Back to Journals » Clinical Ophthalmology » Volume 14
Human Platelets and Derived Products in Treating Ocular Surface Diseases – A Systematic Review
Authors You J, Hodge C ![]() , Hoque M, Petsoglou C
, Hoque M, Petsoglou C ![]() , Sutton G
, Sutton G
Received 2 June 2020
Accepted for publication 26 August 2020
Published 12 October 2020 Volume 2020:14 Pages 3195—3210
DOI https://doi.org/10.2147/OPTH.S265701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Jingjing You,1,2 Chris Hodge,1,3– 5 Monira Hoque,4 Constantinos Petsoglou,1,4 Gerard Sutton1,3,4
1Save Sight Institute, Sydney Medical School, University of Sydney, Sydney, NSW, Australia; 2School of Optometry and Vision Science, UNSW Sydney, Sydney, NSW, Australia; 3Vision Eye Institute, Chatswood, Sydney, NSW, Australia; 4NSW Tissue Bank, Sydney, NSW, Australia; 5Graduate School of Health, University of Technology Sydney, Sydney, NSW, Australia
Correspondence: Jingjing You
Save Sight Institute, Sydney Medical School, University of Sydney, 8 Macquarie Street, Sydney 2001, Australia
Email [email protected]
Abstract: Human platelet products have emerged as an alternative treatment for a range of ocular surface diseases such as dry eye and corneal ulceration. With significant therapeutic potential and increasing popularity, this study aimed to conduct a systematic review to detail the various production methods involved in generating platelet-derived products, compare and analyze clinical findings across available studies, and disseminate the relative advantages, limitations, and challenges of using platelet products to treat ocular surface disease. Thirty-eight clinical studies were identified, excluding studies conducted in animals and non-English language. Studies reported clinical outcomes, which included ocular surface disease index, best-corrected visual acuity, and corneal fluorescein staining. Most clinical studies reported improved patient signs and symptoms with an increasing variety of human platelet products including platelet rich plasma eye drops, human platelet lysate and platelet gels. However, due to variations in production methods, and study designs as well as confusing terminology, it was suggested that characterization of platelet products is needed for proper evaluation across studies.
Keywords: platelet rich plasma, human platelet lysate, dry eye syndrome
Introduction
Human platelets were first observed as early as 1865, but were considered as deformed or altered leukocytes or described as a fibrin clot.1 It was not until 1881 that they were identified as an independent composition of blood and their role in wound healing and coagulation determined.1 Research has identified an increasing complexity of human platelet anatomy and identified roles beyond coagulation. Accordingly, the use of human platelets has extended from incorporating treatment of hematological disease to a role in skin regeneration,2 muscle healing,3 joint regeneration,4 stem cell culturing,5,6 and ophthalmic surface treatment,7,8 thereby making it a key element in regenerative medicine.
Platelets store a wide range of biologically active agents inside vesicles known as granules. Some of these active agents include growth factors such as platelet-derived growth factor (PDGF), epidermal growth factor (EGF), fibroblast growth factor (FGF), transforming growth factor (TGF), nerve growth factor (NGF), and insulin-like growth factor (IGF); and cytokines and chemokines.9 Upon platelet activation, either via chemical activation or by physical rupturing of platelet cells, these bioactive molecules are released and have been reported to play an important role in regulating wound healing and tissue regeneration. The interaction between these molecules and their respective receptors in the tissue microenvironment can lead to overall reduced inflammation and the activation of growth related signaling pathways that facilitate wound healing.10 The primary form of the platelet product currently used in clinic is called platelet rich plasma (PRP). PRP is generated initially by isolating and then concentrating platelets into small amounts of plasma. Several additional methods have been developed to generate PRP and through research, further platelet-derived products have been developed including leukocyte rich PRP (L-PRP, LR-PRP or W-PRP), platelet concentrated plasma (PCP), non-coagulating platelet-derived factor concentrate (PFC), platelet gel (PG), platelet lysate (PL), platelet rich fibrin (PRF), and platelet-rich growth factors (PRGF).11,12 It is highly likely that through fresh research, the list of products and applications will continue to expand.
Although a consistent, internationally recognized classification system for platelet products remains unavailable to researchers, there is general agreement in describing PRP derived from disparate methods and subsequent derivative products. Understanding these differences, however, is central to the broader investigation of clinical efficacy and the interchangeability of products for the treatment of ophthalmic disease.
PRP is the platform for all platelet-derived products and can be prepared in numerous ways. Briefly, the preparation methods for PRP used for ophthalmic products can be classified into single or two-step centrifugations with the single centrifugation process most used in ophthalmic clinics (Table 1). Terminology of PRP products vary based largely on group preferences and include eye-PRP (E-PRP) which was developed directly for ophthalmic purposes and PRGF, a derivative from dental surgery. Other known ophthalmic terminology includes platelet-derived eye drops, PRGD [plasma rich in platelet-derived growth factors (PDGF) eye drops] and commercially made PRP. The two-step centrifugation preparation method is routinely used by blood banks for platelet transfusion and represents the classic method for generating PRP. The two-step centrifuge method generates PRP with platelet counts at 109 level compared to the one step centrifuging method of 108 (Table 1). To our knowledge, no clinical comparison of PRP products has been undertaken within ophthalmology.
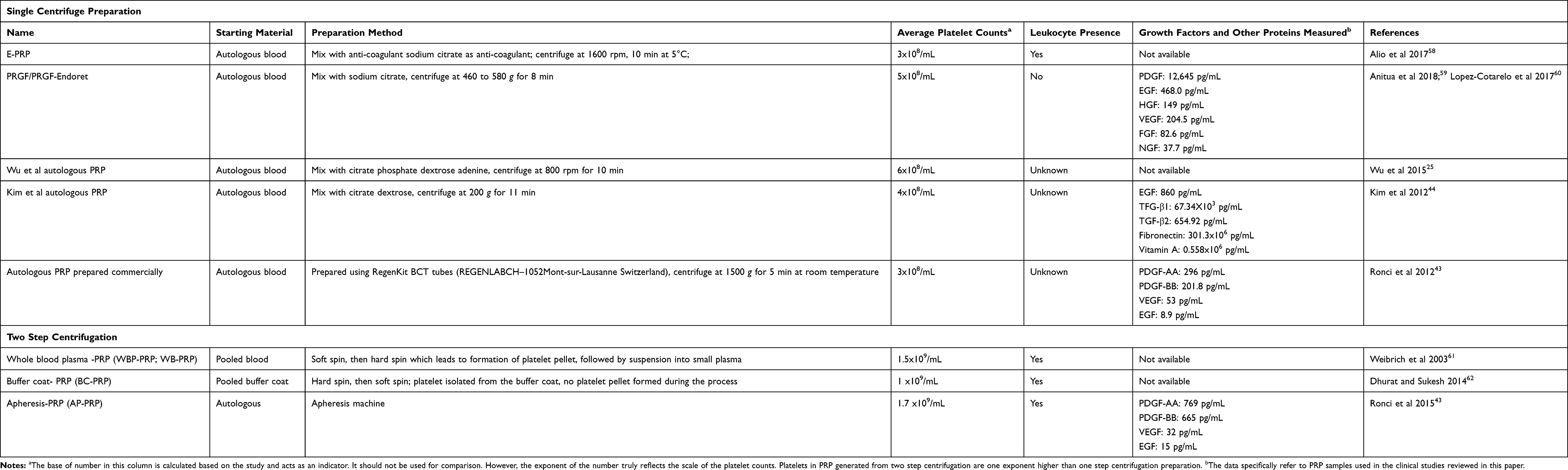 |
Table 1 Summary of Different Types of PRP Used in Ophthalmic Clinics |
Human platelet lysate (PL) is essentially PRP activated by a freeze/thaw process.13–17 Typically, the platelet concentrate is frozen at −80°C however −30°C remains suitable for further use and may reflect an available option within the hospital environment. The concentrate is then thawed at 37°C to break up the platelets.13,14 The process targets growth factor release and may not necessarily lead to gel formation which is essential to clinical use.17 The number of freeze/thaw cycles used in different studies range from one to five.15,16 A comparison of the optimal number of freeze/thaw cycles and the exact conditions of each cycle is yet to be published.
Platelet activation may also form a fibrin matrix, often referred to as PRF and PG. The development of PRF was reviewed18 and associated terminology identified two major types of platelet-derived fibrin matrix: those self-clotted and those formed through the addition of exogenous activator/coagulation factors. Based on their recommendations, the term PRF should be used only when referring to the self-clotted fibrin matrix.18,19
Furthermore, fibrin matrix formed by addition of coagulation factors was designated the name platelet-rich fibrin matrix (PRFM).18 Other publications have used PG,20 E-PRP clot,8 or PRGF gel.21 Unfortunately, no single terminology has been accepted to encompass this formulation for easy reference and subsequently we use PG to refer to fibrin matrix formed when liquid PRP products are exposed to thrombin or calcium chloride (in order to stimulate fibrin formation and platelet degranulation).22 Little is known of the biological, physical, and clinical differences between self-assembled fibrin matrix and PG.
As expected, the rapid development in platelet research has not been without challenges. Variation in method preparation, confusing terminology and unclear classification and reporting requirements for existing products have made it difficult for both scientists and clinicians to evaluate function and efficacy across published papers. This review will focus on the relative advantages and disadvantages of the clinical application of various platelet products in treating ocular surface diseases. In doing so, we hope to provide guidance on the criteria required for the development and accurate reporting of platelet products in clinical ophthalmology.
Materials and Methods
Data Sources and Searches
The study was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses.23 The search was performed to find relevant literature examining the therapeutic use of platelet products in treating ocular surface diseases. Relevant studies were retrieved from PubMed using the following keywords: platelet rich plasma OR plasma rich in growth factors OR platelet lysate OR platelet glue AND ocular. Due to low strength of evidence coupled with the significant variations of PRP used, a meta-analysis was considered inappropriate and an independent evaluation of studies undertaken. This review aims to identify efficacy and safety across available products and to detail the variety in preparation methods and protocols between studies.
Study Selection
The search generated 117 papers. Results were screened using inclusive criteria of original clinical study papers, use of human subjects, eye disease, English language and excluding duplicates which led to 35 clinical papers. Review and individual clinical papers were further screened for clinical studies not previously identified which led to an additional 3 clinical papers. In total, we identified 38 clinical papers (Table 2).
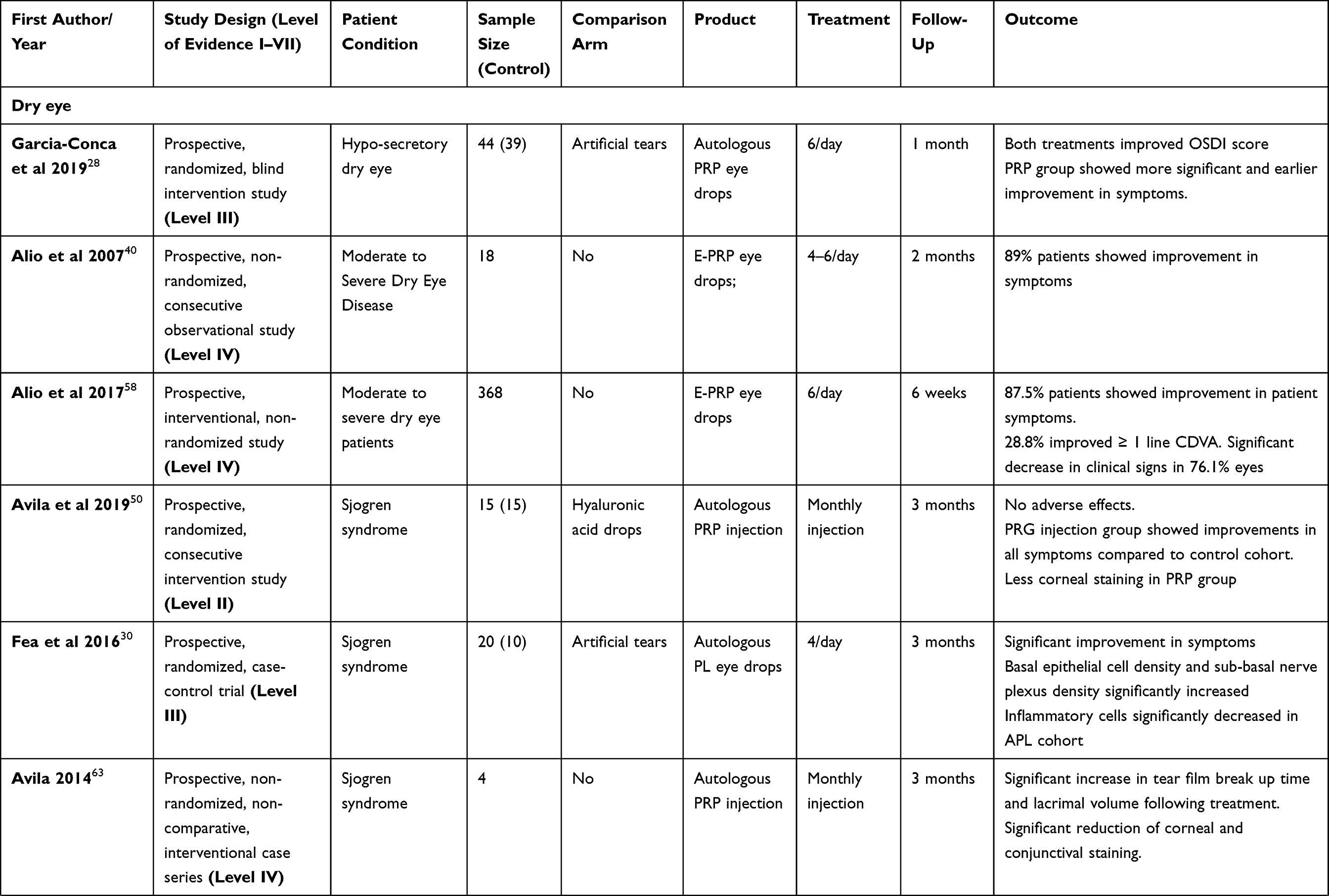 | >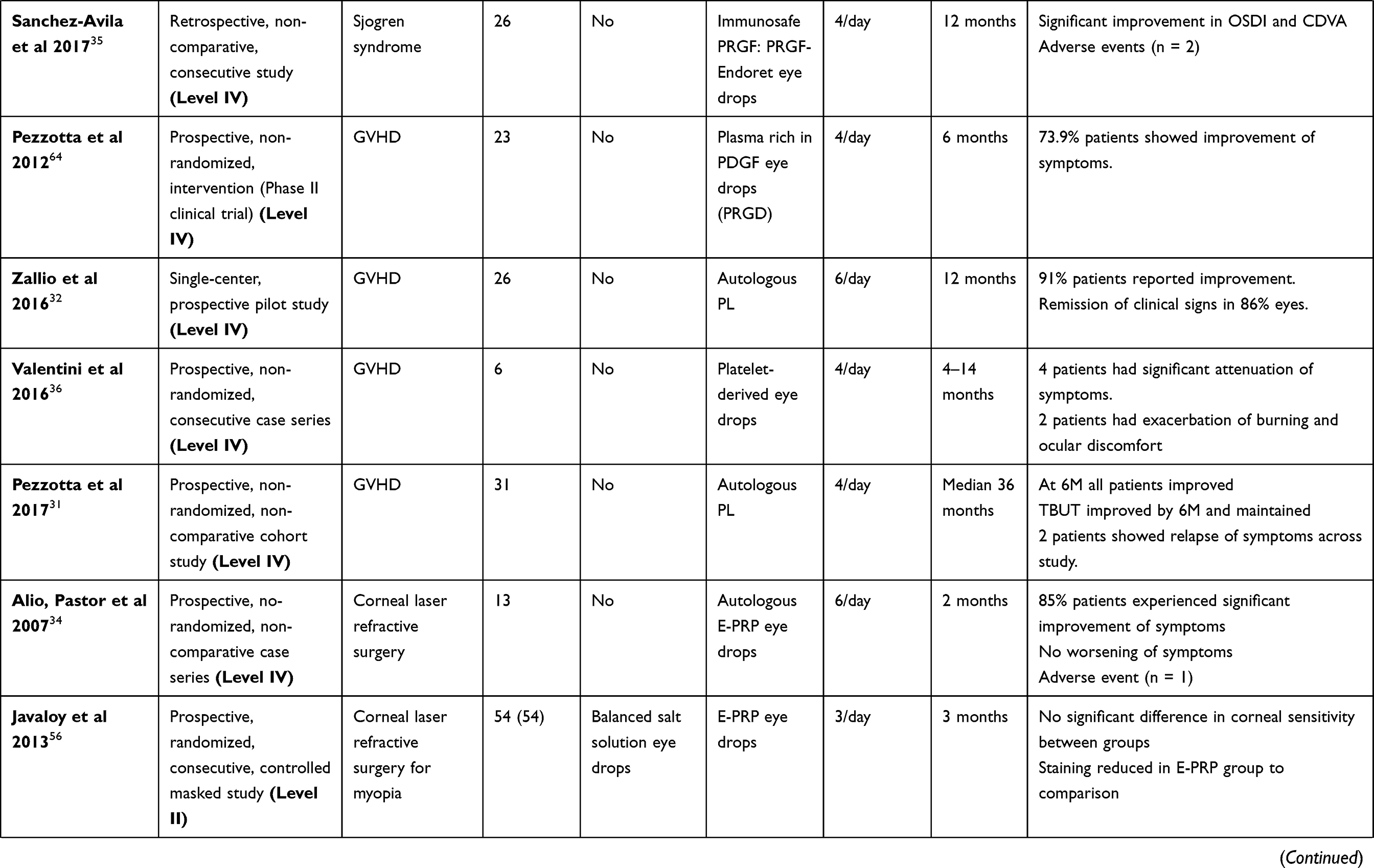 | >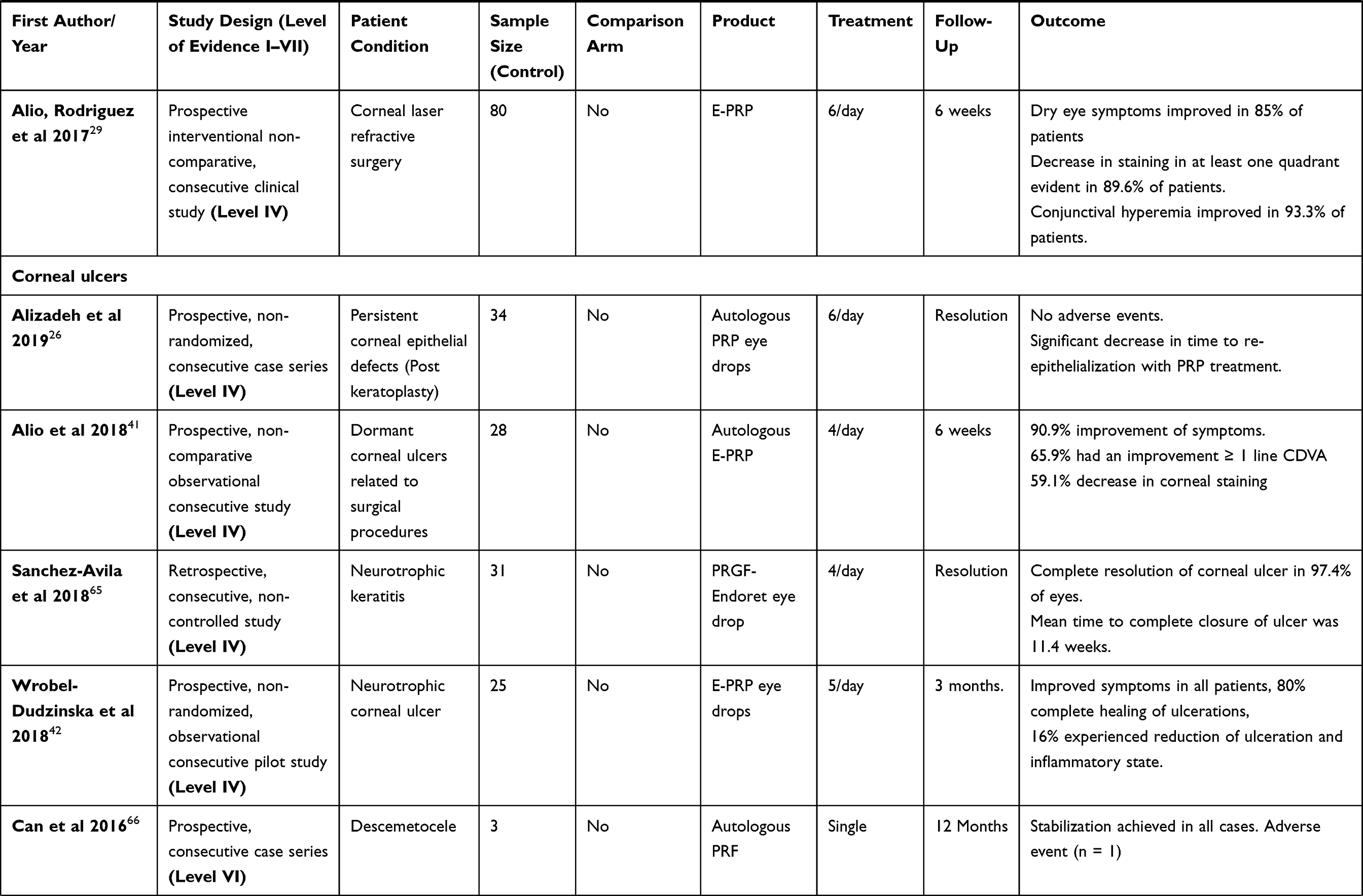 | >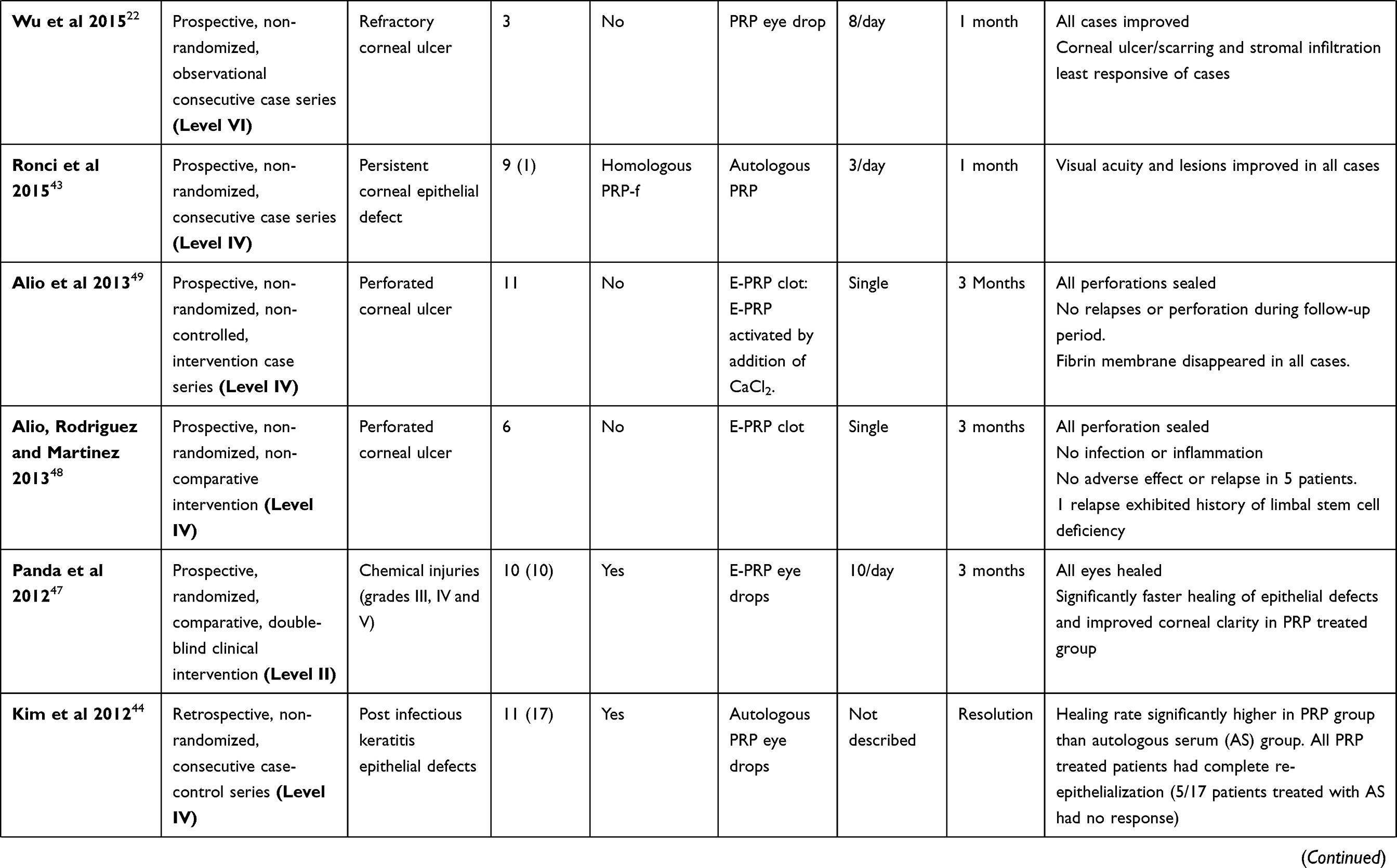 | >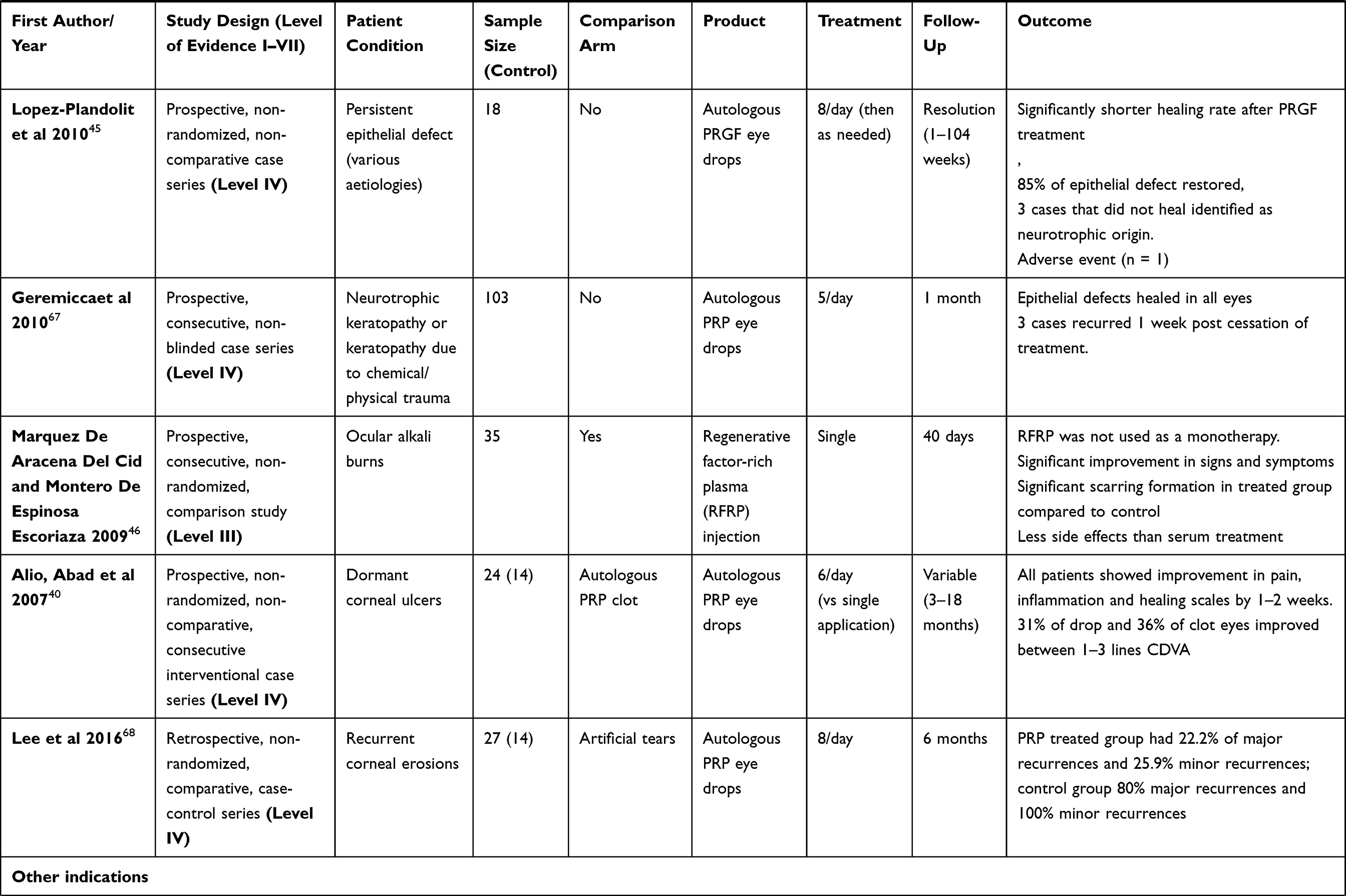 | >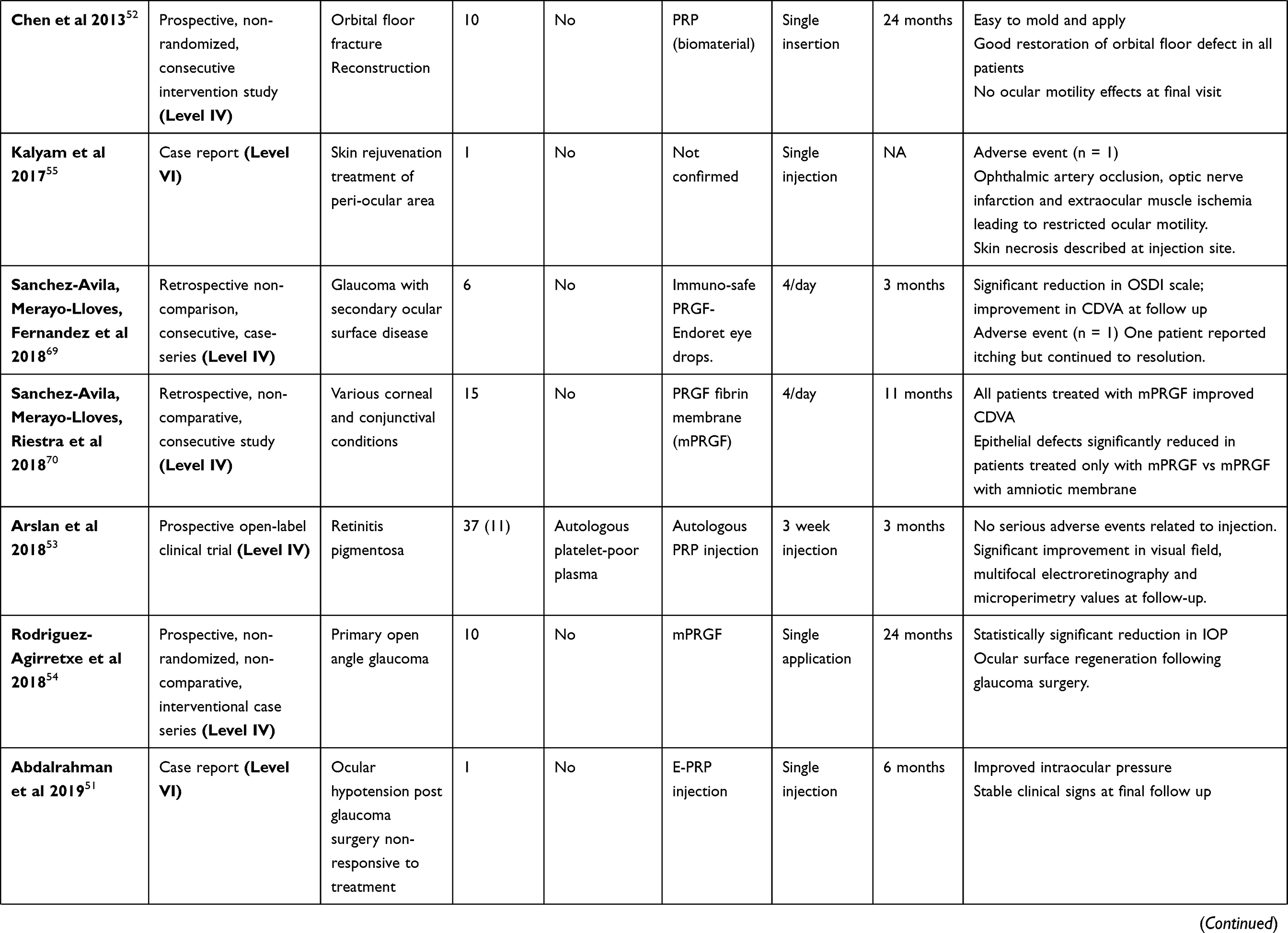 |
Table 2 Clinical Studies Using Platelet Products for Ocular Surface Diseases Treatment |
Measurements
All the clinical studies were graded into clinical evidence levels according to Evidence-based Nursing Care Guidelines24 as follows. Level I: systematic review or meta-analysis of randomized controlled trials (RCTs) or three or more RCTs of good quality with similar results. Level II: at least one well designed RCT. Level III: controlled trials with or without randomization. Level IV: well-designed case-control or cohort studies. Level V: systematic reviews of descriptive and qualitative studies. Level VI: single descriptive or qualitative study. Level VII: expert opinion.24 Different subjective and objective utilities were used to quantify and evaluate the effect of platelet products on the treatment of ocular surface disorders. Typically, studies reported the following internationally recognised scores: ocular surface disease index (OSDI) for symptom analysis; best-corrected visual acuity; visual analogy scale; Schirmer test; tear breakup time (TBUT); and corneal fluorescein staining.
Results
Analysis
The platelet products used in current clinical studies have shown composition differences in platelet numbers, growth factors, activation stage (freeze-thaw cycle, calcium activation), and have been used as eye drops, injections, or surgical dressings. Twenty-three clinical studies used PRP in the form of eye drops, among which twenty reported using PRP eye drops and three used PL. Notably eighteen of the twenty studies either transported PRP eye drops frozen or instructed patients to store unused portions frozen. As mentioned previously, the thawing process inevitably activates platelets turning PRP into PL. The two remaining studies instructed patients to keep PRP eye drops in the fridge and therefore remain the only studies that can be truly referred to as using PRP.25,26 The lack of awareness of the freeze/thaw activation disavows any reasonable comparison between the efficacy of PRP and PL in treating ocular conditions. Additionally, PRP eye drops were prepared without dilution, whereas PL eye drops were diluted with saline by either 30% or 50% (v/v). The variable dilution further prevents a direct comparison across studies. We believe the difference between PRP and PL should be addressed in all future clinical studies to provide a consistent reporting system and to evaluate if the differences in growth factor levels are clinically relevant.
Primary and Secondary Dry Eye Diseases
Among all studies treating dry eye diseases (DED), Avila et al27 was designated at clinical evidence level II, and Garcia-Conca et al28 at clinical level III. Both studies included a comparison group and used PRP eye drops. Avila et al used a prospective, randomized, consecutive intervention design. All patients had Sjogren’s-related dry eye and were divided into the treatment group using autologous PRP eye drops made by the clinic (n = 15) or the comparison group treated with hyaluronic acid drops (n = 15). Generated PRP was injected into the lacrimal gland monthly (up to 3 months). All patients in the treatment group showed improvement in symptoms and significantly improved TBUT scores, and greater reduction in corneal fluorescein staining compared to control cohort with no adverse effects observed. The limited sample size precluded broader application of success in a larger population, however. Garcia-Conca et al conducted a prospective, randomized, blinded intervention study for patients with hypo-secretory dry eye. Forty-four were treated with PRP eye drops generated by RegenKit and 39 treated with artificial tears for 30 days. Both treatments improved OSDI scores however the PRP group showed more significant and immediate improvement in symptoms across the treatment period. The authors suggested this may be due to the biological stability of growth factors and platelets being affected over time.
Among the rest of studies that ranked at clinical evidence IV or lower, Alio et al, 2017, conducted a non-randomized, non-comparison monotherapy review using E-PRP in 368 patients with moderate to severe dry eye, representing the largest available cohort.29 The patients were instructed to use E-PRP eye drops 6 times a day for 6 weeks. Over 80% of patients showed improvement in symptoms, and 28.8% improved at least 1 line of best-corrected visual acuity. Concurrently, over 75% of patients showed a reduction in clinical signs from baseline. Similar findings have been reported by other studies using both PRP eye drops and PL eye drops (Table 2).
Significant improvements in patient symptoms and clinical signs including both corneal epithelial cell and nerve plexus density were found in Sjogren syndrome patients treated with PL eye drops compared to patients treated with preservative free artificial tears.30 Pezzotta et al used PL eye drops to treat graft versus host disease (GVHD) patients (n=31) for a duration of 6 months and showed that the patients responded to the treatment, with a significant improvement in dry eye symptoms.31 Zallio et al similarly used autologous PL eye drops over an extended period (12 months) in patients suffering from chronic GVHD and found that 86% experienced remission of objective corneal signs and 73% had improved subjective national standardized health scores including 8% of patients who described complete resolution of dry eye symptoms.32
Laser in situ keratomileusis (LASIK) surgery is the most commonly performed refractive surgical procedure.33 Post-LASIK ocular surface syndrome (OSS) is used to describe a spectrum of DED following surgery. Alio et al in 2007 showed that post-LASIK dry eye symptoms improved in 85% of patients treated with E-PRP. Three eyes presented with severe punctate keratitis (1.9%) following surgery, all of which healed completely.34 Conjunctival hyperemia improved in 93.3% of the patients with previous signs of ocular surface inflammation. More recently, a retrospective, comparative study of 77 eyes in 42 patients suffering from post-LASIK OSS, showed that 1–4 cycles of treatment with PRGF (1 cycle = 6 weeks, 4 drops/day) significantly improved the symptoms compared to standard treatments inclusive of artificial tears and corticosteroids.34
Only four studies have reported adverse effects. Sanchez-Avila et al used autologous immuno-safe PRGF (PRGF prepared with an additional heating step at 56°C for 60 min) to treat 26 patients with Sjogren syndrome.35 Two patients developed eye irritation directly related to the use of PRGF. Pezzotta et al used autologous platelet lysate to treat 26 patients with GVHD and found 2 patients had relapse of symptoms.31 Alio et al in 2007 used E-PRP to treat 13 dry eye patients due to corneal laser refractive surgery with one patient developing intolerance to PRP after 4 weeks.34 No further explanation has been given by these groups. Valentini et al used platelet-derived eye drops (autologous PRP prepared in-house) on 6 GVHD patients with 2 patients experiencing burning and ocular discomfort.36
Corneal Ulcers
Topical platelet-derived products and platelet glue have been used to treat corneal ulcers and epithelial defects. The main cause of persistent epithelial defects (PED) is direct ocular injury, however the condition may be exacerbated through various pathologies including neurotrophic keratopathy, GVHD or herpes simplex infection.37–39 Conventional treatments such as artificial tears, therapeutic contact lenses, anti-inflammatory drops and oral antibiotics will provide symptomatic relief, however, often do little to provide long-term resolution of the condition.
Autologous PRP eye drops have been reported in numerous studies as an effective treatment for corneal ulcers. Alio et al in 2007 used it on 26 patients with PED caused by either neurotrophic, herpetic or immunologic factors not responsive to conventional treatments. The authors found that 50% of corneal ulcers resolved with an additional 42% showing significant clinical improvement.40 Only 2 eyes showed no clinically significant change. No explanation was provided to identify a lack of response. Furthermore, inflammation and pain were reduced in all patients.40 Alio et al in 2018 also used autologous PRP eye drops to treat 44 eyes of 28 patients with dormant ulcerations caused by surgery including keratoplasty, refractive surgery, cross-linking and chronic post-surgical corneal edema.41 Here, almost two-thirds of patients (59.1%) experienced a reduction or complete closure of the ulcer and subsequent improvement in visual acuity by at least one line of best-corrected visual acuity (65.1%). The majority (90.9%) of patients reported an improvement of symptoms.
Wrobel-Dudzinska et al used autologous PRP eye drops on 25 patients with neurotrophic corneal ulcers caused by herpes infection or cranial nerve palsy (V or VII), and no prior response to conventional treatment.42 The authors showed that at 3 months post-treatment, 80% of patients were healed, and of the remaining patients, 16% experienced a reduction in size, depth, and inflammatory status of the ulceration. The progression of corneal thinning was halted in all patients.42 Both autologous and allogenic PRP eye drops were examined by Ronci et al. Autologous PRP was used in 9 patients and allogenic PRP was used to treat only one patient with GVHD. Although all eyes reported improvement and similar healing time the small sample size prevents a direct comparison on the effectiveness between autologous and allogenic PRPart.43
The use of PRGF eye drops has been examined in PED and ulceration caused by various conditions. Kim et al treated a total of 28 eyes experiencing PED following an episode of infectious keratitis, and found that the healing rate of the corneal epithelium was significantly higher in the group treated with PRGF compared to autologous serum group.44 In a separate study, PRGF activated by calcium, was used to treat 18 patients for PED, with 85% of participants showing resolution within 11 weeks.45
Two studies evaluated the efficacy of PRGF in the treatment of corneal burns. One study used PRGF to treat 35 patients with moderate and severe ocular alkali burns, finding that corneal and conjunctival healing time was reduced with PRGF compared to conventional topical treatment and autohemotherapy treatment.46 Panda et al compared PRGF to artificial tears on PED caused by grade III to V chemical injuries (n = 10).47 Day 7 showed a significant reduction in epithelial defect area in the eyes treated with PRGF, despite no significant difference in overall healing time between the two groups. Eyes treated with PRGF also showed improved corneal transparency and visual acuity in comparison to standard treatment alone.
The clinical use of PG has mainly been examined in perforated corneal ulcers. Alio et al, 2013, generated PG by activating the autologous PRP with calcium, terming the autologous PRP used in their studies E-PRP and PG as solid E-PRP or E-PRP clot.48 They used PG in conjunction with other membranes including amniotic membrane, tutopatch or autologous fibrin membrane to treat various perforated corneal conditions.48 In all treatments, PG was placed directly in contact with the perforated site with other membranes acting as an anchor placed on top of PG and sutured into the conjunctiva.48
In conjunction with amniotic membrane, Alio et al, 2007, applied PG to 14 eyes with perforations or impending perforations. All eyes showed reduced inflammation and pain, and 10 of 14 eyes healed completely. There was no direct comparison to amniotic membrane alone.40 In conjunction with tutopatch, six cases of corneal perforation resulting from severe corneal ulcerations were successfully sealed with no relapses or perforations detected in 5 of 6 cases after 3 months. The only case which relapsed had additional severe limbal stem cell deficiency.49 When PG was used in combination with autologous fibrin membrane with central perforated ulcers (n =11), all perforations were sealed, and epithelial closures were observed in all patients. Stromal thinning was observed in less than half of all patients (5 of 11).48,49 No infection, inflammation or other clinical symptoms (pain, discomfort and other complications) were observed in all patients, and no relapses were detected after 3 months follow-up. The fibrin membrane gradually disappeared after the initial 3–5 days, allowing 7 of 11 patients to undergo corneal grafting following the initial treatment.
Other Indications
We identified 5 other conditions using platelet products, and one negative case report. The 5 conditions include: injecting E-PRP into anterior chamber to treat keratoconus hydrops (one case),50 intracameral E-PRP injection to treat ocular hypotension post glaucoma surgery (one case),51 using PRP from blood bank to mix with other materials to form a moldable paste to reconstruct orbital floor fracture (10 cases),52 injecting autologous PRP to treat retinitis pigmentosa (37 patients),53 and using PRGF fibrin membrane to treat medically uncontrolled primary open angel glaucoma (n=10).54 All these studies reported positive outcomes with significant improvement in clinical signs and symptoms.
One case reported irreversible blindness (severe ischemia) caused by injecting autologous PRP into peri-ocular area in a skin rejuvenation treatment. This treatment was performed by an unlicensed practitioner and details of PRP preparation not recorded.55
Discussion
In the present study, we conducted a comprehensive systematic review based on published studies in the last 10 years pertaining to the use of platelet products for the treatment of ocular surface diseases.
In the treatment of DED, all clinical studies reported a positive outcome in at least two-thirds of patients using various platelet products to treat dry eye disease including both primary or secondary (Sjogren, GVHD or refractive surgery) (Table 1). This suggests that all products, although variable in growth factor content, were able to assist in healing. In cases where patients were experiencing ocular discomfort,36 the authors measured various cytokine concentrations in the PRP and patient’s plasma and found that they were similar. Furthermore, these patients had a higher level of chemokine (C-X-C motif) ligand 10 (CXCL10), a crucial protein involved in developing cutaneous GVHD and in skin-related inflammation which may be detrimental to the ocular surface. It is possible the cytokines may have been generated during the PRP preparation process suggesting the potential downside of using a patient’s own plasma when patient health may be intrinsically compromised.36 A further study showed that although PRP drops may be beneficial in promoting epithelial status after LASIK, it had no positive effect on the recovery of corneal sensitivity. This may be due to the limited bioavailability of growth factors in corneal stroma when the substance is topically administered.56 It is also possible that the variability found across studies may have simply reflected the initial clinical presentation which ranged from mild dry eye as found in post-refractive surgery eyes to severe ocular surface irritation as commonly found in patients with GVHD.
For the treatment of corneal ulceration, most studies indicate a clinical improvement using platelet products. However, one study suggested that PRP may provide limited effect albeit in a minimal sample.25 In their study, autologous PRP was used to treat three cases: corneal ulceration associated with diabetic neurotrophy, corneal ulceration with a diffuse corneal epithelial defect with severe infiltration and corneal infection with herpetic keratitis combined with limbal deficiency. Autologous PRP was used for all cases. PRP treatment was found to be effective in healing the epithelial defect, however corneal scarring and stromal infiltration were minimally responsive to PRP treatment. This suggests that the regenerative ability of platelet preparations may also be dependent on both the concurrent medical condition and the depth of ulceration. Further investigations in a similar, larger sample are required. In a separate study, it was also found that allogenic PRP had significantly higher platelet counts and at least two-fold higher amount of growth factors including PDGF AA, PDGF BB, vascular endothelial growth factor (VEGF) and EGF compared to autologous PRP.43 Despite the small sample size, the similar healing times between the two types of PRP may give insight into the minimum requirement of growth factors necessary for corneal healing. The same study also indicated that one freeze/thaw cycle significantly increased the level of growth factors in both types of PRPs,43 inferring that platelet activation via freeze/thaw should become a necessary production step.
For the treatment of perforated corneas, combining PG with different membranes can be a safe and effective remedy. It is believed that the combination treatment provides a better outcome due to the increased amount of growth factors available. Future investigation of PG of variable composition may provide an option without the requirement of an additional membrane. This may minimise the risk of intraoperative complications, improving overall healing time and comfort for the patient.
In most studies reported, various platelet related products have shown improvement in cases that were not responsive to conventional methods. The variety of study designs and products available however, suggest more appropriate methodology and consistency of products is essential to understand the mechanism of action. Equally important is perhaps the characterization of the generated platelet products with few studies reporting growth factor levels, platelet counts, presence of leukocytes, and cytokine levels. This information is crucial for comparison across the studies, and to investigate the factors that promote treatment or cause the adverse effect. We cannot conclude if the different types of platelet products have a unique therapeutic effect, or if they may be interchangeable.
The majority of published studies have used autologous platelet products albeit two studies using an allogeneic source have also reported successful outcomes.43 Autologous products do not revoke an immune response; however their use may not represent an available option in every patient including those immuno-compromised patients, or patients with infectious disease.
Conclusion
There is an urgent need to reach international consensus on a standardized reporting system on platelet products. Researchers from other areas have proposed a PAW classification system encoding three key elements: the absolute number of platelets, method of platelet activations and presence of white blood cells when referring a platelet product.12 Furthermore, based on the review, our recommendation would be to incorporate the following key criteria into method preparation to ensure a more effective comparison across multiple studies, that is; the presence of leukocytes; platelet activation taking into consideration storage condition (freeze/thaw cycle); growth factor measurement to at least include PDGF and EGF; and cytokine profiling, in particular when autologous platelet product is used. Along with the standardizing and accurate reporting of the actual platelet product formulation, other researchers have also stressed the importance of standardizing treatment regimen to reflect information such as dose-size modulation, mode of delivery to ocular surface, length of treatment and number of cycles.57
Research and clinical studies have shown that platelet-derived products are likely to provide a superior healing effect in the treatment of ocular surface diseases in comparison to standard, currently available treatments. This suggests an ongoing, if not increasing role for platelets and derived products in clinical treatments. It is important at this stage to recognize the great potential of using platelet products but also its associated challenges, limitations, and potential risks to prepare a better and safer product for wider use in clinics.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Ribatti D, Crivellato E. Giulio Bizzozero and the discovery of platelets. Leuk Res. 2007;31(10):1339–1341. doi:10.1016/j.leukres.2007.02.008
2. Fabi S, Sundaram H. The potential of topical and injectable growth factors and cytokines for skin rejuvenation. Facial Plastic Surgery. 2014;30(2):157–171. doi:10.1055/s-0034-1372423
3. Borrione P, Fagnani F, Di Gianfrancesco A, Mancini A, Pigozzi F, Pitsiladis Y. The Role of Platelet-Rich Plasma in Muscle Healing. Curr Sports Med Rep. 2017;16(6):459–463.
4. Filardo G, Kon E, Roffi A, Di Matteo B, Merli ML, Marcacci M. Platelet-rich plasma: why intra-articular? A systematic review of preclinical studies and clinical evidence on PRP for joint degeneration. Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2459–2474.
5. Shih DT, Burnouf T. Preparation, quality criteria, and properties of human blood platelet lysate supplements for ex vivo stem cell expansion. N Biotechnol. 2015;32(1):199–211.
6. Suri K, Gong HK, Yuan C, Kaufman SC. Human Platelet Lysate as a Replacement for Fetal Bovine Serum in Limbal Stem Cell Therapy. Curr Eye Res. 2016;41(10):1266–1273.
7. van der Meer PF, Seghatchian J, Marks DC. Quality standards, safety and efficacy of blood-derived serum eye drops: A review. Transfus Apher Sci. 2016;54(1):164–167.
8. Alio JL, Arnalich-Montiel F, Rodriguez AE. The role of “eye platelet rich plasma” (E-PRP) for wound healing in ophthalmology. Curr Pharm Biotechnol. 2012;13(7):1257–1265.
9. Mussano F, Genova T, Munaron L, Petrillo S, Erovigni F, Carossa S. Cytokine, chemokine, and growth factor profile of platelet-rich plasma. Platelets. 2016;27(5):467–471.
10. El-Sharkawy H, Kantarci A, Deady J, et al. Platelet-rich plasma: growth factors and pro- and anti-inflammatory properties. J Periodontol. 2007;78(4):661–669. doi:10.1902/jop.2007.060302
11. Araki J, Jona M, Eto H, et al. Optimized preparation method of platelet-concentrated plasma and noncoagulating platelet-derived factor concentrates: maximization of platelet concentration and removal of fibrinogen. Tissue Eng Part C Methods. 2012;18(3):176–185. doi:10.1089/ten.tec.2011.0308
12. DeLong JM, Russell RP, Mazzocca AD. Platelet-rich plasma: the PAW classification system. Arthroscopy. 2012;28(7):998–1009. doi:10.1016/j.arthro.2012.04.148
13. Doucet C, Ernou I, Zhang Y, et al. Platelet lysates promote mesenchymal stem cell expansion: a safety substitute for animal serum in cell-based therapy applications. J Cell Physiol. 2005;205(2):228–236. doi:10.1002/jcp.20391
14. Schallmoser K, Bartmann C, Rohde E, et al. Human platelet lysate can replace fetal bovine serum for clinical-scale expansion of functional mesenchymal stromal cells. Transfusion. 2007;47(8):1436–1446. doi:10.1111/j.1537-2995.2007.01220.x
15. Burnouf T, Strunk D, Koh MBC, Schallmoser K. Human platelet lysate: replacing fetal bovine serum as a gold standard for human cell propagation? Biomaterials. 2016;76:371–387. doi:10.1016/j.biomaterials.2015.10.065
16. Hara Y, Steiner M, Baldini MG. Platelets as a source of growth-promoting factor(s) for tumor cells. Cancer Res. 1980;40(4):1212–1216.
17. Wasterlain AS, Braun HJ, Dragoo JL. Contents and Formulations of Platelet-Rich Plasma. Oper Tech Orthop. 2012;22(1):33–42. doi:10.1053/j.oto.2011.11.001
18. Kawase T, Tanaka T. An updated proposal for terminology and classification of platelet-rich fibrin. Regenerative Therapy. 2017;7:80–81.
19. Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunite´ en paro-implantologie: le PRF. Implantodontie. 2001;42:55–62.
20. Crovetti G, Martinelli G, Issi M, et al. Platelet gel for healing cutaneous chronic wounds. Transfus Apher Sci. 2004;30(2):145–151. doi:10.1016/j.transci.2004.01.004
21. Anitua E. Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants. 1999;14(4):529–535.
22. De Pascale MR, Sommese L, Casamassimi A, Napoli C. Platelet derivatives in regenerative medicine: an update. Transfus Med Rev. 2015;29(1):52–61. doi:10.1016/j.tmrv.2014.11.001
23. McInnes MDF, Moher D, Thombs BD, et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: the PRISMA-DTA Statement. JAMA. 2018;319(4):388–396. doi:10.1001/jama.2017.19163
24. Ackley B, Ladwig G, Swan B, Tucker S. Evidenced-Based Nursing Care Guidelines: Medical-Surgical Interventions.
25. Wu TE, Chen CJ, Hu CC, Cheng CK. Easy-to-prepare autologous platelet-rich plasma in the treatment of refractory corneal ulcers. Taiwan J Ophthalmol. 2015;5(3):132–135.
26. Alizadeh S, Balagholi S, Baradaran-Rafii A, et al. Autologous platelet-rich plasma eye drops accelerate re-epithelialization of post-keratoplasty persistent corneal epithelial defects. J Ophthalmic Vis Res. 2019;14(2):131–135. doi:10.4103/jovr.jovr_279_17
27. Avila MY, Igua AM, Mora AM. Randomised, prospective clinical trial of platelet-rich plasma injection in the management of severe dry eye. Br J Ophthalmol. 2019;103(5):648–653. doi:10.1136/bjophthalmol-2018-312072
28. García‐Conca V, Abad‐Collado M, Hueso‐Abancens JR, et al. Efficacy and safety of treatment of hyposecretory dry eye with platelet-rich plasma. Acta Ophthalmol. 2019;97(2):e170–e178. doi:10.1111/aos.13907
29. Alio JL, Rodriguez AE, Abdelghany AA, Oliveira RF. Autologous Platelet-Rich Plasma Eye Drops for the Treatment of Post-LASIK Chronic Ocular Surface Syndrome. J Ophthalmol. 2017;2457620(10):12.
30. Fea AM, Aragno V, Testa V, et al. The Effect of Autologous Platelet Lysate Eye Drops: an In Vivo Confocal Microscopy Study. Biomed Res Int. 2016;8406832(10):20.
31. Pezzotta S, Del Fante C, Scudeller L, et al. Long-term safety and efficacy of autologous platelet lysate drops for treatment of ocular GvHD. Bone Marrow Transplant. 2017;52(1):101–106.
32. Zallio F, Mazzucco L, Monaco F, et al. A Single-Center Pilot Prospective Study of Topical Application of Platelet-Derived Eye Drops for Patients with Ocular Chronic Graft-versus-Host Disease. Biol Blood Marrow Transplant. 2016;22(9):1664–1670.
33. Toda I. LASIK and the ocular surface. Cornea. 2008;27:1.
34. Alio JL, Pastor S, Ruiz-Colecha J, Rodriguez A, Artola A. Treatment of ocular surface syndrome after LASIK with autologous platelet-rich plasma. J Refract Surg. 2007;23(6):617–619.
35. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. The Effect of Immunologically Safe Plasma Rich in Growth Factor Eye Drops in Patients with Sjogren Syndrome. J Ocular Pharmacol Therapeutics. 2017;33(5):391–399.
36. Valentini CG, Nuzzolo ER, Orlando N, et al. Cytokine profile of autologous platelet-derived eye drops in patients with ocular chronic graft-versus-host disease. Vox Sang. 2016;110(2):189–192.
37. Tsubota K, Goto E, Shimmura S, Shimazaki J. Treatment of persistent corneal epithelial defect by autologous serum application. Ophthalmology. 1999;106(10):1984–1989.
38. Vajpayee RB, Mukerji N, Tandon R, et al. Evaluation of umbilical cord serum therapy for persistent corneal epithelial defects. Br J Ophthalmol. 2003;87(11):1312–1316.
39. Lopez-Garcia JS, Garcia-Lozano I, Rivas L, Martinez-Garchitorena J. [Use of autologous serum in ophthalmic practice]. Arch Soc Esp Oftalmol. 2007;82(1):9–20. Spanish.
40. Alio JL, Abad M, Artola A, Rodriguez-Prats JL, Pastor S, Ruiz-Colecha J. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology. 2007;114(7):1286–1293.
41. Alio JL, Rodriguez AE, De Arriba P, Gisbert S, Abdelghany AA. Treatment with platelet-rich plasma of surgically related dormant corneal ulcers. Eur J Ophthalmol. 2018;28(5):515–520.
42. Wrobel-Dudzinska D, Alio J, Rodriguez A, et al. Clinical Efficacy of Platelet-Rich Plasma in the Treatment of Neurotrophic Corneal Ulcer. J Ophthalmol. 2018;20:3538764.
43. Ronci C, Ferraro AS, Lanti A, et al. Platelet-rich plasma as treatment for persistent ocular epithelial defects. Transfus Apher Sci. 2015;52(3):300–304.
44. Kim KM, Shin YT, Kim HK. Effect of autologous platelet-rich plasma on persistent corneal epithelial defect after infectious keratitis. Jpn J Ophthalmol. 2012;56(6):544–550.
45. Lopez-Plandolit S, Morales MC, Freire V, Etxebarria J, Duran JA. Plasma rich in growth factors as a therapeutic agent for persistent corneal epithelial defects. Cornea. 2010;29(8):843–848.
46. Marquez De Aracena Del Cid R, Montero De Espinosa Escoriaza I. Subconjunctival application of regenerative factor-rich plasma for the treatment of ocular alkali burns. Eur J Ophthalmol. 2009;19(6):909–915.
47. Panda A, Jain M, Vanathi M, Velpandian T, Khokhar S, Dada T. Topical autologous platelet-rich plasma eyedrops for acute corneal chemical injury. Cornea. 2012;31(9):989–993.
48. Alio JL, Rodriguez AE, Martinez LM. Bovine pericardium membrane (tutopatch) combined with solid platelet-rich plasma for the management of perforated corneal ulcers. Cornea. 2013;32(5):619–624.
49. Alio JL, Rodriguez AE, Martinez LM, Rio AL. Autologous fibrin membrane combined with solid platelet-rich plasma in the management of perforated corneal ulcers: a pilot study. JAMA Ophthalmol. 2013;131(6):745–751.
50. Alio JL, Toprak I, Rodriguez AE. Treatment of Severe Keratoconus Hydrops With Intracameral Platelet-Rich Plasma Injection. Cornea. 2019;1:254.
51. Abdalrahman O, Rodriguez AE, Alio Del Barrio JL, Alio JL. Treatment of chronic and extreme ocular hypotension following glaucoma surgery with intraocular platelet-rich plasma: A case report. Eur J Ophthalmol. 2019;29(4):NP9–NP12.
52. Chen TM, Tzeng YS, Tsai JC, Single-Donor Allogeneic BT. Platelet Fibrin Glue and Osteoconductive Scaffold in Orbital Floor Fracture Reconstruction. Ann Plast Surg. 2013;70(3):370–374.
53. Arslan U, Ozmert E, Demirel S, Ornek F, Sermet F. Effects of subtenon-injected autologous platelet-rich plasma on visual functions in eyes with retinitis pigmentosa: preliminary clinical results. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):893–908.
54. Rodriguez-Agirretxe I, Freire V, Muruzabal F, et al. Subconjunctival PRGF Fibrin Membrane as an Adjuvant to Nonpenetrating Deep Sclerectomy: A 2-Year Pilot Study. Ophthalmic Res. 2018;59(1):45–52.
55. Kalyam K, Kavoussi SC, Ehrlich M, et al. Irreversible Blindness Following Periocular Autologous Platelet-Rich Plasma Skin Rejuvenation Treatment. Ophthalmic Plast Reconstr Surg. 2017;33(3SSuppl 1):S12–S16.
56. Javaloy J, Alio JL, Rodriguez AE, Vega A, Munoz G. Effect of platelet-rich plasma in nerve regeneration after LASIK. J Refract Surg. 2013;29(3):213–219.
57. Bernabei F, Roda M, Buzzi M, Pellegrini M, Giannaccare G, Blood-Based VP. Treatments for Severe Dry Eye Disease: the Need of a Consensus. J Clin Med. 2019;8:9.
58. Alio JL, Rodriguez AE, Ferreira-Oliveira R, Wrobel-Dudzinska D, Abdelghany AA. Treatment of Dry Eye Disease with Autologous Platelet-Rich Plasma: A Prospective, Interventional, Non-Randomized Study. Ophthalmol Ther. 2017;6(2):285–293.
59. Anitua E, Prado R, Nurden AT, Nurden P. Characterization of Plasma Rich in Growth Factors (PRGF): components and formulations. Platelet Rich Plasma Orthopaedics Sports Med. 2018;29–45.
60. Lopez-Cotarelo P, Gomez-Moreira C, Criado-Garcia O, Sanchez L, Rodriguez-Fernandez JL. Beyond Chemoattraction: multifunctionality of Chemokine Receptors in Leukocytes. Trends Immunol. 2017;38(12):927–941.
61. Weibrich G, Kleis WK, Hafner G, Hitzler WE, Wagner W. Comparison of platelet, leukocyte, and growth factor levels in point-of-care platelet-enriched plasma, prepared using a modified Curasan kit, with preparations received from a local blood bank. Clin Oral Implants Res. 2003;14(3):357–362.
62. Dhurat R, Sukesh M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J Cutan Aesthet Surg. 2014;7(4):189–197.
63. Avila MY. Restoration of human lacrimal function following platelet-rich plasma injection. Cornea. 2014;33(1):18–21.
64. Pezzotta S, Del Fante C, Scudeller L, Cervio M, Antoniazzi ER, Perotti C. Autologous platelet lysate for treatment of refractory ocular GVHD. Bone Marrow Transplant. 2012;47(12):1558–1563.
65. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. Treatment of patients with neurotrophic keratitis stages 2 and 3 with plasma rich in growth factors (PRGF-Endoret) eye-drops. Int Ophthalmol. 2018;38(3):1193–1204.
66. Can ME, Dereli Can G, Cagil N, Cakmak HB, Sungu N. Urgent Therapeutic Grafting of Platelet-Rich Fibrin Membrane in Descemetocele. Cornea. 2016;35(9):1245–1249.
67. Geremicca W, Fonte C, Vecchio S. Blood components for topical use in tissue regeneration: evaluation of corneal lesions treated with platelet lysate and considerations on repair mechanisms. Blood Transfusion. 2010;8(2):107–112.
68. Lee JH, Kim MJ, Ha SW, Kim HK. Autologous Platelet-rich Plasma Eye Drops in the Treatment of Recurrent Corneal Erosions. Korean J Ophthalmol. 2016;30(2):101–107.
69. Sanchez-Avila RM, Merayo-Lloves J, Fernandez ML, et al. Plasma rich in growth factors eye drops to treat secondary ocular surface disorders in patients with glaucoma. Int Med Case Rep J. 2018;11:97–103.
70. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. Plasma rich in growth factors membrane as coadjuvant treatment in the surgery of ocular surface disorders. Medicine. 2018;97:17.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.