Back to Journals » Patient Preference and Adherence » Volume 10
“My patients are better than yours”: optimistic bias about patients’ medication adherence by European health care professionals
Authors Clyne W, McLachlan S, Mshelia C, Jones P, De Geest S, Ruppar T ![]() , Siebens K, Dobbels F, Kardas P
, Siebens K, Dobbels F, Kardas P
Received 19 March 2016
Accepted for publication 17 May 2016
Published 26 September 2016 Volume 2016:10 Pages 1937—1944
DOI https://doi.org/10.2147/PPA.S108827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Wendy Clyne,1 Sarah McLachlan,2 Comfort Mshelia,3 Peter Jones,4 Sabina De Geest,5,6 Todd Ruppar,7 Kaat Siebens,6 Fabienne Dobbels,6 Przemyslaw Kardas8
1Faculty of Health and Life Sciences, Coventry University, Coventry, 2Department of Physiotherapy, King’s College London, London, 3Leeds Institute of Health Sciences, University of Leeds, Leeds, 4Institute of Science and Technology in Medicines, Keele University, Keele, UK; 5Institute of Nursing Science, University of Basel, Basel, Switzerland; 6Academic Center for Nursing and Midwifery, KU Leuven, Leuven, Belgium; 7Sinclair School of Nursing, University of Missouri, Columbia, MO, USA; 8Department of Family Medicine, Medical University of Lodz, Lodz, Poland
Objectives: The objectives of this study were to determine the perceptions of European physicians, nurses, and pharmacists about the extent of nonadherence by patients in their country relative to their perception of nonadherence by their own patients, and to investigate the occurrence of optimistic bias about medication adherence. The study explored a key cognitive bias for prevalence and likelihood estimates in the context of health care professionals’ beliefs about patients’ use of medicines.
Methods: A cross-sectional online survey of 3,196 physicians (855), nurses (1,294), and pharmacists (1,047) in ten European countries (Austria, Belgium, England, France, Germany, Hungary, the Netherlands, Poland, Portugal, and Switzerland) was used.
Results: Participants differed in their perceptions of the prevalence of medication adherence initiation, implementation, and persistence present in their own patients with a chronic illness in comparison to patients with a chronic illness in general. Health care professionals demonstrated optimistic bias for initiation and persistence with medicine taking, perceiving their own patients to be more likely to initiate and persist with treatment than other patients, but reported significantly lower prevalence of medication adherence levels for their own patients than for patients in general. This finding is discussed in terms of motivational and cognitive factors that may foster optimistic bias by health care professionals about their patients, including heightened knowledge of, and positive beliefs about, their own professional competence and service delivery relative to care and treatment provided elsewhere.
Conclusion: Health care professionals in Europe demonstrated significant differences in their perceptions of medication adherence prevalence by their own patients in comparison to patients in general. Some evidence of optimistic bias by health care professionals about their patients’ behavior is observed. Further social cognitive theory-based research of health care professional beliefs about medication adherence is warranted to enable theory-based practitioner-focused interventions to be tested and implemented.
Keywords: medication adherence, health care professional beliefs, optimistic bias, unrealistic optimism
Introduction
Research to understand and change patient behavior, and patient medication taking behavior in particular, is often theory based, utilizing social-cognitive theories about the mechanisms that determine patient beliefs, intentions, and actions.1,2 In contrast, understanding of the factors that guide health care professional behavior in clinical practice is both less developed and less theory driven. Godin et al3 argue that the same models that have been used to understand patient beliefs and behavior can reasonably be used to understand the determinants of clinician beliefs and behaviors. An additional component to any model about factors impacting clinician behavior is clinician perceptions about patients. Several studies have explored health care professional perceptions of rates of patient medication adherence. Previous research has shown that physicians and nurses are inaccurate in their estimates of the incidence of nonadherence and their estimates are less accurate than patients’ own estimates.4,5 Health care professionals involved in the care of people with HIV overestimated patient medication adherence by an average of 9%,6 physicians overestimated adherence to osteoporosis medication relative to pharmacy data7,8 and in people prescribed medication for schizophrenia and bipolar disorder,9 and physicians have also been found to be no better than chance in predicting the adherence rates of patients in their care.10
Social cognition theories point to a number of biases in the way that people perceive the prevalence or likelihood of events. Optimistic bias refers to the way in which people tend to see themselves as less at risk and less likely to experience negative life events than others.11,12 Usually, optimistic bias is reported for self-attributes: people perceive, on average, that their own futures are going to be better than others, and that they are exposed to fewer risk factors than other people and that they have more positive personal attributes than other people.13 People rate themselves as less at risk of a host of negative experiences compared to other people like themselves.14 Optimistic bias has been found to be related to perceived social distance; the greater the social distance between the comparison target and oneself, the greater the difference in risk perception or negative life experience that is perceived between oneself and the comparison target.15–17 Self-categorization theory18 has been used to explain these differences. This posits that motivational and cognitive factors driving self and social identity may serve to credit members of an in-group with lower risk and better life experiences, like oneself, relative to members of an out-group.
This study explores whether health care professionals’ perceptions of patient medication adherence are also vulnerable to optimistic bias. We asked European health care professionals to report their perceptions of the prevalence of medication adherence and nonadherence by their patients with chronic illness and the prevalence of medication adherence by patients with chronic illness in their nation. The objectives of the study were to determine the perceptions of physicians, nurses, and pharmacists of the extent of nonadherence by people in their country relative to their perception of nonadherence by their own patients and to investigate the occurrence of optimistic bias about medication adherence.
Methods
Design
An online cross-sectional survey was used to test whether European health care professionals perceive differences in the medication adherence and nonadherence rates of their own patients with a chronic illness versus patients with a chronic illness in general in their country.
Setting and participants
Registered physicians, nurses, and pharmacists from ten European nations (Austria, Belgium, England, France, Germany, Hungary, the Netherlands, Poland, Portugal, and Switzerland) working with adults in primary care settings participated in this study.
Procedure
The survey questions described in this study were embedded in a larger survey of European health care professional beliefs and behaviors related to patient nonadherence, which is described elsewhere.19,20
The online survey was administered using SurveyMonkey.com. Ethics approval was provided by the NRES Committee North West Liverpool East (REC Reference 11/NW/0156) for England. The study and ethics protocol approved for England was used as the basis for ethics and research governance for the survey in other European countries and adapted as necessary to meet national ethical requirements. Alterations to the study protocol were only made to ensure ethical conduct in the country concerned or to align the study to local systems and processes for data collection for health care professionals. Recruitment methods were adapted as necessary in each country, depending upon the availability and accessibility of, for example, national registers of health care professionals. When available, a random sample of health care professionals was sought from national registers of health care professional bodies or associations. Where national registers were not available and accessible, open recruitment was used via professional bodies and associations. All participants indicated consent online before taking part in the survey. If any potential participants tried to access the survey without providing consent they were unable to do so.
In addition to sending out invitation letters, news articles to promote awareness of the survey were sent to health care professional bodies and associations for circulation through the respective organizations’ websites and newsletters. The news article was also distributed to publications whose main audience was health care professionals. The news article contained the same project information and granted access to the survey via the same web link.
Measures
The survey questions and the response scale were adapted from Patel and Davis.21 Three questions were posed about medication adherence regarding patients in general and health care professionals’ own patients, reflecting the definitions of medication adherence proposed by Vrijens et al22 for medication initiation, medication regimen implementation, and persistence.
The first set of questions concerned health care professionals’ perception of nonadherence in all patients: “What percentage of all patients with a chronic condition/illness in your country do you think do not initiate prescribed medication (that is, patients who do not take any of their prescribed medication)?” followed by “What percentage of all patients with a chronic condition/illness IN YOUR COUNTRY and who initiate their prescribed medication, DO take their medicines as prescribed?” and “What percentage of all patients with a chronic condition/illness IN YOUR COUNTRY and who initiate their prescribed medication, DO persist with their medication for 1 year?” These questions were then repeated but concerning perceptions of nonadherence in the participants’ own patients, for example, “What percentage of patients that you see with a chronic condition/illness, do you think do not initiate prescribed medication (that is, patients who do not take any of their prescribed medication)?” A five-point rating scale was provided for respondents to make their ratings for all six questions, with response options of 0%–15%, 16%–35%, 36%–65%, 66%–85%, and 86%–100%, as used by Patel and Davis.21 The broad term “chronic illness” was used to promote the consideration of a broad view by participants, rather than a focus on specific illnesses or conditions.
The questionnaire and the associated survey materials were translated into the official language(s) for each participating country. The workflow and quality management processes used were certified to meet ISO 9001 Quality Management Standards. Forward translations were performed by highly trained, approved, and accredited translators who were native speakers of the target languages and fluent in English. Back translations were performed by persons who were native English speakers and fluent in each target language. A third individual acted as a reviewer who highlighted any discrepancies between the forward and back translations and resolved them by discussion with the translators. The respective national coordinators and their teams of each participating country also proofread each translated document and provided feedback on grammatical errors. They also provided contextual interpretation of the translations to ensure that they reflected the appropriate terminology used in each participating country. In addition to this, the online survey was piloted by at least five people in each country in order to check its technical functionality and also to check for comprehensibility and formatting errors.
Analysis
To assess health care professionals’ optimistic bias for medication adherence, their estimates for the percentages of their own patients who do not initiate prescribed medication, do initiate their medication and implement their medication regimen, and persist with prescribed medication for 1 year were compared with their estimates for patients in general within their nation, for the same aspects of adherence. A series of nonparametric sign tests were conducted to determine whether there were significant differences between the health care professionals’ ratings for their own patients and those for patients in general, for each aspect of adherence.
To explore differences in optimistic bias between the three professional groups, a series of Kruskal–Wallis one-way analyses of variance (ANOVAs) were conducted. Initially, difference scores were computed for each aspect of adherence by subtracting each health care professional’s rating for patients in general from their rating for their own patients; both assessed on the same five-point scale. For noninitiation, negative difference scores indicated optimistic bias, while positive scores reflected the perception that noninitiation was greater in the health care professionals’ own patients than patients in general. For adherence and persistence, positive scores indicated optimistic bias. These difference scores formed the outcome variable for the ANOVAs. Pairwise comparisons using the Mann–Whitney test were then used to explore differences between groups.
Results
A total of 4,967 health care professionals started the survey. However, only those who recorded their profession were included in data analysis, resulting in a final sample of 3,196 health care professionals. Demographic information for the final sample is presented in Table 1.
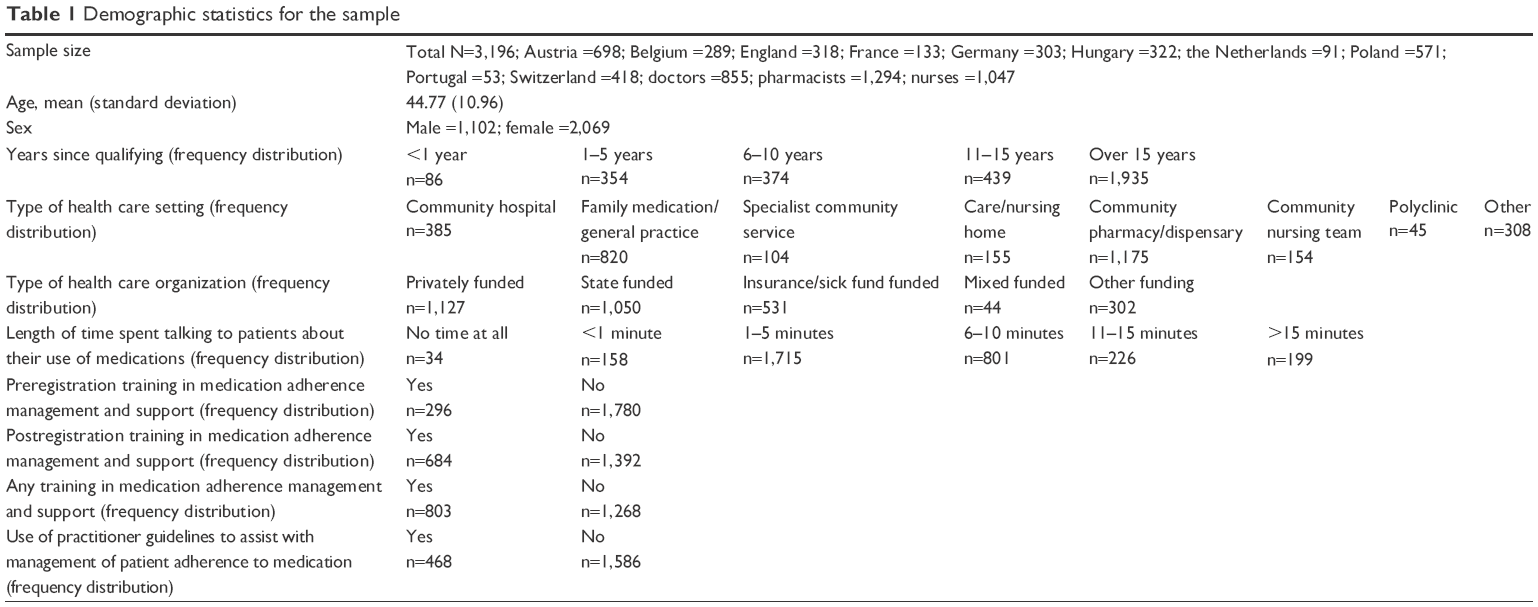 | Table 1 Demographic statistics for the sample |
The percentages for each response category for health care professionals’ own patients and patients in general are provided for the overall sample and for each profession within Table 2. For noninitiation, a nonparametric sign test showed that health care professionals’ ratings for their own patients were significantly lower than those for patients in general, P<0.001, suggesting optimistic bias for health care professionals’ perceptions of their own patients’ noninitiation. For all pairs of responses to the items on noninitiation, 788 ratings (ie, 79.6%) for health care professionals’ own patients were lower than those for patients in general, while 201 (20.3%) ratings were higher. A Wilcoxon signed rank test for the difference in median ratings for health care professionals’ own patients and patients in general confirmed that this difference was significant, P<0.001.
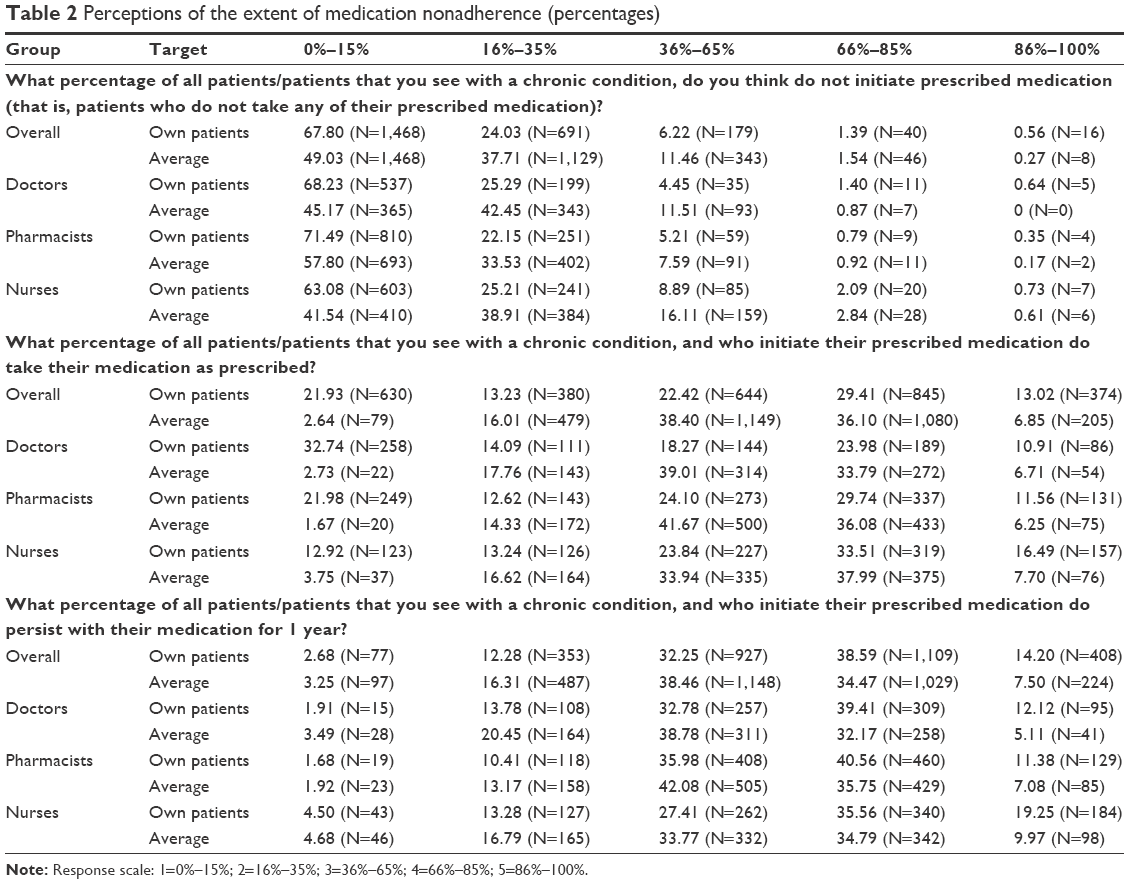 | Table 2 Perceptions of the extent of medication nonadherence (percentages) |
The sign test indicated that ratings for health care professionals’ own patients’ implementation were significantly lower than ratings for implementation by patients in their nation in general, P<0.001. Of all pairs of responses, 894 (55.1%) ratings for health care professionals’ own patients were lower than ratings for patients in general, while 788 (44.9%) were higher. A Wilcoxon signed rank test confirmed that the median rating for health care professionals’ own patients was significantly lower than that for patients in general, P<0.001.
For health care professionals’ estimates of patients’ persistence for 1 year, a sign test indicated that ratings were significantly higher for their own patients than for patients in their nation in general, P<0.001. Of all pairs of ratings, 299 (26.7%) ratings were lower for health care professionals’ own patients, relative to patients in general, while 819 (73.3%) were higher, indicating that optimistic bias is also present in health care professionals’ estimates of patients’ persistence with prescribed medication. A Wilcoxon signed rank test confirmed that the median rating for health care professionals’ own patients was significantly higher than the median rating for patients in their nation in general, P<0.001.
The ANOVA conducted for the noninitiation difference score showed a significant difference between the professional groups, P<0.001. Pairwise comparisons indicated that pharmacists reported significantly more positive difference scores, and therefore less optimistic bias, than doctors and nurses on this variable. There was no significant difference between the difference scores of doctors and nurses.
For health care professionals’ difference scores for patients’ adherence to prescribed medication, a significant difference between the professions emerged; P<0.001. Mann–Whitney tests revealed that the difference scores reported by nurses were significantly more positive than those of doctors and pharmacists, P<0.001, indicating significantly more optimistic bias from nurses. Pharmacists’ scores were also significantly more positive than those of the doctors; P<0.001. A significant difference between professions was also determined for difference scores for patients’ 1 year persistence with prescribed medication; P<0.001. In this case, doctors’ difference scores were significantly more positive than those of pharmacists, P<0.001, and nurses, P<0.05, suggesting that doctors exhibit more optimistic bias for their own patients’ persistence with prescribed medication than either pharmacists or nurses. There was no significant difference between the level of optimistic bias shown by pharmacists and nurses; P>0.05.
Discussion
Participants in this large international study differed in their perceptions of the prevalence of medication adherence initiation, implementation, and persistence in their own patients with a chronic illness in comparison to patients with a chronic illness in general. Health care professionals demonstrated optimistic bias for two of the three items, ie, initiation and persistence with medicine taking, perceiving their own patients to be more likely to initiate and persist with treatment than other patients. Conversely, participants reported significantly lower prevalence of implementation of the medication regimen after initiation for their own patients than for patients in general. Taken with previous research that suggests that clinicians may overestimate medication adherence, it seems that this overestimate may be accentuated, in some circumstances, for perceptions of their own patients rather than being an overestimate about medication adherence by people in general.
Several potential causes of optimistic bias by health care professionals about patient health behavior are plausible. Some theories suggest that optimistic bias can be a self-serving bias, supported by biases in cognitive mechanisms serving a self-enhancing self-protective function. Here, there are clear potential motivations for perceiving that one’s own patients are “better” at adhering than the general population. For health care professionals in the current study, it may be the case that self-enhancement is served by extending this cognitive bias about oneself to include perceptions about “my patients”. One’s own patients thus become an extension of perception of one’s own professional competence and thus are perceived as better than others. Further, it is possible that health care professionals seek confirmation of medication adherence from patients where they expect to find it, but do not seek out nonadherence, thus reinforcing any optimistic bias. Alternatively, differing levels of knowledge may account for different prevalence perceptions. Heightened knowledge of local services and support for patients, and a perception of their superiority, may lead health care professionals to believe their own patients are better supported by health services in the locality and they are therefore more adherent, in contrast to the abstract “other” health services available elsewhere.
There are significant but inconsistent differences between professional groups in response to the three prevalence questions. Doctors are significantly less biased in their perception of their own patients versus patients in general regarding differences in medication initiation and adherence after initiation but are most optimistically biased about persistence at 1 year. The reasons for these differences are unclear, and further research could usefully examine causes for interprofessional differences in perceptions of patterns of medication adherence.
Optimistic bias in patient and general population samples tends to be associated with reduced uptake of preventive health behaviors and has proved to be resistant to debiasing interventions.23 This would lead us to anticipate that optimistic bias in health care professionals about patients’ behavior would be associated with reduced efforts to identify and support patients with medication nonadherence. This hypothesis should be explored in future research to identify any potential relationship between health care professional optimistic bias and behavior and to inform future health care professional-oriented education, training, and interventions.
This is the first study, we are aware of, that demonstrates some evidence of optimistic bias in health care professionals about patient health behavior. However, differences in adherence prevalence by their own patients and patients in general were not all consistent and this first exploration should be repeated and explored in other countries to determine whether these optimistic bias findings may be culturally linked. Future studies might also usefully examine the occurrence of optimistic bias about patient medication adherence for specific long-term conditions and explore any potential association with variation in the prevalence of medication nonadherence at medication and long-term condition levels.
Progress with theory-driven exploration of health care professional beliefs and behaviors about medication adherence falls significantly short of theory-driven exploration of patient adherence behavior. This study demonstrates that investigation of health care professional behavior with theory-based approaches is a valid and relevant approach to understanding medication adherence.
Conclusion
Health care professionals in this international study demonstrated significant differences in their perceptions of medication adherence prevalence by their own patients in comparison to patients in general. Some evidence of optimistic bias by health care professionals about their patients’ behavior is observed. Further social cognitive theory-based research of health care professional beliefs about medication adherence is warranted to enable theory-based practitioner-focused interventions to be tested and implemented to ensure an optimal response from health services in supporting patients appropriately with medicine use.
Acknowledgments
We would like to thank all survey partners for their assistance with data collection across Europe. Austria: Lorenz Auer-Hackenberg, Department of Medicine I, Division of Infectious Diseases and Tropical Medicine, Medical University of Vienna; Univ Lekt Dr Heimo Lagler, Division of Infectious Diseases and Tropical Medicine, Department of Medicine I, Medical University of Vienna; Associate Professor Dr Michael Ramharter, Division of Infectious Diseases and Tropical Medicine, Department of Medicine I, Medical University of Vienna. Belgium: Professor Doctor Veerle Foulon, Faculty of Pharmaceutical Sciences, KU Leuven. France: Fabrice Baton, Kappa Santé; Charlotte Drochon, Kappa Santé; Nathalie Texier, Kappa Santé; Doctor Eric Van Ganse, University of Lyon. Germany: Sabine Breiholz, Drug Commission of German Pharmacists (AMK); Doctor Lilian Krist, Institute for Social Medicine, Epidemiology and Health Economics, Charité University Medical Centre, Berlin; PD Doctor Falk Müller-Riemenschneider, Institute for Social Medicine, Epidemiology and Health Economics, Charité University Medical Centre, Berlin. Hungary: Doctor Balogh Zoltán, President, Hungarian Chamber of Health Professionals; Berend, Dóra, Health Marketing Research Centre, Marketing and Media Institute, Corvinus University, Budapest; Doctor Horváth Tamás, President, Hungarian Chamber of Pharmacists; Doctor Éger István, President, Hungarian Medical Chamber; Doctor Simon Judit, Health Marketing Research Centre, Marketing and Media Institute, Corvinus University, Budapest. The Netherlands: Jan Hermsen, Netherlands Institute for Health Services Research, Utrecht; Doctor Liset van Dijk, Netherlands Institute for Health Services Research, Utrecht. Portugal: Doctor Luis Caldeira, National Authority of Medicines and Health Products (INFARMED), Lisbon; Frederico Saraiva, National Authority of Medicines and Health Products (INFARMED), Lisbon. Switzerland: Professor Doctor Kurt E Hersberger, Department of Pharmaceutical Sciences, University of Basel; Doctor Marie P Schneider, Department of Pharmacy, Policlinique Médicale Universitaire, Lausanne; Esther Spinatsch, Department of Pharmaceutical Sciences, University of Basel; PD Doctor Andreas Zeller, Institute for General Internal Medicine, University of Basel. This study, as part of the ABC project, was funded by the European Commission Seventh Framework programme (FP7 Theme Health, 2007-3.1-5, grant agreement number 223477). The final project report is available at http://abcproject.eu/img/ABC%20Final.pdf.
Author contributions
WC was the principal investigator of the study. WC, CM, SM, SDG, TR, KS, FD, and PK designed the study. PJ analyzed the data. WC, PJ, and SM interpreted the data. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Conn V, Enriquez M, Ruppar T, Chan K. Meta-analyses of theory use in medication adherence intervention studies. Am J Health Behav. 2016;40(2):155–171. | ||
Morrison VL, Holmes EA, Parveen S, et al. Predictors of self-reported adherence to antihypertensive medicines: a multinational, cross-sectional survey. Value Health. 2015;18(2):206–216. | ||
Godin G, Belanger-Gavel A, Eccles M, Grimshaw J. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implement Sci. 2008;3:36. | ||
Macintyre CR, Goebel K, Brown GV. Patient knows best: blinded assessment of nonadherence with antituberculous therapy by physicians, nurses, and patients compared with urine drug levels. Prev Med. 2005;40:41–45. | ||
Kardas P, Lewek P, Strzondała M. Adherence to treatment in asthma and COPD patients in their doctors’ assessment. Pneumonol Alergol Pol. 2015;83(6):436–444. | ||
Miller LG, Liu H, Hays RD, et al. How well do clinicians estimate patients’ adherence to combination antiretroviral therapy? J Gen Intern Med. 2002;17(1):1–11. | ||
Curtis JR, Cai Q, Wade SW, et al. Osteoporosis medication adherence: physician perceptions vs patients’ utilization. Bone. 2013;55(1):1–6. | ||
Copher R, Buzinec P, Zarotsky V, Kazis L, Iqbal SU, Macarios D. Physician perception of patient adherence compared to patient adherence of osteoporosis medications from pharmacy claims. Curr Med Res Opin. 2010;26(4):777–785. | ||
Stephenson JJ, Tunceli O, Gu T. Adherence to oral second-generation antipsychotic medications in patients with schizophrenia and bipolar disorder: physicians’ perceptions of adherence vs pharmacy claims. Int J Clin Pract. 2012;66(6):565–573. | ||
Stephenson BJ, Rowe BH, Haynes B, Macharia WM, Leon G. Is this patient taking the treatment as prescribed? JAMA. 1993;269(21):2779–2781. | ||
Weinstein ND. Unrealistic optimism about future life events. J Pers Soc Psychol. 1980;39:806–820. | ||
Weinstein ND. Unrealistic optimism: about susceptibility in health problems: conclusions from a community-wide sample. J Behav Med. 1987;10(5):481–500. | ||
Weinstein ND, Klein WM. Unrealistic optimism: present and future. J Soc Clin Psychol. 1996;15(1):1–8. | ||
Shepperd JA, Waters E, Weinstein ND, Klein WM. A primer on unrealistic optimism. Curr Dir Psychol Sci. 2015;24(3):232–237. | ||
Perloff LS, Fetzer BK. Self-other judgments and perceived vulnerability to victimization. J Pers Soc Psychol. 1986;50(3):502–510. | ||
Harris PR, Middleton W, Joiner R. The typical student as an in-group member: eliminating optimistic bias by reducing social distance. Eur J Soc Psychol. 2000;30(2):235–253. | ||
Helweg-Larson M, Shepperd JA. Do moderators of the optimistic bias affect personal or target risk estimates? A review of the literature. Pers Soc Psychol Rev. 2001;5(1):74–95. | ||
Turner JC, Hogg MA, Oakes PJ, Reicher SD, Wetherell MS. Rediscovering the social group: a self-categorization theory. In: Contemp Sociol. 94(6). Blackwell, London; 1987. | ||
Clyne W, Mshelia C, Hall S, et al. Management of patient adherence to medications: protocol for an online survey of doctors, pharmacists and nurses in Europe. BMJ Open. 2011;1:e000355. | ||
Clyne W, Mshelia C, McLachlan S, et al. A multinational cross-sectional survey of the management of patient medication adherence by European healthcare professionals. BMJ Open. 2016;6(2):e009610. | ||
Patel UD, Davis MM. Physicians’ attitudes and practices regarding adherence to medical regimens by patients with chronic illness. Clin Pediatr. 2006;45:439–445. | ||
Vrijens B, De Geest S, Hughes DA, et al; ABC Project Team. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. | ||
Weinstein ND, Klein WM. Resistance of personal risk perceptions to debiasing interventions. In: Gilovich T, Griffin D, Kahneman D, editors. Heuristics and Biases: The Psychology of Intuitive Judgment. New York: Cambridge University Press; 2002:313–323. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.