Back to Journals » Clinical Ophthalmology » Volume 14
Long-Term Effects of Botulinum Toxin in Large-Angle Infantile Esotropia
Authors Gallo FG, Plaitano C, Esposito Veneruso P, Magli A
Received 8 July 2020
Accepted for publication 18 August 2020
Published 19 October 2020 Volume 2020:14 Pages 3399—3402
DOI https://doi.org/10.2147/OPTH.S266652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Flavio Gioele Gallo,1 Carmen Plaitano,2 Paolo Esposito Veneruso,3 Adriano Magli1
1Department of Medicine and Surgery, University of Salerno, Salerno, Italy; 2Department of Ophthalmology, A.O.U. San Giovanni Di Dio e Ruggi d’Aragona-Scuola Medica Salernitana, Salerno, Italy; 3Division of Ophthalmology, University Hospital “Federico II”, Naples, Italy
Correspondence: Flavio Gioele Gallo
Department of Medicine and Surgery, University of Salerno, Via Salvador Allende, 43, Baronissi, Salerno 84081, Italy
Tel +39 3898535899
Email [email protected]
Purpose: The purpose of this study is the motor outcome analysis of early Botulinum toxin (BT) treatment in patients affected by large-angle infantile esotropia (IE).
Patients and Methods: Retrospective analysis of 130 medical charts of IE patients who underwent BT injections between 2004 and 2019 was performed. All patients underwent BT injections within 13 months of age.
Results: Thirty patients, matching the inclusion criteria, were included in the study. Twenty-eight patients showing residual ET ≥ 25 PD (34.3± 6.6 PD ranged from 25 to 50) underwent surgery.
Conclusion: Our result after 1 Botulinum toxin injection showed a very low success rate (6.7%) at last follow-up (28.3± 7.2 months). Our data would suggest one Botulinum toxin injection in children affected by large-angle infantile esotropia allows a significant reduction of deviation but does not avoid the need for surgical treatment.
Keywords: strabismus, pediatric, congenital
Introduction
Infantile esotropia (IE) is defined as an early-onset esodeviation, usually within 6 months of age, with an estimated incidence of 0.1–1.0%.1–5 Although the role of visual cortex and cortico-mesencephalic-cerebellar pathways has been proposed, the etiology of IE is still unknown.6
In order to achieve satisfactory motor and sensory outcome in IE patients, some authors recommend first surgery between 2 and 4 years of age, after the appropriate treatment of amblyopia.7 Since 1980, the encouraging results obtained by using the transitory medial rectus (MR) muscles denervation induced by Botulinum toxin (BT) injection in patients affected by IE, made this procedure a reliable alternative to the surgical one, though more debatable results are reported (Table 1).8–19
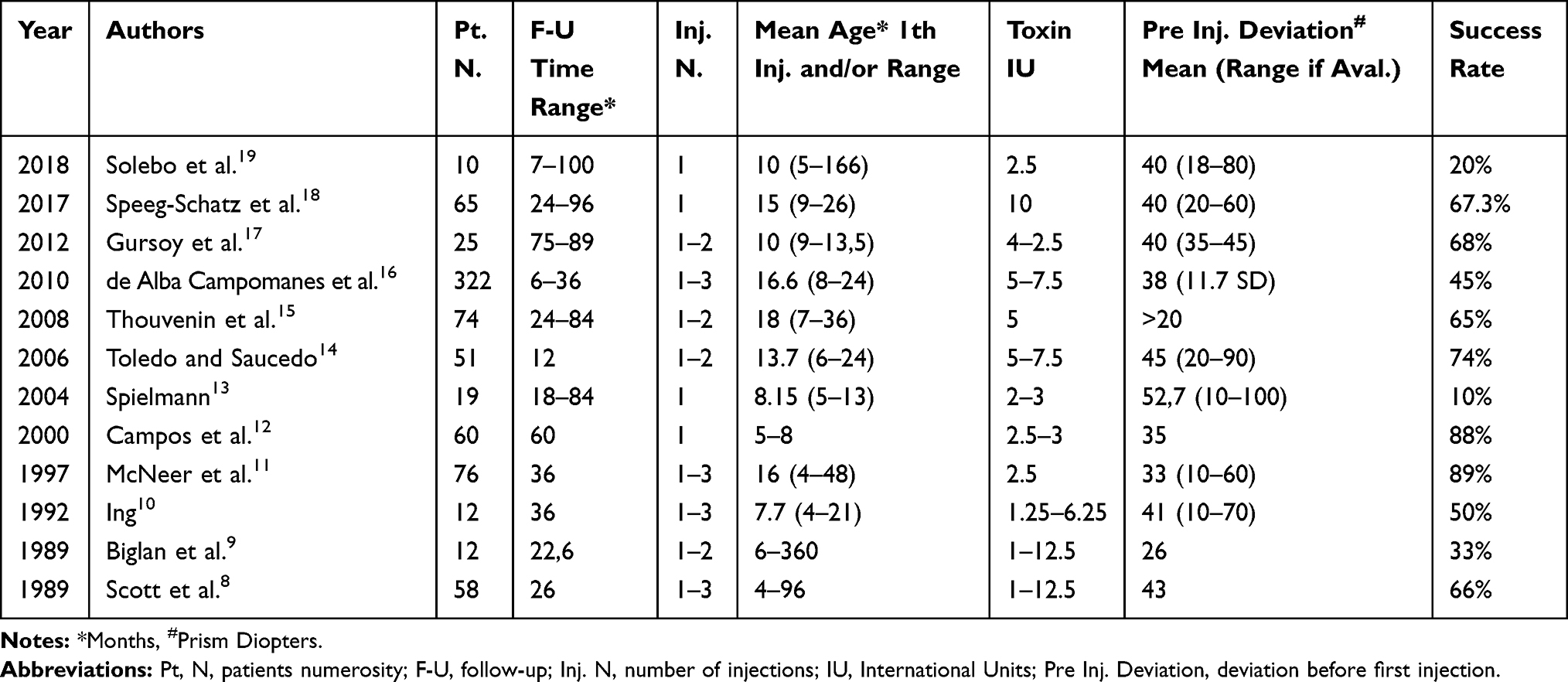 |
Table 1 Results reported by other studies |
The purpose of this study is the motor outcome analysis of early BT treatment in patients affected by large-angle IE.
Patients and Methods
Retrospective analysis of 130 medical charts of IE patients who underwent BT injections between 2004 and 2019 was performed. All patients underwent extensive ophthalmological and orthoptic examination according to the patients’ age and cooperation including best corrected visual acuity (BCVA) using 5 meters Landolt C or Albini E charts, cycloplegic refraction (atropine 0.5%), Krimsky and/or Hirschberg tests, cover, cover-uncover and prismatic alternating cover test, doll’s head maneuver, Worth 4-dot test, TNO stereotest, biomicroscopy and fundus examination.
Inclusion criteria were: large-angle esotropia, ≥40 prism diopters (PD) diagnosed within 6 months of age, hyperopic spherical equivalent (SE) within 3D, follow-up >5 years, BT injection within 13 months of age. Patients showing nystagmus, upshoot, duction limitation, dissociated vertical or horizontal deviation (DVD/DHD), A-V pattern, accommodative component, neurological or systemic disease, ocular abnormalities or previous ocular surgery were excluded from the study.
Botulinum toxin A (Botox; Allergan, Irvine, CA) injection was administered under general anesthesia (sevoflurane inhalation) using a 27-gauge needle on an insulin syringe after conjunctival limbal incision and MR isolation, without electromyographic guidance. Bilateral medial rectus injections of 5 IU in 0.25 mL of saline for deviations between 40 and 50 PD and 7 IU in 0.35 mL for deviations greater than 50 PD were performed.
Residual esotropia ≥20 PD in patients beyond 24 months of age were surgically treated according to the Helveston recommendations.20
Written informed consent for treatment and to review the patient’s medical records for research purposes was provided by parents or legal guardians before each treatment for all patients. The study followed the tenets of the Declaration of Helsinki. Ethical approval for the protocol was obtained from the Institutional Review Board of University of Salerno.
Results
Thirty patients, matching the inclusion criteria, were included in the study. Clinical and demographic data are shown in Table 2.
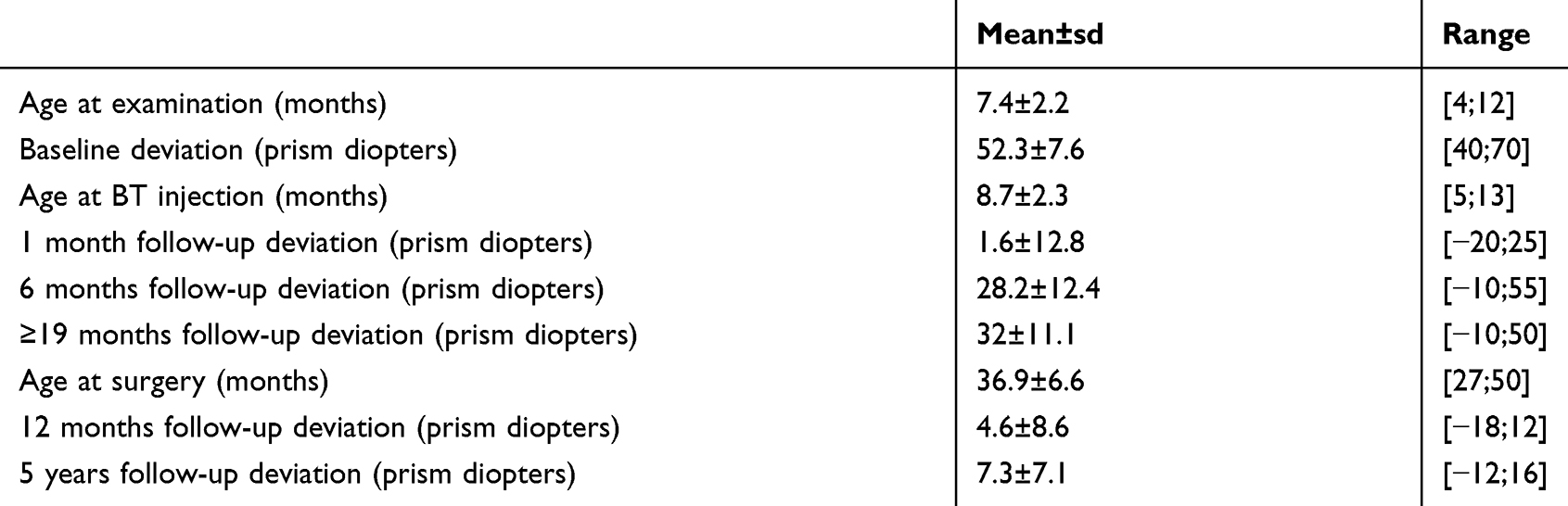 |
Table 2 Demographic and Clinical Data |
All patients underwent BT injection within 13 months of age with a mean follow-up period of 28.3±7.2 months (ranged from 19 to 43). At 1 month post-injection examination, all patients showed a significant reduction of deviation (ranged from −20 to 25 PD); 5 patients were orthotropic (16.7%), 11 showed a consecutive XT (36.7%) and 14 showed residual ET (46.7%). Seventeen patients showed a residual deviation of ±10 PD (success rate of 56.7%). At 6 months follow-up the success rate decreased to 6.7% and was unvaried at the last follow-up (28.3±12.4 months). Mean deviation from baseline to last follow-up decreased by 20.3±13.3 (ranged from 0 to 60).
Twenty-eight patients showing residual ET ≥25 PD (34.3±6.6 PD ranged from 25 to 50) underwent surgery. At 6 months and 3 years after surgery follow-up mean deviation was 3.9±9.3 PD (ranged from −18 to 10) and 4.1±8.5 PD (ranged −12 to 14), respectively.
At the final examination, 28 patients (93.3%) showed monocular or alternating suppression, 7 (23.3%) showed gross stereopsis (>480 arc) and 23 (76.7%) had no stereopsis.
Discussion
The effects of Botulinum toxin in patients affected by infantile esotropia represent a controversial issue. Previous literature data including age at injection, BT dose, number of injections, amount of deviation and consequently results are extremely variable and, considering the lack of standards, the procedure settings actually rely on each surgeon (Table 1).
Although Campos et al.12 reported patients treated at or before 6.5 months were more likely to respond favorably to BT treatment and Speeg-Schatz et al.18 reported a positive correlation between age at injection and postoperative angle, McNeer et al.11 did not find any statistical difference between patients injected before and after 12 months of age even if his limited sample size needs to be considered. Moreover, multivariate analysis performed by de Alba Campomanes et al.16 in one of the largest prospective studies, showed the most important predictor of alignment was the preoperative amount of deviation. They reported a significant difference between the amount of deviation in patients who achieved satisfactory motor outcome and those who did not; independently by age at treatment and number of injections the success rate of ≤30∆ esotropia BT-treated was not different than that of surgery. Thouvenin et al.15 reported similar results on 74 esotropic patients, describing that the only predictive factor of treatment failure was the presence of high adduction.
Early treatment of infantile esotropia should consider the spontaneous resolution rate, in infants under 9 months, of 27%, typically occurring in the intermittent or variable form of esotropia, and 9% in constant ones, as reported by PEDIG.21
In our study only constant, large-angle esotropia with no vertical deviation, injected before 13 months of age, were considered in order to minimize bias related to a wide range of baseline deviation, age at injection, recurrence of deviation due to vertical component/inferior oblique overaction or variable deviation due to associated accommodative component. Our results after 1 Botulinum toxin injection showed a very low success rate (6.7%) at last follow-up (28.3±7.2 months). Differences between our results and those describing success rates from 66% up to 89% (Table 1) might be partially explained by our strict inclusion criteria, especially the baseline deviation one. We found a mean reduction of baseline deviation (52±7.5; range 40–70 PD) of 19.3±11.2 PD at last follow up, significantly lower than 33 PD reported by McNeer et al. (who included multiple injection patients), but wide enough to justify, according to Campomanes et al., the efficacy of BT in the treatment of small-to-moderate angle esotropia. Although there are frequent complications of Botulinum toxin injections, such as transient ptosis, subconjunctival hemorrhage, and vertical deviation, no serious complication were observed in our series, but diffusion of the toxin was observed in 1 patient showing ptosis, which spontaneously resolved in 4 months. Exotropia as overcorrection is considered a desirable outcome of BT injection readjusting the fusion pathway though the visual feedback.12 Exotropia was present in 7 patients (23.3%) at 6 months follow-up and in only 1 patient (3.3%) at the last one.
More than 90% of BT-treated patients showed a significant amount of esotropia requiring surgery.
Recession-resection procedure performed in a patient with more than 20 PD of residual esotropia, according to previous literature, showed a success rate of 78.5% and 64.3% at 6 months and 5 years follow-up, respectively. At final examination, patients with a residual deviation of 0 to +8 PD achieved a gross stereopsis (25%).
Despite the limitations of the study, such as limited sample size and lack of control group, this represents, to our knowledge, the first study focused exclusively on treatment of large-angle infantile esotropia treatment. Large-scale multicentre clinical trials using well established inclusion criteria would be very useful to clarify Botulinum toxin's effective role in infantile esotropia management.
Conclusion
In conclusion, our data would suggest one Botulinum toxin injection in children affected by large-angle infantile esotropia allows a significant reduction of deviation but does not avoid the need for surgical treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nixon RB, Helveston EM, Miller K, Archer SM, Ellis FD. Incidence of strabismus in neonates. Am J Ophthalmol. 1985;100(6):
2. Friedman Z, Neumann E, Hyams SW, Peleg B. Ophthalmic screening of 38,000 children, age 1 to 2 1/2 years, in child welfare clinics. J Pediatr Ophthalmol Strabismus. 1980;17(4):261–267.
3. Scobee RG. Esotropia. Incidence, etiology, and results of therapy. Am J Ophthalmol. 1951;34(6):817–833.
4. Louwagie CR, Diehl NN, Greenberg AE, Mohney BG. Is the incidence of infantile esotropia declining?: a population-based study from Olmsted County, Minnesota, 1965 to 1994. Arch Ophthalmol. 2009;127(2):200–203. doi:10.1001/archophthalmol.2008.568
5. Major A, Maples WC, Toomey S, DeRosier W, Gahn D. Variables associated with the incidence of infantile esotropia. Optometry. 2007;78(10):534–541. doi:10.1016/j.optm.2006.11.017
6. Brodsky MC. An expanded view of infantile esotropia: bottoms up! Arch Ophthalmol. 2012;130(9):1199–1202. doi:10.1001/archophthalmol.2012.2067
7. Simonsz HJ, Kolling GH. Best age for surgery for infantile esotropia. Eur J Paediatr Neurol. 2011;15(3):205–208. doi:10.1016/j.ejpn.2011.03.004
8. Scott AB, Magoon EH, McNeer KW, Stager DR. Botulinum treatment of strabismus in children. Trans Am Ophthalmol Soc. 1989;87:174–184.
9. Biglan AW, Burnstine RA, Rogers GL, Saunders RA. Management of strabismus with botulinum A toxin. Ophthalmology. 1989;96(7):935–943. doi:10.1016/s0161-6420(89)32776-x
10. Ing MR. Botulinum alignment for congenital esotropia. Trans Am Ophthalmol Soc. 1992;90:361–371.
11. McNeer KW, Tucker MG, Spencer RF. Botulinum toxin management of essential infantile esotropia in children. Arch Ophthalmol. 1997;115(11):1411–1418. doi:10.1001/archopht.1997.01100160581010
12. Campos EC, Schiavi C, Bellusci C. Critical age of botulinum toxin treatment in essential infantile esotropia. J Pediatr Ophthalmol Strabismus. 2000;37(6):328–355.
13. Spielmann AC. La toxine botulique dans les ésotropies précoces [Botulinum toxin in infantile estropia: long-term results]. J Fr Ophtalmol. 2004;27(4):358–365. doi:10.1016/s0181-5512(04)96141-4
14. Toledo R, Saucedo A. Resultados en endotropia no acomodativas tratadas con toxina botulinica. Rev Mex Oftalmol. 2006;80:64–68.
15. Thouvenin D, Lesage-Beaudon C, Arné JL. Injection de toxine botulique dans les strabismes précoces. Efficacité et incidence sur les indications chirurgicales ultérieures. A propos de 74 cas traités avant l’âge de 36 mois [Botulinum injection in infantile strabismus. Results and incidence on secondary surgery in a long-term survey of 74 cases treated before 36 months of age]. J Fr Ophtalmol. 2008;31(1):42–50. doi:10.1016/s0181-5512(08)70329-2
16. de Alba Campomanes AG, Binenbaum G, Campomanes Eguiarte G. Comparison of botulinum toxin with surgery as primary treatment for infantile esotropia. J AAPOS. 2010;14(2):111–116. doi:10.1016/j.jaapos.2009.12.162
17. Gursoy H, Basmak H, Sahin A, Yildirim N, Aydin Y, Colak E. Long-term follow-up of bilateral botulinum toxin injections versus bilateral recessions of the medial rectus muscles for treatment of infantile esotropia. J AAPOS. 2012;16(3):269–273. doi:10.1016/j.jaapos.2012.01.010
18. Speeg-Schatz C, Burgun P, Gottenkiene S. To what extent may Botulinum toxin type A injections be an alternative choice to surgery in infantile esotropia? Eur J Ophthalmol. 2017;27(3):285–288. doi:10.5301/ejo.5000947
19. Solebo AL, Austin AM, Theodorou M, Timms C, Hancox J, Adams GGW. Botulinum toxin chemodenervation for childhood strabismus in England: national and local patterns of practice. PLoS One. 2018;13(6):e0199074. doi:10.1371/journal.pone.0199074
20. Helveston EM. A logical scheme for the planning of strabismus surgery. In: Craven L, editor. Surgical Management of Strabismus: An Atlas of Strabismus Surgery.
21. Pediatric Eye Disease Investigator Group. Spontaneous resolution of early-onset esotropia: experience of the congenital esotropia observational study. Am J Ophthalmol. 2002;133(1):109–118. doi:10.1016/s0002-9394(01)01316-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.