Back to Journals » Patient Preference and Adherence » Volume 13
Investigation of medication adherence and reasons for poor adherence in patients on long-term glaucoma treatment regimes
Authors McClelland JF ![]() , Bodle L, Little JA
, Bodle L, Little JA ![]()
Received 6 June 2018
Accepted for publication 1 December 2018
Published 12 August 2019 Volume 2019:13 Pages 431—439
DOI https://doi.org/10.2147/PPA.S176412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Julie F McClelland,1 Lynne Bodle,1,2 Julie-Anne Little1
1Vision Science Research Group, Biomedical Sciences Research Institute, Ulster University, Coleraine, UK; 2Department of Ophthalmology, Flinders Medical Centre, Flinders University, Adelaide, SA, Australia
Purpose: Long-term treatment adherence for a chronic asymptomatic condition is a demanding task for many patients. Treating progressive glaucoma can also be confounding for physicians, particularly when management relies on assumption of adherence. This study investigated associations between self-reported adherence and frequency of medication changes due to glaucoma progression.
Methods: A total of 128 participants with primary open angle glaucoma were recruited from glaucoma clinics in Flinders Eye Center, South Australia, and completed confidential questionnaires. Information was obtained regarding beliefs about glaucoma and their treatment. Adherence was assessed using the four-item Morisky, Green and Levine Medication Adherence Questionnaire (MGL). Medical records were analyzed for the number of medication changes, due to glaucoma progression.
Results: Adherence to topical glaucoma medication was categorized as ‘high’ in 41.4% (Morisky, Green and Levine (MGL). Data were analyzed for behaviors affecting adherence, history of adherence, and reasons for changed adherence. Chi-squared test demonstrated that there was no significant association noted between adherence and changes in medication regime (χ2 (2,128)=0.968, P=0.915); however, a significantly lower adherence was detected if participants had difficulties with their drop regime (χ2 (2,128)=7.24, P=0.027) or had help with drop insertion (χ2 (1,128)=9.77, P=0.008).
Conclusion: This study revealed a higher rate of non-adherence than has previously been demonstrated in other studies. This may be attributed to the unique design of the confidential questionnaire and the independent and sympathetic questioning techniques used. Further work to develop a specific glaucoma medication adherence questionnaire would be valuable to enhance glaucoma management.
Keywords: glaucoma, compliance, adherence, topical medication, questionnaire
Plain language summary
Glaucoma detection and management is a significant chronic health care burden. In order to ensure value from any treatment provided for individuals with glaucoma, it is important that we evaluate patients’ adherence to prescribed medication and discuss how to optimize the information received in a meaningful way. This study makes a valuable contribution to the literature by demonstrating significant levels of non-adherence with medication in a large population of people with glaucoma. It also reveals that effective adherence monitoring should be independent from the treating medics and that adherence monitoring should be a vital part of glaucoma management. Consideration of these factors should be incorporated into glaucoma patient treatment regimes.
Introduction
The WHO categorizes glaucoma as the second leading cause of preventable blindness, with primary open-angle glaucoma (POAG) accounting for the largest proportion.1 Glaucoma prevalence is estimated to be 3% for people over 40 years, increasing to 10% for people over 70 years.2 Glaucoma care costs are currently estimated at $2.9 billion (US) and $144.2 million (Australia),2 and this is likely to increase as the population ages in developed countries. As glaucoma care costs increase with disease severity,3 preventing progression is imperative to limit cost escalation.
Topical hypotensive therapy is the primary treatment option, the aim of which is to reduce intra-ocular pressure (IOP) to a “target” level. This “target” level varies depending on diagnosis and disease severity, but is aimed at preventing further glaucomatous damage.4
Presently, there is no firm evidence to substantiate that non-adherence to topical medication results in progression.5 This is largely due to the difficulties in measuring non-adherence in glaucoma patients. It is well known that the treating physicians’ ability to judge adherence is poor.6–9 Several methods have been utilized in efforts to assess adherence in patients, which have resulted in non-adherence figures for topical glaucoma medication varying from 12% to 60%.10–20
Several studies have utilized electronic dosing aids to measure adherence to topical medication. These dosing aids are embedded with an electronic chip that records the time and date the drop container is opened and closed. Cate et al11 compared an electronic adherence monitor with self-reported adherence in a trial involving 208 participants. They found that patients significantly overestimated their adherence compared to the electronic monitoring measurement. Chang et al10 used a two-phase study to develop a predictive model for non-adherence (n=122). They first used an electronic monitor to measure adherence over a 3-month period; the second phase then used the same drop monitor and an alert system in an attempt to improve adherence. They found that black ethnicity, a lower self-reported adherence rate, and a shorter duration of glaucoma treatment were all positive indicators of non-adherence. The Travatan Dosing Aid study (n=196)7 reported electronic dosing aid median adherence to be 71%, notably lower than self-reported adherence (95%). Adherence, which was assessed from 3 weeks after the initial visit to 2 weeks before the follow-up visit, was defined as patients taking 75% of the prescribed daily dose.7
Electronic dosing aids, although considered to be the gold standard of adherence measures, have their limitations. They are expensive, can only be used over short periods, are only available for certain medications, and as patients are aware of monitoring, could result in increased adherence compared to “typical” behavior. They also assume that evidence of recorded doses is evidence of instillation. Additionally, many of the studies using electronic dosing aids only include participants on monotherapy (one type of drop), which has been shown to have better adherence than those prescribed additional medication.21,22 Furthermore, Okeke et al7 reported a marked increase in adherence just before clinic appointments. They also found that treating doctors were unable to distinguish patients that were deemed adherent with using their eyedrops (95% used) from those that were deemed non-adherent (20% used). These highlight the difficulties treating physicians face with managing progressive glaucoma, especially when patients demonstrate good IOP control.
Numerous studies have attempted to judge adherence by looking at prescription refills and pharmacy records. Medication possession ratio (MPR) is the amount of medication a patient has (days’ supply) divided by the time (number of days) between prescription refills. Insufficient medication over a period results in an MPR <1. The Glaucoma Adherence and Persistence Study (GAPS)23 is the largest retrospective study to measure adherence. Pharmacy claims were analyzed for 13,977 subjects, and a mean MPR of 0.64 was reported, over a follow-up period of 22 months. However, the main limitation of using MPR to determine adherence is that possession of medication is not evidence of instillation. Also, if repeated prescriptions are given with other medications, then patients may be “stockpiling” rather than being adherent.
Questionnaires have been used extensively to investigate self-reported non-adherence to medicines.11,12,14,23–27 Understanding the reasons behind non-adherence, and addressing these issues, could be invaluable in improving future adherence. However, since there is no available standardized, validated questionnaire, specifically designed to assess adherence to topical medication, comparison between studies is difficult. In addition, physicians involved in glaucoma care often conduct these questionnaires, and patients are less likely to admit to non-adherence in this situation.8 This study investigated self-reported adherence in POAG by a researcher independent of the care team. Uniquely, this study also assessed the effect that changes in medication regimes have on adherence.
Methods
This study received ethical approval from Ulster University Biomedical Sciences Ethics Filter Committee and South Australia Health Human Research Ethics Committee. All participants gave written informed consent prior to involvement in the study.
Consecutive patients with POAG were recruited from specialist glaucoma clinics within Flinders Eye Center (South Australia) from May 2013 to May 2014. Eligible participants had a confirmed diagnosis of POAG and had been using topical glaucoma medication for at least 3 years. Participants were excluded if they had undergone previous glaucoma surgery, were using topical medication for any other eye condition, were over 85 years old, or unable to read English. Participants were given a full explanation of the study and written informed consent was obtained.
Participants were escorted to a quiet room to complete the questionnaire in private. Once given the questionnaire, it was reiterated that all responses were completely anonymous and that their treating physician would have no access to any information given to the researcher.
Participant records were later examined once the patient had left the clinic and the numbers of medication changes were recorded. Medication changes were only included if the reason for change was due to evidence of progression (ie, from IOP measurements, visual fields progression, or Optical Coherence Tomography [OCT] analysis). They were not included if the rationale for change was due to side effects of eye drops or problems with administration.
Questionnaire
To explore medication adherence in POAG, a customized questionnaire was developed, which included questions adapted from the Morisky, Green and Levine Medication Adherence Questionnaire (MGL)28 and was based on analysis of existing studies and questionnaire design specific to POAG. The MGL is an extensively used questionnaire which has been validated for use with oral hypertensive medications and patients with Type 2 diabetes.28,29,30 Questions from the MGL were used in the present study, comprising four questions with an option of a yes/no response. A “yes” was given a score of 0 and a “no” 1. Therefore, total scores varied between 0-4. The adherence scores were calculated, and participants were categorized as: MGL=0-1 representing low adherence, MGL=2-3 representing moderate adherence and MGL=4 representing high adherence. Other questions included in the questionnaire assessed patients’ knowledge and beliefs about glaucoma, necessity of medication, and the trust they had in their doctor and their treatment, as well as factors that can predict non-adherence, based on previous reports of glaucoma medication adherence.10–12,14,23,25,31,32 Questions also assessed patients’ use of eye drops, and their routine and insertion techniques.
An independent researcher, a qualified optometrist not involved with the participants’ treatment regime, administered the questionnaire. Participants were allowed an open dialogue and encouraged to volunteer as much information as possible to make them feel more comfortable in admitting non-adherence. Any participants who had specific concerns that could not be answered by the researcher were encouraged to discuss these with their glaucoma physician.
Data were entered into SPSS version 21.0 and demographic and adherence behaviors were compiled. Analysis of the medication change data found a non-normal distribution, and median values were therefore reported. Medication changes were therefore grouped into three categories: group 1 (0 changes), group 2 (1 change), and group 3 (2–4 changes). Non-parametric chi-squared analyses were employed to assess adherence and behaviors.
Results
Of the 138 participants recruited, ten were excluded for the following reasons: four participants had previous trabeculectomies, three had been on topical medication for less than 3 years, one had experienced angle closure, and two had their drops inserted by a carer in a nursing home.
Almost half of the participants were male (47.7%) and the median age was 72.5 years (SD ±9.86). A large proportion (71.1%) of participants had a family history of glaucoma. The majority of participants in the study lived with family (75.8%). A large proportion of the sample (87.5%) was taking other chronic medications in addition to their glaucoma eye drops. The median time since diagnosis of POAG was 9 years (SD ±5.89).
Adherence
For the remaining 128 participants, complete adherence to topical medication was found in 41.4% (MGL=4). ‘Moderate adherence’ was demonstrated by 69 participants (53.9%) and ‘low adherence’ by six participants (4.7%). The reasons cited for non-adherence that participants mentioned more than once are included in Table 1.
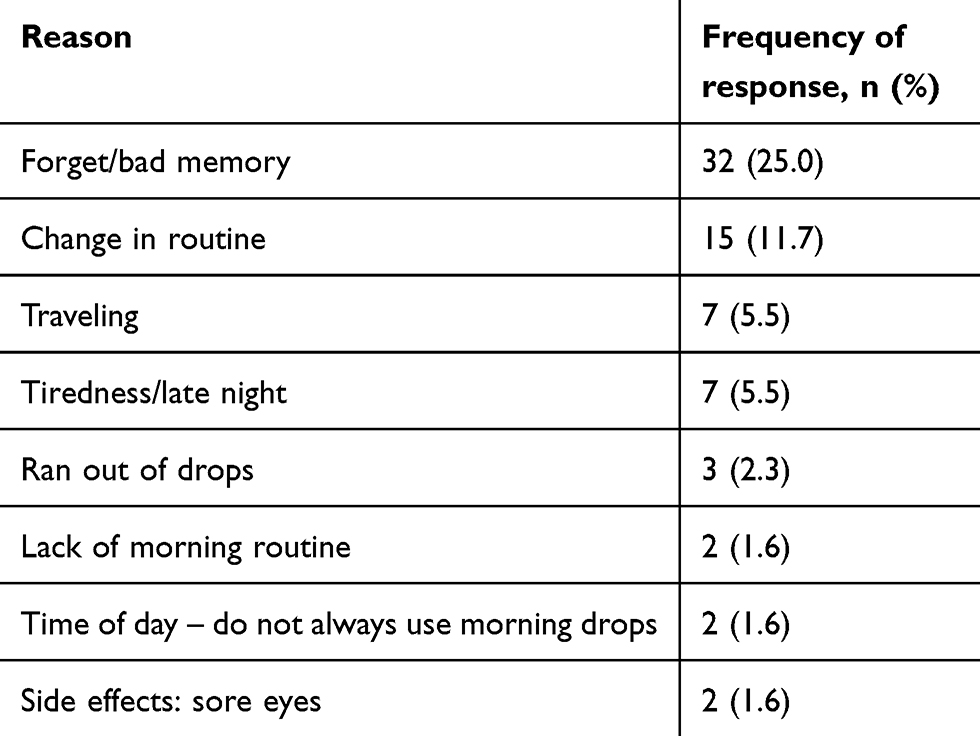 |
Table 1 Participants’ reasons for not using eyedrops |
Demographics and adherence
Table 2 summarizes the difference in participants categorised as having low, moderate or high adherence to their medication. Older participants (over 70 years of age) were more likely to demonstrate low adherence compared with the younger individuals (χ2 (4,128)=10.62, P=0.031). None of the parameters reached statistical significance (chi-squared, P>0.05) (Table 2).
 |
Table 2 Demographics compared with adherence rating with the MGL medication adherence questionnaire |
History of adherence
The majority of participants (n=107, 83.6%) reported no change in adherence behavior over the previous 6 months. A chi-squared test demonstrated that participants who reported no change in adherence behavior were more likely to be in the ‘high adherence’ group (χ2 (4,128)=15.89, P=0.03). Of the remaining 21 participants, 12 reported that they used their medication more regularly over the previous 6 months, and nine less regularly. Table 3 summarizes the reasons given for changes in adherence.
 |
Table 3 Reasons for changes in adherence behavior over the previous 6 months |
Knowledge of disease/patient perception
Less than half the participants (47.7%) felt they knew “a lot/fair amount” about their glaucoma condition (Table 4).
 |
Table 4 Knowledge of disease perception and adherence |
A chi-squared test demonstrated no significant associations between adherence and participants’ perception of their knowledge of glaucoma when glaucoma knowledge was categorized as knowing a ‘lot’, ‘a fair amount’, ‘very little’ or ‘none’, χ2 (6,128)=2.56, P=0.862 (Table 4). Also, no significant associations were noted between participants ‘knowledge of glaucoma if left untreated’ and adherence (χ2 (2,128)=3.84, P=0.146). Half of participants (50%) reported they didn’t know or were unsure how the drops for glaucoma worked, χ2 (2, 128)=7.89, P=0.096.
Less than a half (44.5%) of participants knew what would happen if glaucoma was not treated.
Treatment of glaucoma
A large proportion of patients (66.4%) were very happy with their treatment of glaucoma, the remainder were mostly happy (29.7%), and a very small proportion (3.9%) unhappy. Chi-squared test revealed that participants reporting that they were “happy” with their treatment were more likely to be adherent with their treatment, however this did not reach statistical significance, χ2 (2,128)=8.41, P=0.078) (Table 5). When asked if they thought their eye drops were working, half (50%) thought that their eye drops were working, almost half (46.1%) replied that they were not sure, and the remainder (3.9%) responded “no”.
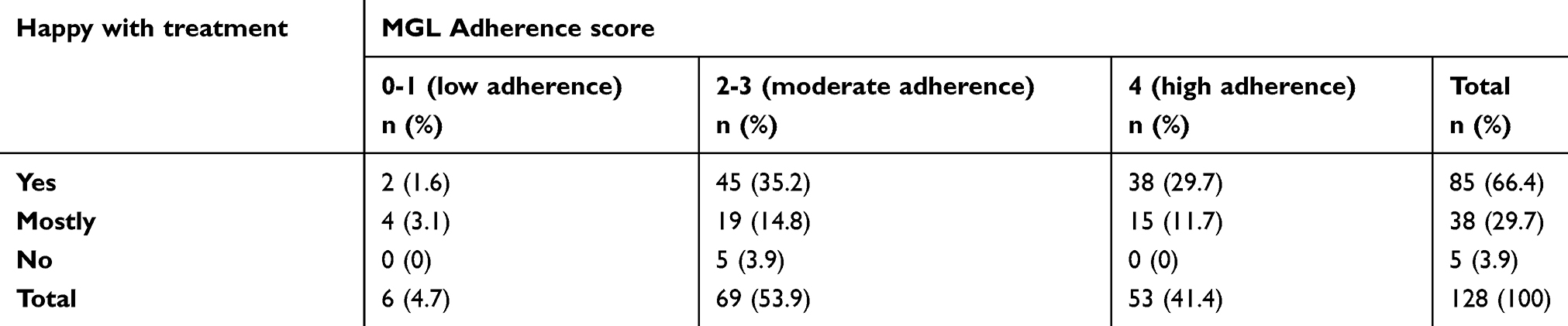 |
Table 5 Participants’ perception of whether they were “happy” with their treatment |
Use of eye drops
Most participants (89.1%) reported that they were confident with their eye drop regime. The majority of participants used their drops either once daily (54.7%) or twice daily (39.1%), and 6.3% used them more than three times daily. Similarly, most participants used either one (60.9%) or two types of drops (33.6%), with 5.5% of participants using three types of drops. Chi-squared test illustrated no significant associations between the frequency of drop regime and adherence (χ2 (3, n=128)=2.47.46, P=0.872). The majority of participants (82.8%) did not find their drop regime “hard to follow”. Chi-squared analysis indicated that participants with no difficulties following with their drop regime had significantly higher adherence than those who reported difficulties, (χ2 (2,128)=7.24, P=0.027) (Table 6). Eye drops stinging on insertion was reported as “always” by 13.3% of participants and “sometimes” by 32.0%. Side effects using drops was reported by 24.2% of participants: the most common side effect reported was red eyes (14.1%). There was no association found between participants that reported “drops stung on insertion” and their adherence (χ2 (4,128)=1.24 P=0.871).
The majority of participants reported that they were “always” confident inserting their drops (73.4%), with 15.6% reporting confidence with drop insertion “most of the time”, 6.3% “occasionally”, and 4.7% “never”. Chi-squared test revealed that over half the participants (52.3%) had help with drop insertion at home if they required it, and were more likely to be in the low-adherence group (χ2 (1,128]=9.77, P=0.008). Just over a third (37.5%) could recall being shown how to instill eye drops properly or “could not remember” (39.9%), and the remainder (22.7%) reported they had “never” been shown how to instill drops properly. A large proportion (85.2%) of participants had never asked for advice on drop instillation.
 |
Table 6 Participants’ perception of whether their glaucoma medication regime was difficult to follow |
Discussion
It has previously been reported that physicians are not well placed to accurately judge medication adherence6,7,9 and that patients are unlikely to admit to non-adherence within a clinic environment.8 Self-reported adherence is conventionally disclosed as higher than other measures of adherence, since social desirability compels patients to overestimate adherence.
Interestingly, the adherence rate (41.4%) in this study is one of the lowest reported rates using a questionnaire-based study. Rees et al12 and Cate et al11 used the same medication adherence and found a self-reported adherence of 61.7% (n=107) and 87.8% (n=82), respectively; however, both the studies were conducted in a clinical environment. The present study demonstrates that segregating participants from the clinic environment encourages non-adherence disclosure.
While the MGL questions allowed a quick and easy validated measure of adherence, its weakness is the inability to measure the degree of non-adherence. 58.6% of participants scored either a ‘low adherence’ or ‘moderate adherence’ score (MGL 0-3), with a significant proportion in the ‘moderate adherence’ group. These two groups were not quantified in terms of the number of times or regularity with which they missed doses. The ‘moderately-adherent’ patients could be classed as non-intentional, ie, they simply forgot, whereas the group of low adherence patients (scoring 0-1 on the MGL [4.7% of total]) could indicate more intentional non-adherence behaviors (eg, lack of faith in treatment). These two differing patterns of behaviors need altered approaches to management. Addressing the most commonly reported reasons for non-adherence (eg, forgetting) may simply require patient counseling on the importance of drops, effects of missed drops, and ways to improve future adherence. Patients that are intentionally non-adherent may need a more diverse approach.
No significant associations between adherence and the number of changes in medication regime were found in this study. There was a greater percentage of participants having zero changes in medication’ in the ‘high adherence’ group, however, only 21% of participants overall had two or more glaucoma medication changes, thus limiting the conclusions one can draw from this finding.
Of those found to have increased adherence over the previous 6 months, reasons included better instillation techniques, simpler medication regimes, and greater understanding of the disease. Reasons for decreased adherence were a result of drop insertion difficulties and an increase in drop frequency. Participants reported that they are often hesitant to ask for help within a busy clinic environment, particularly if they have been using drops for long term and feel embarrassed or unwilling to admit that they require help with something they should be adept at. When asked if they had ever asked for help with drop instillation, 85.2% said no, and yet comments such as “always put in a couple of times because of poor aim” and “trouble with aim” show a need for intervention. Assistance could be a productive addition to clinics, with patients given the opportunity to ask questions and receive help for difficulties with topical medication.
The present study revealed that there was a larger percentage of participants with the least knowledge of “how their drops worked” and the least knowledge of “what would happen if glaucoma was not treated”, in the 'low adherence' group, however this did not reach statistical significance. This is consistent with previous published literature,23 which reported that doctor–patient relationships are one of the most important factors for adherence to topical medication. Friedmann et al23 reported that understanding how glaucoma affected vision increased adherence and not knowing how drops worked decreased adherence. Of the 57 participants (44.5%) that could articulate what happens if POAG is not treated, only one person mentioned that the disease was asymptomatic. This aspect is important when addressing adherence, particularly in the group of “intentional non-compliers” who responded with comments including: “Feel like eyes need a rest from drops” and “Do not bother with morning dose”, highlighting a lack of knowledge of the consequences of non-adherence.
Another notable finding was when asked about whether they “think their eye drops are working”; almost half (46.1%) of the participants “were not sure”. This suggests that patients are using drops without any knowledge of whether they are effectively controlling glaucoma progression. Feedback during appointments, such as a written record of their IOP or results of visual field tests, could be a straightforward yet beneficial way of encouraging adherence, demonstrating effectiveness of topical medication. Comments given regarding glaucoma knowledge such as “Would be nice to know what’s happening”, “More information would help me manage my condition” demonstrates a desire for further communication regarding the disease. However, over half of the participants (54.7%) also answered “no” to wanting more knowledge, with a large proportion remarking they “know enough” or they “trust the doctor”. One participant with excellent adherence and good knowledge of glaucoma stated at the end of the questionnaire “I do not think I have glaucoma though, but I use the drops because that’s what the doctor tells me”.
In the present study, those participants who found their drop regime “hard to follow” had significantly lower adherence, and the group with “no difficulties” demonstrated statistically significant higher adherence. Previous research has reported higher adherence rates with a simpler dosing regime and that a single daily dose results in improved adherence.19,35,35 However, although in the present study there were a greater proportion of participants using one drop daily in the adherent group, no significant associations were noted between adherence and drop frequency. This may have been the result of small numbers recruited in these groups.
Surprisingly, there was a significantly larger proportion of participants who had help with drops at home in the the ‘low adherence’ group. A possible reason for this non-adherence may be a reliance on others to administer drops and consequently involving a third party for whom the importance of the medication may be eclipsed by other priorities.
The comments section of the questionnaire allowed participants to discuss any aspect of the clinic, their treatment, and glaucoma. Although some aspects of the discussion were outside the control of their glaucoma management (eg, parking), there were some insightful discussions. One younger participant suggested, “Counseling should be available for newly diagnosed patients, especially if they are younger”. This is a perceptive comment as there is evidence to show that adherence with glaucoma treatment is lower in the first year of diagnosis35 and counseling to help with the initial distress of diagnosis may help patients persevere with their treatment. Adherence has also been shown to be lower in the younger age groups, often due to a busy lifestyle and work commitments.14 The present study found that 77.8% of the youngest age group were within the ‘low/moderate adherence’. This reinforces the need to educate patients on controlling glaucoma at a young age and soon after initial diagnosis, hopefully preventing progression to visual impairment.
Addressing non-adherence requires a multifaceted approach, dependent on the patients’ needs, attitudes, and lifestyle. A Cochrane review on interventions to improve adherence to topical hypotensive therapy35 reported that individualized patient education and care resulted in improvements in adherence. Strategies to address adherence depend on the reasons behind individual non-adherence. The most common reason for non-adherence, “forgetting”, may benefit from education on the benefits of reminder techniques and establishing strategies to coordinate drop use with daily events. Adherence can also be improved by using the simplest treatment regime available. The use of once-daily dosing or fixed combination drugs are advised for those who require changes to their medication regime. Despite conflicting comments on the necessity of glaucoma knowledge by participants in this study, provisions should be made available to those who need it. When participants were asked whether they would like more knowledge about glaucoma and its treatment, 45.3% replied that they would. Several patients mentioned that they would like more knowledge, if not for themselves, for their children so they could advise them about future testing. Many also asked about the possibility of genetic testing for family members. This education, for it to be individualized, needs to be in a form other than patient leaflets. Lacey et al27 found that most patients were dissatisfied with this type of education and prefer alternative formats.
Conclusion
Identifying non-adherent patients and addressing their reasons for not using topical medication consistently are essential at an early stage to prevent progression. Those patients who use drops just before clinic appointments but not consistently in-between appointments may explain why patients progress when they present with IOP in their target range. The use of eye drop monitors is expensive, and monitors are only available for certain medications and therefore are not a viable long-term option. This study has shown the value of administration of a adherence assessment questionnaire by someone independent of the eye care team. A simple validated questionnaire that could be completed by patients on arrival at an outpatient’s appointment would allow these “personal” factors of non-adherent to be addressed before a patient leaves the clinic. This would be beneficial not only for glaucoma patients but also for other ophthalmic patients on long-term topical medication.
Acknowledgments
The authors would like to thank Prof D Morisky for use of his MGL Medication Adherence Questionnaire and help in the preparation of this manuscript. The authors would also like to thank Prof J Craig, Director of the Flinders Centre for Ophthalmology, Eye and Vision Research, Flinders University College of Medicine and Public Health for his support of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267.
2. Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011;152(4):515–522.
3. Lee PP, Walt JW, Rosenblatt LC, Siegartel LR, Stern LS; Glaucoma Care Study Group. Association between intraocular pressure variation and glaucoma progression: data from a United States chart review. Am J Ophthalmol. 2007;144(6):901–907.
4. NICE. Glaucoma: Diagnosis and Management of Chronic Open Angle Glaucoma and Ocular Hypertension. National Collaborating Centre for Acute Care. London, UK: National Institute for Health and Clinical Excellence; 2009.
5. Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Nonadherence with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112(6):953–961.
6. Kass MA, Meltzer DW, Gordon M, Cooper D, Goldberg J. Compliance with topical pilocarpine treatment. Am J Ophthalmol. 1986;101(5):515–523.
7. Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the Travatan dosing aid study. Ophthalmology. 2009;116(2):191–199.
8. Budenz DL. A clinician’s guide to the assessment and management of nonadherence in glaucoma. Ophthalmology. 2009;116(11):S43–S47.
9. Hahn SR. Patient-centered communication to assess and enhance patient adherence to glaucoma medication. Ophthalmology. 2009;116(11):S37–S42.
10. Chang DS, Friedman DS, Frazier T, Plyler R, Boland MV. Development and validation of a predictive model for nonadherence with once-daily glaucoma medications. Ophthalmology. 2013;120(7):1396–1402.
11. Cate H, Bhattacharya D, Clark A, Holland R, Broadway DC. Patterns of adherence behaviour for patients with glaucoma. Eye. 2013;27(4):545–553.
12. Rees G, Chong XL, Cheung CY. Beliefs and adherence to glaucoma treatment: a comparison of patients from diverse cultures. J Glaucoma. 2013;23:293–298.
13. Lu VH, Goldberg I, Lu CY. Use of glaucoma medications: state of the science and directions for observational research. Am J Ophthalmol. 2010;150(4):569–574.
14. Rees G, Leong O, Crowston JG, Lamoureux EL. Intentional and unintentional nonadherence to ocular hypotensive treatment in patients with glaucoma. Ophthalmology. 2010;117(5):903–908.
15. Morley AM, Murdoch I. The future of glaucoma clinics. Br J Ophthalmol. 2006;90(5):640–645.
16. Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009;116(11):S30–S36.
17. Schwartz GF. Compliance and persistency in glaucoma follow-up treatment. Curr Opin Ophthalmol. 2005;16(2):114–121.
18. Newman-Casey PA, Killeen OJ, Renner M, Robin AL, Lee P, Heisler M. Access to and experiences with e-health technology among glaucoma patients and their relationship with medication adherence. Telemed J E Health. 2018;24(12).
19. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmo. 2015;122(7):1308–1316.
20. Thompson AC, Woolson S, Olsen MK, Danus S, Bosworth HB, Muir KW. Relationship between electronically measured medication adherence and vision-related quality of life in a cohort of patients with open-angle glaucoma. BMJ Open Ophthalmol. 2018;3(1):e000114.
21. Buller AJ, Morgan LH, Hercules BL. Patients prefer once-daily glaucoma drops. Graefe’s Arch Clin Exp Ophthalmol. 2007;245(2):293–294.
22. Saini SD, Schoenfeld P, Kaulback K, Dubinsky MC. Effect of medication dosing frequency on adherence in chronic diseases. Am J Manag Care. 2009;15(6):e22–e33.
23. Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the glaucoma adherence and persistency study. Ophthalmology. 2008;115(8):1320–1327.
24. Mansouri K, Iliev ME, Rohrer K, Shaarawy T. Compliance and knowledge about glaucoma in patients at tertiary glaucoma units. Int Ophthalmol. 2011;31(5):369–376.
25. Regnault A, Viala-Danten M, Gilet H, Berdeaux G. Scoring and psychometric properties of the eye-drop satisfaction questionnaire (EDSQ), an instrument to assess satisfaction and adherence with glaucoma treatment. BMC Ophthalmol. 2010;10(1):1.
26. Stryker JE, Beck AD, Primo SA, et al. An exploratory study of factors influencing glaucoma treatment adherence. J Glaucoma. 2010;19(1):66–72.
27. Lacey J, Cate H, Broadway DC. Barriers to adherence with glaucoma medications: a qualitative research study. Eye. 2009;23(4):924–932.
28. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74.
29. Beyhaghi H, Reeve BB, Rogers JE, Stearns SC. Psychometric Properties of the Four-Item Morisky Green Levine Medication Adherence Scale among Atherosclerosis Risk in Communities Study (ARIC) Participants. Value Health. 2016; 19: 996–1001.
30. Wang Y, Lee J, Ko Y. Validity and reliability of a self-reported measure of medication adherence in patients with Type 2 diabetes mellitus in Singapore. Diabet Med. 2012 Sep;29(9):e338–44.
31. Park MH, Kang KD, Moon J. Nonadherence with glaucoma medication in Korean patients: a multicenter qualitative study. The Korean Glaucoma Compliance Study Group. Jpn J Ophthalmol. 2013; 57:47–56.
32. Nordmann JP, Baudouin C, Renard JP, Denis P, Regnault A, Berdeaux G. Identification of noncompliant glaucoma patients using Bayesian networks and the Eye-Drop Satisfaction Questionnaire. Clin Ophthalmo. 2010; 8: 1489–1496.
33. Hermann MM, Ustündag C, Diestelhorst M. Electronic adherence monitoring of topical treatment after ophthalmic surgery. Int Ophthalmol. 2010; 30: 385–390.
34. Robin AL, Covert D. Does adjunctive glaucoma therapy affect adherence to the initial primary therapy? Ophthalmology. 2005; 112: 863–868.
35. Waterman H, Evans JR, Gray TA, Henson D, Harper R. Interventions for improving adherence to ocular hypotensive therapy. Cochrane Database Syst Rev. 2013; 4: CD006132.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.