Back to Journals » Hepatic Medicine: Evidence and Research » Volume 12
Identifying High-Risk NASH Patients: What We Know so Far
Received 31 May 2020
Accepted for publication 24 July 2020
Published 21 August 2020 Volume 2020:12 Pages 125—138
DOI https://doi.org/10.2147/HMER.S265473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Marten Schulz, Frank Tacke
Department of Hepatology and Gastroenterology, Charité Universitätsmedizin Berlin, Campus Virchow-Klinikum (CVK) Und Campus Charité Mitte (CCM), Berlin, Germany
Correspondence: Marten Schulz Email [email protected]
Abstract: Steatosis is a condition of hepatic fat overload that is associated with overweight and the metabolic syndrome. Nonalcoholic fatty liver disease (NAFLD) has become the most common liver disease with a global impact on healthcare. A proportion of NAFLD patients develops nonalcoholic steatohepatitis (NASH), liver fibrosis, cirrhosis or hepatocellular carcinoma (HCC). Identifying patients at risk for potentially life-threatening complications is crucial in their prevention, surveillance and treatment. In addition to hepatic disease progression (cirrhosis, portal hypertension, HCC), NAFLD patients are also at risk of cardiovascular and metabolic diseases as well as extrahepatic malignancies. Liver fibrosis is related to morbidity and mortality in NASH patients, and biomarkers, imaging techniques (ultrasound, elastography, MRI) as well as liver biopsy help in diagnosing fibrosis. In this review, we discuss the tools for identifying patients at risk and their reasonable application in clinical routine in order to stratify prevention and treatment of this emerging disease.
Keywords: NAFLD, fibrosis, cirrhosis, hepatocellular carcinoma, elastography, liver-stiffness measurement
Epidemiology of Fatty Liver Disease
Nonalcoholic fatty liver disease (NAFLD) is a chronic disease characterized by excessive hepatocytic accumulation of triglycerides and subsequent steatosis. If inflammation and liver injury are also present, patients may develop nonalcoholic steatohepatitis (NASH) that can progress to liver fibrosis, cirrhosis and hepatocellular carcinoma (HCC). Steatosis can progress to NASH but also directly to liver fibrosis.1 The natural course of disease is variable: In a study of 108 NAFLD patients, 42% displayed progression of fibrosis while 18% had a regression of fibrosis within 6.6 years.1 Severity of fibrosis is a predictor of the subsequent need for liver transplantation and also of mortality.2 In a recent meta-analysis, biopsy-confirmed fibrosis was associated with liver-related morbidity and overall mortality during long-term follow-up in patients with NAFLD.3 Fibrosis is subclassified in early fibrosis (F0/1), significant fibrosis (F2), advanced fibrosis (F3) and cirrhosis (F4).4
NASH is strongly associated with the metabolic syndrome, a widespread cluster of conditions including central obesity, hypertriglyceridemia, reduced HDL-cholesterol, hypertension and impaired fasting glucose.5 Nevertheless, it can also be present in lean persons.6 NAFLD in lean persons is diagnosed in 10% to 20% of nonobese Americans and Caucasians. Suspected risk factors in this patient group include amongst others metabolic disorders such as visceral obesity, altered lipid turnover or decreased muscle mass.7 Two position papers, which are controversially discussed in the field, have recently proposed changing the name “NAFLD“ to “MAFLD“, ie metabolic associated fatty liver disease, in order to highlight the metabolic disorder aspect of the disease.8 NAFLD and NASH have to be distinguished from excessive alcohol consumption which is usually defined as daily intake of more than 20g/d in women and more than 30g/d in men4 and from secondary causes of steatosis such as parenteral nutrition or storage diseases.9
NAFLD is a common disease with a global prevalence of about 25% in adults and is in more than 50% associated with obesity.10 47% of NASH patients also have diabetes mellitus.10 Vice versa, more than 50% of patients with type 2 diabetes also have NAFLD.11 NASH prevalence is estimated to be around 6.45% in the general population.10 Some extent of fibrosis is present in more than 60% of patients with NAFLD.12
Fibrosis progression rates estimate that around 2% of American adults develop NASH cirrhosis, and these cirrhotic patients display an incidence of 1–2% per year of HCC development.13
NASH is also highly common in children and adolescents who are at risk of liver-related morbidity such as cirrhosis or liver cancer later in life.14,15 A recent population-based study in the UK found that one in five young people at the age of around 24 years has NAFLD and one in 40 has liver fibrosis.16 It has been shown that NASH already is the second leading cause of liver disease of patients awaiting liver transplantation in the US.17
Fibrosis, Cirrhosis and HCC: The Hepatic Complications of NAFLD
The risk of liver-related mortality increases exponentially with the stage of fibrosis (F0-F4).18 Recently, a large survey of primary care databases in Europe found a significantly increased risk of HCC and cirrhosis in patients with NAFLD and NASH. The risk was greater in patients with NASH compared to NAFLD and higher in patients with fibrosis.19 Hence diagnosis and grading of fibrosis and progression of fibrosis are immensely important in predicting disease outcome in NAFLD and NASH.
HCC incidence was found to be 2.4-12.8% in NASH cirrhosis and was lower than in controls with hepatitis C virus (HCV)-related cirrhosis.20 NAFLD-associated HCC is often diagnosed in more advanced tumor stages than in other underlying liver diseases such as HCV cirrhosis, possibly explaining the overall worse prognosis that was found in two cohort studies.21,22 Other studies comparing NAFLD with HCV cohorts, however, found similar mortalities.23,24
As fibrosis can derive directly from NAFLD without steatohepatitis,12 HCC development is not necessarily related to cirrhosis but can also be seen in early stages of NASH fibrosis25,26 or in NAFLD.10 A study of a cohort of US veterans with HCC found that 34.6% of patients with HCC and NAFLD had no evidence of cirrhosis.22 Accordingly, a systematic review by White et al found a majority of more than 70% of HCC patients to be cirrhotic.20 Guidelines recommend to screen patients with cirrhosis for HCC,27 which is the fifth most cancer worldwide.28 Given the high prevalence of NAFLD and the relatively small proportion of related HCC or liver-related mortality, optimal screening and follow-up strategies are still under debate.4,29
Identifying patients at risk for NAFLD and NASH related morbidity and mortality is crucial in defining surveillance and treatment strategies.
Comorbidities Associated with Increased Risk for NAFLD Progression
The progression of NAFLD is not only driven by lifestyle (eg nutrition, exercise), genetic risk factors and patient characteristics (eg age, male sex, obesity), but heavily impacted by comorbidities, particularly metabolic diseases30 as depicted in Figure 1.
 |
Figure 1 Risk factors for NAFLD progression. Sedentary lifestyle with over-alimentation, obesity and diabetes are the main risk factors that promote disease severity progression from simple steatosis to NASH, fibrosis (stages F1-F3) and cirrhosis. |
Diabetes was found to be an independent risk factor for progression to cirrhosis or HCC in NAFLD/NASH patients10,19 and screening for diabetes (by determining blood glucose, HbA1c or glucose tolerance test) is therefore considered mandatory in patients with NAFLD.4 Older age and iron overload may also predispose for HCC in NAFLD patients.31 Alcohol is another risk factor in patients who already have liver fibrosis. Heavy alcohol intake may accelerate fibrosis progression, and even moderate alcohol use may increase the risk of liver cancer in patients with advanced fibrosis.32
Extrahepatic Complications of NAFLD
Fatty liver disease patients are not only at risk of developing liver-related complications but also carry an increased risk of extrahepatic morbidity. Cardiovascular or cancer-related mortality can surpass liver-related death in NAFLD patients.33
Cardiovascular Disease
NAFLD and cardiovascular disease, which includes ischaemic heart disease and stroke, relate to common risk factors such as the metabolic syndrome, abdominal obesity, atherogenic dyslipidaemia, hypertension and hyperglycaemia.34 Therefore, an increased risk for cardiovascular disease is associated with NAFLD which is mediated by various mechanisms such as insulin resistance, systemic inflammation, oxidative stress and changes in the gut microbiota.35 Despite these joint pathomechanisms, Alexander et al could not find an association of NAFLD and acute myocardial infarction (AMI) or stroke in a large European cohort study,36 which warrants more research on identifying NAFLD patients at risk for AMI or stroke. Fatty liver disease has been associated with a higher likelihood of cardiovascular death than liver-related mortality.10,34 In biopsy-diagnosed NAFLD, all-cause, cardiovascular and liver-related mortality is elevated.37 Even at advanced fibrosis, the top causes for mortality are cardiovascular diseases and non-HCC malignancies, then followed by liver-related complications.38
Diabetes Mellitus
Patients with type 2 diabetes mellitus (T2DM) have a two- to threefold elevated mortality risk due to non-alcohol and non-virus-related chronic liver disease which is mainly attributable to NAFLD.39 The association of T2DM with NAFLD has been shown by examination of biochemical markers40 or non-invasive imaging.41 Ekstedt et al described higher risk of developing T2DM in NASH than in simple steatosis by histologic assessment.42 It is uncertain if currently available biomarkers for monitoring NAFLD severity or progression can be applied evenly on the especially vulnerable cohort of patients with NAFLD and T2DM.37
Chronic Kidney Disease
The prevalence of chronic kidney disease (CKD) is elevated in patients with fatty liver disease.43,44 It has been shown that in biopsy-diagnosed NAFLD, liver disease severity was associated with CKD stages.43,45 A meta-analysis by Musso et al found that NASH was associated with a higher prevalence and incidence of CKD than simple steatosis. Accordingly, advanced fibrosis was associated with a higher prevalence and incidence of CKD than non-advanced fibrosis.46 The relationship between NAFLD and CKD is not completely understood. However, mechanisms linking NAFLD and CKD such as an altered renin-angiotensin system activation, impaired antioxidant defense, and damaged lipogenesis are in the focus of further research.47
Extrahepatic Cancer
Extrahepatic malignancies are another leading cause for mortality in NAFLD patients.33 In a large longitudinal cohort study by Allen and colleagues, a nearly 2-fold increase in the risk of incident cancers in 4722 NAFLD patients was found over a period of 21 years. Malignancies other than in the liver were located in the uterus, stomach, pancreas and colon. Increased cancer risk was stronger associated with NAFLD than to obesity.48
Diagnostic Tools for Detection of High-Risk Patients
Genetic Factors
Genetic investigations revealed hereditary single-nucleotide polymorphisms (SNPs) that indicate an increased risk for NASH, fibrosis and cirrhosis in patients with NAFLD such as patatin-like phospholipase domain-containing protein 3 (PNPLA3) and transmembrane 6 superfamily member 2 (TM6SF2).49,50 In a meta-analysis by Singal and colleagues, an increased PNPLA3-related risk of HCC was found in patients with NASH or alcohol-related cirrhosis (OR 1.67, 95% CI 1.27–2.21).51 Donati et al demonstrated an association of the membrane-bound O-acyltransferase domain-containing 7 (MBOAT7) rs641738 variant with HCC in patients without cirrhosis.52 This variant increases the risk of liver inflammation and fibrosis and not only in NAFLD53 but also in hepatitis B54 and C.55 17β-Hydroxysteroid dehydrogenase 13 (HSD17B13) is an enzyme that has a critical role in the regulation of hepatic homeostasis since it promotes lipid accumulation in the liver. Therefore, it may have a role as a biomarker in patients with NAFLD.56 However, guidelines do not recommend testing of genetic polymorphisms for surveillance in NAFLD, since it is not cost-effective.4
Identifying NAFLD Patients with Liver Fibrosis
Histology
Diagnosing and staging liver fibrosis as the crucial prognostic factor can be achieved via biopsy or in a non-invasive way. Besides providing a reliable distinction between NAFLD and NASH and assessment of histological disease activity by scores such as the NAFLD activity score (NAS),57 biopsy is regarded as gold standard for fibrosis measurement.
Several histopathological fibrosis staging schemes according to different underlying diseases have been described. Commonly used scores are METAVIR58 and Ishak59 score which are primarily used in hepatitis B and C and Brunt score for NAFLD and NASH.60 These scores scale a visual accumulation of fibrous tissue from 0 to 4: F1: portal fibrosis without septa; F2: portal fibrosis with few septa between portal tracts or hepatic veins; F3: bridging septa between central and portal veins and F4: cirrhosis with regenerative nodules. Stage F2 and higher is commonly regarded as advanced fibrosis.
Since liver biopsies only display a small part of the liver, sampling error and intraobserver variation can occur.61 These limitations are a particular challenge in clinical trials evaluating anti-NASH drugs, as this lack of reliability can potentially affect the patient population (eg, introducing patients who do not properly meet study entry criteria) or misclassify fibrosis and treatment effects.62 In addition, biopsies cannot be easily repeated during follow-up of individual patients, because the procedure is comparatively expensive and, even though liver biopsy-related mortality is low, procedural risks such as bleeding, intestinal perforation and pneumothorax cannot be ruled out completely.63
Therefore, fibrosis measurement has shifted towards non-invasive techniques as first-line investigation. Non-invasive methods of assessing fibrosis in NAFLD and NASH patients include laboratory-based scores, blood tests, ultrasound, liver stiffness measurement via transient elastography (TE), shear wave elastography (SWE), point shear wave elastography (pSWE) and magnetic resonance elastography (MRE).
Scoring Systems
Several scores have been developed to determine the presence of fibrosis using clinical data and laboratory results (see Table 1). The overall idea of these scores is to integrate routine parameters of liver injury (eg transaminase activity, platelet count) and risk characteristics (eg obesity, age, diabetes).
 |
Table 1 Commonly Used Scores for NAFLD, NASH and Fibrosis |
Angulo et al showed that the NAFLD fibrosis score (NFS), that comprises age, albumin, aminotransferases, body mass index (BMI), blood glucose and platelet count, had a high negative predictive value (NPV) of 93% (at a low cut-off score) in excluding advanced fibrosis, while a high cut-off score had high positive predictive value for advanced fibrosis (90%).64 Other schemes such as Fib-4 score that encompasses age, aminotransferases and platelets or APRI (AST/platelet ratio) are used to exclude advanced fibrosis.65 The rather simple APRI score did show an inferior predictive value in NAFLD patients when compared to HCV patients and is therefore preferably used in this context.66 The BARD score is calculated by summing BMI, AST/ALT ratio and diabetes mellitus. Since it showed a high negative predictive value (≥95%) for the presence of advanced fibrosis, it can be used for excluding advanced fibrosis in NAFLD patients.67 A longitudinal study by Angulo and colleagues suggested that the mentioned four scores, especially NFS, can predict liver-related complications or death.68 In a recent cross-sectional study, FIB-4, APRI, and NFS detected advanced fibrosis and fibrosis progression in patients with NAFLD.69 However, all these scores have a limited ability to screen for fibrosis in the general population. In a large population-based analysis, higher scores from noninvasive scoring systems such as APRI, NFS or FIB-4 were associated with an increased risk of cirrhosis, but their predictive ability was very modest in the general population.70 Another novel score is the ADAPT Score. In addition to age, platelets and diabetes, the ADAPT algorithm also includes PRO-C3, a marker of type III collagen formation, that is an independent predictor of fibrosis stage in NAFLD.71
Novel Composite Tests and Biomarkers
More expensive blood tests for evaluating liver fibrosis are FibroTest (FT), Fibrometer and the Enhanced Liver Fibrosis Test (ELF).
As displayed in Table 2, FT includes α2-macroglobulin, apolipoprotein A1, haptoglobin, total bilirubin, and γ-glutamyl-transpeptidase (GGT). It was demonstrated that a lower FT cut-off of 0.30 had a 90% NPV for advanced fibrosis while a higher FT cut-off of 0.70 had a 73% positive predictive value for the presence of advanced fibrosis in NAFLD patients.72 Fibrometer is based on platelets, prothrombin index, aspartate aminotransferase, α2‐macroglobulin, hyaluronate, urea and age73 and has displayed a high accuracy of 91.4% applying to three diagnostic intervals (F0/1, F0/1/2, F2/3/4) in NAFLD patients.74 Enhanced Liver Fibrosis (ELF) test incorporates hyaluronic acid, tissue inhibitor of matrix metalloproteinases-1 and aminoterminal propeptide of procollagen type III. ELF test was shown to predict liver-related outcome in a cohort of patients with chronic liver disease including NAFLD.75 In a recent meta-analysis, ELF test exhibited a high sensitivity but limited specificity to exclude advanced and significant fibrosis in NAFLD patients when low cutoff parameters were applied. In a context of low disease prevalence, the use of higher cutoff scores was found to be associated with a more limited test performance.76 The NAFLD Diagnostic Panel contains adiponectin, resistin, glucose, M30, M65, Tissue inhibitor of metalloproteinases-1, ProCollagen 3 N-terminal peptide and hyaluronic acid. In the validation study, the panel displayed an AUROC of 0.80 for predicting any degree of fibrosis.77
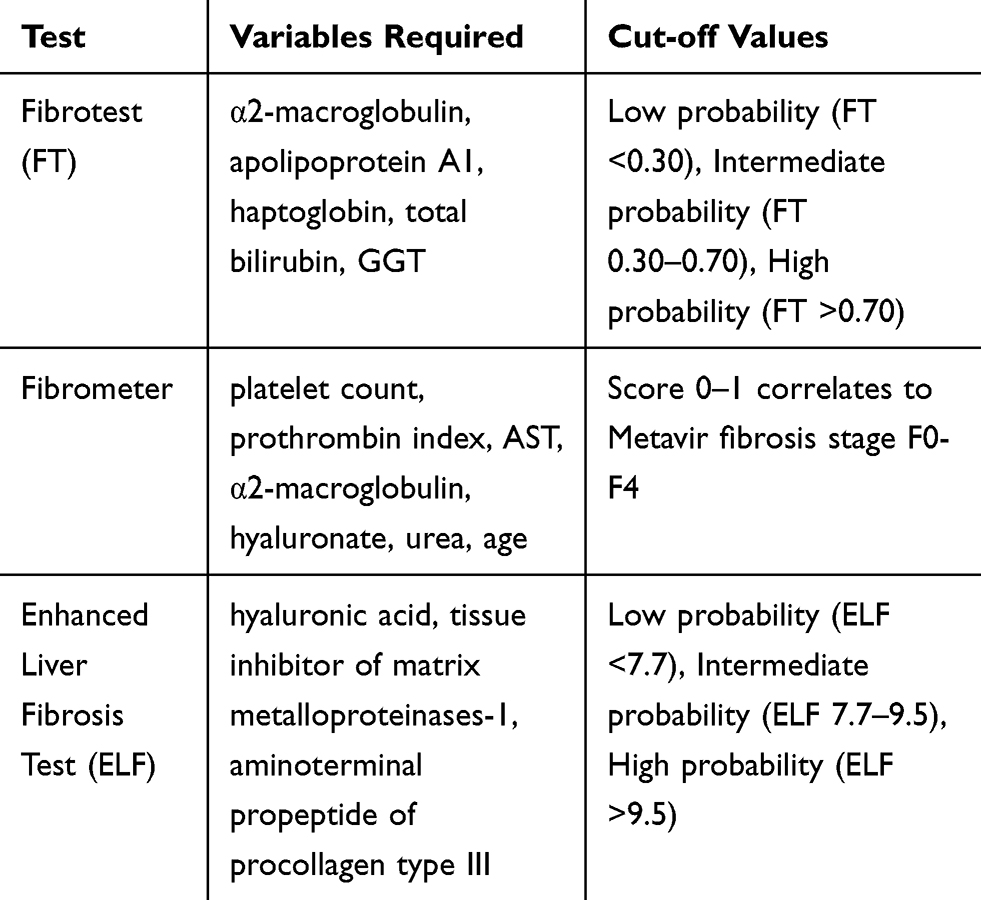 |
Table 2 Composite Fibrosis Tests |
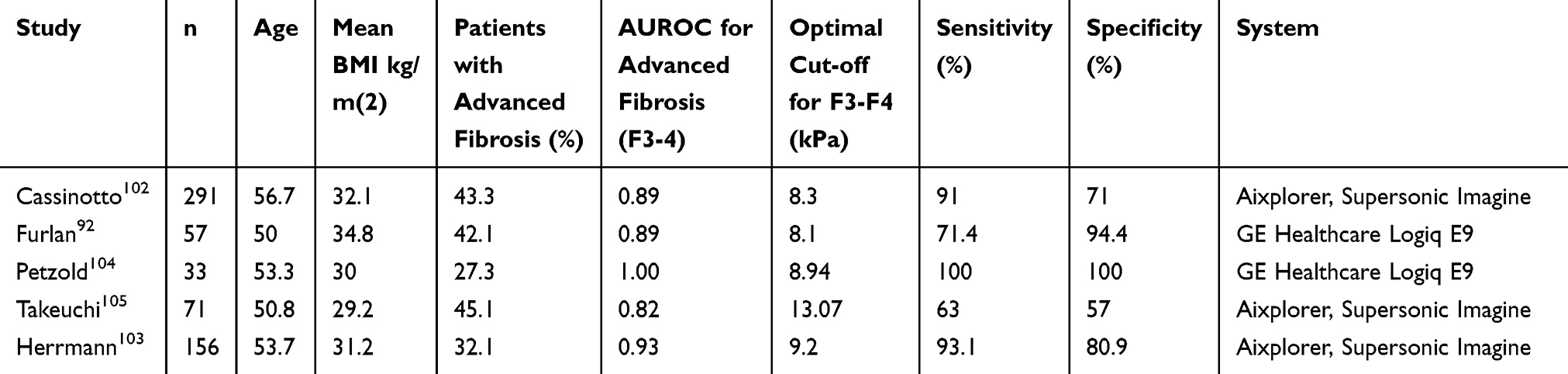 |
Table 3 SWE in Patients with NAFLD |
However, many of these tests include parameters that are not widely available and/or use patented (and thereby expensive) algorithms. In addition, non-invasive liver fibrosis assessment scores and blood tests have been usually tested and validated in heterogeneous, in part highly selected patient cohorts, often in the setting of underlying HCV infection and need further validation in different clinical frameworks in NAFLD patients. As it has been demonstrated for the ELF test, it can be necessary for the clinician to consider the local NAFLD prevalence in order to obtain the most accurate test result by a suitable test. Another potential biomarker in NAFLD is the macrophage activation marker sCD163,78 which has been linked to histological inflammatory activity and fibrosis in hepatitis C.79
The intestinal microbiome influences hepatic carbohydrate and lipid metabolism and also affects the balance between pro‐inflammatory and anti‐inflammatory effectors in the liver.80 Via various possible mechanisms such as the dysbiosis-induced dysregulation of gut endothelial barrier function leading to bacterial translocation and hepatic inflammation, the microbiome has been linked to chronic liver disease81 and changes in the gut microbiota composition have been linked to liver fibrosis82 or liver cancer83 and is a field of ongoing research. Another new approach in finding biomarkers associated with NAFLD and its complications are microRNAs (miRNAs)84 that control complementary target mRNAs at the post-transcriptional level and whose dysregulation has been shown to have a prognostic impact in NAFLD.85 In the future, miRNAs may serve as novel biomarkers for identifying NAFLD patients at risk. For example, miR-34a and miR-122 circulating levels were correlated with liver enzymes, inflammation activity and fibrosis score.86 Furthermore, miR-192 and miR-200a also have associations with NAFLD severity by histology87 indicating a potential role in risk stratification of NAFLD patients.
Liver Stiffness Measurement
In recent years, different ultrasound-based liver stiffness measurement (LSM) techniques have been introduced in clinical routines. These techniques differ in methodology, handling, interpretation and accuracy. All methods have to struggle with a poorer transmission of the ultrasound or mechanical beam in obese patients, which is common in NAFLD. Furthermore, possible confounders in LSM are influences on the viscoelasticity of the liver such as congestion, post-prandial hepatic hyperaemia and severe hepatitis (eg ALT levels >3 times the upper limit of normal).88 Cutoff values may vary among underlying disease and manufacturers of the different LSM systems.
Transient Elastography
A commonly used non-invasive technique is transient elastography (TE), which is the most widely studied liver stiffness measurement instrument. It can be operated by trained medical assistants but results should be interpreted by a physician who is aware of the patient´s clinical context. In TE, a probe (“M-probe”) emits a low‐energy 3.5 MHz ultrasound wave into the liver transcutaneously within a right intercostal space, and wave propagation is then evaluated by a receiver in the probe. Results are expressed in kilopascals (kPa) as depicted in Figure 2.
 |
Figure 2 Transient elastography: TE (Fibroscan, Echosens): Display of a reconstructed view of the wavefront that passes through the liver from the handheld probe (M or XL). Controlled attenuation parameter (CAP) measurement is displayed on the left-hand side. |
Using the M-probe, Castera et al found a failure rate of 3.1% in TE that was associated with the presence of obesity,89 failure rates in severely obese patients have been reported to be as high as 35%.90 In obese patients, a specific XL probe (2.5MHz) has shown improved reliability.91 It was demonstrated that TE has a good diagnostic accuracy in detecting advanced fibrosis (F3-F4) in NAFLD (using M- or XL-probe).92 A systematic review of nine studies including 1047 NAFLD patients (out of which in 854 patients the M-probe was used) showed a high accuracy in diagnosing F3 and F4 fibrosis (sensitivity 85% and 92% specificity 82% and 92%). For F2 fibrosis, accuracy was lower (79% sensitivity, 75% specificity).93 At a cutoff value of 7.9 kPa, the NPV for F3 or greater disease was found to be 97% (using M-probe), which indicates that TE is helpful in excluding advanced fibrosis.94 Recently, TE was reported to be an effective non-invasive tool in predicting survival in NAFLD patients.95
TE also allows to estimate the amount of hepatic fat by determination of so-called controlled attenuation parameter (CAP). A meta-analysis determined a cut-off for mild steatosis (>S0) of 248 dB/m and for moderate steatosis (>S1) of 268 dB/m.96 CAP has also shown good accuracy in patients with fibrosis.97
The possible interference of the excessive hepatic storage of fat in NAFLD patients in TE has been addressed by various studies. It has been shown that severe steatosis may bear a risk of false positive results in TE, especially in patients without advanced fibrosis.98 In contrary, Eddowes and colleagues found no affection of LSM due to steatosis.99 However, modification of TE results by simultaneous CAP measurement may reduce the possible confounder of severe steatosis.100
Shear Wave Elastography
Shear wave elastography (SWE) allows to perform an LSM via ultrasonography. Avoiding large vessels, a region of interest (ROI) at least 1 cm below the liver capsule is selected in a right intercostal position during a transient breath hold (see Figure 3). The shearwave propagation in the liver is visualized in the ultrasound picture and measured at least 3 times in m/s and can be converted to kPa.101
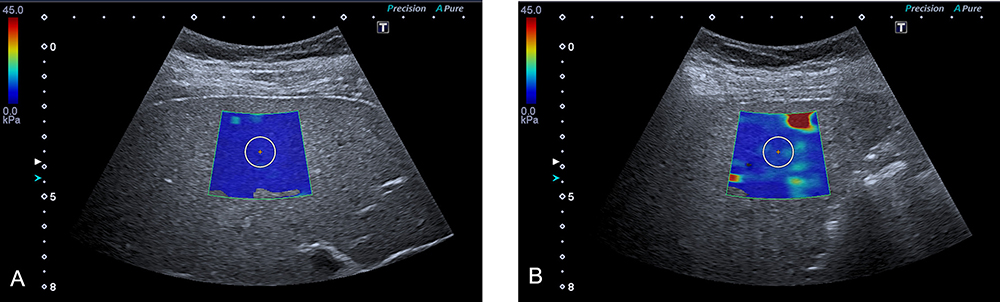 |
Figure 3 SWE measurement: SWE (Aplio 500, Toshiba) in a right intercostal probe position, LSM in region of interest (ROI) displayed by the white circle in the colour overlay style shearwave measurement. The color scale shows the distribution of the measured elasticity. (A) SWE in a 20-year-old female with a healthy liver; LSM was 4.9 kPa. (B) SWE in a 66-year-old female with NASH fibrosis; LSM was 8.7 kPa. |
As displayed in Table 3, data for SWE in NAFLD patients are limited. In the largest study on SWE in 291 NAFLD patients, Cassinotto et al found a good accuracy in detecting advanced fibrosis (AUROC 0.89). Using a cutoff of 8.3kPa, sensitivity was 91%, while at a cutoff of 10.7kPa specificity was 90% for F3 fibrosis or higher.102 A retrospective meta-analysis of 13 centers using the Aixplorer SWE equipment (SuperSonic Imagine, France) found comparable results for the NAFLD subgroup as displayed in Table 3.103
Point Shear Wave Elastography
Point shear wave elastography (pSWE) is another LSM technique that is also integrated in a conventional ultrasound machine. The operator must place a ROI in ultrasound imaging where the regional shear wave speed is measured (see Figure 4). While acoustic radiation force imaging (ARFI) is a similar technology introduced by Siemens, pSWE is offered by multiple manufacturers. If examination quality is insufficient, the user is warned by an estimation algorithm. A recent meta-analysis of Jiang et al included nine studies evaluating pSWE found an AUROC of 0.94 for advanced fibrosis and 0.86 for significant fibrosis detection, indicating a good accuracy for fibrosis assessment in NAFLD patients particularly in more advanced stages.106
However, shear wave based stiffness measurement has a varying procedural duration and requires sufficient training of operators in addition to availability of the appropriate equipment.107 Research on cost-effectiveness is needed.
 |
Figure 4 pSWE in NAFLD: pSWE (Arietta V70, HITACHI) in a right intercostal probe position, LSM in region of interest (ROI) displayed by the yellow box. (A) pSWE in a 35-year-old male with a healthy liver; LSM was 2.88 kPa. (B) pSWE in a 84-year-old male with NASH fibrosis; LSM was 9.28 kPa. |
Magnetic Resonance Elastography
In addition to a conventional MRI scanner, magnetic resonance elastography (MRE) requires special software and added hardware to generate mechanical waves. A continuous vibration of 60Hz is transmitted into the abdomen via a passive driver attached to the patient anterior to the liver. As depicted in Figure 5, resulting shear waves are then visualized and processed by a specialized software resulting in an elastogram, that quantitatively depicts stiffness of the liver. By drawing ROIs into the elastogram, stiffness can be assessed.108
 |
Figure 5 Magnetic resonance elastography: MRE of the liver in a cirrhotic patient. Stiffness measures are depicted in a quantitative colour scale. |
MRE is less operator-dependent than ultrasound-based LSM and the risk of failure in patients with severe obesity is lower.109 However, hepatic iron overload, ascites and overweight can be a reason for technical failure in MRE and failure rate was found to be 7.7% in a cohort of NASH patients.110 Patients with claustrophobia, extreme body weight or metal implants may be excluded from MRE. As additional examination during an MRE, proton density fat fraction (PDFF) allows to perform a quantification of fat accumulation in the liver (as CAP provides fat accumulation assessment in TE). Accuracy of PDFF is considered to be higher than in CAP.111 Comparing TE and MRE, Park et al described a superior fibrosis detection rate (for ≤F1 fibrosis) in MRE with an AUROC of 0.82 versus 0.67 in TE.112 In a recent study in 61 NAFLD patients comparing SWE, TE and MRE, MRE accuracy for detection of significant fibrosis was highest (AUROC 0.80, 0.77 and 0.85, respectively).92 Limitations for a wide utilization of MRE in NAFLD fibrosis assessment are mainly high costs and low accessibility.
Risk Stratification Strategies in NAFLD
As described above, multiple diagnostic tools for risk stratification of NAFLD patients with acceptable accuracies exist, especially for excluding advanced fibrosis. Given the high prevalence of NAFLD and its immense impact on morbidity and mortality now and in the future, determining diagnostic and surveillance strategies for NAFLD is crucial. In different healthcare systems, cost-effectiveness, allocation and availability of diagnostic instruments need to be investigated in detail in order to achieve the best possible outcome for patients that are at risk for NAFLD related complications. With new pharmacological treatment options on the horizon that will likely also have a substantial financial repercussion, it must be secured that as many patients who require special treatment or further surveillance are detected in the most reliable and cost-effective way.
Scores that include routine laboratory results and clinical aspects such as Fib-4 and NFS are widely available and inexpensive and could serve as the first (but preliminary) stratification in NAFLD patients. NFS alone and the combination of (increasingly available) TE and NFS has been shown to be cost-effective.113 Whether blood tests like FT or Fibrometer, TE, pSWE or SWE should be used, is often dependent on local technical equipment, reimbursement regulations and the operator expertise.
New pathways are currently being tested that combine different modalities. In a prospective longitudinal cohort study in a primary care setting, a 2-step algorithm (with FIB-4 and ELF) greatly improved the detection of advanced fibrosis and cirrhosis, while reducing unnecessary referrals to secondary care centers in patients with NAFLD.114 In a similar intention, combining LSM by transient elastography, CAP, and AST, designated FAST (FibroScan-AST), in a predictive model was efficient in identifying patients with progressing NASH.115
MRE is less expensive than liver biopsy108 but way more expensive than ultrasound based fibrosis assessment methods. Therefore, its utilization is currently restricted to selected cases such as severely obese patients in whom advanced fibrosis is suspected through scores or blood tests and patients with indeterminate results using other modalities. In the rising presence and availability of highly accurate non-invasive fibrosis measurement methods and large numbers of NAFLD patients, the role of liver biopsy needs to be discussed. Currently, including NAFLD patients in clinical trials requires liver biopsy,116 because histological endpoints are mandated by regulatory agencies as surrogates for clinically meaningful endpoints in NASH trials.117
Genetic testing and the search for new biomarkers in the intestinal flora are fields of ongoing research and are currently not part of clinical routine testing.
HCC Surveillance in NAFLD Patients
HCC surveillance is recommended and well established in cirrhotic patients. Its role in non-cirrhotic NAFLD patients is not fully determined. In patients with NAFLD and earlier stages of fibrosis, systematic screening is not recommended by guidelines but there is consensus that NAFLD patients with advanced fibrosis are at an increased risk for HCC development, and HCC screening may be performed in this cohort,27,118 especially when other risk factors such as older age, diabetes, iron overload, augmented alcohol consumption or genetic polymorphisms (such as PNPLA3 or MBOAT7) are present.
Alpha-fetoprotein (AFP) is the most widely tested tumor biomarker for HCC.27,118 AFP levels in patients with viral hepatitis of 20 ng/mL showed a good sensitivity but a low specificity, while at values above 200ng/mL the sensitivity was low with a high specificity.119 Using AFP as a screening tool for HCC did not improve mortality.120 The addition of AFP to screening ultrasound can lead to additional costs related to false-positive findings.121 Because of unclear cost-effectiveness and uncertainty regarding a potential benefit in mortality, AFP is not recommended as a surveillance parameter for HCC detection in NAFLD patients by European guidelines27 while American guidelines recommend screening ultrasound with or without AFP.122
Surveillance recommendations differ in the utilization of AFP, but agree on ultrasound as the essential screening tool at least every 6 months.27,123 Among chronic liver diseases, detection of HCC via operator-dependent ultrasound is especially challenging in NAFLD patients since these patients are often obese (which impairs visualization of focal lesions) and may display inhomogeneous steatosis.124 Given the high prevalence of NAFLD, high costs, limited availability and radiation exposure, MRI and computed tomography (CT) are currently not commonly recommended as surveillance imaging procedures.122 Nevertheless, in selected cohorts such as severely obese patients, MRI or CT can have a role in HCC surveillance.125 The recent best practice advices on HCC screening in NAFLD patients by the American Gastroenterological Association (AGA) recommend MRI or CT in case of suboptimal quality of screening ultrasound.118
Conclusions
Facing consequences of a sedentary lifestyle, overnutrition and rising numbers of obese patients, the growing burden of NAFLD is an urging challenge for individuals and healthcare systems. Since mortality affects only a minority of NAFLD patients, it is crucial to identify patients at risk. This will become even more important with more treatment options for NASH on the horizon.
A variety of invasive and non-invasive tests with high accuracy is already available for risk stratification in NAFLD. Further research on non-invasive biomarkers, that can be cost-effective in large cohorts, is needed for the early identification of high-risk NAFLD patients.
Acknowledgments
The authors thank S.R. Marticorena Garcia (Department of Radiology, Charité - Universitätsmedizin Berlin, Berlin, Germany) for providing an image of a MR elastography of the liver.
Disclosure
Professor Frank Tacke reports grants from BMS, Allergan, Inventiva, Galapagos, personal fees from Allergan, Pfizer, Novartis, NGM, Bayer, Gilead, Falk, Abbvie, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. McPherson S, Hardy T, Henderson E, Burt AD, Day CP, Anstee QM. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol. 2015;62(5):1148–1155. doi:10.1016/j.jhep.2014.11.034
2. Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology. 2015;149(2):389–397.e310. doi:10.1053/j.gastro.2015.04.043
3. Taylor RS, Taylor RJ, Bayliss S, et al. Association between fibrosis stage and outcomes of patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterology. 2020;158(6):1611–1625.e1612. doi:10.1053/j.gastro.2020.01.043
4. EASL-EASD-EASO. clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
5. Grundy SM, Brewer HB
6. Younossi ZM, Stepanova M, Negro F, et al. Nonalcoholic fatty liver disease in lean individuals in the United States. Medicine. 2012;91(6):319–327. doi:10.1097/MD.0b013e3182779d49
7. Younes R, Bugianesi E. NASH in lean individuals. Semin Liver Dis. 2019;39(1):86–95. doi:10.1055/s-0038-1677517
8. Eslam M, Sanyal AJ, George J. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014.e1991. doi:10.1053/j.gastro.2019.11.312
9. Keitel V, Vom Dahl S, Häussinger D. [Secondary causes of fatty liver disease - an update on pathogenesis, diagnosis and treatment strategies]. Dtsch Med Wochenschr. 2020;145(3):140–145. doi:10.1055/a-0965-9648. German.
10. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
11. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
12. Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol. 2015;13(4):
13. Diehl AM, Day C. Cause, pathogenesis, and treatment of nonalcoholic steatohepatitis. N Engl J Med. 2017;377(21):2063–2072. doi:10.1056/NEJMra1503519
14. Anderson EL, Howe LD, Jones HE, Higgins JP, Lawlor DA, Fraser A. The prevalence of non-alcoholic fatty liver disease in children and adolescents: a systematic review and meta-analysis. PLoS One. 2015;10(10):e0140908.
15. Crespo M, Lappe S, Feldstein AE, Alkhouri N. Similarities and differences between pediatric and adult nonalcoholic fatty liver disease. Metabolism. 2016;65(8):1161–1171. doi:10.1016/j.metabol.2016.01.008
16. Abeysekera KWM, Fernandes GS, Hammerton G, et al. Prevalence of steatosis and fibrosis in young adults in the UK: a population-based study. Lancet Gastroenterol Hepatol. 2020;5:295–305. doi:10.1016/S2468-1253(19)30419-4
17. Wong RJ, Aguilar M, Cheung R, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148(3):547–555. doi:10.1053/j.gastro.2014.11.039
18. Dulai PS, Singh S, Patel J, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology. 2017;65(5):1557–1565. doi:10.1002/hep.29085
19. Alexander M, Loomis AK, van der Lei J, et al. Risks and clinical predictors of cirrhosis and hepatocellular carcinoma diagnoses in adults with diagnosed NAFLD: real-world study of 18 million patients in four European cohorts. BMC Med. 2019;17(1):95. doi:10.1186/s12916-019-1321-x
20. White DL, Kanwal F, El-Serag HB. Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin Gastroenterol Hepatol. 2012;10(12):1342–1359.e1342. doi:10.1016/j.cgh.2012.10.001
21. Piscaglia F, Svegliati-Baroni G, Barchetti A, et al. Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: A multicenter prospective study. Hepatology. 2016;63(3):827–838. doi:10.1002/hep.28368
22. Mittal S, El-Serag HB, Sada YH, et al. Hepatocellular carcinoma in the absence of cirrhosis in united states veterans is associated with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2016;14(1):124–131.e121. doi:10.1016/j.cgh.2015.07.019
23. Hui JM, Kench JG, Chitturi S, et al. Long-term outcomes of cirrhosis in nonalcoholic steatohepatitis compared with hepatitis C. Hepatology. 2003;38(2):420–427. doi:10.1053/jhep.2003.50320
24. Bhala N, Angulo P, van der Poorten D, et al. The natural history of nonalcoholic fatty liver disease with advanced fibrosis or cirrhosis: an international collaborative study. Hepatology. 2011;54(4):1208–1216. doi:10.1002/hep.24491
25. Yasui K, Hashimoto E, Tokushige K, et al. Clinical and pathological progression of non-alcoholic steatohepatitis to hepatocellular carcinoma. Hepatol Res. 2012;42(8):767–773. doi:10.1111/j.1872-034X.2012.00986.x
26. Ertle J, Dechene A, Sowa JP, et al. Non-alcoholic fatty liver disease progresses to hepatocellular carcinoma in the absence of apparent cirrhosis. Int J Cancer. 2011;128(10):2436–2443. doi:10.1002/ijc.25797
27. EASL Clinical Practice. Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
28. Akinyemiju T, Abera S, Ahmed M, et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol. 2017;3(12):1683–1691. doi:10.1001/jamaoncol.2017.3055
29. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the study of liver diseases. Hepatology. 2018;67(1):328–357. doi:10.1002/hep.29367
30. Jarvis H, Craig D, Barker R, et al. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS Med. 2020;17(4):e1003100. doi:10.1371/journal.pmed.1003100
31. Dongiovanni P, Romeo S, Valenti L. Hepatocellular carcinoma in nonalcoholic fatty liver: role of environmental and genetic factors. World J Gastroenterol. 2014;20(36):12945–12955. doi:10.3748/wjg.v20.i36.12945
32. Ajmera VH, Terrault NA, Harrison SA. Is moderate alcohol use in nonalcoholic fatty liver disease good or bad? A critical review. Hepatology. 2017;65(6):2090–2099. doi:10.1002/hep.29055
33. Kim D, Kim WR, Kim HJ, Therneau TM. Association between noninvasive fibrosis markers and mortality among adults with nonalcoholic fatty liver disease in the United States. Hepatology. 2013;57(4):1357–1365. doi:10.1002/hep.26156
34. Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66(6):1138–1153. doi:10.1136/gutjnl-2017-313884
35. Targher G, Byrne CD, Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;
36. Alexander M, Loomis AK, van der Lei J, et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults. BMJ. 2019;367:l5367. doi:10.1136/bmj.l5367
37. Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62(1 Suppl):S4764. doi:10.1016/j.jhep.2014.12.012
38. Vilar-Gomez E, Calzadilla-Bertot L, Wai-Sun Wong V, et al. Fibrosis severity as a determinant of cause-specific mortality in patients with advanced nonalcoholic fatty liver disease: a multi-national cohort study. Gastroenterology. 2018;155(2):443–457.e417. doi:10.1053/j.gastro.2018.04.034
39. Zoppini G, Fedeli U, Gennaro N, Saugo M, Targher G, Bonora E. Mortality from chronic liver diseases in diabetes. Am J Gastroenterol. 2014;109(7):1020–1025. doi:10.1038/ajg.2014.132
40. Balkau B, Lange C, Vol S, Fumeron F, Bonnet F. Nine-year incident diabetes is predicted by fatty liver indices: the French D.E.S.I.R. study. BMC Gastroenterol. 2010;10:56. doi:10.1186/1471-230X-10-56
41. Park SK, Seo MH, Shin HC, Ryoo JH. Clinical availability of nonalcoholic fatty liver disease as an early predictor of type 2 diabetes mellitus in Korean men: 5-year prospective cohort study. Hepatology. 2013;57(4):1378–1383. doi:10.1002/hep.26183
42. Ekstedt M, Franzén LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology. 2006;44(4):865–873. doi:10.1002/hep.21327
43. Machado MV, Gonçalves S, Carepa F, Coutinho J, Costa A, Cortez-Pinto H. Impaired renal function in morbid obese patients with nonalcoholic fatty liver disease. Liver Int. 2012;32(2):241–248. doi:10.1111/j.1478-3231.2011.02623.x
44. Yasui K, Sumida Y, Mori Y, et al. Nonalcoholic steatohepatitis and increased risk of chronic kidney disease. Metabolism. 2011;60(5):735–739. doi:10.1016/j.metabol.2010.07.022
45. Yilmaz Y, Alahdab YO, Yonal O, et al. Microalbuminuria in nondiabetic patients with nonalcoholic fatty liver disease: association with liver fibrosis. Metabolism. 2010;59(9):1327–1330. doi:10.1016/j.metabol.2009.12.012
46. Musso G, Gambino R, Tabibian JH, et al. Association of non-alcoholic fatty liver disease with chronic kidney disease: a systematic review and meta-analysis. PLoS Med. 2014;11(7):e1001680. doi:10.1371/journal.pmed.1001680
47. Marcuccilli M, Chonchol M. NAFLD and chronic kidney disease. Int J Mol Sci. 2016;17(4):562. doi:10.3390/ijms17040562
48. Allen AM, Hicks SB, Mara KC, Larson JJ, Therneau TM. The risk of incident extrahepatic cancers is higher in non-alcoholic fatty liver disease than obesity - A longitudinal cohort study. J Hepatol. 2019;71(6):1229–1236. doi:10.1016/j.jhep.2019.08.018
49. Anstee QM, Day CP. The genetics of nonalcoholic fatty liver disease: spotlight on PNPLA3 and TM6SF2. Semin Liver Dis. 2015;35(3):270–290. doi:10.1055/s-0035-1562947
50. Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet. 2008;40(12):1461–1465. doi:10.1038/ng.257
51. Singal AG, Manjunath H, Yopp AC, et al. The effect of PNPLA3 on fibrosis progression and development of hepatocellular carcinoma: a meta-analysis. Am J Gastroenterol. 2014;109(3):325–334. doi:10.1038/ajg.2013.476
52. Donati B, Dongiovanni P, Romeo S, et al. MBOAT7 rs641738 variant and hepatocellular carcinoma in non-cirrhotic individuals. Sci Rep. 2017;7(1):4492. doi:10.1038/s41598-017-04991-0
53. Mancina RM, Dongiovanni P, Petta S, et al. The MBOAT7-TMC4 variant rs641738 increases risk of nonalcoholic fatty liver disease in individuals of European descent. Gastroenterology. 2016;150(5):1219–1230.e1216. doi:10.1053/j.gastro.2016.01.032
54. Thabet K, Chan HLY, Petta S, et al. The membrane-bound O-acyltransferase domain-containing 7 variant rs641738 increases inflammation and fibrosis in chronic hepatitis B. Hepatology. 2017;65(6):1840–1850. doi:10.1002/hep.29064
55. Thabet K, Asimakopoulos A, Shojaei M, et al. MBOAT7 rs641738 increases risk of liver inflammation and transition to fibrosis in chronic hepatitis C. Nat Commun. 2016;7:12757. doi:10.1038/ncomms12757
56. Su W, Mao Z, Liu Y, et al. Role of HSD17B13 in the liver physiology and pathophysiology. Mol Cell Endocrinol. 2019;489:119–125. doi:10.1016/j.mce.2018.10.014
57. Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–1321. doi:10.1002/hep.20701
58. Bedossa P, Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology. 1996;24(2):289–293. doi:10.1002/hep.510240201
59. Ishak K, Baptista A, Bianchi L, et al. Histological grading and staging of chronic hepatitis. J Hepatol. 1995;22(6):696–699. doi:10.1016/0168-8278(95)80226-6
60. Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-Tetri BA, Bacon BR. Nonalcoholic steatohepatitis: a proposal for grading and staging the histological lesions. Am J Gastroenterol. 1999;94(9):2467–2474. doi:10.1111/j.1572-0241.1999.01377.x
61. Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am J Gastroenterol. 2002;97(10):2614–2618. doi:10.1111/j.1572-0241.2002.06038.x
62. Davison BA, Harrison SA, Cotter G, et al. Suboptimal reliability of liver biopsy evaluation has implications for randomized clinical trials. J Hepatol. 2020. doi:10.1016/j.jhep.2020.06.025
63. Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD. Liver biopsy. Hepatology. 2009;49(3):1017–1044. doi:10.1002/hep.22742
64. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
65. McPherson S, Stewart SF, Henderson E, Burt AD, Day CP. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut. 2010;59(9):1265–1269. doi:10.1136/gut.2010.216077
66. Peleg N, Issachar A, Sneh-Arbib O, Shlomai A. AST to platelet ratio index and fibrosis 4 calculator scores for non-invasive assessment of hepatic fibrosis in patients with non-alcoholic fatty liver disease. Dig Liver Dis. 2017;49(10):1133–1138. doi:10.1016/j.dld.2017.05.002
67. Harrison SA, Oliver D, Arnold HL, Gogia S, Neuschwander-Tetri BA. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut. 2008;57(10):1441–1447. doi:10.1136/gut.2007.146019
68. Angulo P, Bugianesi E, Bjornsson ES, et al. Simple noninvasive systems predict long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology. 2013;145(4):782–789.e784. doi:10.1053/j.gastro.2013.06.057
69. Siddiqui MS, Yamada G, Vuppalanchi R, et al. Diagnostic accuracy of noninvasive fibrosis models to detect change in fibrosis stage. Clin Gastroenterol Hepatol. 2019;17(9):1877–1885.e1875. doi:10.1016/j.cgh.2018.12.031
70. Hagström H, Talbäck M, Andreasson A, Walldius G, Hammar N. Ability of noninvasive scoring systems to identify individuals in the population at risk for severe liver disease. Gastroenterology. 2020;158(1):200–214.
71. Daniels SJ, Leeming DJ, Eslam M, et al. ADAPT: an algorithm incorporating PRO-C3 accurately identifies patients with NAFLD and advanced fibrosis. Hepatology. 2019;69(3):1075–1086. doi:10.1002/hep.30163
72. Ratziu V, Massard J, Charlotte F, et al. Diagnostic value of biochemical markers (FibroTest-FibroSURE) for the prediction of liver fibrosis in patients with non-alcoholic fatty liver disease. BMC Gastroenterol. 2006;6:6. doi:10.1186/1471-230X-6-6
73. Cales P, Oberti F, Michalak S, et al. A novel panel of blood markers to assess the degree of liver fibrosis. Hepatology. 2005;42(6):1373–1381. doi:10.1002/hep.20935
74. Cales P, Laine F, Boursier J, et al. Comparison of blood tests for liver fibrosis specific or not to NAFLD. J Hepatol. 2009;50(1):165–173. doi:10.1016/j.jhep.2008.07.035
75. Parkes J, Roderick P, Harris S, et al. Enhanced liver fibrosis test can predict clinical outcomes in patients with chronic liver disease. Gut. 2010;59(9):1245–1251. doi:10.1136/gut.2009.203166
76. Vali Y, Lee J, Boursier J, et al. Enhanced liver fibrosis test for the non-invasive diagnosis of fibrosis in patients with NAFLD: A systematic review and meta-analysis. J Hepatol. 2020;73:252–262. doi:10.1016/j.jhep.2020.03.036
77. Younossi ZM, Page S, Rafiq N, et al. A biomarker panel for non-alcoholic steatohepatitis (NASH) and NASH-related fibrosis. Obes Surg. 2011;21(4):431–439. doi:10.1007/s11695-010-0204-1
78. Kazankov K, Barrera F, Møller HJ, et al. The macrophage activation marker sCD163 is associated with morphological disease stages in patients with non-alcoholic fatty liver disease. Liver Int. 2016;36(10):1549–1557. doi:10.1111/liv.13150
79. Lund Laursen T, Brøckner Siggard C, Kazankov K, et al. Rapid and persistent decline in soluble CD163 with successful direct-acting antiviral therapy and associations with chronic hepatitis C histology. Scand J Gastroenterol. 2018;53(8):986–993. doi:10.1080/00365521.2018.1481996
80. Kolodziejczyk AA, Zheng D, Shibolet O, Elinav E. The role of the microbiome in NAFLD and NASH. EMBO Mol Med. 2019;11:2. doi:10.15252/emmm.201809302
81. Safari Z, Gérard P. The links between the gut microbiome and non-alcoholic fatty liver disease (NAFLD). Cell Mol Life Sci. 2019;76(8):1541–1558. doi:10.1007/s00018-019-03011-w
82. De Minicis S, Rychlicki C, Agostinelli L, et al. Dysbiosis contributes to fibrogenesis in the course of chronic liver injury in mice. Hepatology. 2014;59(5):1738–1749. doi:10.1002/hep.26695
83. Yoshimoto S, Loo TM, Atarashi K, et al. Obesity-induced gut microbial metabolite promotes liver cancer through senescence secretome. Nature. 2013;499(7456):97–101. doi:10.1038/nature12347
84. Vincent R, Sanyal A. Recent advances in understanding of NASH: microRNAs as both biochemical markers and players. Curr Pathobiol Rep. 2014;2(3):109–115. doi:10.1007/s40139-014-0049-8
85. Dongiovanni P, Meroni M, Longo M, Fargion S, Fracanzani AL. miRNA signature in NAFLD: a turning point for a non-invasive diagnosis. Int J Mol Sci. 2018;19:12. doi:10.3390/ijms19123966
86. Cermelli S, Ruggieri A, Marrero JA, Ioannou GN, Beretta L. Circulating microRNAs in patients with chronic hepatitis C and non-alcoholic fatty liver disease. PLoS One. 2011;6(8):e23937. doi:10.1371/journal.pone.0023937
87. Ezaz G, Trivedi HD, Connelly MA, et al. Differential associations of circulating MicroRNAs with pathogenic factors in NAFLD. Hepatol Commun. 2020;4(5):670–680. doi:10.1002/hep4.1501
88. Tapper EB, Cohen EB, Patel K, et al. Levels of alanine aminotransferase confound use of transient elastography to diagnose fibrosis in patients with chronic hepatitis C virus infection. Clin Gastroenterol Hepatol. 2012;10(8):932–937.e931. doi:10.1016/j.cgh.2012.01.015
89. Castera L, Foucher J, Bernard PH, et al. Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology. 2010;51(3):828–835. doi:10.1002/hep.23425
90. Wong VW, Vergniol J, Wong GL, et al. Liver stiffness measurement using XL probe in patients with nonalcoholic fatty liver disease. Am J Gastroenterol. 2012;107(12):1862–1871. doi:10.1038/ajg.2012.331
91. de Ledinghen V, Wong VW, Vergniol J, et al. Diagnosis of liver fibrosis and cirrhosis using liver stiffness measurement: comparison between M and XL probe of FibroScan(R). J Hepatol. 2012;56(4):833–839. doi:10.1016/j.jhep.2011.10.017
92. Furlan A, Tublin ME, Yu L, Chopra KB, Lippello A, Behari J. Comparison of 2D shear wave elastography, transient elastography, and MR elastography for the diagnosis of fibrosis in patients with nonalcoholic fatty liver disease. AJR Am J Roentgenol. 2020;214(1):W20w26. doi:10.2214/AJR.19.21267
93. Kwok R, Tse YK, Wong GL, et al. Systematic review with meta-analysis: non-invasive assessment of non-alcoholic fatty liver disease–the role of transient elastography and plasma cytokeratin-18 fragments. Aliment Pharmacol Ther. 2014;39(3):254–269. doi:10.1111/apt.12569
94. Wong VW, Vergniol J, Wong GL, et al. Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology. 2010;51(2):454–462. doi:10.1002/hep.23312
95. Shili-Masmoudi S, Wong GL-H, Hiriart J-B, et al. Liver stiffness measurement predicts long-term survival and complications in non-alcoholic fatty liver disease. Liver Int. 2019. doi:10.1111/liv.14301
96. Karlas T, Petroff D, Sasso M, et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J Hepatol. 2017;66(5):1022–1030. doi:10.1016/j.jhep.2016.12.022
97. Piccinni R, Rodrigues SG, Montani M, et al. Controlled attenuation parameter reflects steatosis in compensated advanced chronic liver disease. Liver Int. 2019.
98. Petta S, Maida M, Macaluso FS, et al. The severity of steatosis influences liver stiffness measurement in patients with nonalcoholic fatty liver disease. Hepatology. 2015;62(4):1101–1110. doi:10.1002/hep.27844
99. Eddowes PJ, Sasso M, Allison M, et al. Accuracy of fibroscan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156(6):1717–1730. doi:10.1053/j.gastro.2019.01.042
100. Petta S, Wong VW, Camma C, et al. Improved noninvasive prediction of liver fibrosis by liver stiffness measurement in patients with nonalcoholic fatty liver disease accounting for controlled attenuation parameter values. Hepatology. 2017;65(4):1145–1155. doi:10.1002/hep.28843
101. Sporea I, Gradinaru-Tascau O, Bota S, et al. How many measurements are needed for liver stiffness assessment by 2D-Shear Wave Elastography (2D-SWE) and which value should be used: the mean or median? Med Ultrason. 2013;15(4):268–272. doi:10.11152/mu.2013.2066.154.isp2
102. Cassinotto C, Boursier J, de Ledinghen V, et al. Liver stiffness in nonalcoholic fatty liver disease: A comparison of supersonic shear imaging, FibroScan, and ARFI with liver biopsy. Hepatology. 2016;63(6):1817–1827. doi:10.1002/hep.28394
103. Herrmann E, de Ledinghen V, Cassinotto C, et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: an individual patient data-based meta-analysis. Hepatology. 2018;67(1):260–272. doi:10.1002/hep.29179
104. Petzold G, Bremer SCB, Knoop RF, et al. Noninvasive assessment of liver fibrosis in a real-world cohort of patients with known or suspected chronic liver disease using 2D-shear wave elastography. Eur J Gastroenterol Hepatol. 2020. doi:10.1097/MEG.0000000000001675
105. Takeuchi H, Sugimoto K, Oshiro H, et al. Liver fibrosis: noninvasive assessment using supersonic shear imaging and FIB4 index in patients with non-alcoholic fatty liver disease. J Med Ultrason. 2018;45(2):243–249. doi:10.1007/s10396-017-0840-3
106. Jiang W, Huang S, Teng H, et al. Diagnostic accuracy of point shear wave elastography and transient elastography for staging hepatic fibrosis in patients with non-alcoholic fatty liver disease: a meta-analysis. BMJ Open. 2018;8(8):e021787. doi:10.1136/bmjopen-2018-021787
107. Dietrich CF, Bamber J, Berzigotti A, et al. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017 (long version). Ultraschall Med. 2017;38(4):e48. doi:10.1055/a-0641-0076
108. Venkatesh SK, Yin M, Ehman RL. Magnetic resonance elastography of liver: technique, analysis, and clinical applications. J Magn Reson Imaging. 2013;37(3):544–555. doi:10.1002/jmri.23731
109. Chen J, Yin M, Talwalkar JA, et al. Diagnostic performance of MR elastography and vibration-controlled transient elastography in the detection of hepatic fibrosis in patients with severe to morbid obesity. Radiology. 2017;283(2):418–428. doi:10.1148/radiol.2016160685
110. Wagner M, Corcuera-Solano I, Lo G, et al. Technical failure of MR elastography examinations of the liver: experience from a large single-center study. Radiology. 2017;284(2):401–412. doi:10.1148/radiol.2016160863
111. Imajo K, Kessoku T, Honda Y, et al. Magnetic resonance imaging more accurately classifies steatosis and fibrosis in patients with nonalcoholic fatty liver disease than transient elastography. Gastroenterology. 2016;150(3):626–637.e627. doi:10.1053/j.gastro.2015.11.048
112. Park CC, Nguyen P, Hernandez C, et al. Magnetic resonance elastography vs transient elastography in detection of fibrosis and noninvasive measurement of steatosis in patients with biopsy-proven nonalcoholic fatty liver disease. Gastroenterology. 2017;152(3):598–607.e592. doi:10.1053/j.gastro.2016.10.026
113. Tapper EB, Sengupta N, Hunink MGM, Afdhal NH, Lai M. Cost-effective evaluation of nonalcoholic fatty liver disease with NAFLD fibrosis score and vibration controlled transient elastography. Am J Gastroenterol. 2015;110(9):1298–1304. doi:10.1038/ajg.2015.241
114. Srivastava A, Gailer R, Tanwar S, et al. Prospective evaluation of a primary care referral pathway for patients with non-alcoholic fatty liver disease. J Hepatol. 2019;71(2):371–378. doi:10.1016/j.jhep.2019.03.033
115. Newsome PN, Sasso M, Deeks JJ, et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: a prospective derivation and global validation study. Lancet Gastroenterol Hepatol. 2020;5:362–373. doi:10.1016/S2468-1253(19)30383-8
116. Sanyal AJ, Friedman SL, McCullough AJ, et al. Challenges and opportunities in drug and biomarker development for nonalcoholic steatohepatitis: findings and recommendations from an American Association for the Study of liver diseases-U.S. Food and Drug Administration joint workshop. Hepatology. 2015;61(4):1392–1405. doi:10.1002/hep.27678
117. Rinella ME, Tacke F, Sanyal AJ, Anstee QM. Report on the AASLD/EASL joint workshop on clinical trial endpoints in NAFLD. J Hepatol. 2019;71(4):823–833. doi:10.1016/j.jhep.2019.04.019
118. Loomba R, Lim JK, Patton H, El-Serag HB. AGA clinical practice update on screening and surveillance for hepatocellular carcinoma in patients with nonalcoholic fatty liver disease: expert review. Gastroenterology. 2020;158(6):1822–1830. doi:10.1053/j.gastro.2019.12.053
119. Trevisani F, D’Intino PE, Morselli-Labate AM, et al. Serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: influence of HBsAg and anti-HCV status. J Hepatol. 2001;34(4):570–575. doi:10.1016/S0168-8278(00)00053-2
120. Chen JG, Parkin DM, Chen QG, et al. Screening for liver cancer: results of a randomised controlled trial in Qidong, China. J Med Screen. 2003;10(4):204–209. doi:10.1258/096914103771773320
121. Zhang B, Yang B. Combined alpha fetoprotein testing and ultrasonography as a screening test for primary liver cancer. J Med Screen. 1999;6(2):108–110. doi:10.1136/jms.6.2.108
122. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the american association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
123. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
124. Della Corte C, Colombo M. Surveillance for hepatocellular carcinoma. Semin Oncol. 2012;39(4):384–398. doi:10.1053/j.seminoncol.2012.05.002
125. Samoylova ML, Mehta N, Roberts JP, Yao FY. Predictors of ultrasound failure to detect hepatocellular carcinoma. Liver Transpl. 2018;24(9):1171–1177. doi:10.1002/lt.25202
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.