Back to Journals » Clinical Ophthalmology » Volume 14
Inter-Ocular Asymmetry in Anterior Corneal Aberrations Using Placido Disk-Based Topography
Authors Alzaben Z ![]() , Gammoh Y
, Gammoh Y ![]() , Freixas M, Zaben A, Zapata MA, Koff DN
, Freixas M, Zaben A, Zapata MA, Koff DN
Received 23 March 2020
Accepted for publication 8 May 2020
Published 27 May 2020 Volume 2020:14 Pages 1451—1457
DOI https://doi.org/10.2147/OPTH.S255086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zeyad Alzaben, 1,* Yazan Gammoh, 1, 2,* Marta Freixas, 1 Ahmad Zaben, 3 Miguel A Zapata, 4 Dana N Koff 2
1Department of Optometry, Opticalia Clinic, Olot, Spain; 2Department of Optometry Science, Faculty of Allied Medical Sciences, Al-Ahliyya Amman University, Amman, Jordan; 3Optipunt Eye Clinic, Figueres, Spain; 4Ophthalmology Department, Vall d’Hebron Hospital, Barcelona, Spain
*These authors contributed equally to this work.
Correspondence: Zeyad Alzaben
Department of Optometry, Opticalia Clinic, (Plz/Clarà, 12), Olot, Catalonia 17800, Spain
Tel +34 678922564
Email [email protected]
Objective: Inter-ocular asymmetry in anterior corneal high-order aberrations has previously not been investigated. This study aims to investigate the normal range of inter-ocular asymmetry in corneal high-order aberrations (HOAs) using a Placido disk-based corneal topographer to explore the relationship between the HOA parameters of the anterior corneal for each eye individually and the refractive error.
Patients and Methods: A total of 257 subjects (98 males and 159 females) were participated, with an age range of 6 to 81 years (average of 40.2 ± 17.53). Participants were divided into three groups: myopia (spherical equivalent (SEQ) of refraction ≥− 0.50 D), hypermetropia (SEQ ≥+0.50 D), and emmetropia. For all patients, high-order aberrations were measured using a corneal topographer (CA.200TM; Topcon). Inter-ocular asymmetry was represented by RMS (root mean square) for three, five, and seven mm as pupil entry; aberrations for five mm pupil (vertical and oblique trefoil, vertical and horizontal comma, and primary spherical aberration) were recorded using the instrument’s built-in software.
Results: Hypermetropes exhibit the highest inter-ocular asymmetry of all RMS values, mostly in spherical aberrations, and higher-order trefoil values. Oblique trefoil aberrations had the highest interocular asymmetry in the myopic groups. The interocular asymmetry in horizontal coma values was the highest in emmetropes and the lowest in hypermetropes.
Conclusion: To our knowledge, this is the first observational study of inter-ocular differences in high-order aberrations of the anterior corneal surface of the human eye. This study’s results could be used to establish normal values of inter-ocular asymmetry of HOAs of the anterior cornea. The use of such normal values should be investigated further to serve as a guideline for clinicians when establishing the best management route for the patient’s refractive error.
Keywords: anterior corneal aberrations, high-order aberrations, inter-ocular asymmetry, Zernike analysis
Introduction
Previous studies have reported that high-order aberrations may play a role in the development or progression of refractive errors by altering the quality of the retinal image.1 Furthermore, HOAs are of clinical relevance as some dysphotopsias such as night halos and glare have been associated with high amounts of high-order aberrations.2,3 With the advancement in diagnostic techniques and precise corrections of corneal aberrations with lasers, the HOAs have been at the center stage of research for improving the efficiency of the ocular system.4–10
There is currently no gold standard modality for the evaluation of corneal aberrations.11 Nevertheless, the widespread use of corneal topographers is permitting researchers and clinicians to explore the corneal changes associated with refractive errors.11,12
The relationship between the anterior corneal aberrations and the changes in the vision of patients is still unclear. To the knowledge of the authors, no studies have evaluated inter-ocular asymmetry in anterior corneal high-order aberrations (measured using corneal topography) and their correlations with refractive error. Therefore, understanding the nature and degree of association between morphological changes of the cornea and presence or absence of HOAs in patients without refractive error (emmetropic) and with refractive error (ametropic) is of vital importance since it could serve as a guideline for clinicians when considering the best strategy for the management of the present refractive error.
Previous studies have explored the symmetrical distribution of the anterior corneal surface HOAs in healthy patients between right and left eye without establishing any difference limits to be used as a guideline for the clinician to detect any abnormality in the anterior corneal surface.13 This study aimed to 1) Measure the inter-ocular asymmetry in anterior corneal high-order aberrations using corneal topography in emmetropia, myopia, and hypermetropia; 2) Establish a possible relationship between HOAs of the anterior cornea with refractive error. Thus, establishing the different tolerance limits for each refractive type and the amount of the inter-ocular asymmetry for each subject.
Patients and Methods
Subjects
In this observational study, a total of 257 patients were included. These patients included 94 emmetropic, 93 myopic, and 70 hypermetropic patients. The inclusion criteria for the control group (ie, emmetropes) were patients with spherical equivalent between +0.50 D and −0.50 D. Myopia was defined as a spherical equivalent of refraction ≥−0.50 D. Hyperopia was defined as a spherical equivalent of ≥+0.50 D.
Patients with a history of trauma or ocular pathology, ocular or refractive surgery, diabetes mellitus, without central fixation, and those with corneal topographers’ predictors that are compatible with keratoconus were excluded from the study, as well as those with anisometropia ≥ 0.5 D. Patients were also excluded if they did not sign the consent form and if they did not understand the test requirements.
All patients were informed of the purpose of the study (parents were informed if the patients are minors) and received a written document containing information related to the tests. They signed a consent form regarding the details of the exam and the right to analyze all the data collected and for use in future investigations while guaranteeing all participants the confidential treatment of all personal data. A parent or legal guardian provided written informed consent for any participants who were minors. The study was conducted in accordance with the principles of the Helsinki Declaration. This study received the approval of the Ethics Review Board of the Hospital Universitari de Girona Doctor Josep Trueta, Spain.
Instruments Used
To fulfill the objectives of the study, the instruments found in an optometry clinic were used to perform a routine visual examination. These instruments included the retinoscope, manual phoropter (Nidek), digital slit lamp (SL-D4; Topcon), automatic keratorefractometer (ARK.1; Nidek), Early Treatment Diabetic Retinopathy Study (ETDRS) logarithmic visual acuity chart with annotations for testing at 4 meters (13 feet) from the “1” card - Precision Vision ™, and a near visual acuity chart (Gold standard ETDRS near visual acuity chart).
In addition to these instruments, the following instrument was used for the evaluation of the cornea:
CA.200 Corneal Topographer; Topcon.
Procedure
At the first visit, an optometric/ophthalmological history of all patients was recorded, including demographic information of name, sex, age, general medical history, family ocular history any previous or current use of medications.
Next, the patients had a complete visual evaluation and an exam to determine if they were candidates for the study according to the inclusion/exclusion criteria.
Retinoscopy was performed to determine the amount and type of refractive error. Then, the best-corrected visual acuity for distance vision was measured with an ETDRS (Precision Vision ™) test - a backlit box presented at a distance of four meters. Visual acuity data were recorded in logMAR notation.
Corneal Topography
A bite bar was used to maintain the head, and an auxiliary monitor was employed to align the center of the pupil, while the patient was focusing on a central green fixation point, which provides accurate alignment of the subject’s line of sight to the measurement axis. Corneal asphericity for 4.5mm pupil, keratoconus prediction index, and high-order aberration values represented by RMS for three, five, and seven mm as pupil entry, and aberrations for five mm pupil (vertical and oblique trefoil, vertical and horizontal comma values, and spherical aberration) were recorded using the instrument’s built-in software (CA.200, Topcon). The integrated software of the corneal topography has a computational method, which was used for reducing pupil size to simulate the experimental situation of different pupil entries in mm. All measurements of the corneal topography device were taken by the same examiner.
Data Analysis
All data obtained were analyzed using the Statistical Package for Social Sciences (IBM SPSS, V.24; IBM, Inc) Windows software. Data were evaluated for normality with the Kolmogorov–Smirnov test, which revealed that all variables under examination followed a normal distribution. The detailed statistics for controlled, myopic, and hyperopic groups were obtained in mean and standard deviation (SD) from which the absolute intraocular differences of high-order aberrations were obtained, and a 95% confidence interval (CI) was calculated. Inferential statistics were conducted with the Student’s t-test for matched pairs when comparing data from the right (RE) and left eyes (LE) or with the Student’s t-test for unmatched pairs if data belonged to different study groups (such as control, myopic, and hypermetropic groups). Post hoc a test Bonferroni correction was conducted. Inter-ocular differences are shown as (2.5%-97.5%). Pearson’s correlation coefficients were calculated to find the correlations (if any) between anterior corneal high-order aberrations and the mean of the refractive error. A P value of 0.05 was considered as the threshold for statistical significance.
Results
Demographic Distribution
A total of 257 subjects (98 males and 159 females) participated in the study, which was conducted from October 2018 to March 2019. The control group had 27 males, 67 females (n=94) with an age of 37.73 ± 16.27 (range from six to 81 years). Refractive error in the control group was OD +0.005 ± 0.28 (range +0.50 to −0.50) and OS −0.001 ± 0.28 (range +0.50 to −0.50); P = 0.77.
The myopic group comprised of 43 males, 50 females (n=93). The mean age was 31.99 ± 14.33 (range from nine to 69 years), and the refractive error OD −1.79 ± 1.29 D (Range −0.50 to −6.75), OS −1.76 ± 1.26 D (Range −0.50 to −7.88) with P = 0.56 was present.
The hypermetropic group had 28 males, 42 females (n=70) with an average age of 54.14 ± 14.24 (range from 11 to 77 years) and a refractive error of OD +1.43 ± 0.86 D (Range +0.75 to +4.38), OS +1.49 ± 0.91 D (Range +0.75 to +5.13); P = 0.09. Descriptive statistics of refractive and corneal astigmatism for control, myopia, and hypermetropia groups are shown in Table 1.
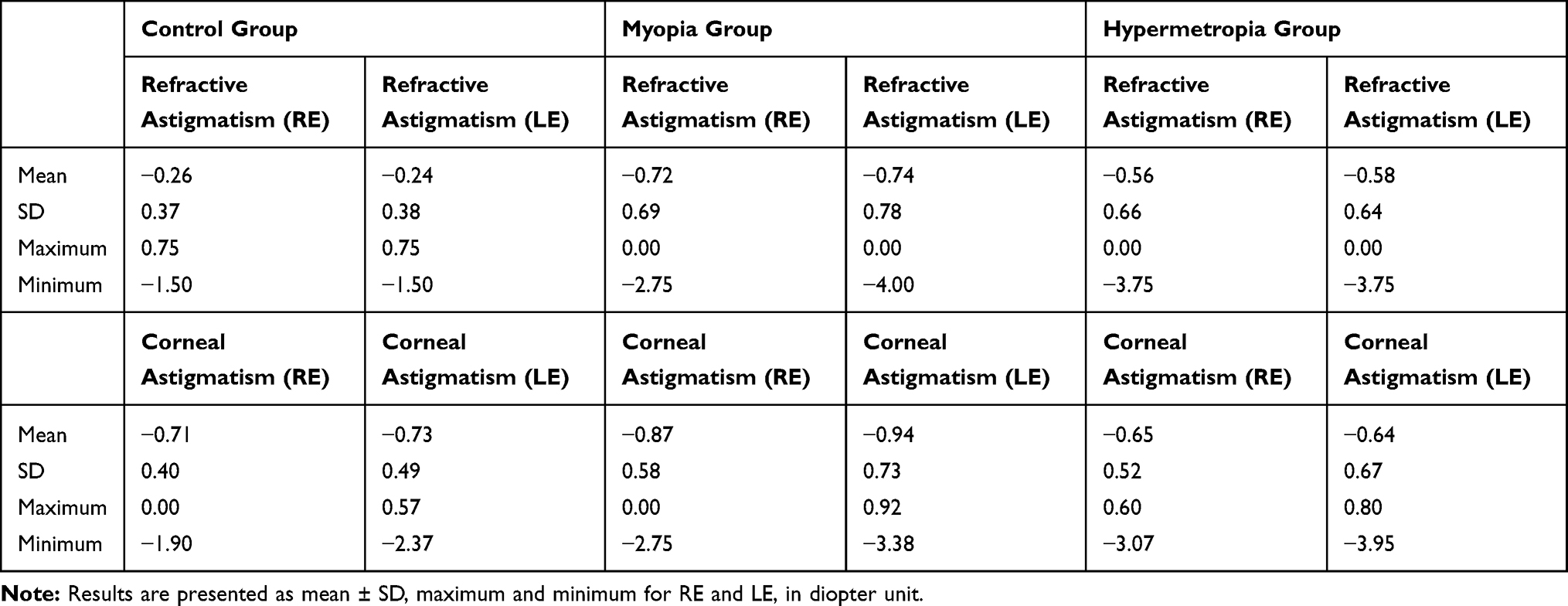 |
Table 1 Descriptive Statistics of Refractive and Corneal Astigmatism for Control, Myopia, and Hypermetropia Groups |
Higher-Order Aberrations
Data were analyzed for the correlation of high-order aberrations (RMS for pupil entry of three, five, and seven mm), and aberrations for five mm pupil (Vertical Trefoil, Horizontal Trefoil, Vertical Coma, Horizontal Coma, Primary Spherical). The inter-ocular variation of Horizontal Coma was found to be more prevalent in all three of the study groups compared to other high-order aberrations, as shown in Tables 2 and 3. The mean absolute inter-ocular differences of Horizontal Coma in control were −0.02 ± 0.1 SD (95% CI), in the myopic group was −0.03 ± 0.1 SD (95% CI), and the hyperopic group was −0.02 ± 0.07 SD (95% CI). The post hoc test Bonferroni correction revealed that the horizontal coma was statistically different for the three groups. The absolute inter-ocular differences of other high-order aberrations with Mean ± SD (95% CI) are listed in Table 4.
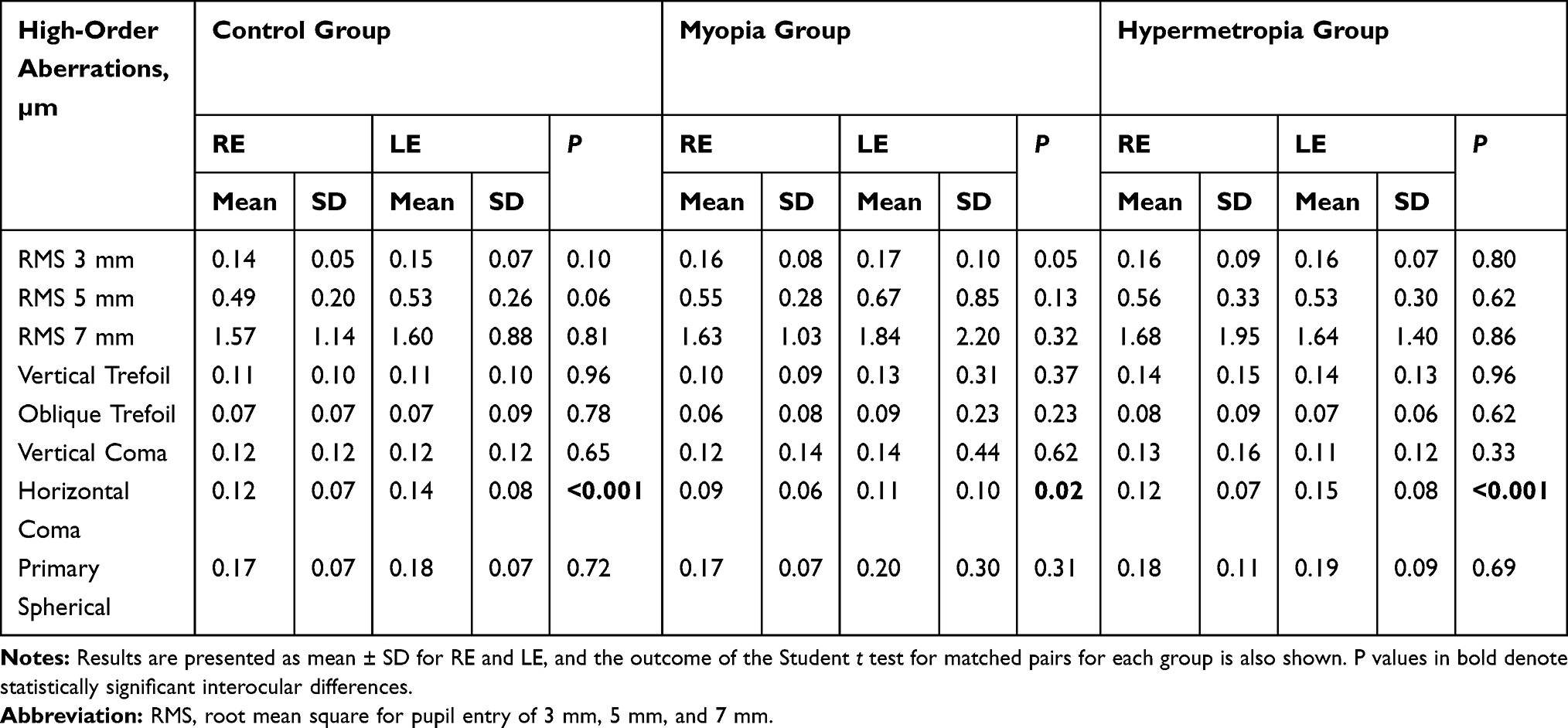 |
Table 2 Mean High-Order Aberrations for Control, Myopia, and Hypermetropia Groups |
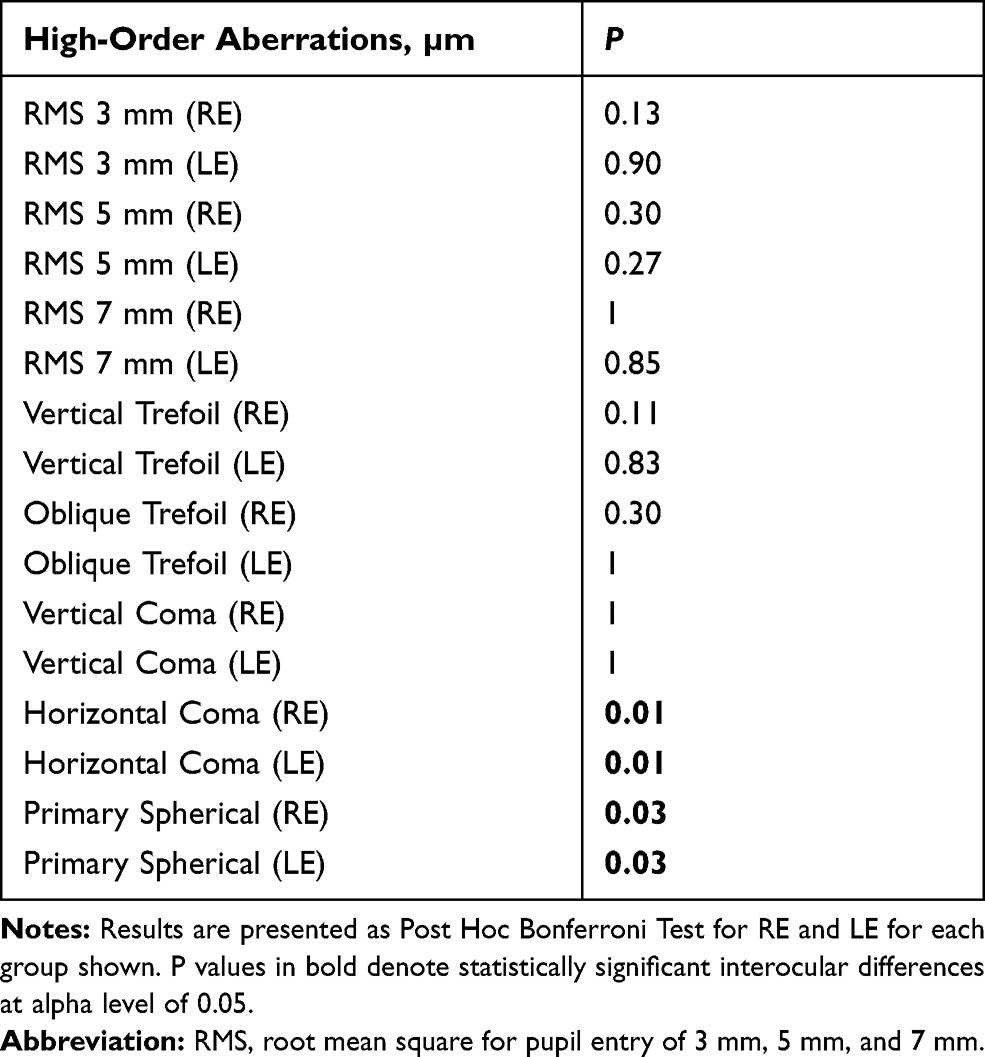 |
Table 3 P values of High-Order Aberrations for All Groups Using Post Hoc Bonferroni Test for Right and Left Eyes |
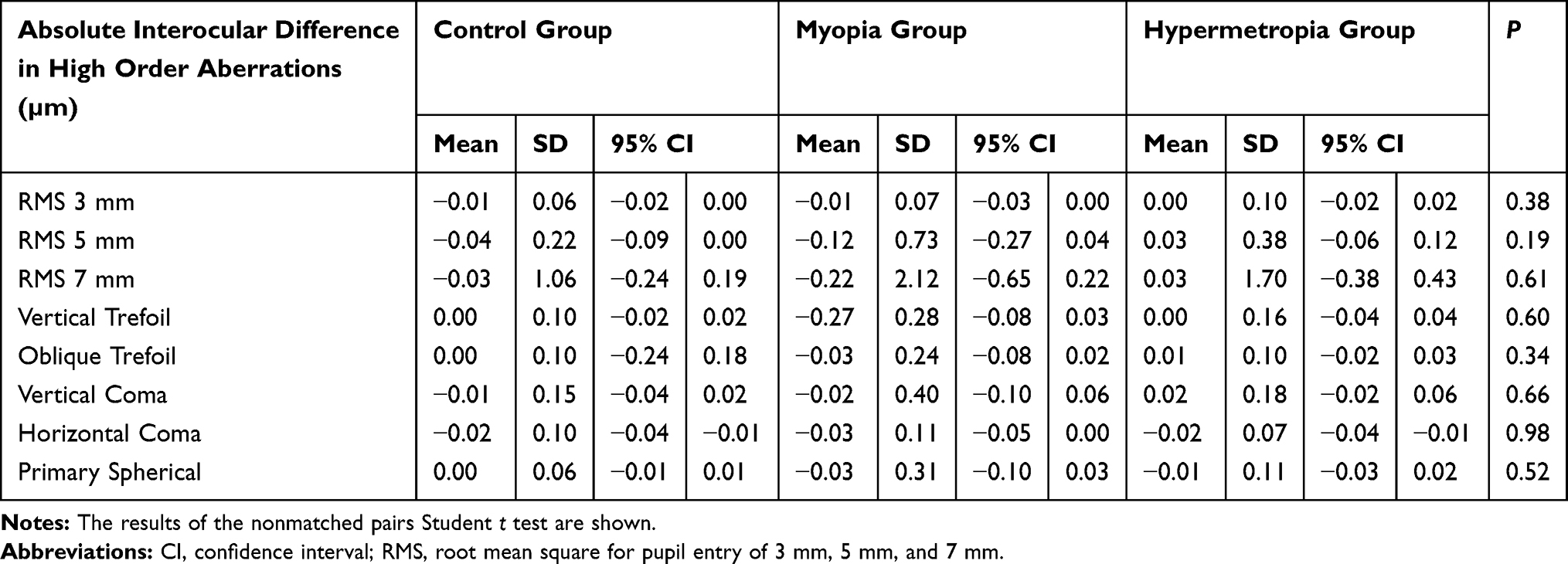 |
Table 4 Absolute Interocular Differences in High-Order Aberrations in Mean ± SD (95% CI) for Control, Myopia, and Hypermetropia Groups |
For most eyes in our study, the significance of anterior corneal aberrations increased with pupil diameter.
Table 5 displays the 95% limits of difference in terms of the 2.5% and 97.5% percentiles.
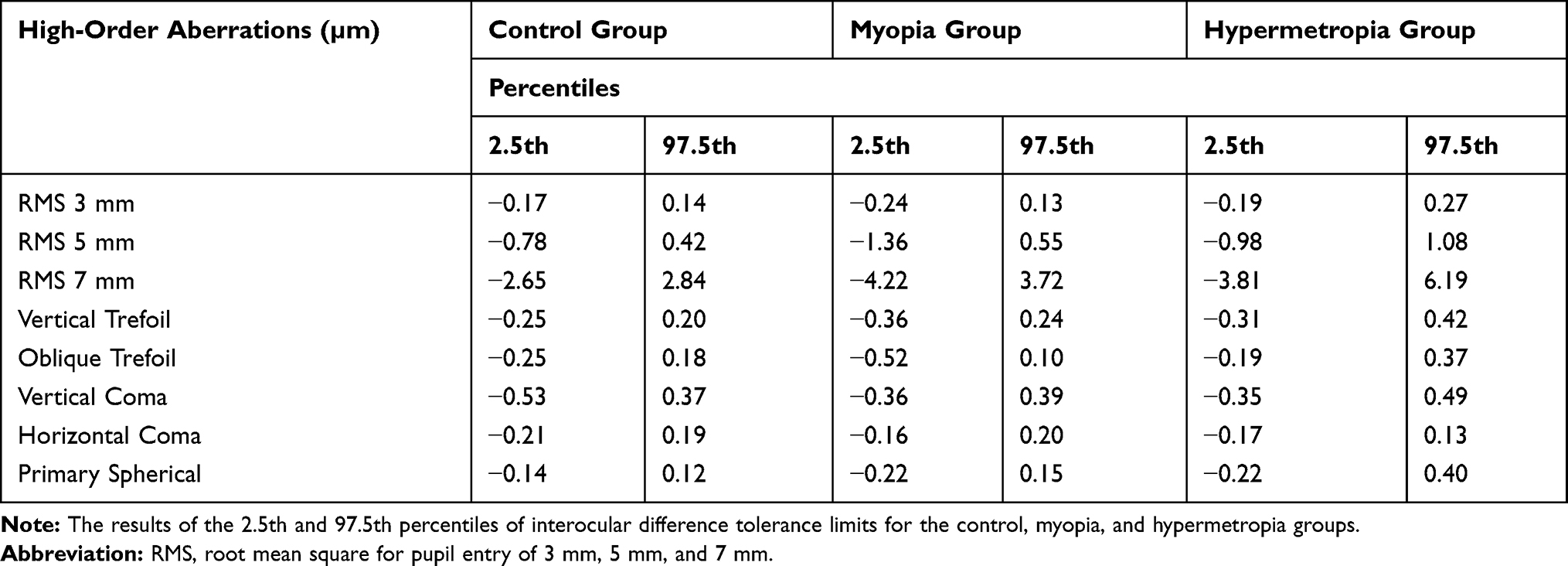 |
Table 5 Percentile Distribution of Interocular Differences (Right Eye Minus Left Eye) in High-Order Aberrations (µm) for Control, Myopia, and Hypermetropia Groups |
High-Order Aberrations and Refractive Errors
Statistically significant, albeit weak correlation, was found only in the myopic group, between the mean spherical equivalent of refraction and RMS for pupil entry of 7 mm in the left eye (r = 0.23; p = 0.02), as well as between mean spherical equivalent and horizontal coma for pupil entry of 5 mm in the right eye (r = 0.40; p <0.001). There was no statistically significant correlation between either anterior corneal aberrations or the spherical equivalent of refraction with age.
Discussion
Low-order aberrations such as myopia, hyperopia, and astigmatism can be easily and efficiently corrected with the use of spectacles, contact lenses, laser procedures, and intraocular lens (IOL) implantation.14 On the other hand, patients with high-order aberrations require detailed ocular examination and complex procedures for the correction of their visual acuity. Nevertheless, the return of 100% corrected vision remains a matter of concern, with many complications arising after corrective procedures. This highlights the importance of understanding the anterior corneal high-order aberrations to establish normative data on their asymmetry, and on how this asymmetry may change with different refractive errors. Thus, enabling the clinician to better understand how the anterior corneal surface changes a wave-front of light entering the eye.
The main objective of the present study was to determine the limits of normal anterior corneal asymmetry in a sample of Caucasian patients using a corneal topographer. Evaluation of asymmetry of HOAs at the anterior corneal surface level is of relevance for predicting the visual outcomes after refractive surgeries, which may lead to a significant alteration of the optical quality before changes are documented with standard visual acuity measurement. This would be important as previous studies demonstrated a strong correlation between the presence of high-order aberrations and corneal astigmatism.15 The CA200 provides asymmetry value within the same corneal surface (ie, for each eye) to detect if there is keratoconus. In our study, all subjects have a normal asymmetry value, presented by the green numerical color in our maps. Thus, all HOAs shown were for normal corneal asymmetries.
The corneal topographer (CA200; Topcon) employed, has 24 rings that measure over 10,000 data points resulting in an axial resolution of 3 microns. To provide improved workflow, the capture system of the CA-200 is automatic and selects the best-focused image to be captured. Without this automatic feature, the corneal rings from the observational screen would look ruptured or defocused. To control the influence of dynamic tear film changes after eye-opening, the patients were asked to blink after the corneal rings had been defocused so that we would get a uniformed tear film covering; thus, ensuring results obtained are related to the corneal surface.
Given the significant role of the cornea in the refractive ocular system, establishing a normative data about the asymmetry of anterior corneal aberrations would lead to a change of the patient’s refractive error management strategy by better understanding the inter-ocular difference tolerance limits. For that, the concept of inter-ocular asymmetry is crucial in both the planning of clinical evaluations and the interpretation of their results. The previous studies have explored the symmetrical distribution of high-order aberrations parameters in small samples without establishing normal difference limits to be employed as a guideline for any abnormality of the anterior cornea such as corneal dystrophy.3 The current study found an association between the variations in the inter-ocular values of HOAs in emmetropic and ametropic groups. The asymmetric presence of horizontal coma was the most common of all HOAs in these groups.
Marcos and Burns16 explored the symmetry between eyes of wave-front aberration and cone directionality in a sample of 12 subjects (Spherical refraction ranged from 0 to −6.0) using a spatially resolved refractometer and a reflectometric imaging technique, respectively. The pupils were dilated with tropicamide 5%. They assumed that, in general, the pattern of aberrations is non-symmetric. This is in agreement with our study; where the inter-ocular differences demonstrate that the aberration value of each parameter under evaluation was higher in the left eye than the right eye for all groups, except the horizontal coma in hypermetropia, which was highest in the right eye.
The normal tolerance difference limits were presented in Table 5. The asymmetry of each explored RMS value, as well as the primary spherical of the Zernike aberration coefficients, was highest in the hypermetropia group and lowest in the control group. Similarly, all higher-order trefoil values were highest in the hypermetropia group and lowest in the control group, except for the oblique trefoil aberration where it was highest in the myopic group. On the contrary, horizontal coma values were highest in the control group and lowest in the hypermetropia group.
The above results highlight the difference between the higher-order aberrations of one eye in comparison to the fellow eye and to estimate how much variation the ocular health practitioners should expect to enable them to evaluate the higher-order aberrations of the anterior corneal surface beyond emmetropia and ametropia.
The study was aimed at assessing the inter-ocular asymmetry in anterior corneal aberrations using instruments that are readily and commonly available in most optometric practices or stand-alone ophthalmology clinics which has led to some limitations in the study. First, as also noted by previous authors,17 the inability to have precisely equal pupil size in the explored eyes affects reliable comparison and requires caution. Second, the Placido-based topographers are limited to providing analysis of data obtained from the anterior cornea; thus, the lack of information about the posterior corneal surface indicates that further research would be beneficial to study the concept of inter-ocular asymmetry in posterior corneal aberrations using an aberrometer, which is not commonly available in an optometric setting or many stand-alone ophthalmology clinics.
As far as the authors’ knowledge, this is the first study to investigate the inter-ocular differences in high-order aberrations of the anterior corneal surface using a Placido disk-based topography in emmetropia, myopia, and hypermetropia in the absence of ocular complications. Our findings revealed a range of inter-ocular differences in ametropia within a controlled clinical setting. This study demonstrates how practitioners can use the tools already available at their disposal to maximize the best results for a patient. The established normal values of inter-ocular differences in high-order aberrations at the anterior cornea could be investigated further as a potential guideline for clinicians during decision making when refractive error correction is considered.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cade F, Cruzat A, Paschalis EI, Espírito Santo L, Pineda R. Analysis of four aberrometers for evaluating lower and higher order aberrations. PLoS One. 2013;8(1):e54990. doi:10.1371/journal.pone.0054990
2. Giers BC, Khoramnia R, Varadi D, et al. Functional results and photic phenomena with new extended-depth-of-focus intraocular Lens. BMC Ophthalmol. 2019;19(1):197. doi:10.1186/s12886-019-1201-3
3. Yagi-Yaguchi Y, Yamaguchi T, Okuyama Y, Satake Y, Tsubota K, Shimazaki J. Corneal higher order aberrations in granular, lattice and macular corneal dystrophies. PLoS One. 2016;11(8):e0161075. doi:10.1371/journal.pone.0161075
4. Little JA, McCullough SJ, Breslin KM, Saunders KJ. Higher order ocular aberrations and their relation to refractive error and ocular biometry in children. Invest Ophthalmol Vis Sci. 2014;55(8):4791–4800. doi:10.1167/iovs.13-13533
5. Khan MS, Humayun S, Fawad A, Ishaq M, Arzoo S, Mashhadi F. Comparison of higher order aberrations in patients with various refractive errors. Pak J Med Sci. 2015;31(4):812–815. doi:10.12669/pjms.314.7538
6. de Castro LE, Sandoval HP, Bartholomew LR, Vroman DT, Solomon KD. High-order aberrations and preoperative associated factors. Acta Ophthalmol Scand. 2007;85(1):106–110. doi:10.1111/j.1600-0420.2006.00757.x
7. Wang J, Ren Y, Liang K, Jiang Z, Tao L. Changes of corneal high-order aberrations after femtosecond laser-assisted in situ keratomileusis. Medicine (Baltimore). 2018;97(18):e0618. doi:10.1097/MD.0000000000010618
8. Bühren J, Pesudovs K, Martin T, Strenger A, Yoon G, Kohnen T. Comparison of optical quality metrics to predict subjective quality of vision after laser in situ keratomileusis. J Cataract Refract Surg. 2009;35(5):846–855. doi:10.1016/j.jcrs.2008.12.039
9. Kim TI, Alió Del Barrio JL, Wilkins M, Cochener B, Ang M. Refractive surgery. Lancet. 2019;393(10185):2085–2098. doi:10.1016/S0140-6736(18)33209-4
10. Kasahara K, Maeda N, Fujikado T, et al. Characteristics of higher-order aberrations and anterior segment tomography in patients with pathologic myopia. Int Ophthalmol. 2017;37(6):1279–1288. doi:10.1007/s10792-016-0356-7
11. Martin R. Cornea and anterior eye assessment with placido-disc keratoscopy, slit scanning evaluation topography and scheimpflug imaging tomography. Indian J Ophthalmol. 2018;66(3):360–366. doi:10.4103/ijo.IJO_850_17
12. Penna RR, de Sanctis U, Catalano M, Brusasco L, Grignolo FM. Placido disk-based topography versus high-resolution rotating Scheimpflug camera for corneal power measurements in keratoconic and post-LASIK eyes: reliability and agreement. Int J Ophthalmol. 2017;10(3):453–460. doi:10.18240/ijo.2017.03.20
13. Thibos LN, Hong X, Bradley A, et al. Statistical variation of aberration structure and image quality in a normal population of healthy eyes. J Opt Soc Am a Opt Image Sci Vis. 2002;19(12):2329–2348. doi:10.1364/josaa.19.002329
14. Anbar M, Mohamed Mostafa E, Elhawary AM, Awny I, Farouk MM, Mounir A. Evaluation of corneal higher-order aberrations by scheimpflug-placido topography in patients with different refractive errors: a retrospective observational study. J Ophthalmol. 2019;2019:5640356. doi:10.1155/2019/5640356
15. Leung TW, Lam AK, Kee CS. Ocular aberrations and corneal shape in adults with and without Astigmatism. Optom Vis Sci. 2015;92(5):604–614. doi:10.1097/OPX.0000000000000581
16. Marcos S, Burns SA. On the symmetry between eyes of wavefront aberration and cone directionality. Vision Res. 2000;40(18):2437–2447. doi:10.1016/s0042-6989(00)00103-6
17. Anbar M, Mohamed Mostafa E, Elhawary AM, et al. Evaluation of corneal higher-order aberrations by scheimpflug-placido topography in patients with different refractive errors: a retrospective observational study. J Ophthalmol. 2019;2019:5640356. doi:10.1155/2019/5640356
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.