35 patients noted that this maculopathy is associated with long-term exposure to PPS with a median of 15 years and a range of 3–22 years.10 Common symptoms of the maculopathy included difficulty reading, metamorphopsia, impaired dark adaptation, and nyctalopia.11 While several studies have shown the association of PPS to a maculopathy, some studies have discussed the possibility of IC causing the maculopathy itself.12,13
Given these findings, we conducted a retrospective chart review at our institution to look for evidence of retinal pathology in patients with PPS. Our suspect group was found to have been taking PPS for an average of 4.2 years and an average dosage 380g respectively while the non-suspect group took it for an average of 3.6 years at 442g. However, the median cumulative dosage for the non-suspect group was lower than that of the suspect group at 188.1g as opposed to 317g. This suggests that a majority of patients without pigmentary changes had lower exposure to the drug, with either a shorter duration and/or lower doses when compared to those in the suspect group.
Two patients from our cohort had fundus findings that were consistent with the maculopathy described by Pearce et al. However, it is of note that even patients with as little as 0.3 years on the drug had evidence of pigmentary changes documented in their chart. In our study cohort, age, gender, visual acuity, and duration of drug therapy were not found to be significant factors in the development of PPS-related maculopathy.
Although this is a retrospective analysis, this emphasizes the need to start monitoring patients on PPS early on as well as documenting a baseline comprehensive eye exam to identify any changes that occur during the use of the drug. When pathology was noted, it was commonly diagnosed as age-related macular degeneration or pattern dystrophy. Such diagnoses were also noted in the prior study by Hanif et al.8 Imaging analyses reported by Hadad et al showed that all patients (n=17) using 100mg of PPS daily for at least 3 years had mottling changes of the retina on near-infrared imaging, 75% of patients showed a hypoautofluorescence defect in the macula similar to those reported by Pearce et al,4 and hyperreflectivity, thickening of the foci of the RPE, and a flying saucer macular sign were also noted on OCT imaging.14
A recent prospective study by Wang et al found that patients with a cumulative dosage over 1500g had a significant risk of developing a PPS-associated maculopathy.6 They recommend baseline ophthalmological examinations with multimodal imaging of patients who are to receive PPS in a cumulative dose of about 500g. In our study cohort, Patient 9 was found to have prominent macular pigmentary findings that were consistent with the previously described PPS-associated maculopathy. However, this patient only had a cumulative dosage of 304.4g. Further study is needed to determine at what cumulative dosage patients become at risk for the development of PPS-associated macular changes.
Additionally, some patients in our suspect group were examined in the clinic post-drug cessation, so it is unclear at which point in their course of treatment pigmentary changes developed. A recent case study discussed the possibility of progressing maculopathy after discontinuation of the drug, where a 67-year-old woman with a history of PPS use for 18 years presented with worsening vision despite stopping the drug at the age of 62.15 Additionally, a retrospective study by Shah et al proposed that pigmentary changes can continue to develop for at least ten years after the cessation of PPS.16 Longitudinal study is required to understand the course of the PPS-associated maculopathy development.
Strengths of our work include the fact that our study cohort includes all patients taking PPS seen at the Northwestern Ophthalmology clinic during our study period, not just those seen in by a retina specialist. This prevented potential bias towards the existence of retinal findings. We were able to establish a relationship between the drug and macular pathology, and confirm recent findings by other authors. Lastly, since it was a retrospective study, there was minimal selection or recall bias. There are limitations to our study. Given that it was a single center study, the number of patients included in the analysis were limited. Consequently, our non-suspect group does not serve strictly as a control group because patients in both the suspect and non-suspect group experienced ocular comorbidities. This is one likely explanation for the lack of difference in average visual acuity between the two groups. Additionally, dates of medication discontinuation may not always be entered into the appropriate sections of the EHR and patients occasionally discontinue their medications on their own. The last date of PPS use was missing in the EHR for 48% of our patients, who may or may not have discontinued the drug. This affected our analysis for the true duration and cumulative dosage of the drug. Because of the retrospective nature of this study, data was derived from the existing EHR. Consequently, not all patients in the cohort had imaging on file, likely because conditions for which they were seen in the ophthalmology clinic frequently did not warrant any multimodal or posterior segment imaging. Even when posterior segment examination was performed, mild findings of early stages of the retinopathy could be easily missed. Educating eye providers is critical in early identification of patients who are on the drug, improving detection of new changes that develop during therapy, and ensuring regular follow up. Further, patients should be counseled on the potential side effects of the drug along with a careful consideration of the risks and benefits prior to starting PPS therapy. Lyons et al also recommend prescribing the lowest dose and duration of the medication if the decision to start PPS is made.17
Our study adds to the growing body of work that supports the presence of a distinct pigmentary maculopathy associated with chronic usage of PPS. Future study is warranted, and guidelines are in the process of being established for the screening for PPS-associated maculopathy. A prospective analysis employing baseline ophthalmologic exams, regular follow-up, along with multimodal imaging is important in understanding the course of the disease while patients are on the medication as well as after discontinuation.
Acknowledgments
Saena A. Sadiq, BS for her work which was critical in the revision of the manuscript, including additional literature review and incorporation of new findings into the manuscript, updating the tables, and reformatting the images.
Funding
No financial support was received for this study.
Disclosure
The authors have no proprietary or commercial interest in any of the materials discussed in this article and report no conflicts of interest in this work.
References
1. Berry SH, Elliott MN, Suttorp M, et al. Prevalence of symptoms of bladder pain syndrome/interstitial cystitis among adult females in the United States. J Urol. 2011;186(2):540–544. doi:10.1016/j.juro.2011.03.132
2. Chancellor MB, Yoshimura N. Treatment of interstitial cystitis. Urology. 2004;63(3):85–92. doi:10.1016/j.urology.2003.10.034
3. Anderson VR, Perry CM. Pentosan polysulfate. Drugs. 2006;66(6):821–835. doi:10.2165/00003495-200666060-00006
4. Pearce WA, Chen R, Jain N. Pigmentary maculopathy associated with chronic exposure to pentosan polysulfate sodium. Ophthalmology. 2018;125(11):1793–1802. doi:10.1016/j.ophtha.2018.04.026
5. Barnes AC, Hanif AM, Jain N. Pentosan polysulfate maculopathy versus inherited macular dystrophies: comparative assessment with multimodal imaging. Ophthalmol Retina. 2020;4(12):1196–1201. doi:10.1016/j.oret.2020.05.008
6. Wang D, Au A, Gunnemann F, et al. Pentosan-associated maculopathy: prevalence, screening guidelines, and spectrum of findings based on prospective multimodal analysis. Can J Ophthalmol. 2020;55(2):116–125. doi:10.1016/j.jcjo.2019.12.001
7. Vora RA, Patel AP, Melles R. Prevalence of maculopathy associated with long-term pentosan polysulfate therapy. Ophthalmology. 2020;27(6):835–836. doi:10.1016/j.ophtha.2020.01.017
8. Greenlee T, Hom G, Conti T, Babiuch AS, Singh R. Re: pearce et al.: pigmentary maculopathy associated with chronic exposure to pentosan polysulfate sodium (Ophthalmology. 2018; 125 (11):1793-1802). Ophthalmology. 2019;126(7):e51. doi:10.1016/j.ophtha.2018.12.037
9. Hanif AM, Armenti ST, Taylor SC, et al. Phenotypic spectrum of pentosan polysulfate sodium–associated maculopathy: a multicenter study. JAMA Ophthalmol. 2019;137(11):1275. doi:10.1001/jamaophthalmol.2019.3392
10. Hanif AM, Shah R, Yan J, et al. Strength of association between pentosan polysulfate and a novel maculopathy. Ophthalmology. 2019;126(10):1464–1466. doi:10.1016/j.ophtha.2019.04.024
11. Mogica JAP, De EJB. Pentosan polysulfate maculopathy: what urologists should know in 2020. Urology. 2020;
12. Ludwig CA, Vail D, Callaway NF, Pasricha MV, Moshfeghi DM. Pentosan polysulfate sodium exposure and drug-induced maculopathy in commercially insured patients in the United States. Ophthalmology. 2020;127(4):535–543. doi:10.1016/j.ophtha.2019.10.036
13. Jain N, Li AL, Yu Y, VanderBeek BL. Association of macular disease with long-term use of pentosan polysulfate sodium: findings from a US cohort. B J Ophthalmol. 2020;104(8):1093–1097. doi:10.1136/bjophthalmol-2019-314765
14. Hadad A, Helmy O, Leeman S, Schaal S, Novel Multimethod A. A novel multimethod image analysis to quantify pentosan polysulfate sodium retinal toxicity. Ophthalmology. 2020;127(3):429–431. doi:10.1016/j.ophtha.2019.10.013
15. Huckfeldt RM, Vavvas DG. Progressive maculopathy after discontinuation of pentosan polysulfate sodium. Ophthalmic Surg Lasers Imaging Retina. 2019;50(10):656–659. doi:10.3928/23258160-20191009-10
16. Shah R, Simonett JM, Lyons RJ, Rao RC, Pennesi ME, Jain N. Disease course in patients with pentosan polysulfate sodium-associated maculopathy after drug cessation. JAMA Ophthalmol. 2020;138(8):894–900. doi:10.1001/jamaophthalmol.2020.2349
17. Lyons RJ, Ahmad S, Ansari S, Foote JE, Jain N. Pentosan polysulfate-associated macular disease in patients with interstitial cystitis. Obstet Gynecol. 2020;135(5):1091–1094. doi:10.1097/AOG.0000000000003794
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.