Back to Journals » Clinical Ophthalmology » Volume 11
Influences on rebubble rate in Descemet's membrane endothelial keratoplasty
Authors Mechels KB, Greenwood MD, Sudhagoni RG, Berdahl JP ![]()
Received 25 July 2017
Accepted for publication 20 October 2017
Published 5 December 2017 Volume 2017:11 Pages 2139—2144
DOI https://doi.org/10.2147/OPTH.S147217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Keegan B Mechels,1 Michael D Greenwood,2 Ramu G Sudhagoni,3 John P Berdahl2
1Sanford School of Medicine, University of South Dakota, Vermillion, SD, 2Vance Thompson Vision, Sioux Falls, SD, 3School of Health Sciences, University of South Dakota, Vermillion, SD, USA
Purpose: Descemet’s membrane endothelial keratoplasty (DMEK) is a minimally invasive partial corneal transplant procedure used in patients with failing endothelial membranes. This study aims to identify those factors which influence the need for a rebubble of the corneal graft.
Methods: A total of 94 eyes that received DMEK between March 2014 and January 2016 at Vance Thompson Vision were used in the study. Demographic and graft data were collected from the patients and donors, and perioperative statistics of the procedures. A logistical regression was used to compare eyes that did and did not require a rebubble.
Results: Among those characteristics that were included (patient age/sex, donor age/sex, death to processing time, donation to surgery time, death to procurement time, specular cell count density, burping procedure, postoperative day 1 intraocular pressure [IOP], and postoperative week 1 IOP, concurrent phacoemulsification, and how well the Descemet graft was centered), only a lower specular cell count density of the corneal graft, and a graft that was not well-centered correlated with needing a rebubble due to partial graft detachment (p=0.021) and (p=0.023), respectively.
Conclusion: An increased specular cell count density may allow for better placement of the corneal graft by allowing for better unfolding in DMEK procedures. A well-centered graft may decrease postoperative complications by increasing adherence. Additionally, postoperative management of IOP may not affect the rebubble rate, and therefore should be left to the discretion of the provider to determine whether it is necessary.
Keywords: descemet, rebubble, keratoplasty, DMEK
Introduction
The endothelial cells of the cornea are a single layer of hexagon-shaped cells whose integrity is crucial for optimal corneal transparency.1,2 The density of this layer of endothelial cells is measured in the number of cells per mm2. Fuchs endothelial corneal dystrophy (FECD) is a corneal disease where damaged endothelial cells migrate and enlarge to form guttae that maintain the monolayer, decreasing visual acuity.3,4 In recent years, various posterior lamellar keratoplasty procedures such as Descemet stripping endothelial keratoplasty (DSEK) and Descemet’s membrane endothelial keratoplasty (DMEK) have started to replace more extensive transplant procedures like penetrating keratoplasty.4
This study will focus on DMEK, a procedure that reduces the invasiveness of the keratoplasty and the thickness of the graft itself, allowing for reduced recovery periods and less likelihood of graft rejection.5–7 However, because of the thin layer of this graft, early postoperative complications of DMEK are common.8–10 The most common complication of DMEK is partial graft detachment, usually defined as more that 30% of graft detachment from the existing cornea or detachment of more than 2 clock hours, though there is no universally agreed upon definition.5–8 In partial detachments of lesser degree, long-term follow-up has showed that it is likely that the graft will reattach on its own.13 However, if a larger partial detachment is left alone, it is more likely the patient will need a repeat DMEK procedure due to graft failure.
To combat partial graft detachment in postoperative DMEK patients, gas can be injected into the anterior segment postoperatively to help approximate the graft with the remaining corneal tissue of the patient in the hope that the partial detachment will spontaneously reattach. This procedure, commonly referred to as a “rebubble,” has been shown to be effective in allowing for spontaneous reattachment of corneal grafts.13
Rebubbling rates vary drastically, and there has yet to be a definitive study that shows which factors lead to higher rates of rebubbling.9,10,15–18 In this study, we aim to identify those factors directly influencing partial corneal graft detachment necessitating a rebubble of the graft.
Materials and methods
Patients
This study looked at 94 eyes that underwent DMEK at Vance Thompson Vision (Sioux Falls, SD, USA) between March of 2014 and January of 2016. All eyes included in the study were set to receive corneal transplant due to FECD causing patients vision to deteriorate. Patients included in this study had data available from preoperative assessment as well as at least 1 week postoperatively and a best-corrected visual acuity (BCVA) at 3 months. Patients who did not have complete information for these visits were excluded. The information collected from each procedure included patient age, donor age, patient sex, donor sex, time from death to procurement of the eye, time from death until processing of the eye to obtain the graft, specular cell count of the donor graft endothelial cells, whether or not interventions to lower intraocular (IOP) pressure postoperatively took place (burp), postoperative day 1 IOP, postoperative week 1 IOP, whether phacoemulsification was done currently with DMEK, whether the graft was determined to be well-centered in the first week postoperatively, and whether or not the graft needed a rebubble to reapproximate with the stroma. As a measure of surgical outcomes, BCVA was measured at 3 months in all patients. This study was approved by the institutional review board at The University of South Dakota, Vermillion, South Dakota, as a retrospective study. Informed consent was waived through The University of South Dakota as all data collected were deidentified and included no more information than what would normally be collected for this procedure.
Graft preparation
The donor tissue is processed by our local eye bank technicians (Dakota Lions Sight and Health, Sioux Falls, SD, USA) by “pre-stripping” donor Descemet’s membrane from the overlying stromal bed, leaving a “hinge” of approximately 10% attachment to keep Descemet’s membrane stable and attached in the transport vial filled with Optisol GS (Bausch and Lomb, Rochester, NY, USA). The hinge location is identified with a notch placed in the sclera by the technician. Trypan blue solution (Vision Blue; Dutch Ophthalmic USA, Exeter, NH, USA) is placed to stain the tissue and identify the edges. The donor corneal–scleral tissue is placed endothelial side up on a trephine block (Moria, Doylestown, PA, USA) and centered according to the edges of the flap of donor Descemet’s membrane.
With direct visualization, the donor trephine, usually 8.0 mm in diameter, is lowered onto the tissue, and the donor Descemet’s membrane is cut and the trephine is removed. The donor membrane peripheral to the cut is removed. The donor graft is gently picked up with a tying forceps to complete the stripping of the hinge area. Trypan blue is then used to stain the tissue again, and the excess fluid is removed via a surgical sponge. The donor corneal–scleral tissue well is filled with balanced salt solution, and the tissue is aspirated into the injector device as previously described by Terry et al.29
Procedure
Prior to bringing the patient to the operating room, an inferior peripheral iridotomy is made with an Nd:YAG laser. The DMEK procedure is as follows. A 1.0 mm paracentesis is made, and intraoperative anesthesia is administered. A cohesive viscoelastic is placed into the anterior chamber, and a 2.4 mm incision is made. An 8.0-mm or larger diameter central area of recipient Descemet’s membrane is stripped and removed. The viscoelastic material is removed by an automated irrigation/aspiration tip. Short-acting pupillary constriction is achieved with acetylcholine, and the pressure is normalized. If the DMEK is combined with cataract surgery, cataract surgery is done in the usual fashion, and once the intraocular lens has been placed, the stripping of the host tissue is performed, and the remaining viscoelastic is removed. Next, the tip of the injector is placed into the anterior chamber through the main wound. The tissue is injected, the pressure in the anterior chamber is lowered through the paracentesis sites with shallowing of the anterior chamber to maintain hypotony, and the injector tip removed, taking care to externally compress the wound central to the tip with a cannula and prevent the tissue from following the injector tip out of the wound. Although self-sealing, the main wound is further secured with a single interrupted 10-0 vicryl suture. Using a modified Yoeruek tap technique with no gas bubble above or below the graft, the tissue is unscrolled. Once centered, injection of 20% SF6 gas is placed between the graft and the iris, for an 80%–90% fill. The eye is brought to a pressure between 15 and 30 mmHg, and the patient is taken out of the operating room. They are left in supine position for 1 hour and then the patient is evaluated with a slit-lamp for examination. An IOP measurement is also taken to ensure normal tension. The eye is shielded, and the patient is discharged. Once home, the patient is instructed to lie in the supine position as much as possible, but allowed up for 15 minutes at a time for meals and toileting. If possible, the patient is encouraged to sleep in the supine position. Patients are instructed to use Durezol and Vigamox (Novartis, Basel, Switzerland) drops four times daily. Patients were followed up with postoperative checks at the 1-day, 1-week, 1-month, and 3-month period.
Statistical analysis
Descriptive analysis is presented for both continuous and categorical variables. A multivariate logistic regression model was used to investigate the associations between response rebubble and several independent variables. A Wilcoxon Rank Sum test procedure was used to compare the population distributions of visual activity between rebubble groups. Significance level was set at 5%. Statistical analysis of data was performed using SAS software, version 9.4, (SAS Institute, Cary, NC, USA).
Results
Of 108 eyes that received partial cornea transplant between March 24, 2014 and January 11, 2016, 14 were excluded because they received DSEK or there was insufficient data postoperatively to justify inclusion, leaving 94 eyes in the study group. The mean age of patients was 70.4±11.7 years at time of surgery with a range between 39 and 89 years. There were 24 males included and 70 females. Of the 94 eyes that met the criteria for inclusion, 21 eyes required a rebubble procedure postoperatively and 73 eyes did not (22.3%). Fifty-seven of the patients had phacoemulsification done concurrently with DMEK. Demographic data for patients and donors as well as perioperative statistics for all patients can be found in Tables 1 and 2, respectively.
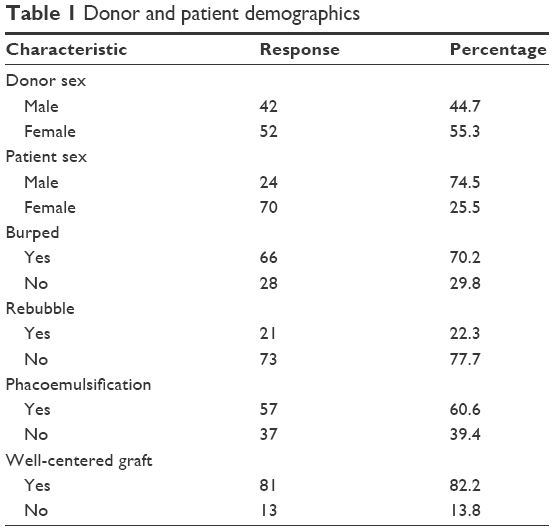 | Table 1 Donor and patient demographics |
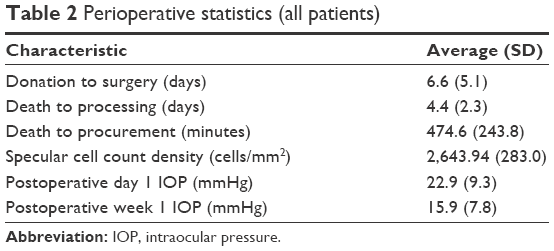 | Table 2 Perioperative statistics (all patients) |
Of the 21 patients who required a rebubble, the mean age of patients was 71.5±9.5 years, while the age of donors of the corneal graft was 64.7±6.8 years in these cases. Fourteen of the 21 patients were female. When looking at donor sex, eight of the 21 patients who required rebubbling received their graft from a male. The donation to surgery time was 8.6±9.8 days. The time from death to procurement in these patients was 481.5±271.8 minutes. The time from death to processing of the graft was 4.61±2.5 days. The donor grafts that eventually required a rebubble had a specular cell count density of 2,479.0±282.9 cells/mm2. Five of the eyes that needed a rebubble underwent postoperative lowering of the IOP at 1-hour postoperative check via a wound burp (24%). The IOP at the 1-day postoperative visit was 19.6±8.2 mmHg, while the 1-week postoperative visit IOP was 12.9±6.8 mmHg. Seven of the patients had grafts that were not well-centered (33%). Twelve of the patients had phacoemulsification done concurrently at the time of surgery (57%).
Of the 73 patients who did not need a rebubble, the mean age of patients was 70.0±11.2 years, while the age of donors of the corneal graft was 63.9±8.0 years in these cases. The donation to surgery time was 5.9±2.3 days. Fifty-eight of the 73 patients were females. When looking at donor sex, 45 of the 73 patients who did not require rebubbling received their graft from a male (62%). The time from death to procurement in these patients was 472.7±362.2 minutes. The time from death to processing of the graft was 4.3±2.2 days. The donor grafts had a specular cell count density of 2,691.4±266.5 cells/mm2. Seventeen patients were male, while 56 were females. Twenty-three eyes had postoperative lowering of the IOP at 1 hour check via wound burp (32%). The IOP at the 1-day postoperative visit was 23.8±9.5 mmHg, while at the 1-week postoperative visit it was 16.8±7.9 mmHg. Forty-five patients had phacoemulsification done at the time of surgery (62%) and 6 patients had grafts that were not well-centered (8%). Demographics and perioperative data are displayed in Table 3 for both rebubble and non-rebubble groups.
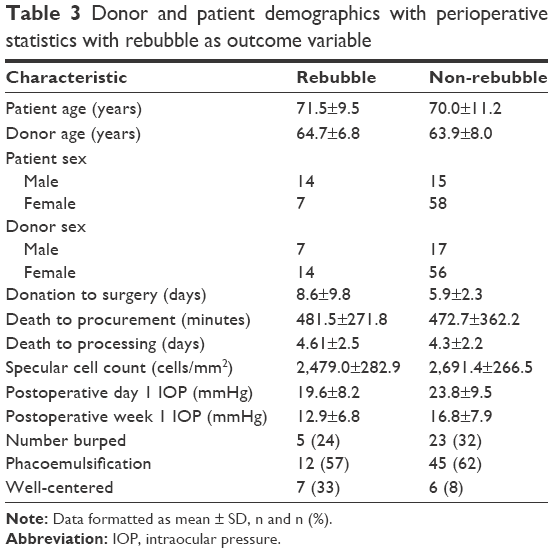 | Table 3 Donor and patient demographics with perioperative statistics with rebubble as outcome variable |
When these factors were inserted into the logistical regression to be compared at the same time, the specular cell count was significantly different between the rebubble and non-rebubble group, with the non-rebubble group having higher specular cell count density (p=0.021). In addition, grafts that were well-centered required a rebubble less often (p=0.023). All other factors including age of patients (0.865), donor age (0.276), donation to surgery time (0.347), donor sex (0.326), death to procurement time (0.189), death to processing days (0.496), recipient sex (0.362), whether the eye was burped or not (0.453), postoperative day 1 pressure (0.106), postoperative week 1 pressure (0.493), and whether the eye had phacoemulsification at time of surgery (0.512) did not significantly contribute to whether a patient received a rebubble. Logistical regression data can be found summarized in Table 4.
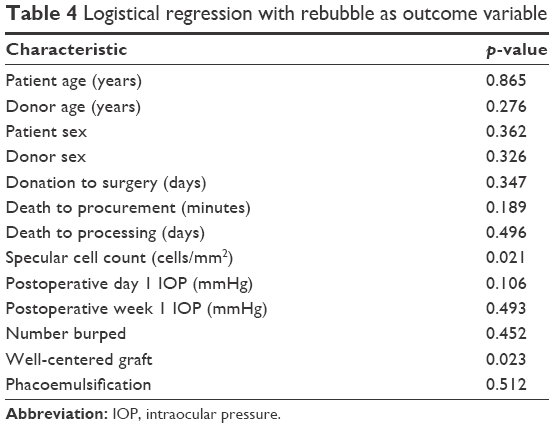 | Table 4 Logistical regression with rebubble as outcome variable |
BCVA for the rebubble and non-rebubble groups were 0.131±0.1145 logMAR and 0.181±0.208 logMAR, respectively (p=0.586).
Discussion
Though surgeons have had the capability to provide DMEK to patients for over a decade now, more surgeons still choose DSEK over DMEK. This has commonly been associated with the steep learning curve of the procedure itself, even though DMEK has proven superior visual outcomes and reduction in the risk of immunological rejection.5,19 The most common complication of this procedure is partial graft detachment, which may be caused by a host of factors but is remedied easily with a rebubble of the graft. While it is true that a rebubble is common following DMEK, the factors that may influence the need for a rebubble are still relatively unknown.17,18 This study aimed to identify what those factors may be so as to avoid consequences of needing a rebubble, such as increased endothelial cell density (ECD) decay and poorer visual acuity outcomes.20
When looking at graft recipient data, the age of the patient had no effect on whether or not the patient would eventually require a rebubble to reattach the graft. These results are consistent with those that have been seen in the past.12,21 Maier et al17 did show that with older recipients, there may be a higher likelihood of graft detachment. However, this association was related to the inability of the older patients to stay supine long enough to get ideal graft attachment.17
In comparison of donor graft demographics and the preparation data on the grafts, it was determined that there was no correlation as to whether or not the recipient would need a rebubble. These results are consistent with other studies that have looked at donor graft demographics.18,22–24 While it has been shown in the past that donor graft age and donor graft storage time may play a role in partial graft detachment, this study concluded that it was grafts from younger donors that were more likely to cause this (<45 years of age).15 This was attributed to grafts from older donors being more rigid and thus less likely to roll tightly, complicating the procedure itself. In our study, only one graft was used where the donor was under this age (39), and this graft did not require a rebubble. It should be noted that Lass et al24 concluded that grafts from older donors, though more favorable for procedural purposes, may in fact lead to increased endothelial cell decay and decreased longevity of the graft.
Though most information about the donor grafts was similar between our groups, it was determined that endothelial cell density was higher in the group that did not require a bubble compared to those who did. While it is unlikely that this has a major effect on graft adherence itself, it is possible that with a higher cell density comes a thicker graft itself.11 This thicker graft would in turn be easier to unfold during the procedure, allowing for more precise placement, less surgical trauma of the graft as it is unrolled, and the higher ECD is ideal for longevity of the graft as well.25
Pressure within the eye postoperatively has been closely studied in DMEK procedure and widely debated among surgeons as well as how much gas should be inserted into the anterior chamber following the procedure.14,22 It is often the case that surgeons prefer to keep postoperative eye pressure slightly above physiologically normal pressure of 10–20 mmHg, though greater gas injection into the anterior chamber does not necessarily lead to higher IOP.12 While it is the case in our study that the pressure at post-operative day 1 in the group that required a rebubble was physiologically normal and the group that did not require a rebubble were in the above physiologically normal range (>20 mmHg), there was not a significant difference between pressures in the two groups when other factors were taken into account in the regression. It should be noted that IOP in both groups fell within the physiologically normal level by 1 week, postoperatively. Schmeckenbacher et al26 concluded, similarly to our study in 2017, that IOP levels did not play a significant role in the partial detachment of the graft.
When DMEK was combined with phacoemulsification for triple procedures (DMEK and cataract surgery concurrently), we found that this did not have an effect on whether or not a patient would need a rebubble procedure. This is consistent with previous literature showing that doing the triple procedure does not increase adverse outcomes versus doing the two procedures separately.28 Patients with a well-centered graft in the week following DMEK surgery were found to need a rebubble procedure less often than those who had a graft that was not well-centered. A graft that overlaps with surrounding tissue and that does not allow the anterior portion of the Descemet graft to adhere to the posterior of the stroma has an increased likelihood to detach and require a rebubble.21
The final aspect that was taken into account was whether or not fluid and/or gas was let out of the anterior chamber following the procedure. This is often done so as to relieve undesirable high pressures, yet to find a balance to appropriately keep the graft attached to the overlying stroma.14,17,27 While surgical preference and technique is usually what influences whether or not a surgeon chooses to tap the eye to relieve pressure, our study concluded that it did not have a correlation with rebubble rates. This can give options to surgeons who prefer to let gas out of the anterior chamber in favor of lower IOP without necessarily affecting the status of adherence of the graft or the eventual outcome. In addition, this study showed that there was no difference in BCVA between the two groups at 3 months after the initial DMEK procedure, showing that use of a rebubble procedure might not necessarily result in worse outcomes.
Aside from the factors taken into account in this study, it is possible that other confounders could influence whether or not a rebubble is necessary, such as disease severity. While all of the patients in this study had FECD as their indication, we did not have patients with other indications included such as bullous keratopathy.20
Conclusion
We find that higher endothelial densities and a well-centered Descemet graft may correlate with fewer postoperative complications when performing DMEK. In addition, the decision by the surgeon on whether or not to remove gas from the anterior chamber following the procedure does not affect whether or not a patient will need a rebubble.
Disclosure
The authors report no conflicts of interest in this work.
References
Wacker K, McLaren JW, Amin SR, Baratz KH, Patel SV. Corneal high-order aberrations and backscatter in Fuchs’ endothelial corneal dystrophy. Ophthalmology. 2015;122(8):1645–1652. | ||
Ali M, Raghunathan V, Li JY, Murphy CJ, Thomasy SM. Biomechanical relationships between the corneal endothelium and Descemet’s membrane. Exp Eye Res. 2016;152:57–70. | ||
Wilson SE, Bourne WM. Fuchs’ dystrophy. Cornea. 1988;7:2–18. | ||
Maurice DM. The location of the fluid pump in the cornea. J Physiol. 1972;221(1):43–54. | ||
Melles GR. Posterior lamellar keratoplasty: DLEK to DSEK to DMEK. Cornea. 2006;25(8):879–881. | ||
Melles GR, Ong TS, Ververs B, van der Wees J. Descemet membrane endothelial keratoplasty (DMEK). Cornea. 2006;25(8):987–990. | ||
Anshu A, Price MO, Price FW Jr. Risk of corneal transplant rejection significantly reduced with Descemet’s membrane endothelial keratoplasty. Ophthalmology. 2012;119(3):536–540. | ||
Hamzaoglu EC, Straiko MD, Mayko ZM, Sales CS, Terry MA. The first 100 eyes of standardized Descemet stripping automated endothelial keratoplasty versus standardized Descemet membrane endothelial keratoplasty. Ophthalmology. 2015;122(11):2193–2199. | ||
Tourtas T, Laaser K, Bachmann BO, Cursiefen C, Kruse FE. Descemet membrane endothelial keratoplasty versus Descemet stripping automated endothelial keratoplasty. Am J Ophthalmol. 2012;153(6):1082–1090.e1082. | ||
Gorovoy MS. DMEK complications. Cornea. 2014;33(1):101–104. | ||
Ham L, van der Wees J, Melles GR. Causes of primary donor failure in Descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2008;145(4):639–644. | ||
Pilger D, Wilkemeyer I, Schroeter J, Maier AB, Torun N. Rebubbling in Descemet membrane endothelial keratoplasty: influence of pressure and duration of the intracameral air tamponade. Am J Ophthalmol. 2017;178:122–128. | ||
Yeh RY, Quilendrino R, Musa FU, Liarakos VS, Dapena I, Melles GR. Predictive value of optical coherence tomography in graft attachment after Descemet’s membrane endothelial keratoplasty. Ophthalmology. 2013;120(2):240–245. | ||
Price MO, Giebel AW, Fairchild KM, Price FW Jr. Descemet’s membrane endothelial keratoplasty: prospective multicenter study of visual and refractive outcomes and endothelial survival. Ophthalmology. 2009;116(12):2361–2368. | ||
Rodriguez-Calvo de Mora M, Groeneveld-van Beek EA, Frank LE, et al. Association between graft storage time and donor age with endothelial cell density and graft adherence after Descemet membrane endothelial keratoplasty. JAMA Ophthalmol. 2016;134(1):91–94. | ||
Stanzel TP, Ersoy L, Sansanayudh W, et al. Immediate postoperative intraocular pressure changes after anterior chamber air fill in Descemet membrane endothelial keratoplasty. Cornea. 2016;35(1):14–19. | ||
Maier AK, Gundlach E, Pilger D, et al. Rate and localization of graft detachment in Descemet membrane endothelial keratoplasty. Cornea. 2016;35(3):308–312. | ||
Brockmann T, Brockmann C, Maier AK, et al. Clinicopathology of graft detachment after Descemet’s membrane endothelial keratoplasty. Acta Ophthalmol. 2014;92(7):e556–e561. | ||
Monnereau C, Bruinsma M, Ham L, Baydoun L, Oellerich S, Melles GR. Endothelial cell changes as an indicator for upcoming allograft rejection following Descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2014;158(3):485–495. | ||
Baydoun L, Ham L, Borderie V, et al. Endothelial survival after Descemet membrane endothelial keratoplasty: effect of surgical indication and graft adherence status. JAMA Ophthalmol. 2015;133(11):1277–1285. | ||
Rock T, Bramkamp M, Bartz-Schmidt KU, Rock D, Yoruk E. Causes that influence the detachment rate after Descemet membrane endothelial keratoplasty. Graefe’s Arch Clin Exp Ophthalmol. 2015;253(12):2217–2222. | ||
Maier AK, Gundlach E, Schroeter J, et al. Influence of the difficulty of graft unfolding and attachment on the outcome in Descemet membrane endothelial keratoplasty. Graefe’s Arch Clin Exp Ophthalmol. 2015;253(6):895–900. | ||
Heindl LM, Bucher F, Caramoy A, Hos D, Matthaei M, Cursiefen C. Safety of donor tissue preparation and use of descemetoschisis and torn tissue in Descemet membrane endothelial keratoplasty. Cornea. 2014;33(10):e7–e9. | ||
Lass JH, Gal RL, Dontchev M, et al. Donor age and corneal endothelial cell loss 5 years after successful corneal transplantation. Specular microscopy ancillary study results. Ophthalmology. 2008;115(4):627–632.e628. | ||
Heinzelmann S, Huther S, Bohringer D, Eberwein P, Reinhard T, Maier P. Influence of donor characteristics on Descemet membrane endothelial keratoplasty. Cornea. 2014;33(6):644–648. | ||
Schmeckenbacher N, Frings A, Kruse FE, Tourtas T. Role of initial intraocular pressure in graft adhesion after Descemet membrane endothelial keratoplasty. Cornea. 2017;36(1):7–10. | ||
Guerra FP, Anshu A, Price MO, Giebel AW, Price FW. Descemet’s membrane endothelial keratoplasty: prospective study of 1-year visual outcomes, graft survival, and endothelial cell loss. Ophthalmology. 2011;118(12):2368–2373. | ||
Chaurasia S, Price FW Jr, Gunderson L, Price MO. Descemet’s membrane endothelial keratoplasty: clinical results of single versus triple procedures (combined with cataract surgery). Ophthalmology. 2014;121(2):454–458. | ||
Terry MA, Straiko MD, Veldman PB, et al. Standardized DMEK technique: reducing complications using prestripped tissue, novel glass injector, and sulfur hexafluoride (SF6) gas. Cornea. 2015;34(8):845–852. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.