Back to Journals » Clinical Ophthalmology » Volume 11
Intraocular pressure and visual field changes in normal-tension glaucoma patients treated using either unoprostone or latanoprost: a prospective comparative study
Authors Takemoto D, Higashide T, Saito Y, Ohkubo S, Udagawa S ![]() , Takeda H, Sugiyama K
, Takeda H, Sugiyama K
Received 19 June 2017
Accepted for publication 5 August 2017
Published 1 September 2017 Volume 2017:11 Pages 1617—1624
DOI https://doi.org/10.2147/OPTH.S144344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Daisuke Takemoto, Tomomi Higashide, Yoshiaki Saito, Shinji Ohkubo, Sachiko Udagawa, Hisashi Takeda, Kazuhisa Sugiyama
Department of Ophthalmology, Kanazawa University Graduate School of Medical Science, Kanazawa, Japan
Purpose: We conducted a prospective study in patients with normal-tension glaucoma (NTG) who received either isopropyl unoprostone or latanoprost. We compared the drugs in terms of their effects on intraocular pressure (IOP) and visual field loss progression over a 3-year period.
Study design: Prospective, randomized controlled study.
Methods: We enrolled 48 patients with newly diagnosed NTG at Kanazawa University Hospital. Eligible patients were randomly allocated (1:1) to receive either unoprostone or latanoprost ophthalmic solutions. The primary outcomes were IOP changes and visual field deterioration within 36 months. Visual field changes were analyzed: the cumulative survival rates were calculated in terms of mean deviation, pattern standard deviation, and total deviation of the upper or lower hemi-visual field, each visual field sector, and guided progression analysis. In addition, we evaluated the progression of glaucomatous optic disc changes using fundus photography and confocal scanning laser ophthalmoscopy.
Results: The mean pretreatment IOP was 15.0±2.4 mmHg in the Unoprostone group and 15.2±1.9 mmHg in the Latanoprost group. The mean IOP during the treatment period was 13.7±2.3 mmHg in the Unoprostone group and 13.0±1.8 mmHg in the Latanoprost group. In both groups, the IOP decreased significantly (p<0.001) from baseline after treatment. The posttreatment IOP values were significantly lower in the Latanoprost group than in the Unoprostone group (p=0.023). Regarding the 3-year cumulative survival rate of visual field loss progression, there were no significant differences between groups in any parameters of the visual field or guided progression analysis. There were no significant differences between groups in disc changes.
Conclusions: No significant differences were found between groups with regard to the visual field and structural progression in patients with NTG, although unoprostone was less effective than latanoprost in lowering the IOP.
Keywords: unoprostone, latanoprost, normal-tension glaucoma, intraocular pressure, visual field
Introduction
Lowering the intraocular pressure (IOP) is the only evidence-based therapy to delay visual field deterioration in patients with glaucoma.1,2 To evaluate the efficacy of various glaucoma drugs, a long-term comparative study is necessary. Latanoprost (Xalatan®; Pfizer Co., Ltd, Tokyo, Japan) has been reported to prevent progressive visual field loss with a strong IOP-lowering effect.3 Saito et al reported that isopropyl unoprostone (unoprostone: Rescula®; R-Tech Ueno Ltd., Tokyo, Japan) prevented visual field loss progression in patients with primary open-angle glaucoma (POAG), including normal-tension glaucoma (NTG),4 although unoprostone was less effective than latanoprost in lowering the IOP.5–9
Recently, the role of unoprostone was demonstrated to be different from that of other prostaglandin-related drugs. On the basis of its pharmacological characteristics, unoprostone was characterized as an ion-channel opener10,11 and was associated with an increase in conventional outflow,12 improvement of microcirculatory blood flow, and a neuroprotective action.13,14
We conducted a prospective, randomized controlled study in patients with NTG. The patients received either unoprostone or latanoprost, and we compared the drugs in terms of their effects on IOP and visual field loss progression over a period of 3 years.
Methods
Subjects
Treatment-naïve patients with NTG were enrolled at the Department of Ophthalmology in Kanazawa University Hospital between March 2004 and April 2009. The inclusion criteria were 1) visual field mean deviation (MD) of −10 dB or better by standard automated perimetry (Humphrey Visual Field Analyzer II, 30–2 Swedish interactive threshold algorithm, Carl Zeiss Meditec, Inc, Dublin, CA), 2) best-corrected visual acuity of 0.7 or more, 3) spherical equivalent refractive error between −10 D and 10 D, and 4) age of 20 years or more. Only one eye from each patient was included in the trial. If both eyes from the same patient were eligible, data from the eye with the lower MD were used for analysis. The exclusion criteria were 1) ocular infection, inflammatory disease, or corneal ulcer that occurred ≤1 month before the start of the trial, 2) cataract, retinal disorder, or other disorder that may affect the visual field, 3) history of ocular surgery or laser treatment, 4) optic nerve degeneration other than glaucoma, and 5) pregnancy or suspected pregnancy.
NTG was defined as involving the following: 1) normal open angle, 2) retinal nerve fiber layer defect, or characteristic thinning of the optic disc rim on fundus photographs (including red-free photos) with corresponding visual field defects, 3) no ocular or systemic disorder responsible for a visual field defect, and 4) an untreated IOP of 21 mmHg or less.
This study was approved by the Institutional Review Board (IRB) of Kanazawa University, and the study was conducted in full accord with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients before screening investigations, and potential adverse effects were fully explained.
Study groups
The subjects were randomly assigned (1:1), with the closed envelope technique, to receive either isopropyl unoprostone eye drops (Rescula; 0.12%, 1 drop twice daily – morning and evening – the Unoprostone group) or latanoprost eye drops (Xalatan, 0.005%, 1 drop once daily – evening – the Latanoprost group). The concomitant use of drugs that may have affected glaucoma (topical/systemic anti-glaucoma drugs or topical/systemic steroids) was not permitted during the study.
Study protocol
The subjects were examined twice before starting treatment and every 3 months thereafter. At each examination, any subject who had forgotten to instill the eye drops on ≥10% of the days during the previous 3 months was excluded from the study. Adherence to the treatment was based on a statement provided by the patient. IOP was measured every 3 months in a masked fashion with a Goldmann applanation tonometer. The ophthalmologist who measured the IOP was blinded to the drug used. Standard automated perimetry was performed twice before treatment and every 6 months thereafter. Visual acuity was assessed every 12 months. The optic nerve head was imaged every 12 months with a fundus camera (Kowa nonmyd WX3D retinal camera; Kowa Co., Tokyo, Japan) and a confocal scanning laser ophthalmoscope (Heidelberg Retina Tomograph II [HRT-II]; Heidelberg Engineering GmbH, Heidelberg, Germany). These examinations were performed by an examiner who was blinded to the drug used.
Topical administration was discontinued or changed if adverse effects or a serious eye disease occurred or if there was a request by the subject or a decision by the investigator, considering various factors including the progression of visual field defects.
Main outcome measures
The main outcome measures were IOP reduction and visual field progression after treatment.
Evaluation of structural changes in the optic nerve head
Three glaucoma specialists compared the pair of fundus photographs taken at baseline and 36 months after treatment initiation, which were projected onto a screen alternatively and repeatedly. The chronological order of the two photos was masked. Structural progression was defined as the presence of increased rim thinning, enlarged cupping, or enlargement or emergence of retinal nerve fiber layer defects. Progression was judged to be positive when the decision was agreed upon by all three graders and the chronological order was correct.
Secondly, stereometric parameters of HRT-II, cup area (mm2), rim area (mm2), cup area/disc area ratio, cup volume (mm3), and rim volume (mm3) were examined. The HRT images with an SD of topography of 50 μm or less were adopted.
Statistical analysis
The mean posttreatment IOP was compared with the baseline IOP by paired t-test in each group. The mean percentage IOP reduction after treatment was compared between groups with the Mann–Whitney U test.
Visual field loss progression was judged to have reached its end point relative to baseline when all of the following conditions were fulfilled: 1) MD deterioration >3 dB demonstrated twice during the follow-up period compared with the two baseline values (defined as “MD criteria”), 2) pattern standard deviation (PSD) deterioration >3 dB demonstrated twice during the follow-up period compared with the two baseline values (defined as “PSD criteria”), 3) total deviation (TD) of the upper or lower hemi-visual field deterioration >3 dB demonstrated twice during the follow-up period compared with the two baseline values (defined as “hemi-visual field TD criteria”), 4) when guided progression analysis (GPA) was applicable, the time of either “possible progression” or “highly possible progression”, 5) TD in each sector of a Garway–Heath sector format15 deteriorated >3 dB twice during the follow-up period compared with the two baseline values. Dropout for any reason, including visual acuity decrease (<0.7), adverse reactions, alteration of unoprostone or latanoprost treatment, or addition of another medication, was treated as a treatment failure in each set of criteria. The cumulative probability of survival was compared between groups with the Kaplan–Meier method (log-rank test) for each set of end point criteria listed above.
The number of dropouts and the number of eyes with optic disc progression were compared between groups with Fisher’s exact probability test.
Stereometric parameters of HRT-II were compared between groups with Mann–Whitney U test.
SPSS statistical software, version 17.0J for Windows (SPSS, Inc., Chicago, IL, USA), was used for analysis, and a p-value of <0.05 was considered statistically significant. Values are stated as mean ± SD.
Results
A total of 48 eyes from 48 patients were enrolled in this trial. The characteristics of the patients in each group are shown in Table 1. There were no statistically significant differences between the Unoprostone (n=24) and the Latanoprost (n=24) groups in terms of age, sex, visual acuity, spherical equivalent refractive error, pretreatment IOP, MD, PSD, or duration of follow-up.
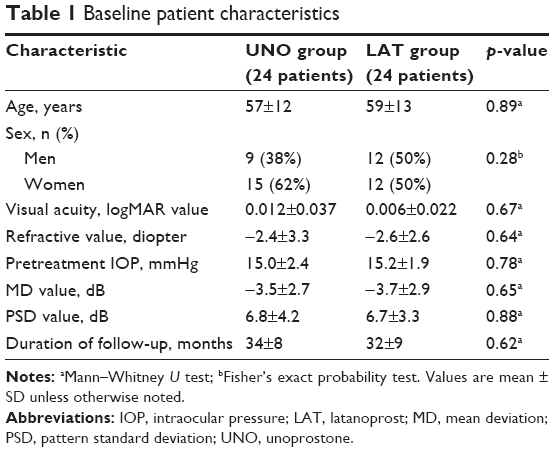 | Table 1 Baseline patient characteristics |
Figure 1 demonstrates the IOP in each group at baseline and every 3 months after treatment. The pretreatment IOP was 15.0±2.4 mmHg in the Unoprostone group and 15.2±1.9 mmHg in the Latanoprost group. The mean IOP during the entire treatment period was 13.7±2.3 mmHg in the Unoprostone group and 13.0±1.8 mmHg in the Latanoprost group. Thus, the mean percentage IOP reduction after treatment was 9%±10% in the Unoprostone group and 14%±13% in the Latanoprost group. In both groups, the mean IOP during the entire treatment period had decreased significantly compared with baseline IOP (Unoprostone group: p<0.001; Latanoprost group: p<0.001). The mean percentage IOP reduction after treatment was significantly greater in the Latanoprost group than in the Unoprostone group (p=0.023).
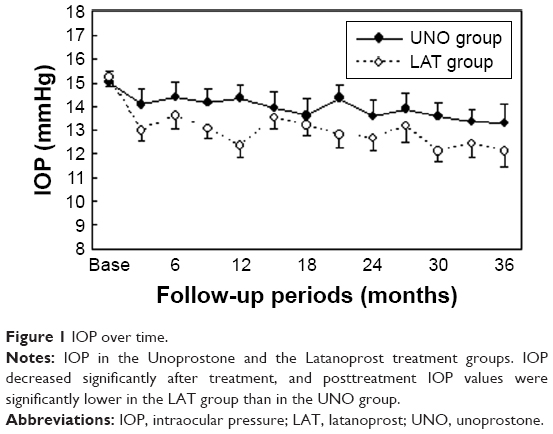 | Figure 1 IOP over time. |
Figures 2 and 3 show the cumulative probability of visual field nonprogression in the Unoprostone group and the Latanoprost group. The cumulative survival rates after 3 years were 74% in the Unoprostone group and 80% in the Latanoprost group when the end point was defined by MD criteria (Figure 2A); 94% in the Unoprostone group and 90% in the Latanoprost group by PSD criteria (Figure 2B); 77% in the Unoprostone group and 70% in the Latanoprost group by hemi-visual field TD criteria (Figure 2C); 67% in the Unoprostone group and 49% in the Latanoprost group defined by “possible progression” in GPA (Figure 3A); and 94% in the Unoprostone group and 75% in the Latanoprost group defined by “highly possible progression” in GPA (Figure 3B). There were no significant differences between groups in any analyses including six sector analyses with regard to the rates of visual field nonprogression (Table 2).
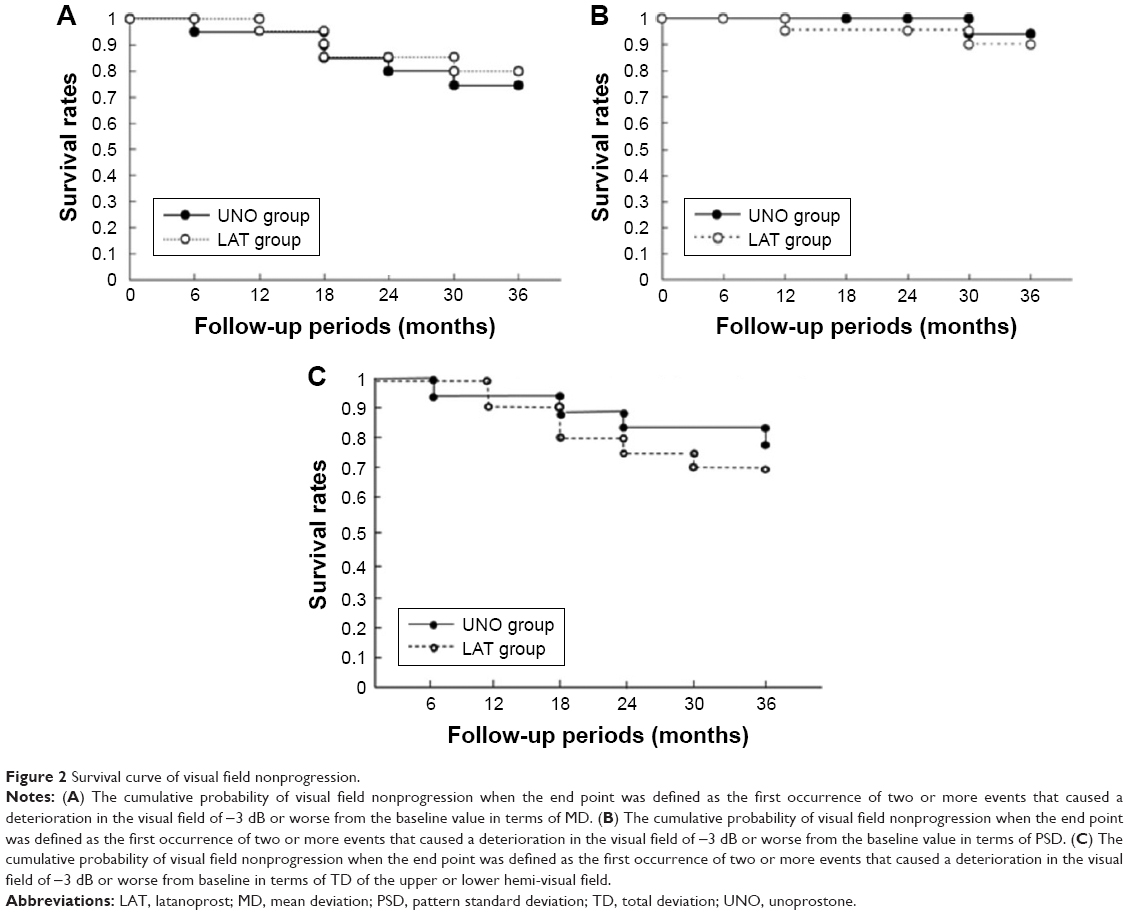 | Figure 2 Survival curve of visual field nonprogression. |
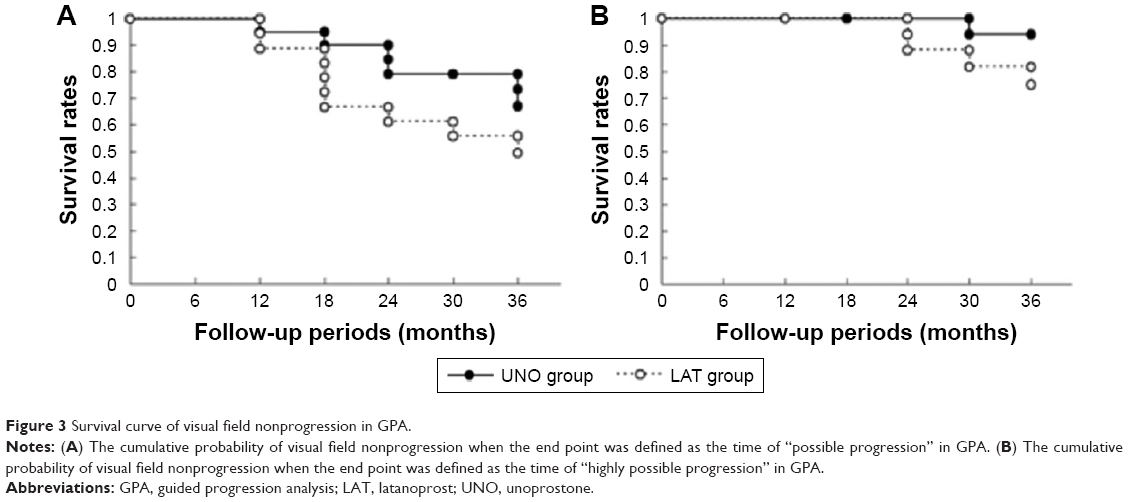 | Figure 3 Survival curve of visual field nonprogression in GPA. |
 | Table 2 Analysis of the rate of nonprogression of visual field loss |
In the fundus photograph assessment, 8 (33.3%) eyes were classified as having progression, whereas 16 (66.7%) eyes were classified as having no progression in both groups (p=1.00).
As shown in Table 3, there were no significant differences between groups with regard to any of the stereometric parameters mentioned above, that is, cup area (mm2), rim area (mm2), cup/disc area ratio, cup volume (mm3), or rim volume (mm3).
 | Table 3 HRT-II changes |
There were no dropouts due to visual acuity decrease in either group during the study. The rate of patient dropout is shown in Table 4. There were no significant differences between groups in terms of the total number of patient dropouts, the number of patient dropouts due to adverse reactions, and change of therapy (p=0.50, p=0.30, and p=0.49, respectively). Two patients in the Unoprostone group were subjected to a change in therapy due to visual field progression.
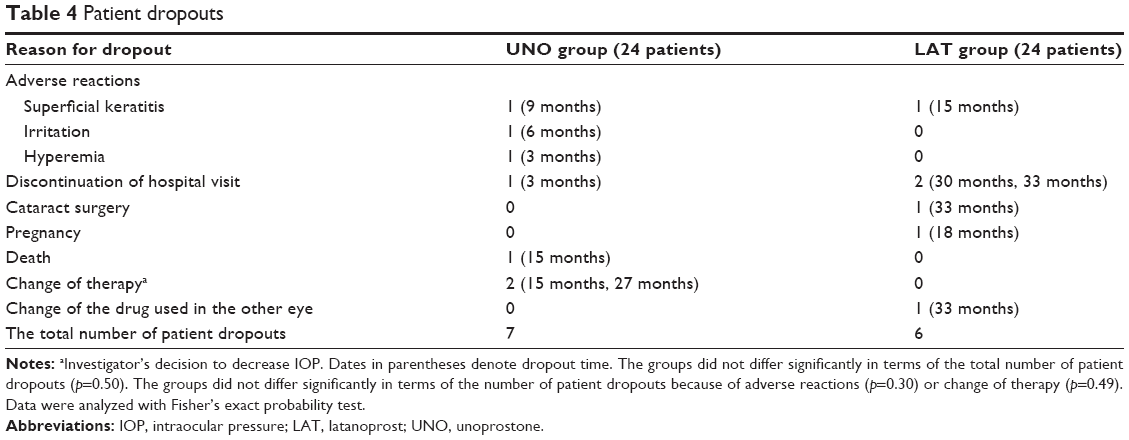 | Table 4 Patient dropouts |
Discussion
Regarding the long-term effects of unoprostone monotherapy, IOP decreased from 13.7±3.0 mmHg to 12.0±2.2 mmHg after 6 years of treatment in patients with NTG.16 Our previous study demonstrated that the mean IOP had decreased significantly from 14.7±3.0 mmHg at baseline to 12.7±4.4 mmHg after 4 years in 32 eyes from 32 patients with POAG including NTG with unoprostone monotherapy.4 The 88.0% visual field nonprogression rate for 4 years in the study was higher than that in a previous report in untreated NTG patients (55.5% nonprogression rate for 4 years).17
Prospective studies that compared the efficacy of unoprostone with that of latanoprost for 8 or 12 weeks were performed by many investigators.5–8,18 Both unoprostone and latanoprost were found to reduce IOP; however, unoprostone was less effective than latanoprost in patients with either POAG or ocular hypertension. Sponsel et al reported that there were no significant differences between unoprostone and latanoprost in MD or PSD using the 10-2 program (Humphrey Visual Field Analyzer), but after 4 weeks of treatment, the MD of the unoprostone group, using frequency-doubling technology, was improved by 1.7 dB over the pretreatment value.9 In patients with NTG, no prospective studies comparing the effects of unoprostone with other drugs have been reported.
Isopropyl unoprostone was developed in Japan in 1994 as the world’s first prostaglandin-related drug and was reported to lower the IOP to a similar degree as timolol in patients with either POAG or ocular hypertension.19 Later, several prostaglandin-related drugs, including latanoprost, were launched and found to reduce IOP even more strongly than conventional products, including unoprostone. Such prostaglandin analogues are now the first-choice drugs in glaucoma therapy.
We conducted a 3-year comparative study in patients with NTG who received either unoprostone or latanoprost alone. Not only did we investigate the effects of the drugs on IOP, but we also focused on visual field loss progression.
Latanoprost conferred a significantly greater reduction in IOP than unoprostone after 3 years of treatment. Our study period of 3 years is the longest among all of the reports mentioned so far,5–8,18 all of which compared IOP reduction between groups for a period of 8–12 weeks.
Additionally, Sponsel et al were the only other investigators to compare the groups in terms of visual field changes.9 Their prospective study with a 4-week observation period seemed too short to detect visual field changes. To detect visual field changes reliably, we used not only MD, but also PSD, TD of the upper or lower hemi-visual field, GPA, and TD by sector, all of which can be indicators of local visual field deterioration. There were no significant differences between the groups with regard to any of these indices. We also investigated structural changes of the optic nerve head using a fundus photograph and the HRT-II. However, no significant differences were found between groups.
The “Collaborative NTG study”1,2 demonstrated that IOP reduction prevented visual field progression, even when the baseline IOP was in the normal range (NTG). Our present study demonstrated that unoprostone may have effects comparable to latanoprost in preventing the visual field loss, even though the IOP reduction was significantly weaker in the Unoprostone group than in the Latanoprost group. Thus, it implies that unoprostone may prevent visual field deterioration not only by lowering the IOP but also by improving optic nerve blood flow or providing neuroprotection. As unoprostone has an extremely low affinity for prostaglandin F2α (FP) receptors, its pharmacological action is unclear. Nonetheless, many studies have addressed the various functions of unoprostone, such as its ability to improve blood circulation and protect neurons. Sugiyama and Azuma reported that subconjunctival injection of unoprostone into rabbit eyes inhibited the decrease of optic disc blood flow induced by intravitreal injection of endothelin-1.20 Moreover, Cuppoletti et al reported that unoprostone relaxes vascular smooth muscle cells,11 and Kimura et al showed that unoprostone increases blood flow to the optic nerve head.13 Thieme et al demonstrated that unoprostone opens membrane Big Potassium (BK) channels (Ca2+-activated Maxi-K channels) and inhibits the elevation of intracellular Ca2+ concentration induced by endothelin-1.10 Unoprostone inhibits cell contraction of the trabecular meshwork and thus causes an increase in conventional outflow, which results in a decrease in IOP, as shown by Toris et al.12 Furthermore, Melamed showed that unoprostone inhibits cell apoptosis by acting on retinal ganglion cells, which implies a direct neuroprotective effect.21
Our study has several limitations, including a relatively small sample size, even though it was a randomized prospective study with a long-term observation period. However, even if the sample size were larger, unoprostone may not be found to be worse than latanoprost in terms of the visual field, because unoprostone showed comparable survival rates to latanoprost on all visual field criteria. Another limitation was the blinding procedures. Ideally, both investigators and patients should be blinded to the treatment groups by using the same eye drop bottles and the same number of instillations. In our study, although examinations including IOP measurements were performed in a masked fashion, the investigators and patients were not blinded as to the treatment groups, which may have affected decisions regarding treatment alteration.
In conclusion, our present study demonstrated that although unoprostone reduced the IOP less than latanoprost in eyes with NTG, there were no significant differences in visual field loss progression between the two groups. This suggests that unoprostone may preserve the visual field to the same degree as latanoprost. Unoprostone may play a significant role in preventing visual field deterioration not only by lowering the IOP but also by other factors, such as improving optic nerve blood flow or neuroprotection.
Acknowledgment
This work was funded by Pfizer and Sucampo Pharma (formerly R-TECH UENO).
Disclosure
Kazuhisa Sugiyama received funding from Pfizer and Sucampo Pharma (formerly R-TECH UENO). The other authors report no conflicts of interest in this work.
References
Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol. 1998;126(4):487–497. | ||
Collaborative Normal-Tension Glaucoma Study Group. The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Am J Ophthalmol. 1998;126(4):498–504. | ||
Garway-Heath DF, Crabb DP, Bunce C, et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;385(9975):1295–1304. | ||
Saito Y, Saeki T, Sugiyama K. [Long-term effects of isopropyl unoprostone monotherapy on intraocular pressure and visual field for normal tension glaucoma and primary open angle glaucoma patients]. Nippon Ganka Gakkai Zasshi. 2006;110(9):717–722. Japanese. | ||
Saito M, Takano R, Shirato S. Effects of latanoprost and unoprostone when used alone or in combination for open-angle glaucoma. Am J Ophthalmol. 2001;132(4):485–489. | ||
Susanna R Jr, Giampani J Jr, Borges AS, Vessani RM, Jordao ML. A double-masked, randomized clinical trial comparing latanoprost with unoprostone in patients with open-angle glaucoma or ocular hypertension. Ophthalmology. 2001;108(2):259–263. | ||
Aung T, Chew PT, Yip CC, et al. A randomized double-masked crossover study comparing latanoprost 0.005% with unoprostone 0.12% in patients with primary open-angle glaucoma and ocular hypertension. Am J Ophthalmol. 2001;131(5):636–642. | ||
Jampel HD, Bacharach J, Sheu WP, et al. Randomized clinical trial of latanoprost and unoprostone in patients with elevated intraocular pressure. Am J Ophthalmol. 2002;134(6):863–871. | ||
Sponsel WE, Paris G, Trigo Y, Pena M. Comparative effects of latanoprost (Xalatan) and unoprostone (Rescula) in patients with open-angle glaucoma and suspected glaucoma. Am J Ophthalmol. 2002;134(4):552–559. | ||
Thieme H, Stumpff F, Ottlecz A, Pericot CL, Lambrou GN, Wiederholt M. Mechanisms of action of unoprostone on trabecular meshwork contractility. Invest Ophthalmol Vis Sci. 2001;42(13):3193–3201. | ||
Cuppoletti J, Malinowska DH, Tewari KP, Chakrabarti J, Ueno R. Unoprostone isopropyl and metabolite M1 activate BK channels and prevent ET-1-induced [Ca2+]i increases in human trabecular meshwork and smooth muscle. Invest Ophthalmol Vis Sci. 2012;53(9):5178–5189. | ||
Toris CB, Zhan G, Camras CB. Increase in outflow facility with unoprostone treatment in ocular hypertensive patients. Arch Ophthalmol. 2004;122(12):1782–1787. | ||
Kimura I, Shinoda K, Tanino T, Ohtake Y, Mashima Y. Effect of topical unoprostone isopropyl on optic nerve head circulation in controls and in normal-tension glaucoma patients. Jpn J Ophthalmol. 2005;49(4):287–293. | ||
Sugiyama T, Mashima Y, Yoshioka Y, Oku H, Ikeda T. Effect of unoprostone on topographic and blood flow changes in the ischemic optic nerve head of rabbits. Arch Ophthalmol. 2009;127(4):454–459. | ||
Garway-Heath DF, Poinoosawmy D, Fitzke FW, Hitchings RA. Mapping the visual field to the optic disc in normal tension glaucoma eyes. Ophthalmology. 2000;107(10):1809–1815. | ||
Ogawa I, Imai K. Long-term effects on visual fields of unoprostone for normal-tension glaucoma. Folia Ophthalmol Jpn. 2003:54;571–577. | ||
Shirai H, Sakuma T, Sogano S, Kitazawa Y. [Visual field change and risk factors for progression of visual field damage in low tension glaucoma]. Nippon Ganka Gakkai zasshi. 1992:96(3);352–358. Japanese. | ||
Kobayashi H, Kobayashi K, Okinami S. A comparison of intraocular pressure-lowering effect of prostaglandin F2-α analogues, latanoprost, and unoprostone isopropyl. J Glaucoma. 2001;10(6):487–492. | ||
Azuma I, Masuda K, Kitazawa Y, Takase M, Yamaura H. Double-masked comparative study of UF-021 and timolol ophthalmic solutions in patients with primary open-angle glaucoma or ocular hypertension. Jpn J Ophthalmol. 1993;37(4):514–525. | ||
Sugiyama T, Azuma I. Effect of UF-021 on optic nerve head circulation in rabbits. Jpn J Ophthalmol. 1995;39(2):124–129. | ||
Melamed S. Neuroprotective properties of a synthetic docosanoid, unoprostone isopropyl: clinical benefits in the treatment of glaucoma. Drugs Exp Clin Res. 2002;28(2–3):63–73. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.