Back to Journals » Nursing: Research and Reviews » Volume 5
Living with fibromyalgia: results from the functioning with fibro survey highlight patients' experiences and relationships with health care providers
Authors Golden A, D'Arcy Y, Masters ET, Clair A, Malik V
Received 3 March 2015
Accepted for publication 12 July 2015
Published 20 November 2015 Volume 2015:5 Pages 109—117
DOI https://doi.org/10.2147/NRR.S83847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Cindy Hudson
Angela Golden,1 Yvonne D'Arcy,2 Elizabeth T Masters,3 Andrew Clair3
1NP from Home, LLC, Munds Park, AZ, 2Pain Management and Palliative Care, Suburban Hospital-Johns Hopkins Medicine, Bethesda, MD, 3Pfizer, New York, NY, USA
Abstract: Fibromyalgia (FM) is a chronic disorder characterized by widespread pain, which can limit patients' physical function and daily activities. FM can be challenging to treat, and the treatment approach could benefit from a greater understanding of patients' perspectives on their condition and their care. Patients with FM participated in an online survey conducted in the USA that sought to identify the symptoms that had the greatest impact on patients' daily lives. The purpose of the survey was to facilitate efforts toward improving care of patients by nurse practitioners, primary care providers, and specialists, in addition to contributing to the development of new outcome measures in both clinical trials and general practice. A total of 1,228 patients with FM completed the survey, responding to specific questions pertaining to symptoms, impact of symptoms, management of FM, and the relationship with health care providers. Chronic pain was identified as the key FM symptom, affecting personal and professional relationships, and restricting physical activity, work, and social commitments. Patients felt that the severity of their condition was underestimated by family, friends, and health care providers. The results of this survey highlight the need for nurse practitioners, primary care providers, and specialists to provide understanding and support to patients as they work together to enable effective diagnosis and management of FM.
Keywords: fibromyalgia, pain, survey, impact, support
Introduction
Fibromyalgia (FM), a multifactorial disease that predominantly affects women, is characterized by widespread pain and associated with a range of symptoms, including sleep disturbance, fatigue, and headache.1,2 Onset of symptoms is typically in the age range of 30–40 years, and often results in limitations in physical function and daily activities, severely impacting patients’ quality of life.3,4 FM affects between 2% and 6% of the US adult population and is associated with a significant economic burden on health care systems, patients with FM, and their families.5–7
The lack of widespread understanding of FM symptoms, coupled with an overlap of these symptoms with other conditions such as chronic fatigue syndrome, depression, anxiety, and irritable bowel syndrome, means that FM can be challenging to diagnose and treat.8,9 A recent survey reported that the mean time between a patient initially experiencing symptoms of FM and the first visit to a physician was 11 months, with a mean time from first visit to diagnosis of FM of 2 years.10 Many primary care practices do not require specialized training in FM and are underprepared to fully address the needs of patients with FM. In some cases, diagnosis of FM can take up to 5 years, significantly extending patient contact time with health care providers (HCPs) and placing an emotional and financial burden on patients.8 A large proportion of physicians report that patients with FM appear to find it difficult to communicate their symptoms.11 Moreover, some physicians state difficulty in developing a long-term treatment plan for patients with FM, mainly owing to a reported lack of awareness and understanding of the condition.10 The absence of a consensus on diagnosis and treatment approaches among physicians can result in misdiagnosis and under-treatment in the management of patients with FM, and adds to the significant economic burden for health care systems and patients.11 At the same time, this negatively impacts the credibility of FM as a “real” disorder with an underlying pathological basis of dysfunctional pain processing in the central nervous system.12 Patient education following diagnosis is the first key step toward management of FM in order to provide reassurance and validation of the cause of symptoms, and can improve patients’ outlook and well-being.13 Patients take confidence from physicians’ support, as together they can establish realistic expectations on coping with FM, along with discussing treatment options and their long-term prognosis.14
Patient self-report via questionnaires may be used to gain an insight into the impact of FM, and may act as a precursor to defining optimal outcome measures in clinical trials.15 Thus far, only a small number of surveys have measured patient perspectives on living with FM.3,10,16 The results of these surveys, together with insights shared by patients and their HCPs, suggest that of the symptoms experienced by patients with FM, pain can have the greatest impact on daily life. Moreover, there continues to be a perceived stigma associated with FM, potentially due to the lack of a physiological basis of the condition.3,17 A greater awareness of how this perceived stigma impacts patients may help to dispel it.
Here, we report findings from the Functioning with Fibro survey, the goal of which was to document patients’ perspectives on living with FM and to better understand the impact of pain on their overall quality of life. The results presented here provide an overview of FM patients’ abilities to perform daily tasks, take part in physical activities, as well as the impact of FM-associated pain on personal and professional relationships. The support that patients with FM receive from personal and professional networks was also assessed. Insights from the findings of this study may benefit nurse practitioners (NPs), physician assistants, primary care providers (PCPs), and specialists as they work with FM patients to help them better understand and manage their pain and other symptoms.
Methods
Survey design
The Functioning with Fibro survey was a noninterventional survey of patients with FM, conducted from August 9 to 23, 2013, by Kelton Global, and designed and carried out in the USA in collaboration with the National Fibromyalgia and Chronic Pain Association and the American Association of Nurse Practitioners. The participants provided consent and approval for the use of their data by third parties prior to undertaking an online survey. This study was conducted in accordance with the Declaration of Helsinki and adhered to the US Code of Standards and Ethics for Market, Opinion, and Social Research. Participation was encouraged without undue intrusion with the privacy and confidentiality of participants protected. Patients were compensated, up to a maximum of US$3, for taking part in the survey.
Participants were recruited by Kelton Global via Survey Sampling International (SSI), LLC, which is a market research sample provider. The participants in SSI’s web panel were recruited from different regions of the USA, following Internet newsletter campaigns, registration with panel partners, as well as by affiliate and media networks. The demographic information of the participants was pooled prior to sampling to ensure consistency and even distribution of the sample population.
In order to qualify, patients had to self-report that they were diagnosed with FM by an HCP. The 23,706 patients randomly selected from SSI’s database were sent email invitations with a link to the survey. The 1,936 respondents to the email invitations were further asked a screener question to confirm their FM diagnosis by an HCP, in addition to diagnosis of any comorbid disorders. A total of 708 patients were terminated from the survey because of the inability to fulfill the inclusion criteria. The remaining 1,228 patients completed the survey and were included in this analysis.
Survey questions
The survey questionnaire consisted of 57 items and included sections on demographics, FM diagnosis, symptoms, the impact of FM on activities of daily living, personal and professional relationships, and questions relating to treatment and symptom management. The survey used five-point Likert scales (eg, 1= no impact at all to 5= extreme impact; 1= not at all helpful to 5= extremely helpful; 1= not at all to 5= an extremely significant amount; 1= much more severe to 5= much better; 1= not at all important to 5= extremely important; and 1= no understanding at all to 5= extremely understanding). Participants were asked to rate their FM-related pain on a typical day using a numeric rating scale (range 1–10, where 1= no pain at all and 10= worst possible pain). An agreement scale (range 1–4, where 1= strongly agree and 4= strongly disagree) was also used.
Data analysis
A small-scale test survey including ~100 participants was conducted before the full launch to ensure the viability of the responses to the survey questionnaire. The responses collected from the small-scale test survey were included in the final data set. The number of patients who completed the survey was estimated to provide 95% confidence of a margin of error of no >2.8% points in any response. Data were summarized descriptively with proportions, and mean and median scores were calculated.
Results
Demographic characteristics
A total of 1,228 patients with FM (aged ≥18 years) from each region of the USA (Northeast: 19%, Midwest: 26%, South: 35%, and West: 21%) completed the online survey. Their mean age was 50.7 years, and the majority were female (85%). Overall, 746 (61%) were married or in a serious relationship, and 409 (33%) were employed in some capacity (Table 1). The most common patient-reported comorbid disorders were arthritis (57%) and depression (53%) (Table 2).
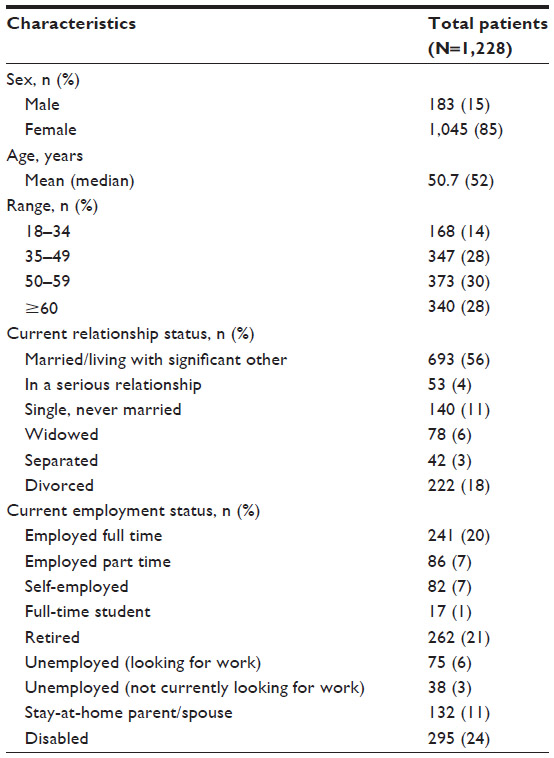 | Table 1 Patient demographics |
 | Table 2 Clinical characteristics |
Patients’ perspectives on FM and impact on daily activities and relationships
Participants were asked to state the level of impact of 17 common FM symptoms on their daily activities. The largest proportion of patients reported fatigue/low energy (77%) and chronic widespread pain (75%) as having a great impact (score of 4 or 5 on the five-point Likert scale, where 1= no impact at all and 5= extreme impact) on their day-to-day lives (Figure 1).
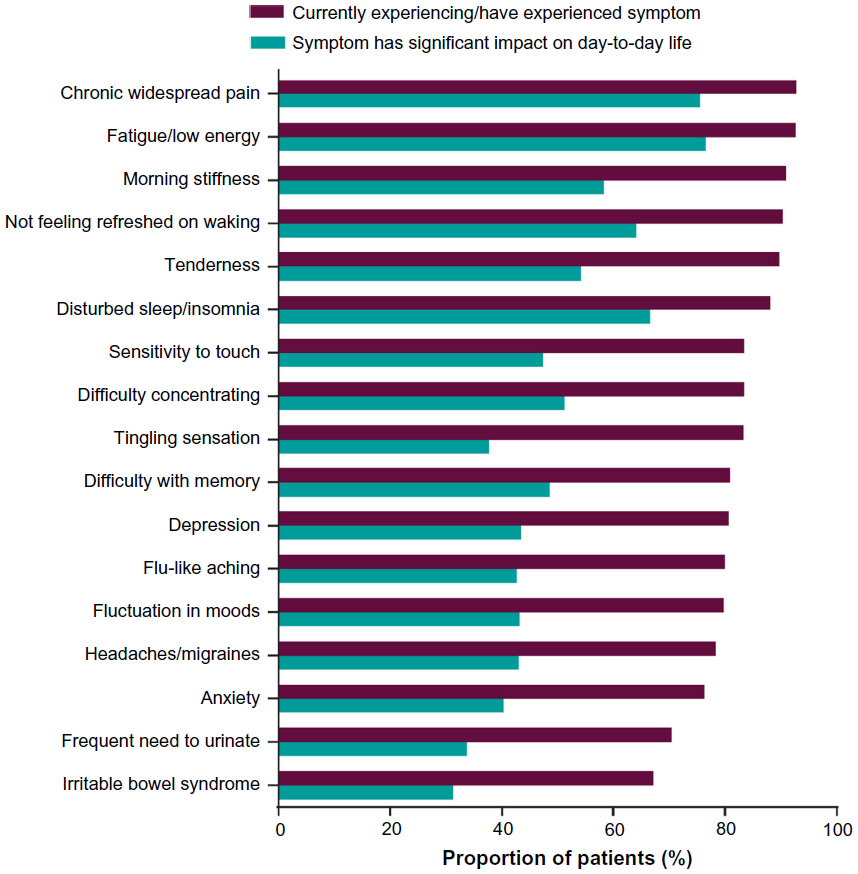 | Figure 1 Common symptoms and their impact on daily life. |
When asked to state the one symptom that had the greatest impact on their day-to-day lives, 41% of patients selected chronic widespread pain. The next most common responses were fatigue/low energy (19%) and disturbed sleep/insomnia (8%). When asked how much (if at all) FM pain limited their ability to carry out daily activities, the majority (55%) of patients stated that they were limited by a somewhat significant to an extremely significant amount (ie, by 51%–100%). When asked about the level of impact of FM-associated pain on reducing the ability to perform a list of specific daily activities, >70% of patients reported a severe impact (score of 4 or 5 on the five-point Likert scale, where 1 = no impact at all and 5 = extreme impact) on their ability to participate in a leisurely physical activity, as well as their ability to sleep (Figure 2).
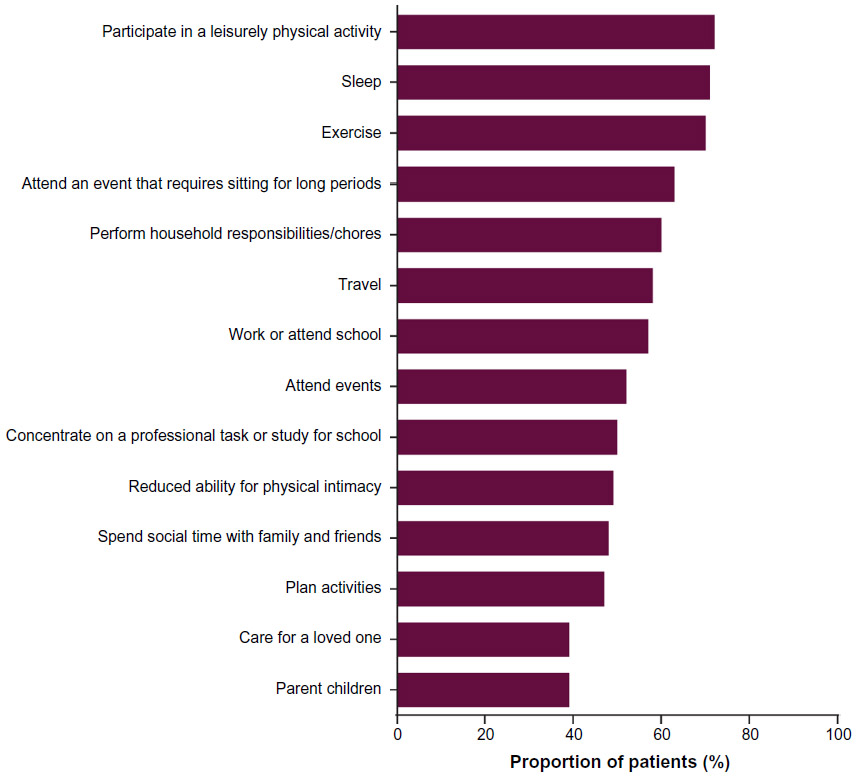 | Figure 2 Impact of fibromyalgia-associated pain on daily life. |
Male patients were not more likely than female patients to report a severe impact of FM-related pain on daily activities. However, a higher proportion of female patients reported being inactive as a result of FM-related pain (38% [399/1,045] vs 26% [47/183] of males).
FM pain was reported to have negatively impacted romantic relationships of the majority (55%) of patients. Of these, 68% (457/676) indicated that pain had forced them to limit physical intimacy with their partners. Of all patients, many also felt that FM pain had negatively impacted friendships and social relationships (54%), as well as family relationships (48%), which included relationships with children, grandchildren, or siblings.
Of those patients who were employed, 50% (205/409) had missed ≥1 day of work in the 12 months prior to the survey as a result of FM pain, with an estimated mean (median) 32.2 (8) total days missed.
Patient awareness and management of FM pain
A total of 57% of patients reported that they currently had a good understanding of treatment and management strategies when asked about the ways in which they managed and sought treatment for FM symptoms. However, the proportion of patients with a good understanding of the available pain treatment strategies upon being initially diagnosed was much lower (33%). The majority (75%) of patients were using at least one medication to treat their FM symptoms, of which the proportion of males was higher than females (86% [157/183] vs 73% [766/1,045]). A higher proportion of patients who had never been on medication or were not taking medication at the time of the survey rated their pain as “severe” (8–10 on the survey pain rating scale), as compared with those who were currently on medication (33% vs 5%, respectively). Mean (median) pain scores were 4.9 (5) for patients on medication and 7.1 (7) for patients not taking medication.
While many patients (61% [752/1,228]) were not satisfied with the level of pain relief following treatment and lifestyle changes, most patients (72%) believed that the combination of both medication and lifestyle changes (as opposed to either alone) would best contribute to an improvement in quality of life and reduction of FM-associated pain. The majority (97%) of patients had followed at least one lifestyle strategy or plan in an attempt to improve their ability to cope with FM pain. The most commonly employed strategies were to minimize stress (68%), use vitamins or supplements (63%), and set limits such as taking on fewer commitments (55%). Many patients (64%) also engaged in some form of physical exercise (eg, swimming and walking) for ≥30 minutes at least once per week. Of those patients who engaged in any form of physical exercise, 26% (203/782) reported an improvement in their pain/symptoms, whereas 41% (321/782) reported worsening of FM symptoms following exercise.
Relationship between patients and HCPs/personal support network
In order to manage their condition, 45% of patients consulted a PCP (including family doctor, internist, or obstetrician/gynecologist) more often than any other single source. Other common sources of support included rheumatologists (16%) and pain management specialists (13%), while only 5% of patients reported having consulted an NP most often for their condition. Overall, 64% of patients stated that pain management was the most commonly discussed topic with their HCPs (including PCPs, NPs, PAs, and specialists). Despite this, only 34% of patients believed that their relationship with their HCPs had improved their management of FM, so that they were able to better manage pain associated with FM as a result. When asked to identify those who were very helpful in influencing their understanding of identifying symptoms, finding support, and managing the condition, 61% identified their HCPs, 45% identified friends who have FM, and 40% identified their family. Of the HCPs visited for their condition, 40% of patients stated that rheumatologists best understood their pain compared with 11% who felt that NPs did.
The majority of patients set personal goals for improving their FM, either by themselves or together with their HCPs. Of the patients who tracked their progress in reaching their FM goals, 32% (344/1,076) discussed their goals with their HCPs, whereas 24% (258/1,076) of patients discussed their goals with friends and family. Moreover, 23% (244/1,076) believed that their goals motivated them to adhere to their treatment plan, 22% (236/1,076) felt that these goals were helpful in their overall treatment plan, and 34% (364/1,076) stated that they sometimes felt disappointed at not being able to reach a specific goal. Some patients (15% [166/1,076]) used alternative therapy, including massage and acupuncture, in an attempt to reach their goals.
For most patients, it was very important that individuals around them, including family members, coworkers, and their HCPs, understood what they were experiencing with FM pain. However, a lower proportion of patients felt that individuals supporting them had a very good understanding of their current experiences with FM pain (Figure 3). Of those patients who experienced days with more pronounced symptoms (“flare-up” days), 44% (531/1,207) felt that their family and friends did not take their pain seriously and thought that they were overreacting.
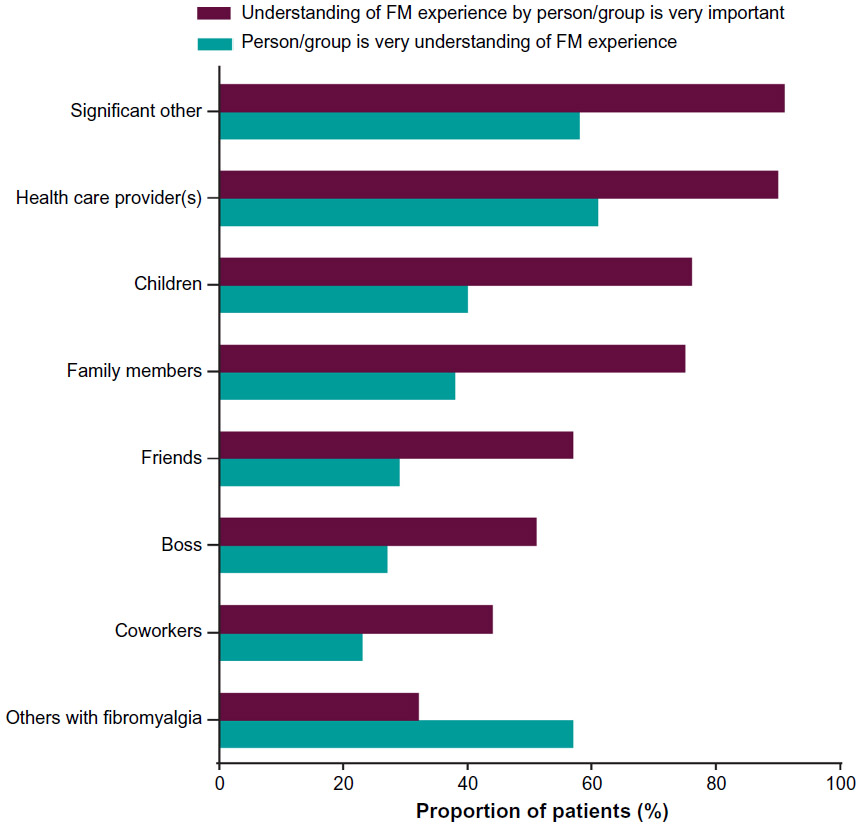 | Figure 3 Understanding of FM pain by support networks. |
Discussion
This survey demonstrates that FM imparts a significant burden on patients and negatively impacts their day-to-day activities and emotional well-being. FM is characterized by multiple symptoms, but here chronic widespread pain and fatigue were reported to be most commonly experienced by patients. Although the issues surrounding FM management may be common to other chronic pain conditions, the impact of these issues may be more pronounced in the case of FM than other pain conditions that have an established etiology and are void of the societal stigma associated with FM.
The high prevalence of sleep difficulty symptoms reported by 88% of patients is also noteworthy. Chronic widespread pain was reported by the majority of patients with FM as being disruptive to activities of daily living, with a severe impact on overall quality of life. Although pain is a hallmark symptom of FM, it is currently unclear if the symptoms of non-restorative sleep and fatigue occur secondary to pain or result from other physiological conditions.18
For the majority of the questions in this survey, there were no notable differences in the responses given by females and males. Female patients were more likely to be inactive as a result of FM-related pain compared to males, and males were more likely to be taking medication for FM symptoms. However, these differences were not large and, given the relatively low number of male participants in the survey (183 vs 1,045 female), may not be broadly generalizable.
While the initial diagnostic criteria published by the American College of Rheumatology had the requirement of a tender point examination to confirm diagnosis,1 the updated criteria (2010)19 characterized FM as a pain disorder while considering the impact of comorbid conditions. This study again shows that pain is the key symptom for patients with FM.
However, several studies have reported the lack of recognition of FM symptoms by physicians.20,21 This lack of symptom observation in the absence of objective measures for their recognition can negatively impact the timely diagnosis of FM, thereby posing a major hurdle for the effective clinical management of patients. Previous studies have also concluded that physicians find it challenging to diagnose FM due to an overlap of symptoms with other conditions, or because of other commonly experienced comorbid conditions.11,22 This fact was highlighted in a recent survey, where only 44% of physicians expressed a willingness to accept patients with FM, with their hesitancy mainly owing to the difficulty in treating an array of symptoms as well as to the emotional impact and stigma that patients face as a result of the condition.17,20 Physicians who attributed preexisting risk factors or “stressors”, such as physical trauma contributing to FM,23,24 were more likely to offer support and treatment to patients with FM than those who regarded FM as a psychological condition, with greater support and treatment more likely to lead to better outcomes for patients.20
The lack of appropriate training, lack of knowledge of FM, as well as patients’ difficulty in communicating their symptoms have been identified by HCPs as factors leading to delayed diagnosis.11 Providing improved training to HCPs on the available diagnostic criteria as well as efforts to improve HCP–patient dialog may reduce time to FM diagnosis, resulting in streamlining of contact between patients and physicians. This would enable physicians to develop a treatment plan earlier in the course of the disease, and in turn may help reduce disease burden.6,20 FM is characterized by the presence of multiple symptoms where outcomes are likely affected by genetic, cognitive, and social factors. A multidisciplinary, personalized treatment approach is therefore advocated, wherein the treatment plan reflects patients’ priorities and expectations, level of function, and presence of comorbid conditions.13,25,26 The optimal treatment regimen therefore requires a collaborative effort from the HCP and the patient and should involve patient education, along with a multimodal treatment approach comprising pharmacological and nonpharmacological elements.27 This survey demonstrates that most patients understand the need for a multimodal approach, with 72% of the patients believing that a combination of medication and lifestyle changes, such as rest, stress reduction, massage, sleep hygiene, mild physical activity, and cognitive behavioral therapy,13 is required for improvement.
While patients in this survey who were taking prescription medication to treat their FM symptoms did have notably lower pain scores than those who were not, most patients nevertheless indicated that they were not satisfied with the level of pain relief following medication. This further highlights the importance of a treatment approach that addresses the range of FM symptoms. The inclusion of physical activity, such as aerobic exercises, alone, or in combination with other nonpharmacological therapies, can address the long-term management of fatigue and has proven beneficial toward improving function.27 However, in this survey, patients were more likely to report worsening of symptoms than improvement with exercise (41% vs 26%). This survey did not record the level of activity and managed exercise tailored to the capabilities of the patient may be required to improve function.
Only one third of patients in this study had a good understanding of FM treatment and management strategies at the time of initial diagnosis. Educating the patients about disease pathogenesis, symptoms, treatment, and self-management not only plays a vital role as the initial step toward FM management but, when incorporated into the treatment plan, can also positively impact patients dealing with the condition.13,23,27,28 Self-management techniques that help with tasks of daily living and lifestyle changes can be adopted through ongoing patient education, and may prove more effective with input from the patient’s support group. In this regard, it is unfortunate to observe the extent to which patients in this survey experience isolation from their friends, family, colleagues, and HCPs. Patients in this survey believed that friends and family underestimated their condition and viewed the patients as overreacting. This lack of understanding could stem from the absence of a single set of diagnostic criteria agreed upon by HCPs, or a set of standardized and reliable objective measures of FM symptoms, and can eventually lead to social withdrawal by patients because their condition is deemed not “real” and is often considered psychosomatic.29 It is notable that the one support group that patients felt understood their condition to a greater extent than was expected/desired was other patients with FM.
A higher proportion of patients in this survey believed that rheumatologists better understood the patients’ condition as compared with other specialists or PCPs. In a previous survey of physicians, a higher proportion of rheumatologists were confident in recognizing and differentiating FM symptoms from other conditions than PCPs, pain specialists, and neurologists.11 FM is often diagnosed as a secondary disorder to primary rheumatic conditions, and this may explain rheumatologists’ familiarity with FM.18,30 The patient-centered approach toward developing a treatment plan for patients with FM is based on an effective dialog with their HCPs in order to assess the aspects of life most affected, prioritize treatment goals, and track progress.13 NPs can form an integral part of the treatment team and can not only perform FM diagnosis, but also devise an appropriate treatment regimen based on associated comorbidities and FM severity.14
It should be noted that as this was an observational study and data were collected from patients actively seeking care, as such the results might not be representative of a broader FM population. In addition, comorbid conditions experienced by patients, such as arthritis or other painful musculoskeletal conditions, could have influenced patients’ reporting of clinical outcomes in this study. As mentioned earlier, the survey did not collect information on every aspect of patients’ daily lives, eg, the impact of level of activity on their physical function.
Conclusion
The results of this survey identify key symptom domains and their impact on daily life; they also highlight a gap in the level of understanding that patients with FM expect/desire from their support group and the level of understanding patients feel they receive. HCPs should endeavor to more actively consider issues surrounding patients’ experience with FM, including the societal stigma associated with the condition that can lead to patient isolation. Ongoing communication between patients with FM and NPs, PCPs, and specialists requires an empathetic approach from the HCP and is the key to developing an effective treatment plan and improving patients’ quality of life.
Acknowledgments
This study was sponsored by Pfizer, which was involved in the design and conduct of the study. The authors would like to thank Carrie Goldstein (Pfizer, New York, NY, USA) for her assistance with data collection for this manuscript. Medical writing support was provided by Vatsala Malik, PhD, of Engage Scientific Solutions, and funded by Pfizer.
Disclosure
Andrew Clair and Elizabeth T Masters are full-time employees of Pfizer. Yvonne D’Arcy has served on Advisory Boards for Pfizer and AstraZeneca. Angela Golden reports no conflicts of interest in this work.
References
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. | |
Mease P. Fibromyalgia syndrome: review of clinical presentation, pathogenesis, outcome measures, and treatment. J Rheumatol Suppl. 2005;75:6–21. | |
Arnold LM, Crofford LJ, Mease PJ, et al. Patient perspectives on the impact of fibromyalgia. Patient Educ Couns. 2008;73(1):114–120. | |
Firestone KA, Holton KF, Mist SD, Wright CL, Jones KD. Optimizing fibromyalgia management. Nurse Pract. 2012;37(4):12–21; quiz21–12. | |
Vincent A, Lahr BD, Wolfe F, et al. Prevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology Project. Arthritis Care Res. 2013;65(5):786–792. | |
Brown TM, Garg S, Chandran AB, McNett M, Silverman SL, Hadker N. The impact of ‘best-practice’ patient care in fibromyalgia on practice economics. J Eval Clin Pract. 2012;18(4):793–798. | |
Chandran A, Schaefer C, Ryan K, Baik R, McNett M, Zlateva G. The comparative economic burden of mild, moderate, and severe fibromyalgia: results from a retrospective chart review and cross-sectional survey of working-age US adults. J Manag Care Pharm. 2012;18(6):415–426. | |
Arnold LM, Clauw DJ, McCarberg BH. Improving the recognition and diagnosis of fibromyalgia. Mayo Clin Proc. 2011;86(5):457–464. | |
Dennis NL, Larkin M, Derbyshire SW. ‘A giant mess’ – making sense of complexity in the accounts of people with fibromyalgia. Br J Health Psychol. 2013;18(4):763–781. | |
Choy E, Perrot S, Leon T, et al. A patient survey of the impact of fibromyalgia and the journey to diagnosis. BMC Health Serv Res. 2010;10:102. | |
Perrot S, Choy E, Petersel D, Ginovker A, Kramer E. Survey of physician experiences and perceptions about the diagnosis and treatment of fibromyalgia. BMC Health Serv Res. 2012;12:356. | |
Phillips K, Clauw DJ. Central pain mechanisms in chronic pain states – maybe it is all in their head. Best Pract Res Clin Rheumatol. 2011;25(2):141–154. | |
Arnold LM, Clauw DJ, Dunegan LJ, Turk DC. A framework for fibromyalgia management for primary care providers. Mayo Clin Proc. 2012;87(5):488–496. | |
Paiva ES, Jones KD. Rational treatment of fibromyalgia for a solo practitioner. Best Pract Res Clin Rheumatol. 2010;24(3):341–352. | |
Bennett R. The Fibromyalgia Impact Questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S154–S162. | |
Bennett RM, Jones J, Turk DC, Russell IJ, Matallana L. An internet survey of 2,596 people with fibromyalgia. BMC Musculoskelet Disord. 2007;8:27. | |
Asbring P, Närvänen AL. Women’s experiences of stigma in relation to chronic fatigue syndrome and fibromyalgia. Qual Health Res. 2002;12(2):148–160. | |
Clauw DJ, Arnold LM, McCarberg BH. The science of fibromyalgia. Mayo Clin Proc. 2011;86(9):907–911. | |
Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610. | |
Homma M, Ishikawa H, Kiuchi T. Association of physicians’ illness perception of fibromyalgia with frustration and resistance to accepting patients: a cross-sectional study. Clin Rheumatol. Epub 2014 Aug 3. | |
Pastor M, Roig S, Johnston M, Rafael G, Daza P. Clinical self-efficacy and illness beliefs in ambiguous chronic pain conditions: general practitioners’ management of fibromyalgia. An. Psicol. 2012;28(2):417–425. | |
Clark P, Paiva ES, Ginovker A, Salomón PA. A patient and physician survey of fibromyalgia across Latin America and Europe. BMC Musculoskelet Disord. 2013;14:188. | |
Wolfe F, Hauser W, Walitt BT, Katz RS, Rasker JJ, Russell AS. Fibromyalgia and physical trauma: the concepts we invent. J Rheumatol. 2014;41(9):1737–1745. | |
McLean SA, Switzer M, Jones CW, et al. Emergency department physiologic predictors of pain and psychological sequelae after motor vehicle collision. Paper presented at: ACR/ARHP Scientific Meeting; November 10–15, 2006; Washington, DC. | |
Han C, Lee SJ, Lee SY, et al. Available therapies and current management of fibromyalgia: focusing on pharmacological agents. Drugs Today (Barc). 2011;47(7):539–557. | |
Lawson K. Treatment options and patient perspectives in the management of fibromyalgia: future trends. Neuropsychiatr Dis Treat. 2008;4(6):1059–1071. | |
Vincent A, Whipple MO, Oh TH, Guderian JA, Barton DL, Luedtke CA. Early experience with a brief, multimodal, multidisciplinary treatment program for fibromyalgia. Pain Manag Nurs. 2013;14(4):228–235. | |
Hassett AL, Gevirtz RN. Nonpharmacologic treatment for fibromyalgia: patient education, cognitive-behavioral therapy, relaxation techniques, and complementary and alternative medicine. Rheum Dis Clin North Am. 2009;35(2):393–407. | |
Briones-Vozmediano E, Vives-Cases C, Ronda-Perez E, Gil-Gonzalez D. Patients’ and professionals’ views on managing fibromyalgia. Pain Res Manag. 2013;18(1):19–24. | |
Boomershine CS, Crofford LJ. A symptom-based approach to pharmacologic management of fibromyalgia. Nat Rev Rheumatol. 2009;5(4):191–199. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.