Back to Journals » Clinical Ophthalmology » Volume 12
Influence of pupil dilation on predicted postoperative refraction and recommended IOL to obtain target postoperative refraction calculated by using third- and fourth-generation calculation formulas
Authors Teshigawara T ![]() , Meguro A
, Meguro A ![]() , Mizuki N
, Mizuki N
Received 3 May 2018
Accepted for publication 4 August 2018
Published 2 October 2018 Volume 2018:12 Pages 1913—1919
DOI https://doi.org/10.2147/OPTH.S172846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Takeshi Teshigawara,1–3 Akira Meguro,3 Nobuhisa Mizuki3
1Yokosuka Chuoh Eye Clinic, Yokosuka, Kanagawa, Japan; 2Tsurumi Chuoh Eye Clinic, Yokohama, Kanagawa, Japan; 3Department of Ophthalmology, Yokohama City University School of Medicine, Yokohama, Kanagawa, Japan
Purpose: To evaluate the influence of pupil dilation on predicted postoperative refraction (PPR) and recommended intraocular lens (IOL) power to obtain target postoperative refraction calculated by using the third- and fourth-generation IOL power calculation formulas with a new optical biometer.
Methods: This retrospective study included 162 eyes with cataract that underwent uneventful phacoemulsification with IOL implantation. PPR, recommended IOL power, anterior chamber depth (ACD), and lens thickness (LT) were measured pre- and post-pupil dilation. The change in PPR detected by using third-generation (Hoffer Q and SRK/T) and fourth-generation formulas (Haigis and Holladay 2) and the changes in ACD and LT were evaluated pre- and postdilation. The influence of dilation on the recommended IOL power calculated by each formula was analyzed.
Result: ACD and LT significantly changed from pre- to postdilation. The mean absolute change in PPR between pre- and postdilation was significantly higher for fourth-generation formulas compared with third-generation formulas. The change in PPR between pre- and postdilation showed a significantly positive correlation with change in ACD and a significantly negative correlation with change in LT with fourth-generation formulas, but not with third-generation formulas. The discrepancy rate of recommended IOL power between pre- and postdilation calculated by fourth-generation formulas was significantly higher than that calculated by third-generation formulas.
Conclusion: ACD and LT significantly changed by dilation. PPR and recommended IOL power significantly changed more by dilation when using fourth-generation formulas compared with third-generation formulas. Given the significant correlations of the change in PPR (between the pre- and postdilation) in the fourth-generation formulas and the changes in ACD and LT, the latter changes may be key in influencing dilation in the fourth-generation power calculation. Knowledge of the influence of dilation on fourth-generation formulas could help improve IOL calculation.
Keywords: pupil dilation, IOL power calculation, predicted postoperative refraction
Introduction
Until recently, both ophthalmologists and patients regarded removal of opaque lenses and correction of blurred vision to be the only goal of cataract surgery. Thus, a minor refractive error after cataract surgery was acceptable. However, as patients’ expectations of postoperative refractive outcome have increased in recent years, merely correcting blurred vision is no longer a satisfactory outcome because patients expect less dependency on glasses after surgery. In a sense, cataract surgery is now considered a part of refractive surgery. Therefore, there is a need for more precise prediction of postoperative refraction and intraocular lens (IOL) power calculation.1–3
As third-generation IOL calculation formulas such as SRK/T and Hoffer Q do not include anterior chamber depth (ACD) and lens thickness (LT) as variables, which can change between pre- and post-pupil dilation, biometric measurements are most likely performed either pre- and post-pupil dilation.4,5 However, fourth-generation IOL calculation formulas such as Haigis and Holladay 2 include both ACD and LT as variables.6–8
Sympathetic nerve stimulation causes relaxation and contraction of the ciliary and dilator muscles, respectively. When the ciliary muscle is relaxed, the suspensory ligaments are taut, which cause the lens to be thinner; thus, ACD becomes deeper. Although the degree of this phenomenon varies from patient to patient, the change in ACD may influence predicted postoperative refraction (PPR) and recommended IOL power calculated by power calculation formulas. However, in most cases, the effect of pupil dilation is still not considered serious enough. Given how important precise prediction of postoperative refraction is, it may be worth analyzing the influence of pupil dilation on PPR and recommended IOL by third- and fourth-generation IOL calculation formulas.
The purpose of this study was thus to evaluate the influence of pupil dilation on biometric measurement and recommended IOL power calculated by third- and fourth-generation formulas. The correlation between all variables was also analyzed.
Methods
This retrospective study comprises 162 eyes from 87 patients with cataract who underwent uneventful phacoemulsification with IOL implantation (SN60WF, Alcon Laboratories, Inc., Fort Worth, TX, USA) at Yokohama Tsurumi Chuoh Eye Clinic or Yokosuka Chuoh Eye Clinic in Japan. This study was approved by the ethical committees of both institutes (Yokohama Tsurumi Chuoh Eye Clinic and Yokosuka Chuoh Eye Clinic). Patients gave consent to review their medical records for this study. Patients with good quality IOL Master 700 (Carl Zeiss Meditec AG, Jena, Germany) measurements and postoperative best-corrected visual acuities higher than 20/40 were included in this study. Patients with a history of traumatic or uveitis cataracts, intraocular or corneal operation, and intra- or postoperative complications were excluded.
Preoperatively, biometric measurements of axial length (AL), ACD, and LT were obtained with IOL Master 700. PPR and recommended IOL power for SN60WF (Alcon Laboratories, Inc.) were calculated by third-generation (Hoffer Q and SRK/T) and fourth-generation (Haigis and Holladay 2) IOL calculation formulas. A constant of 119.0 for SN60WF provided by the User Group for Laser Interference Biometry was used. After the first measurement, topical tropicamide and phenylephrine (Midrin-P®, Santen, Osaka, Japan) was administered every 15 minutes until full pupil dilation. Then, the second measurement for the same variables was performed. All data collection adhered to the tenets of the Declaration of Helsinki. Patient provided written informed consent for their participation and publication of this study.
After all variables were measured or calculated pre- and post-pupil dilation, mean absolute change in PPR in each formula and mean change in ACD and LT were analyzed. Based on the above data, correlation between the change in PPR and the change in ACD and LT was also analyzed. We also analyzed the influence of pupil dilation on recommended IOL power.
Wilcoxon signed-rank test was used to compare ACD, LT, and PPR between pre- and post-pupil dilation and to compare changes in PPR pre- and post-pupil dilation between IOL power calculation formulas. Spearman’s rank-order correlation test was applied to assess the strength of association between ACD or LT pre-pupil dilation and changes in ACD or LT pre- and post-pupil dilation and to assess the strength of association between changes in PPR and changes in ACD or LT pre- and post-pupil dilation. A deviation of ≤±0.5D in recommended IOL power calculation was considered acceptable, and Fisher’s exact test was used to compare the coincidence of recommended IOL power calculated by third- and fourth-generation calculation formulas between pre- and post-pupil dilation. P<0.05 was considered statistically significant. All statistical analyses were performed using Bell Curve for Excel, version 1.03 (Social Survey Research Information Co., Ltd., Tokyo, Japan).
Results
The clinical characteristics of the 87 study patients are shown in Table 1. The mean patient age was 72.9±7.7 years (range: 51–87 years), and 39.6% of patients were male. For the 162 eyes assessed in this study, the average preoperative AL, ACD, and LT were 23.94±1.51 mm (range: 21.62–28.87 mm), 3.09±0.43 mm (range: 2.01–4.90 mm), and 4.61±0.45 mm (range: 3.44–6.28 mm), respectively.
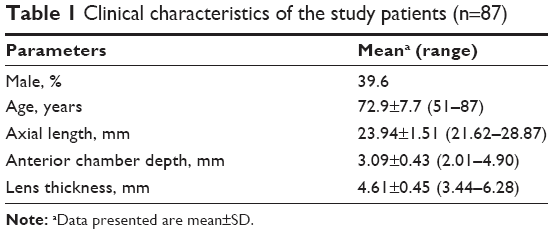 | Table 1 Clinical characteristics of the study patients (n=87) |
Table 2 shows the effect of pupil dilation on ACD and LT. Pupil dilation significantly affected ACD and LT (P<0.0001). The ACD increased and LT decreased after pupil dilation. Changes in ACD between pre- and post-pupil dilation showed a significantly positive correlation with the deepening of ACD predilation (Spearman’s rho = 0.24, P=0.0022), whereas changes in LT between pre- and post-pupil dilation did not show a correlation with the size of LT predilation (Spearman’s rho = −0.074, P=0.35) (Figure 1). On the contrary, AL did not show a significant change between pre- and postdilation. We assessed the mean absolute change between pre- and post-pupil dilation PPR among the four formulas (Table 3). The results showed that calculated values using Haigis (0.039±0.026) and Holladay 2 (0.038±0.023) were significantly higher than those using Hoffer Q (0.0072±0.0070) and SRK/T (0.0050±0.0055) (P<0.0001). Changes in pre- and postdilation PPR showed a significantly positive correlation with changes in pre- and postdilation ACD with both Haigis and Holladay 2 (Spearman’s rho = 0.95, P<0.0001), whereas this correlation was not observed for Hoffer Q and SRK/T (Spearman’s rho = −0.0084 and −0.016, respectively) (Figure 2). However, changes in pre- and postdilation PPR demonstrated a significantly negative correlation with the change in pre- and postdilation LT with both Haigis and Holladay 2 (Spearman’s rho = −0.45 and −0.42, respectively; P<0.0001); this correlation was not shown for Hoffer Q and SRK/T (Spearman’s rho = −0.096, −0.0078, respectively) (Figure 3).
 | Table 2 Effect of pupil dilation on axial length, anterior chamber depth, and lens thickness |
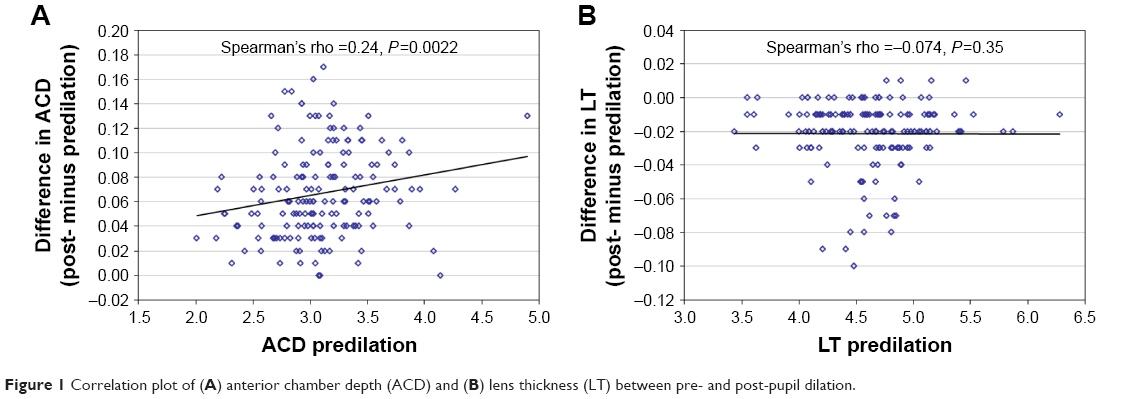 | Figure 1 Correlation plot of (A) anterior chamber depth (ACD) and (B) lens thickness (LT) between pre- and post-pupil dilation. |
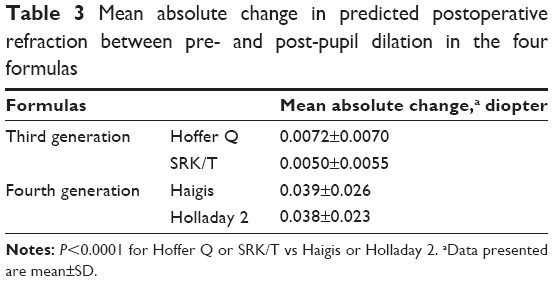 | Table 3 Mean absolute change in predicted postoperative refraction between pre- and post-pupil dilation in the four formulas |
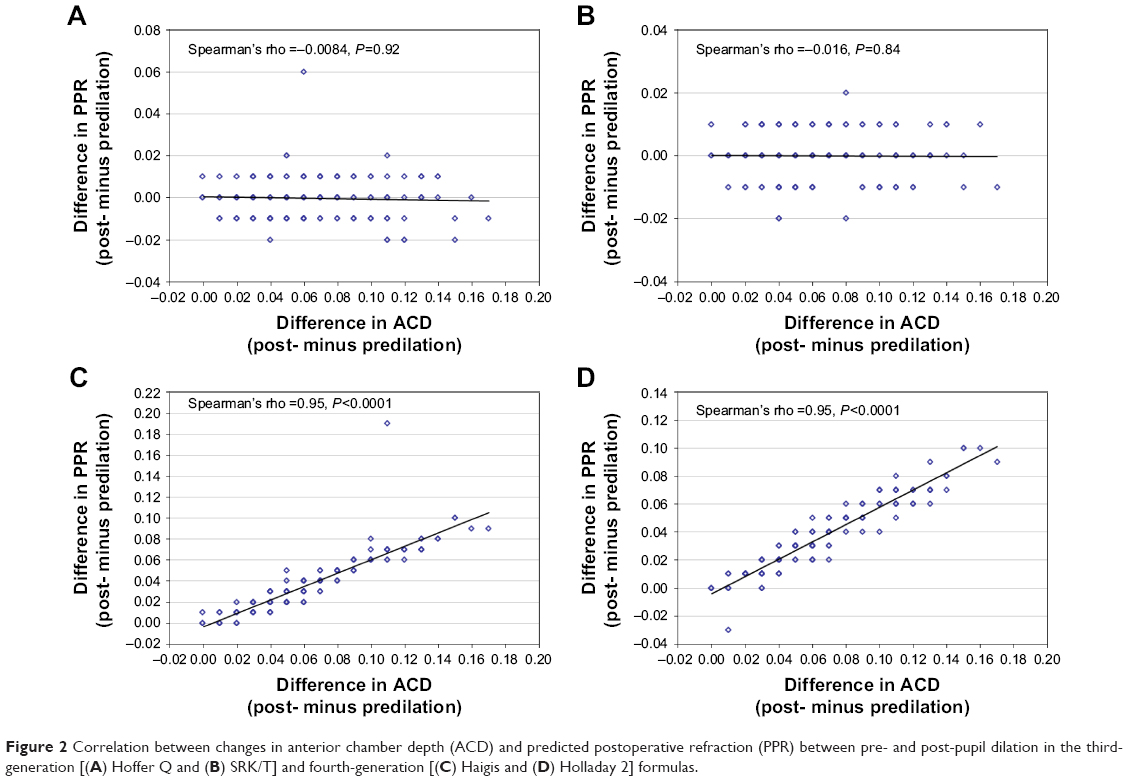 | Figure 2 Correlation between changes in anterior chamber depth (ACD) and predicted postoperative refraction (PPR) between pre- and post-pupil dilation in the third-generation [(A) Hoffer Q and (B) SRK/T] and fourth-generation [(C) Haigis and (D) Holladay 2] formulas. |
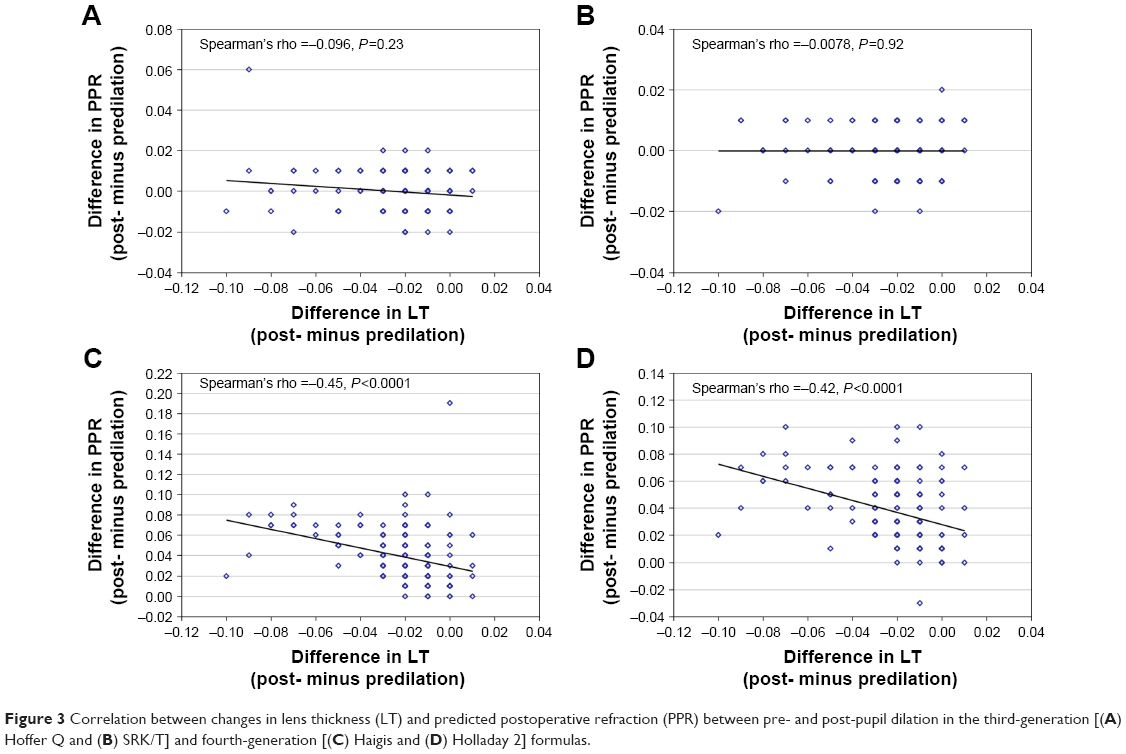 | Figure 3 Correlation between changes in lens thickness (LT) and predicted postoperative refraction (PPR) between pre- and post-pupil dilation in the third-generation [(A) Hoffer Q and (B) SRK/T] and fourth-generation [(C) Haigis and (D) Holladay 2] formulas. |
Table 4 shows the result of the coincidence of recommended IOL power between pre- and post-pupil dilation calculated by the same formulas. Recommended IOL power calculated using Haigis and Holladay 2 changed between pre- and postdilation in 7.4% and 8.6% of the assessed eyes, respectively, whereas Hoffer Q and SRK/T showed no or few changes (0.1% in Hoffer Q and 0.0% in SRK/T). The discrepancy rates of recommended IOL power between pre- and post-pupil dilation calculated by the fourth-generation formulas were significantly higher than those calculated by the third-generation formulas (P<0.0001).
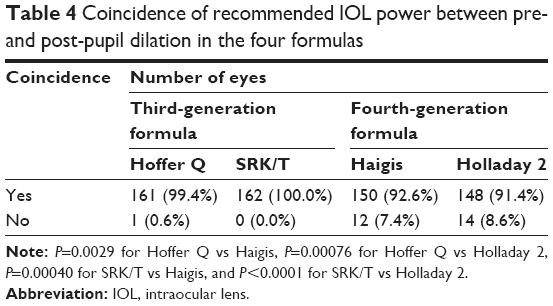 | Table 4 Coincidence of recommended IOL power between pre- and post-pupil dilation in the four formulas |
Discussion
Pupil dilation is an important part of preoperative ophthalmic examination. In addition, the choice of IOL calculation formula is vital to improve the accuracy of PPR. Although both third- and fourth-generation formulas are commonly used, physicians’ preference of these formulas varies from country to country. Thus far, only few studies have explored the influence of pupil dilation on biometric measurement, PPR, and recommended IOL power calculated by all available formulas. Even in regular clinical settings, it is challenging to assertively say whether the effect of pupil dilation is considered based on the available literature. Thus, the purpose of our study was to determine the possible influence of pupil dilation not only on ACD and LT but also on PPR and recommended IOL power calculated by third- and fourth-generation formulas.
A number of studies have reported the influence of pupil dilation on biometric measurements. Cheung et al,9 Huang et al,10 and Sheng et al11 found that AL was not significantly affected by pupil dilation. Arriola-Villalobos et al12 observed no change in corneal curvature radius after dilation, but Saitoh et al13 demonstrated that pupil dilation could influence corneal curvature radius. Khambhiphant et al14 showed that ACD was significantly influenced by pupil dilation. Similar results were reported by other studies.9–11,15 Thus, most studies found a significant influence of pupil dilation on ACD. We did not find any relevant publication that addressed the pupil’s influence on LT and/or the correlation between the change in ACD and LT and the change between pre- and post-pupil dilation PPR. Both correlations were analyzed in this research.
With regard to the influence of pupil dilation on IOL calculation formulas, the results of past studies vary depending on the kind of IOL calculation formula used. Khambhiphant et al14 found significant differences in ACD after dilation, while the AL, corneal curvature radius, and SRK/T-calculated PPR did not change significantly. They concluded that since SRK/T does not use ACD as a parameter, pupil dilation does not need to be taken into consideration for SRK/T, which is the most commonly used third-generation IOL calculation formula. Adler et al16 showed a similar result. Regarding the fourth-generation formulas, Rodriguez-Raton et al17 presented that pupil dilation caused significant increase in ACD, and PPR calculated by the Haigis formula also showed a significant change. They discussed how these changes resulted in recommended IOL power prediction according to the Haigis formula, which uses ACD to calculate the effective lens position (ELP). On the contrary, Arriola-Villalobos et al18 found that PPR calculated by the Holladay 2 formula did not significantly change between pre- and post-pupil dilation. However, the availability of published literature on the influence of pupil dilation on PPR and recommended IOL using fourth-generation formulas is still less than that of third-generation formulas.
As above, the influence of pupil dilation on PPR can vary from formula to formula, as IOL calculation formula includes different variables. Thus, it is important to know the components of third- and fourth-generation formulas to discuss the influence of pupil dilation on PPR and recommended IOL. Fyodorov and Kolinko formulated the first IOL calculation formula in 1967.19 Most third-generation theoretical IOL calculation formulas including SRK/T and Hoffer Q were formulated based on Fyodorov’s formula.
SRK/T was formulated by Retzlaff et al in 1990.4 Although the formula is very complicated, the key point to understanding it is that ELP is predicted based on corneal curvature radius and AL. The other third-generation formula – Hoffer Q – also uses corneal curvature radius and AL to estimate ELP.5 One of the major differences between these formulas is that while SRK/T uses the Pythagorean theorem, Hoffer Q uses trigonometric function to calculate ELP.
Fourth-generation IOL calculation formula is also a theoretical formula. Holladay 2 was introduced by Holladay in 1996.7 Although the details of the composition of Holladay 2 are not publicly available, the formula includes AL, corneal curvature radius, transverse corneal diameter, age, sex, and preoperative ACD to predict ELP. Haigis was published in 2004.6 Like Holladay 2, the details of Haigis are not very well-known; however, one of the major characteristic features of Haigis is the use of preoperative ACD and AL with a regression equation to calculate ELP, instead of the corneal curvature radius.
Thus, while third-generation formula does not use ACD to predict ELP, fourth-generation formula does. Therefore, as reported by several previous studies, it is clearly understood why PPR is not influenced by pupil dilation in the third-generation formula, rather only in the fourth-generation formula. Furthermore, it is yet unclear whether LT is included in the fourth-generation formula, although it did show a significant decrease between pre- and postdilation in our study.
In our study, we also determined the role of changes in ACD and LT after pupil dilation in third- and fourth-generation IOL calculation formulas. ACD increased and LT decreased significantly after pupil dilation. The mean absolute change in pre- and postdilation PPR by using fourth-generation formulas was significantly higher than that obtained by using third-generation formulas. Our study also presented that in the fourth-generation formulas, there was a significant positive correlation between the change in PPR and the change in ACD, whereas the change in PPR showed significant negative correlation with the change in LT. These correlations were not seen in third-generation formulas. This analysis indicated that ACD and LT can play important roles to calculate postoperative refraction in fourth-generation formulas, but not in third-generation formulas. Furthermore, in fourth-generation formulas, in 15.4% of cases, the change in PPR was large enough to change the recommended IOL power; this was not the case with third-generation formulas, which could affect the doctor’s selection of IOL.
Thus, IOL calculation using fourth-generation formulas was significantly influenced by pupil dilation. However, in reality, this influence is not necessarily taken into consideration when preoperative tests are performed. Given the fact that cataract surgeries are now considered a part of refractive surgery, in-depth knowledge of the influence of pupil dilation on fourth-generation formulas is vital to improve IOL calculation.
One of the limitations of this study is that we did not investigate the influence of pupil dilation on prediction error in refraction. This additional procedure may enable optimization of the constant for measurement with or without pupil dilation, which is likely more useful to improve the accuracy of IOL power calculation. We plan to include this investigation in our future research.
Acknowledgments
This study was presented on February 8, 2017, at the Meeting of Associated Research Vision of Ophthalmology Asia (ARVO-Asia), Brisbane Convention and Exhibition Centre, Brisbane, Australia.
Disclosure
All researchers involved in this study have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest. The authors report no conflicts of interest in this work.
References
Lee AC, Qazi MA, Pepose JS. Biometry and intraocular lens power calculation. Curr Opin Ophthalmol. 2008;19(1):13–17. | ||
Kielhorn I, Rajan MS, Tesha PM, Subryan VR, Bell JA. Clinical assessment of the Zeiss IOLMaster. J Cataract Refract Surg. 2003;29(3):518–522. | ||
Németh J, Fekete O, Pesztenlehrer N. Optical and ultrasound measurement of axial length and anterior chamber depth for intraocular lens power calculation. J Cataract Refract Surg. 2003;29(1):85–88. | ||
Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. | ||
Hoffer KJ, Kenneth J. The Hoffer Q formula: a comparison of theoretic and regression formulas. J Cataract Refract Surg. 1993;19(6):700–712. | ||
Haigis W. The Haigis formula. In: Shammas H, editor. Intraocular Lens Power Calculations. Thorofare, NJ: Slack; 2004:41–57. | ||
Holladay JT. Holladay IOL Consultant Computer Program. Houston, TX: Holladay IOL Consultant; 1996. | ||
Hoffer KJ. Clinical results using the Holladay 2 intraocular lens power formula. J Cataract Refract Surg. 2000;26(8):1233–1237. | ||
Cheung SW, Chan R, Cheng RC, Cho P. Effect of cycloplegia on axial length and anterior chamber depth measurements in children. Clin Exp Optom. 2009;92(6):476–481. | ||
Huang J, Mcalinden C, Su B, et al. The effect of cycloplegia on the lenstar and the IOLMaster biometry. Optom Vis Sci. 2012;89(12):1691–1696. | ||
Sheng H, Bottjer CA, Bullimore MA. Cycloplegia had no significant effect on IOL Master axial length measurements. Optom Vis Sci. 2004;81(1):27–34. | ||
Arriola-Villalobos P, Díaz-Valle D, Garzòn N, et al. Effect of pharmacologic pupil dilation on OLCR optical biometry measurements for IOL predictions. Eur J Ophthalmol. 2014;24(1):53–57. | ||
Saitoh K, Yoshida K, Hamatsu Y, Tazawa Y. Changes in the shape of the anterior and posterior corneal surfaces caused by mydriasis and miosis: detailed analysis. J Cataract Refract Surg. 2004;30(5):1024–1030. | ||
Khambhiphant B, Chatbunchachai N, Pongpirul K. The effect of pupillary dilatation on IOL power measurement by using the IOLMaster. Int Ophthalmol. 2015;35(6):853–859. | ||
Bakbak B, Koktekir BE, Gedik S, Guzel H. The effect of pupil dilation on biometric parameters of the Lenstar 900. Cornea. 2013;32(4):e21–e24. | ||
Adler G, Shahar J, Kesner R, et al. Effect of pupil size on biometry measurements using the IOLMaster. Am J Ophthalmol. 2015;159(5):940–944. | ||
Rodriguez-Raton A, Jimenez-Alvarez M, Arteche-Limousin L, Mediavilla-Peña E, Larrucea-Martinez I. Effect of pupil dilation on biometry measurements with partial coherence interferometry and its effect on IOL power formula calculation. Eur J Ophthalmol. 2015;25(4):309–314. | ||
Arriola-Villalobos P, Díaz-Valle D, Garzòn N, et al. Effect of pharmacologic pupil dilation on OLCR optical biometry measurements for IOL predictions. Eur J Ophthalmol. 2014;24(1):53–57. | ||
Fyodorov SN, Kolinko AI. Estimation of optical power of the intraocular lens. Vestn Ophthalmol. 1967;80:27–31. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.