Back to Journals » Patient Preference and Adherence » Volume 12
In-depth interviews of patients with primary immunodeficiency who have experienced pump and rapid push subcutaneous infusions of immunoglobulins reveal new insights on their preference and expectations
Authors Cozon GJN ![]() , Clerson P
, Clerson P ![]() , Dokhan A
, Dokhan A ![]() , Fardini Y, Pindi Sala T
, Fardini Y, Pindi Sala T ![]() , Crave JC
, Crave JC
Received 14 November 2017
Accepted for publication 3 February 2018
Published 26 March 2018 Volume 2018:12 Pages 423—429
DOI https://doi.org/10.2147/PPA.S156983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Grégoire Jacques Noël Cozon,1 Pierre Clerson,2 Annaïk Dokhan,3 Yann Fardini,2 Taylor Pindi Sala,4 Jean-Charles Crave4
1Department of Clinical Immunology and Rheumatology, Edouard Herriot Hospital, Lyon, France; 2Soladis Clinical Studies, Roubaix, France; 3KPL, Paris, France; 4Octapharma France, Boulogne, France
Purpose: Patients with primary immunodeficiency (PID) often receive immunoglobulin replacement therapy (IgRT). Physicians and patients have the choice between various methods of administration. For subcutaneous immunoglobulin infusions, patients may use an automated pump (P) or push the plunger of a syringe (rapid push [RP]). P infusions are performed once a week and last around 1 hour. RP decreases the duration of administration, but requires more frequent infusions.
Patients and methods: Eight out of 30 patients (coming from a single center) who had participated in the cross-over, randomized, open-label trial comparing P and RP participated in a focus group or underwent in-depth interviews. Patients had a long history of home-based subcutaneous immunoglobulin using P. The trial suggested that RP had slightly greater interference on daily life than P, but similar efficacy and better cost-effectiveness. When asked about the delivery method they had preferred, around one-third of patients pointed out RP rather than P. In-depth interviews may reveal unforeseen reasons for patients’ preferences.
Results: Interviews underlined the complexity of the relationship that the patients maintain with their disease and IgRT. Even if they recognized the genetic nature of the disease and claimed PID was a part of them, patients tried not to be overwhelmed by the disease. IgRT by P was well integrated in patients’ routine. By contrast, RP too frequently reminded the patients of their disease. In addition, some patients pointed out the difficulty of pushing the plunger due to the viscosity of the product. Coming back too frequently, RP was not perceived as time saving over a week. Long-lasting use of P could partly explain patients’ reasonable reluctance to change to RP.
Conclusion: In-depth interviews of PID patients highlighted unforeseen reasons for patients’ preference that the physician needs to explore during the shared medical decision-making process.
Keywords: in-depth interviews, primary immunodeficiency, patients’ expectations, preference, immunoglobulins, immunoglobulins replacement therapy, pump, rapid push, syringe
Introduction
Primary immunodeficiency (PID) patients are at a high risk of frequent and/or severe infections.1 By restoring sufficiently high serum levels of immunoglobulins (Igs), Ig replacement therapy (IgRT) reduces both the frequency and severity of infections,2 prevents complications such as bronchiectasis and improves the patient’s quality of life.3 Since PID is of genetic origin, IgRT is a lifelong therapy. During the last decades, IgRT has constantly improved, providing increasing autonomy to patients, thanks to home-based administration, causing very less disturbance to daily life activities. Until recently, patients had the choice between monthly intravenous immunoglobulin (IVIg) infusions by pump (P), either in hospital day-care units or at home, or weekly home-based subcutaneous immunoglobulin (SCIg) infusions using an automatic infusion P. SCIg by P takes 1–2 hours even with several catheters infusing several sites all at once. Most, but not all patients choose home-based self-administered SCIg rather than hospital-based IVIg, when given the choice.1 SCIg offers the advantages over IVIg of lower incidence of general reactions,3 better health-related quality of life, higher patient satisfaction4–6 and faster functional recovery with less time off work.7,8 Local reactions, however, are more frequent, although they tend to decrease with time and the patient’s experience.9
Recently, Shapiro10 reported his experience of rapid and manual administration of SCIg using a syringe, the so-called rapid push (RP), that decreases the duration of administration (around 10 minutes per injection at one or two sites simultaneously) but requires more frequent infusions. With this method, patients are expected to be less disturbed in their daily activities. They have to push the plunger of a 20 mL syringe with the potential advantage of being able to adapt the flow rate to their own comfort. We recently conducted the GAMEXPRESS study, which was the first randomized, comparative, open-label, cross-over, multicenter clinical trial aiming at comparing the impact of P and RP on the quality of life and patients’ satisfaction. The results are currently considered for publication. Briefly, 30 patients were randomly allocated to two sequences (P and then RP or RP and then P) for two 3-month periods. Convenience of both methods was evaluated on the quality of life (Life Quality Index [LQI]),11 SF-36 v2,12 satisfaction regarding IgRT (Treatment Satisfaction Questionnaire for Medication-11 [TSQM11]),13 burden of disease and of IgRT delivery method (Pictorial Representation of Illness and Self-Measure [PRISM])14,15 and costs. Patients were also asked to express their preference for one or the other method. The most important findings were: 1) RP had slightly greater interference on daily life than P (LQI factor 1 “treatment interference”); 2) no difference was found in other dimensions of LQI (therapy-related problems and therapy settings) or in SF-36 v2; 3) no difference was found in the incidence and severity of infections; 4) burden of disease and of IgRT delivery method was not different between the periods based on PRISM measures, and 5) after exclusion of direct costs linked to Igs, RP was highly cost-effective with a 70% reduction in indirect costs mainly driven by savings related to the material used for infusions. Additionally, when asked about the delivery method they preferred, around one-third of patients pointed out RP rather than P. These patients had no specific characteristics which could predict their preference.
To better understand patients’ expectations and preferences regarding IgRT, a series of in-depth interviews was conducted in a sample of those patients who participated in the cross-over study.
Patients and methods
Patients selected for this study were recruited from the GAMEXPRESS study that involved 30 patients. Nine patients were included in one center (Lyon). All nine patients were contacted by the physician of the center and invited to participate in the study. Eight patients accepted. Four patients anonymously were interviewed by a professional interviewer (AD). Each interview lasted 1 hour. In addition, four more patients accepted to participate in a focus group conducted by the same interviewer. The structures of interviews and of the focus group were similar as they were based on the same semi-directive approach. Patients were invited to talk about PID and its consequences on their lives, how they integrate IgRT in their daily life, advantages and inconveniences of P and RP, preference for P or RP, and expectations on potential future improvements of IgRT.
Interviews and the focus group were audio-recorded and verbatim transcribed for further analysis. French transcripts were translated into English and reviewed for validation. Content analysis was performed by examining major themes. Analyses output was sorted according to the main topics of the discussion: history of PID and its consequences, IgRT and its impact on daily life before the study, patients’ preference for P or RP after the study and expectations for future IgRT developments. Analyses were reviewed by the different authors to ensure consistency regarding the source data.
Before participation, patients were specifically informed of the study objectives and constraints and gave their written consent to participate in the study. According to the French Public Health Code (Article R1121-1 amended with decree 2017-884), approval of the local ethics committee is not required for surveys related to patient satisfaction. Patients data were processed in compliance with the law of Data Protection of January 6, 1978.
Results
The characteristics of interviewed patients are detailed in Table 1. Patients were between 31 and 80 years of age (mean ± SD 58±22). One out of the eight was a male. Four patients had a professional occupation and four were retired. Five patients started IgRT with hospital-based IVIg and three with home-based SCIg. All had a fairly long-standing history of SCIg by P. Results are presented according to the structure of the interview.
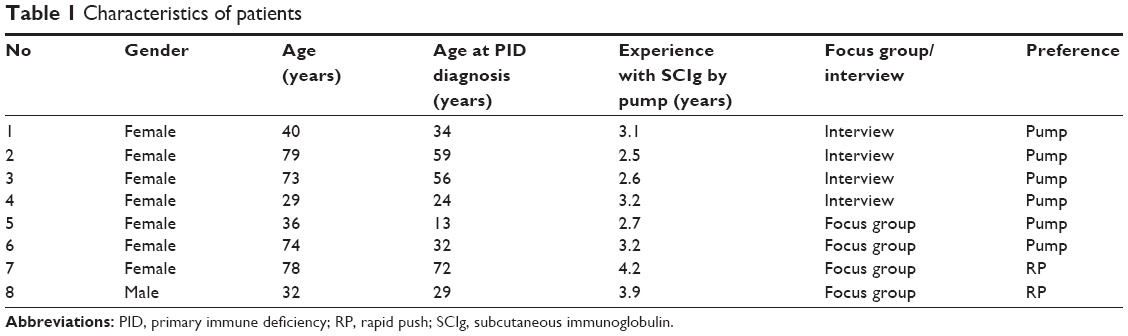 | Table 1 Characteristics of patients |
History of PID and its life consequences
Patients all had in common a long history of infections before PID diagnosis. All of them reported recurrent infections whose frequency (up to 15 episodes per year) and severity had impacted their quality of life, limited their activities, made them feel isolated or even jeopardized their vital prognosis. Infections more frequently affected the respiratory system (pneumonia, bronchitis), ear, nose and throat (otitis) or the digestive system (diarrhea), often since infancy. One patient reported nonspecific symptoms such as myalgia and chronic fatigue and remembered that her relatives did not understand.
They believed I was a fool. [P3]
The diagnosis was usually made after a more severe or long-lasting infection. Before that, however, patients had to go through exploration of allergies, adenoidectomy, tonsillectomy and more invasive surgical procedures until a protein electrophoresis was prescribed.
The patients were able to give clear explanations when asked about PID (“immune deficiency”, “lack of defenses”) and had no difficulty speaking about their disease with their relatives. Some patients did not feel the need or even avoided speaking about it:
I don’t speak about it, it is a part of me. [P8]
I don’t speak a lot about it. I live with it. [P6]
I only have one desire; to forget my disease. [P6]
One patient who was diagnosed in childhood perceived it as an injustice and tried to deny the disease as an adolescent:
I could not go to the swimming pool with my friends. [P4]
I could not travel with my classroom mates. [P6]
IgRT and its impact on daily life before the study
Patients reported they started a new life once being diagnosed with PID and being prescribed IgRT. All of them emphasized they decreased their consumption of antibiotics, quickly being almost free of infections, with improved quality of life and feeling reassured by being able to prevent infections:
It is a comfort I have never known before. [P2]
It changed my life. [P8] “I became normal.” [P6]
I prefer prevention to cure. [P1]
I feel enormously lucky to have this treatment. [P3]
Patients who started IgRT with hospital-based IVIg appreciated the autonomy given by home-based SCIg. IgRT at home allowed them to save time, travel expenses and days off work:
I no more had to drive to the hospital which took me 3 hours. [P6]
I have moved eighty miles far from Lyon and on Friday evening after my infusion, I was feeling too tired to drive to home. [P6]
I could do infusions on Saturday morning. [P5]
My employer did not appreciate that I had days off work every week. [P6]
In patients who began IgRT with IVIg, SCIg was perceived as less anxiety-inducing and helping preserving veins. SCIg were better tolerated than IVIg. For instance, one patient had a history of shock with IVIg. Interestingly, some patients reported they felt better protected with weekly than with monthly infusions.
Before entering the cross-over study, patients were accustomed to weekly home-based infusions using a P. They recognized that infusions once a week had some constraints, but stated they were well integrated in their schedule:
Nothing specific apart from one hour spent by week. I don’t think about it the rest of my time. [P4]
It is a one-hour long perturbation once a week but when the pump is in place, I can do other things. [P5]
I can work when doing my infusion at home. [P6]
Time devoted to infusion is not negligible and must be planned in advance. For a good compliance, patients have ritualized the time of infusions:
Always on the evening during supper. [P2]
On Saturday evening when I am watching TV; if I feel tired I can sleep longer on Sunday. [P7]
While watching TV or ironing. [P1]
However, weekly IgRT was a constraint when the patient was traveling for holidays:
It is complicated when going out for holidays. I need to anticipate immunoglobulins supply. [P6]
It is more bothersome when I have to travel, planning material, storing the product in a cool place. [P8]
Patients’ preference for P or RP after the study
Six out of eight patients preferred P. Automatization of the procedure was underlined:
No need to take care of the pump. [P7]
One can do other things with our two hands. [P5]
A good compromise between the duration and the disagreements of injection. [P4]
P was appreciated for saving time since patients had to prepare the material only once a week. Furthermore, patients agreed that infusions were painless:
I know myself and I know how to make the injections more comfortable. [P6]
In addition, patients emphasized that it was easier to postpone one P injection for a few days than to skip three RP injections during a 10-day vacation. Nonetheless, minor inconveniences were reported:
The pump must be reprogrammed when changing the battery. [P7]
In case the pump breaks, I cannot be sure of the volume injected. [P7]
Two patients (#7 and #8) preferred RP. Patient #8 found RP quicker, more flexible and cost-effective:
I have even more freedom than before. I choose RP for its quickness, its flexibility and its cost; no need to install the pump. [P8]
RP is a revolution; it takes only 5 minutes and therefore gives me more flexibility. [P8]
Injection is more comfortable. [P8]
Patient #7 stated that RP was “easy, efficacious and less expensive”. By contrast to P, RP had also the advantage of reliability like “avoiding breaks of P”:
I was relieved to live without pump; as an old woman, I feared that the pump would break down. [P7]
However, several patients outlined several disadvantages of the RP. Frequency of infusions was clearly a limitation:
I was sure I would be fond of RP but I was amazed to be tired to have to do infusions every other day. It is like a wake-up call that I am sick. I was sure not to come back to pump… but I did it. [P6]
Two times a week is too constraining. [P1]
I do not like to prick myself. I prefer to do it only once a week. [P2]
RP procedure itself appeared to be sometimes too bothersome compared to P:
I cannot do anything else during the injection. [P6]
It is sometimes difficult to push the plunger because the product of too viscous. [P6]
It is difficult to push the plunger regularly. [P7]
Strikingly, patients were not convinced RP would save time. The potential advantages of shorter infusions were not really perceived by the patients when adding the time of preparation and sanitization to the time of infusion:
When counting the time for preparation and asepsis, several infusions per week with RP take more time than one with pump and I am not sure we save time. [P6]
Table 2 summarizes the reasons for patients’ preference.
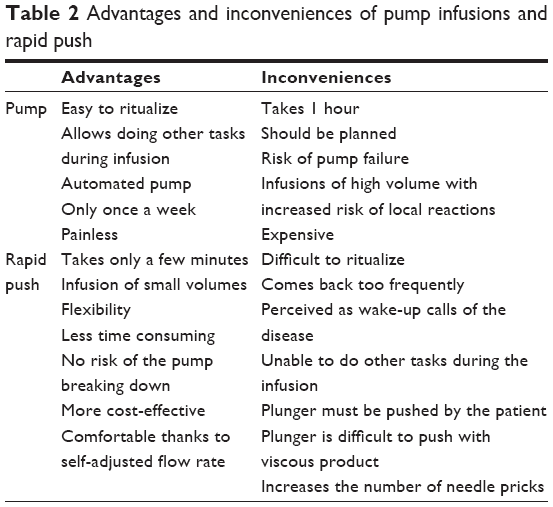 | Table 2 Advantages and inconveniences of pump infusions and rapid push |
Patients’ expectations for future developments
For RP, prefilled syringes would be perceived as an important improvement, shortening the time to prepare infusions. This would result in a gain of time over the week:
It could make me switch back to RP. [P6]
Additionally, patients expected less viscous products that would allow easier self-injections.
For P, patients asked for prefilled syringes and longer intervals between injections.
Discussion
We previously concluded from the GAMEXPRESS study that RP is a new, safe, easy-to-learn and well-accepted method that complements the physician’s armamentarium. Around one-third of patients declared preferring RP rather than P. Unfortunately, we were unable to individualize patients’ characteristics that could predict preference for P or RP. To go further into the understanding of the patients’ relationship with their disease and their preference for an infusion system, a qualitative study using individual interviews and a focus group was led with a sample of patients from the clinical study. Although qualitative studies are numerous, those relying on patients from a parental clinical study are relatively uncommon. Recently, a focus group-based study explored patient and physiotherapist perceptions of different approaches to rehabilitation following lumbar discectomy. The study was embedded within an external pilot and feasibility trial assessing different types of rehabilitation following lumbar discectomy. With this approach, the authors were able to highlight reasons behind their preference for rehabilitation interventions following surgery, such as their need to return to work.16 Clearly, this qualitative approach complements a clinical trial.
As far as we know, we report the first attempt to further explore the results of a treatment-based clinical trial in PID. In-depth interviews suggested that infusions every other day disturbed daily life, were perceived as too frequent wake-up calls of the disease, and did not necessarily decrease the time devoted to injections each week. This information could not have been captured through the initial clinical study settings.
Wake-up calls and rituals
Complaints about too frequent reminders of the disease reflect the relationship that patients maintain with PID. Even if they recognized the genetic nature of the disease and claimed PID was a part of them, patients tried not to be overwhelmed by the disease. Based on PRISM during the GAMEXPRESS study, patients tended to perceive IgRT as more intrusive than the disease, in their lives. According to the interviewees, IgRT has allowed them recovery of a normal life and PID appeared not to be at the forefront of their concerns. By contrast, coming back once a week, IgRT still disturbed patients’ daily life, even if well integrated in their routines. Apart from their role in improving compliance,17 rituals or routines may also be interpreted as attempts to delineate a precise time devoted to treatment, more exactly to specify the limits that must not be exceeded. Interestingly, some patients even performed other tasks such as preparing the meal or ironing during infusion. The integration of routine activities during infusion may be seen as a will not to exclusively dedicate time to the treatment and not to put their daily life on hold during infusions. For instance, in the case of chronic conditions, family rituals have been described as a means of ensuring a sense of normality.17 Patients included in the clinical trial and, therefore, interviewees, had a long history of IgRT, as the primary objective was to demonstrate the non-inferiority of a new method of administration, RP, compared to the well-established one, P. Most of them performed SCIg weekly infusions by P for a long time before entering the study. Whether the preference for P is due to a reasonable reluctance to break well-established routines or an inability to install new rituals with RP needs to be discussed. Regarding routine break, an alternative design with SCIg-naive participants could have obviated potential reluctance to change and this is certainly a limitation of the GAMEXPRESS study. Alternatively, it is also possible that new rituals either would require a habituation period exceeding 3 months or are difficult to install. Installing rituals is a long process and the study has broken routines for a 3-month period with RP. On the other hand, some interviewees expressed real difficulty to ritualize 10 minutes RP on every other day. Indeed, manual injection prevents doing manual activities (cooking, ironing and so on), but other nonmanual activities (watching TV and so on) remain possible. This raises a question regarding the routine activities that may best help to ritualize a treatment.
Interviewees had an average age of 58 years and some reported having difficulty pushing the plunger of the syringe. This could be partly due to insufficient patient education by the nurse or the physician. Almost all patients found that the product to be injected was too viscous. Indeed, high viscosity of some IgG solutions can make it difficult for the patient to handle the RP plunger. Patients included in the clinical trial used a low-viscosity product, Gammanorm® 165 mg/mL (Octapharma AG, Lachen, Switzerland), which has the lowest viscosity of all SCIg products available.19 More concentrated products, such as the 20% product, would require a smaller volume, but the extent to which it could mitigate higher viscosity-related issues during RP procedure is unknown. To our knowledge, no study has compared the difficulties of handling the RP plunger with different products.
Shared decision making
Patient reported a long history before the diagnosis of PID came as a relief. Indeed, the medical system performs poorly with patients seeking care for medically unexplained symptoms.18 To put a name on a disease means to delineate it, to define its limits and consequences, to find a clear explanation for recurrent infectious episodes and to explain at least a part of the mystery.20 It is then a way to confront the condition and to better adjust psychologically. Ultimately, the diagnosis is the opportunity to establish a confident relationship with the physician. Patient’s preferences should be taken into account when starting IgRT that will be a lifelong treatment. Patient adherence is of paramount importance. The patient should be given the choice of a hospital- or a home-based treatment, of self-administration or infusion done by a nurse, of intravenous or subcutaneous route, and now, of administration by P or by RP. Making a shared decision is encouraged by French health authorities.21 It implies providing complete information to the patient to help him/her consider the various possible options and express his/her preferences in order to make joint informed decision with plain acceptance of both parties. RP has been demonstrated to be a new, valuable option for IgRT. However, it will not be accepted or preferred by all patients. It could be proposed by the physician as an alternative to weekly infusions by P. The acceptance by the patient will depend on the relationship with his/her disease. Patients whose main concern is to forget or deny the disease could prefer less frequent, but longer infusions; those who have a peaceful relationship with their disease could appreciate shorter, but more frequent infusions. This information has not been captured by the scales used in our clinical study. This could explain why we were unable to characterize patients who would prefer RP or P. Only a deep and confident relationship between the patient and the physician would help to address these issues.
Strengths and limitations of the study
The key strength of the study was to give the opportunity for patients involved in a clinical study to openly and freely express their opinion on the object of the research in a framework not limited to the original study design. This study was limited by its small sample size, but was satisfying regarding the distribution observed in the study source population and the variety of opinions expressed. Due to its qualitative nature, generalization of the results is limited and must be cautiously made. The study revealed new elements to be taken into account when considering lifelong IgRT administration, which should help to develop and maintain a successful IgRT strategy for the patient.
Conclusion
In-depth interviews of a sample of patients who participated in a cross-over, randomized trial comparing the RP and P infusion of Igs in PID patients have underlined the complexity of the relationship that the patients maintain with their disease and IgRT. They also highlighted unforeseen reasons for patients’ preference that the physician needs to explore during the shared medical decision-making process.
Acknowledgments
This work was supported by Octapharma.
Disclosure
GJN Cozon is part of the scientific committee of the GAMEXPRESS study and earned fees from Octapharma. GJN Cozon was an investigator for the GAMEXPRESS study and has taken part in several scientific boards and also in several studies led by Octapharma. P Clerson and Y Fardini work as independent statisticians and earned fees from Octapharma to draft the manuscript. A Dokhan works as a professional patients’ interviewer and earned fees from Octapharma to lead the interviews. She has no other conflicts of interest to declare. T Pindi Sala and JC Crave are employees of Octapharma France, the funding provider of the study. The authors report no other conflicts of interest in this work.
References
Gardulf A. Immunoglobulin treatment for primary antibody deficiencies: advantages of the subcutaneous route. Biodrugs. 2007;21(2):105–116. | ||
Busse PJ, Razvi S, Cunningham-Rundles C. Efficacy of intravenous immunoglobulin in the prevention of pneumonia in patients with common variable immunodeficiency. J Allergy Clin Immunol. 2002;109(6):1001–1004. | ||
Gardulf A, Nicolay U. Replacement IgG therapy and self-therapy at home improve the health-related quality of life in patients with primary antibody deficiencies. Curr Opin Allergy Clin Immunol. 2006;6(6):434–442. | ||
Gardulf A, Bjorvell H, Andersen V, et al. Lifelong treatment with gammaglobulin for primary antibody deficiencies: the patients’ experiences of subcutaneous self-infusions and home therapy. J Adv Nurs. 1995;21(5):917–927. | ||
Nicolay U, Kiessling P, Berger M, et al. Health-related quality of life and treatment satisfaction in North American patients with primary immunedeficiency diseases receiving subcutaneous IgG self-infusions at home. J Clin Immunol. 2006;26(1):65–72. | ||
Gardulf A, Nicolay U, Math D, et al. Children and adults with primary antibody deficiencies gain quality of life by subcutaneous IgG self-infusions at home. J Allergy Clin Immunol. 2004;114(4):936–942. | ||
Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol. 2012;32(6):1180–1192. | ||
Shapiro RS. Why I use subcutaneous immunoglobulin (SCIG). J Clin Immunol. 2013;33(Suppl 2):S95–S98. | ||
Kobrynski L. Subcutaneous immunoglobulin therapy: a new option for patients with primary immunodeficiency diseases. Biologics. 2012;6:277–287. | ||
Shapiro R. Subcutaneous immunoglobulin therapy by rapid push is preferred to infusion by pump: a retrospective analysis. J Clin Immunol. 2010;30(2):301–307. | ||
Nicolay U, Haag S, Eichmann F, Herget S, Spruck D, Gardulf A. Measuring treatment satisfaction in patients with primary immunodeficiency diseases receiving lifelong immunoglobulin replacement therapy. Qual Life Res. 2005;14(7):1683–1691. | ||
Ware J, Snow K, Kosinski M. SF-36 Health Survey Manual and Interpretation Guide. Lincoln, RI: QualityMetric Inc; 2000. | ||
Bharmal M, Payne K, Atkinson MJ, Desrosiers MP, Morisky DE, Gemmen E. Validation of an abbreviated Treatment Satisfaction Questionnaire for Medication (TSQM-9) among patients on antihypertensive medications. Health Qual Life Outcomes. 2009;7:36. | ||
Buchi S, Buddeberg C, Klaghofer R, et al. Preliminary validation of PRISM (Pictorial Representation of Illness and Self Measure)–a brief method to assess suffering. Psychother Psychosom. 2002;71(6):333–341. | ||
Buchi S, Sensky T. PRISM: pictorial representation of illness and self measure. A brief nonverbal measure of illness impact and therapeutic aid in psychosomatic medicine. Psychosomatics. 1999;40(4):314–320. | ||
Rushton A, Heneghan NR, Heap A, White L, Calvert M, Goodwin PC. Patient and physiotherapist perceptions of rehabilitation following primary lumbar discectomy: a qualitative focus group study embedded within an external pilot and feasibility trial. BMJ Open. 2017;7(4):e015878. | ||
Crespo C, Santos S, Canavarro MC, Kielpikowski M, Pryor J, Féres-Carneiro T. Family routines and rituals in the context of chronic conditions: a review. Int J Psychol. 2013;48(5):729–746. | ||
Smith RC, Lein C, Collins C, et al. Treating patients with medically unexplained symptoms in primary care. J Gen Intern Med. 2003;18(6):478–489. | ||
Gardulf A. Clinical experiences in primary and secondary immunodeficiencies and immune-mediated conditions using Gammanorm®. Immunotherapy. 2016;8(5):633–647. | ||
Sexton S, Loflin R 3rd. The relief of getting a diagnosis. Am Fam Physician. 2009;80(11):1223. | ||
Haute Autorité de Santé. Patient et professionnels de santé: décider ensemble. Concept, aides destinées aux patients et impact de la décision médicale partagée Etat des lieux [French National Authority for Health. Concept, patient support and the impact of shared medical decision. Current status]. French National Authority for Health Location: Saint-Denis, France; 2013. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.