Back to Journals » Patient Preference and Adherence » Volume 12
How to meet patients' individual needs for drug information - a scoping review
Authors Kusch MKP, Haefeli WE ![]() , Seidling HM
, Seidling HM ![]()
Received 9 May 2018
Accepted for publication 4 September 2018
Published 6 November 2018 Volume 2018:12 Pages 2339—2355
DOI https://doi.org/10.2147/PPA.S173651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Marcel KP Kusch,1,2 Walter E Haefeli,1,2 Hanna M Seidling1,2
1Department of Clinical Pharmacology and Pharmacoepidemiology, University of Heidelberg, 69120 Heidelberg, Baden-Wurttemberg, Germany; 2Cooperation Unit Clinical Pharmacy, University of Heidelberg, 69120 Heidelberg, Baden-Wurttemberg, Germany
Purpose: The aim of this study was to 1) describe drug information desired by patients and 2) analyze how such information could be customized to be presented to patients according to their individual information needs.
Materials and methods: We performed a scoping literature search and identified relevant drug information topics by assessing and clustering 1) studies analyzing patients’ enquiries to drug information hotlines and services, and 2) qualitative studies evaluating patient drug information needs. For the two most frequently mentioned topics, we further analyzed which components (ie, information domains) the topics contained and examined patients’ and health care professionals’ (HCPs) views on these components.
Results: Of 27 identified drug information topics in the literature search, patients most frequently requested information on adverse drug reactions (ADRs) and drug–drug interactions (DDIs). Hypothetically, those topics are composed of seven distinct information domains each (eg, ADR and DDI classification by frequency, severity, or onset; information on management strategies, monitoring, and prevention strategies). Patients’ and HCPs’ appraisal concerning the information content of these domains varies greatly and is even lacking sometimes.
Conclusion: Patients particularly request information on ADRs and DDIs. Approaches to customize such information are sparse. The identified information domains of each topic could be used to structure corresponding drug information and to thus facilitate customization to individual information needs.
Keywords: medication information, information needs, customization, adverse drug reactions, side effects, drug–drug interactions
Introduction
Patient-centered care (PCC) emphasizes patient participation in decision making in order to foster the alliance between health care professionals (HCPs) and patients to share power and responsibility.1 Patients appreciate this approach and several studies indicated positive effects on health outcomes as PCC improves communication, patient involvement, patient-HCP relationship, and treatment adherence.2,3 A prerequisite for shared responsibility is the empowerment of patients based on the provision of understandable information that matches the individual patients’ information needs.3 With regard to drug treatment, patients who have received clear and reasonable treatment recommendations and advice are more likely to adhere to their treatment.4
This may be explained by the fact that basic information on drug treatment is mandatory to fulfill the “Five Rights”,5,6 ie, taking the right drug by the right patient in the right dose at the right time following the right technique to prevent unintentional non-adherence. However, in addition to such evident information needs, patients evaluate the benefits of prescribed drugs (necessity belief) and weigh it against their concerns (concern belief). While a profound “necessity belief” appears to predict adherence, a deeper “concern belief” may lead to non-adherence,7 which, in this context, is often called intentional non-adherence.8 Especially in chronic conditions (eg, hypertension) non-adherence is associated with increased overall health care costs, morbidity, and mortality.4 To efficiently address or prevent a patient’s concern and thereby mitigate at least one reason of non-adherence, the provision of subjectively desired information about treatment and drugs seems a promising approach.3
Which information is relevant to a patient depends on several factors including age, socio-economic status, and comorbidities.9 Depending on the patient’s preferences, both receiving “too much” of unsolicited information and receiving not enough information may have negative effects on patient empowerment, thus amplifying patient concerns. Therefore, it is crucial to customize information toward the individual needs of each patient.9 However, systematic data on which drug information patients want and how it should be edited are sparse.
Unmatched drug information needs are reflected in the growing use of online health information services. Taking Germany as an example, approximately half of its population uses the Internet to get health-related information, and especially services such as medication checks and drug–drug interaction (DDI) checks are frequently accessed.10
To satisfy such unmatched information needs, we aimed to 1) describe drug information desired by patients and 2) analyze how such information could be customized to be presented to patients according to their individual information needs.
Materials and methods
We followed the presumption that drug information can be divided into 1) basic drug information and 2) subjectively desired drug information. Basic drug information refers to drug information that is mandatory for every patient in order to be able to conduct the drug treatment following the concept of the “Five Rights”.5 Subjectively desired drug information, on the other hand, satisfies information customized to individual needs and considers concerns or beliefs with regard to the treatment.
While basic drug information often is straightforward, unambiguous, and therefore easily conveyed in medication schedules,11 no overview exists regarding scope and characteristics of subjective drug information needs.
To describe drug information desired by patients, an exploratory number of articles relating to patient information needs with one of the key words “patient information,” “drug information,” “medication information,” and “medicines information” in title/abstract, English or German language, and with a publishing date between January 2000 and February 2017 were searched. The search purposefully identified potentially relevant studies that were subsequently clustered into two groups: the first group 1) comprised studies analyzing patients’ enquiries to drug information hotlines and services, while the second group 2) comprised qualitative studies evaluating patient drug information needs. From the identified studies in the first group, the total number of drug-related enquiries, the enquiry topics, the provider of the information service, and the timeframe of data enquiry were extracted. The enquiry topics were classified according to those previously defined in the respective study by the authors. From the second group, the study design, population, study site, and raised drug information needs were extracted.
Subsequently, we clustered the different enquiry topics (extracted from studies analyzing patients’ enquiries) and the raised drug information needs (extracted from qualitative studies) as defined in the studies into drug information topics, therewith merging enquiry topics according to their content into broader categories that were consistently defined and applied in both study groups (Table S1 and S2). This allocation was conducted by two clinical pharmacists until concordance was reached (MK and VSW). When this was not possible, a third clinical pharmacist was consulted for clarification (HS). The drug information topics were then counted throughout the different studies and arranged according to frequency in order to identify the most often reported drug information topics and to define the two most frequently mentioned ones (Figure 1).
 | Figure 1 Flow chart of information extraction from the identified studies and allocation in order to identify the most often reported drug information topics and to define the two most frequently mentioned ones. |
To analyze how such information could be customized in order to be presented to patients, we focused on the two most frequently mentioned information topics and assessed in more detail which components (ie, information domains) the topics contained. Subsequently, we evaluated patients’ and HCPs’ expectations toward the content and presentation of these information domains as described in the literature.
Results
Drug information desired by patients
We identified 12 studies analyzing patient enquiries to drug information hotlines and services.12–23 Most studies analyzed enquiries to drug information hotlines (number of studies [n]=10), while some analyzed enquiries to online information services (n=2). Studies originated from several countries, namely Australia (n=5), the Netherlands (n=2), Germany (n=2), Finland (n=1), United States of America (n=1), and the United Kingdom (n=1). Most of the studies were performed with data originating from the Australian drug information hotline “National Prescribing Service MedicineWise” (NPS MedicineWise) and comprised a plethora of drug-related patient enquiries, most of which were safety-related, such as information on adverse drug reactions (ADRs) and DDIs (Table 1). In the second group, 15 qualitative studies that addressed drug information needs with different methods and in different settings and populations were identified.24–38 Studies were conducted in different countries, namely the Netherlands (n=3), United States of America (n=2), the United Kingdom (n=2), Norway (n=1), China (n=1), Armenia (n=1), Germany (n=1), Singapore (n=1), Australia (n=1), Canada (n=1), and Belgium (n=1). In addition, the studies were conducted in various settings, which were community pharmacies (n=8), residents not recruited in direct health care setting (n=3), hospitals (n=2), practices (n=1), and senior centers (n=1). Various study designs were used in the studies, namely semi-structured interviews (n=7), questionnaires (n=5), focus group discussions (n=2), and presenting commonly asked questions to assess interest in these (n=1). Also, in these studies the majority of the drug information topics raised by the patients were safety-related, most frequently seeking information on ADRs and DDIs (Table 2). Yet, there seemed to be some differences based on study context and setting. Patients in senior centers and hospitals were not interested in information topics like “drugs and driving” and “drug use and alcohol”.27,34,38
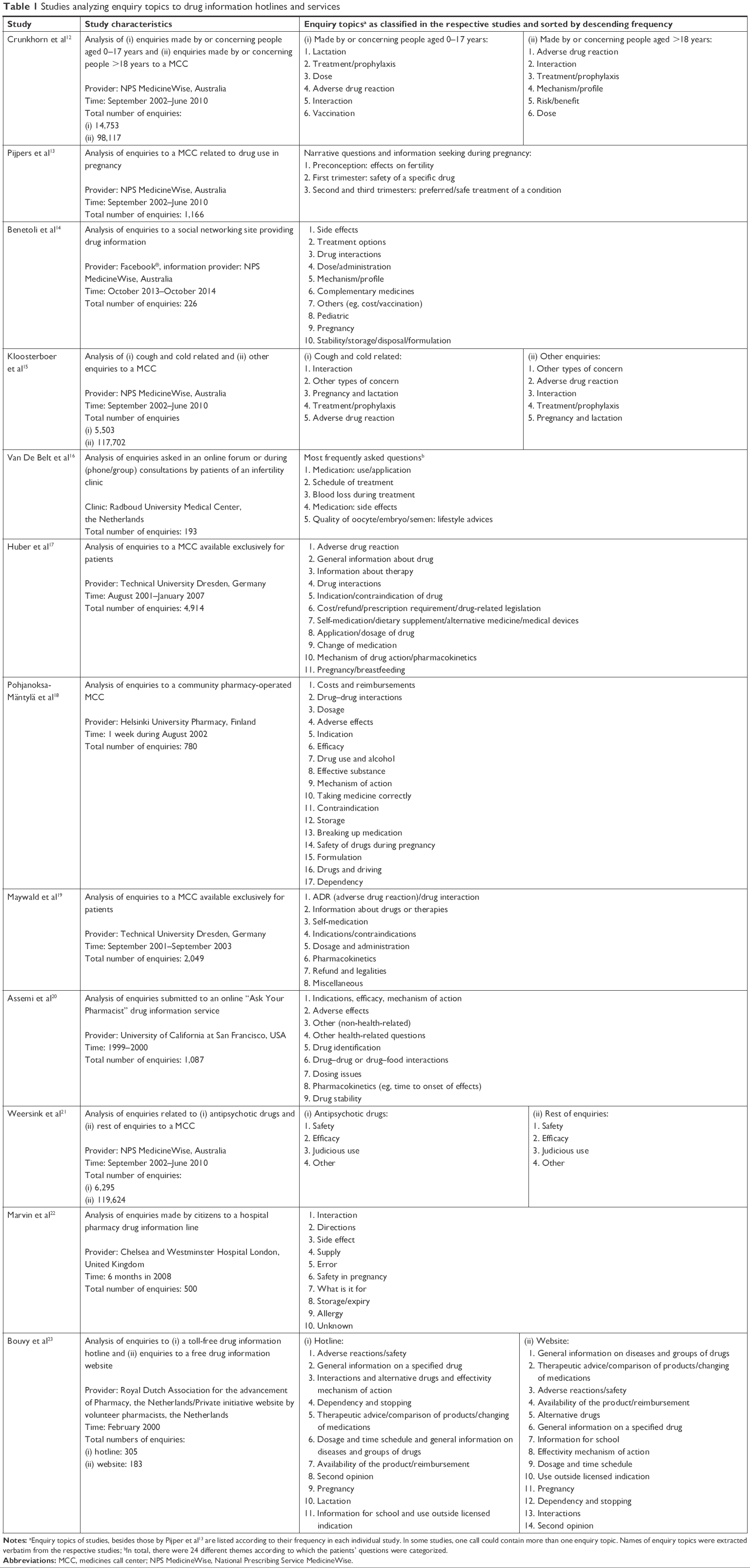 | Table 1 Studies analyzing enquiry topics to drug information hotlines and services |
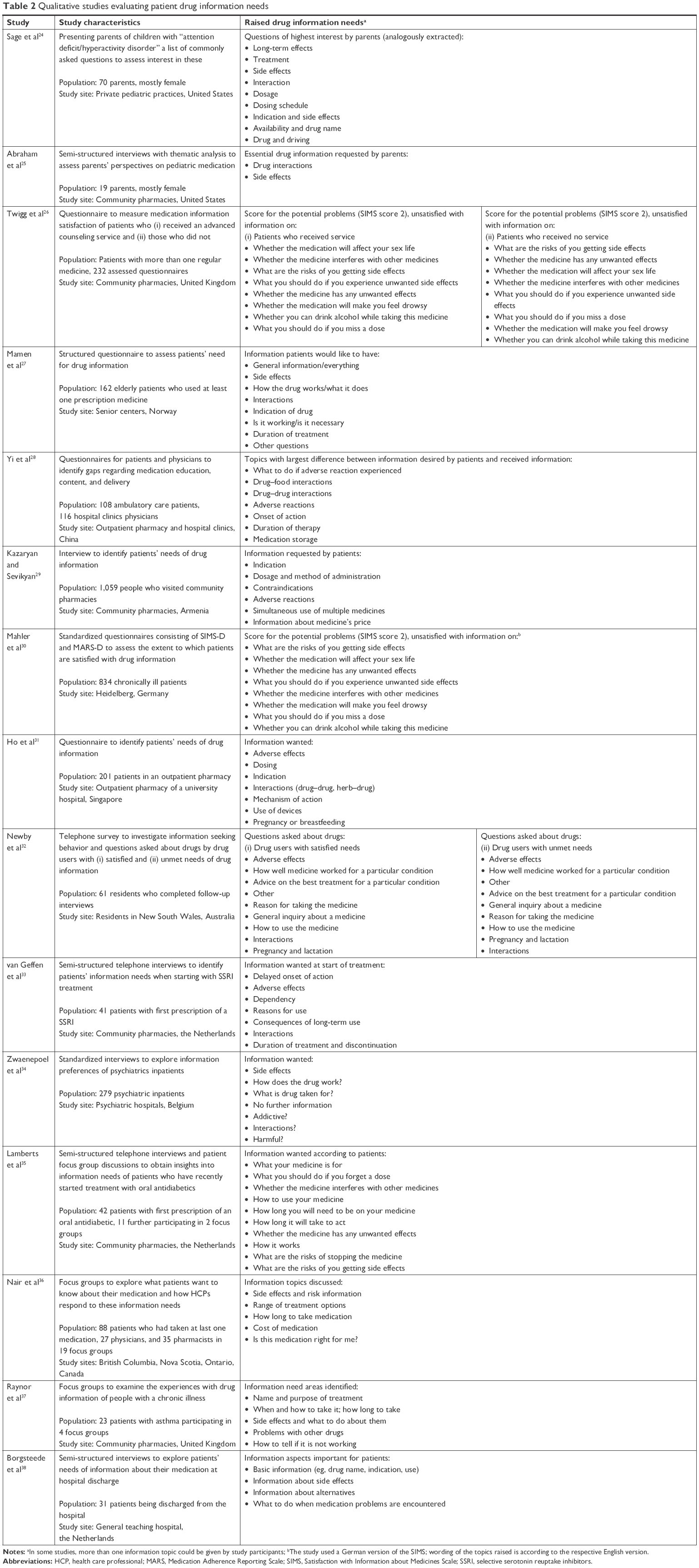 | Table 2 Qualitative studies evaluating patient drug information needs |
Some information topics like “cost, refund, and prescription requirement” and “stability, storage, and disposal” were predominantly mentioned in ambulatory settings (ie, pharmacies and residents).28,29,36 Such topics were also more often mentioned in studies analyzing patient enquiries to drug information hotlines and services. The majority of raised drug information topics were largely identical in the examined studies regardless of whether semi-structured interviews or questionnaires were used. Focus groups that were held between patients and researchers,36 and patients, physicians, and pharmacists,37 also freely discussed predominantly safety-related drug information topics in addition to information topics that can be considered to follow the principle of the “Five Rights,”5 such as “dose and administration,” “indication,” and “duration of treatment.” Arrangement of the allocated drug information topics according to frequency yielded ADRs and DDIs as the drug information topics most often sought by the patients regardless of country, setting, and study design. Other frequently requested drug information topics were dose and administration (ie, how and in which strength to take the drug), indication of a drug, and treatment options (ie, whether alternative drugs can be used to treat the condition). Selected topics of lower interest were information on vaccination, off-label use, drug formulation, and allergy (Figure 2).
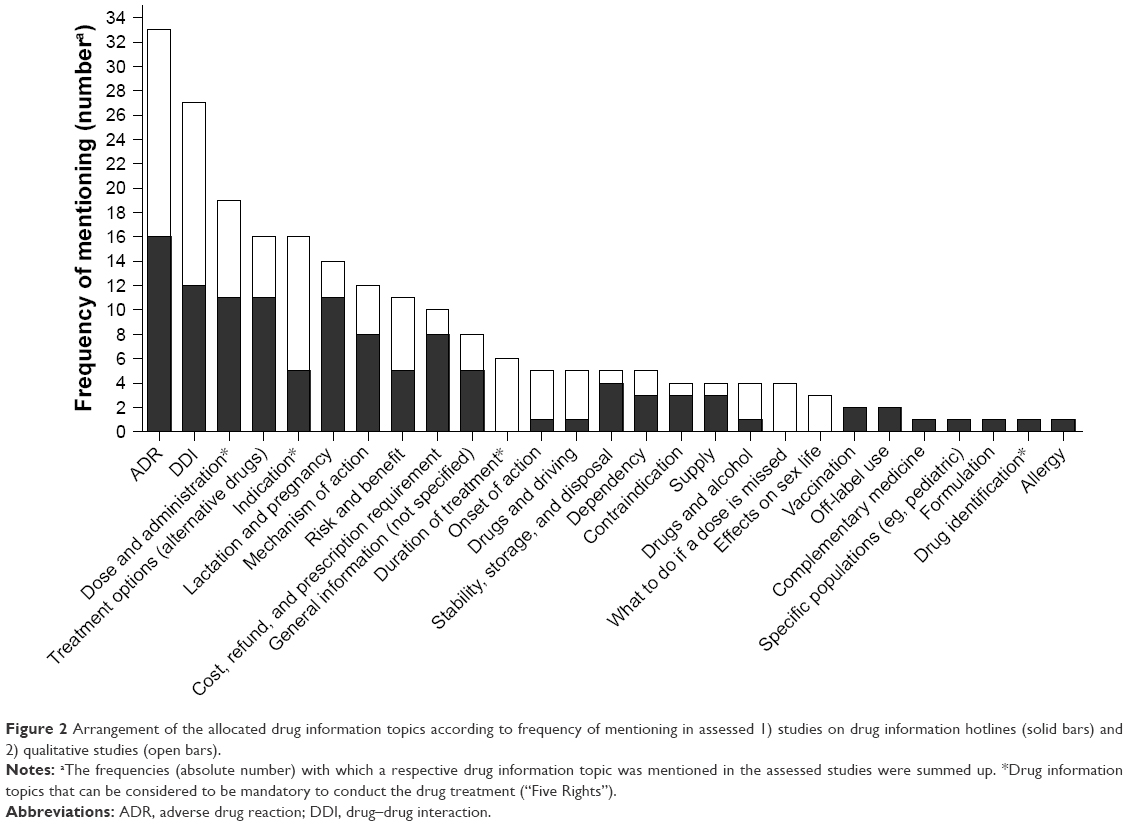 | Figure 2 Arrangement of the allocated drug information topics according to frequency of mentioning in assessed 1) studies on drug information hotlines (solid bars) and 2) qualitative studies (open bars). |
Customization of drug information
Both ADR and DDI information may be composed of seven different information domains each (Table 3): ADR information could be customized according to the frequency, severity, onset of ADRs (eg, start of therapy vs long-term effects), duration of ADRs (eg, long-term vs short-term), and management strategies including limitations of self-management (ie, how to minimize ADRs and when to consult a physician). Moreover, additional information could be given on appropriate monitoring and prevention strategies (eg, tools to cope with ADRs).
 | Table 3 The two most frequently mentioned drug information topics and their information domains |
For DDIs, customization could refer to the identification of DDIs, frequency, severity, or onset of DDIs. Furthermore, additional information on management strategies including limitations of self-management, monitoring, and prevention strategies (eg, different timing, lower dosages, and alternative medicines) could be given.
The subsequent literature search illustrated some of these domains with patients’ needs and HCP perceptions regarding extent of information wanted because especially classification of ADRs by frequency and severity was often mentioned in the assessed literature. However, the majority of the domains were never extensively assessed in patients or HCPs. Hence, knowledge of whether and to which extent patients require the diverse elements of information and to what extent HCPs support them is limited.
Discussion
Patients request largely differing information on their drugs beyond the basic information of the “Five Rights” provided in medication schedules. Thereby, information needs verbalized in qualitative studies are reflected in actual enquiries to information hotlines and services. Undoubtedly, safety-related information on ADRs and DDIs is most often sought.30,37
In comparison to other drug information topics such as appropriate storage of drugs or indication of a drug, relevant information on ADRs and DDIs is broader and less explicit. Hence, if patients request information on ADRs, it typically remains unclear what they actually want to know. For instance, do patients want to learn only about the most frequent ADRs, or the most severe ones, or those they can independently monitor and manage? Nevertheless, such safety-related information might particularly interfere with patient concerns about their drug treatment and may hence also influence their adherence to drug treatment because lacking information might promote a deeper “concern belief” and thus non-adherence.7,8 Owing to the high diversity of ADR and DDI information, it is difficult to satisfy individual needs, identify information deficits, and provide missing details while avoiding to transfer information that is not sought or irrelevant in the current patient situation.
For both ADRs and DDIs, we identified seven distinct information domains that would allow for customizing information. Such customization would then enable HCPs to individually provide patients with the respective drug information of personal interest. Only little is published on patient attitudes toward these information domains and even fewer evidence exists on how patient needs could be assessed to identify unmet information needs.
For instance, there are patients who decline to receive additional information and treatment willingness of some patients already diminishes when the mere presence of possible ADRs is mentioned, regardless of their likelihood of occurrence.61 Often, this fear of potential non-adherence is put forward by HCPs who are reluctant to offer what they deem too much additional information. However, this fear is not reflected in literature.62,63
At the other extreme, some patients want a full disclosure of all possible ADRs. Indeed, patients often seem to follow a safety-conscious strategy and opt for a maximum of information without a real understanding of risk and likelihood.39,46 Furthermore, patients seem to be particularly interested in risks considered most threatening for their own well-being regardless of their likelihood of occurrence.44
The majority of patients probably is situated in between these two extremes, and while customization of information to satisfy individual needs is acknowledged,58 explicit endeavors remain scarce. Often, patients are left with patient information leaflets that follow a “one-size-fits-all” approach and the vast number of ADRs mentioned often causes undesirable emotional reactions (eg, fear) that might promote non-adherence.42 With regard to DDIs, some patients believe that a lot of drugs should not be combined because their efficacy could be altered, whereas other patients believe that co-prescribed medicines are unlikely to interact at all.55 Considering self-medication in particular, there is a need to inform patients and raise awareness about possible DDIs between prescribed drugs and those used in self-medication.
While extensive research has been undertaken to assess professional DDI checkers regarding their content, design, and use in a professional setting, there is very limited information on performance of DDI checkers informing patients and laypersons.64 Many available DDI checkers lack DDI severity information, contain only limited patient-oriented risk communication, and have only limited patient readability.64 Especially, lengthy and complex information on possible DDIs is not well understood.65 Future research is therefore necessary to facilitate 1) customization of ADR information and 2) customization of DDI information with advanced drug information management in order to enable customization possibilities. Besides enabling customization possibilities of drug information, a particular emphasis must be put on making this information easily accessible for future users (eg, patients). Therefore, in a subsequent step, low-threshold dissemination channels must be assessed and validated with patients.
A first step would be to develop, validate, and release a database that contains available drug information in commonly understood language and register that is structured according to relevant identified information domains (Table 3). Such a database would allow selecting only information domains important for the individual patient and would thus individualize information transfer. A second prerequisite would be a tool to assess and identify individual drug information needs and select information domains for which a patient wants additional information. There are already tools available to assess whether patients desire more or less information in general and about their drugs in particular, such as the “Extent of Information Desired” scale,9 and tools that help measuring overall satisfaction with drug information, such as the “Satisfaction with Information about Medicines Scale”.26,30 However, a tool to determine specific information domains on ADRs and DDIs to allow patients to select the amount and content of additional drug information is lacking. To recognize and identify boundaries and implications of customized drug information, it will be crucial on the one hand to identify patient populations benefiting from such a form of information. On the other hand, it will be equally important to find those patients who do not need additional information, and particularly those who are not served by such an approach while being in need of additional information – to this end, it may also be necessary to include further patient characteristics that influence information needs, predominantly the patient’s health literacy.66 Looking at the literature, high desires for information were expressed for instance by patients with diabetes diagnosis, whereas patients with cardiovascular and respiratory diseases expressed lower desires for drug information.9 Additional factors like diseases and comorbidities may therefore also influence individual information needs.9,34 How and in which way such influence takes place should consequently also be assessed.
Limitations
The present work has several limitations. First, we conducted a narrative instead of a systematic review and only assessed a single (albeit large) database (PubMed). However, our aim was to identify the most relevant drug information topics and highlight how such information can be customized. With a narrative approach we were able to include a broad spectrum of articles and therefore widely assess drug information needs. The topics extracted from PubMed articles showed strong consistency and little deviation of topics mentioned, therewith suggesting an already sufficient approach. Furthermore, while not applying the full range of the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) statement, we still applied various checklist items in our review process whenever possible (eg, eligibility criteria, information sources, data collection progress, synthesis of results, study characteristics, summary of evidence, limitations, conclusions, and funding).67
Second, our approach to assess unsatisfied drug information needs by analyzing enquiries to drug information hotlines and services might be biased by the fact that actively calling a hotline requires some basic interest in drug-related topics and ambition to self-reliantly acquire information; therefore, more “empowered” and proactive patients may be selected by this approach and less empowered patients might be missed. Nevertheless, the second assessment of unmatched information needs including a variety of qualitative studies yielded similar results, supporting the conclusion that these findings indeed reflect the drug information needs of a broad population of patients.
Conclusion
Patients particularly request safety-related drug information that exceeds the typical scope of medication schedules. While it is well known that extent and content of the favored information can vary, evidence on how to assess information needs and correspondingly customize information is sparse. This review suggests that for both ADRs and DDIs, rather diverse but only limited information domains are needed and that individual patients largely differ with respect to their information needs.
Acknowledgments
The authors thank Viktoria S Wurmbach (VSW) for her help in allocating the enquiry topics and raised drug information topics into broader categories (drug information topics). In addition, the authors thank the members of the “Cooperation Unit Clinical Pharmacy” for valuable input regarding the information domains for the two most frequently mentioned drug information topics. Part of this work was supported by the “Klaus Tschira Foundation gGmbH (KTS),” Heidelberg, Germany. The funding sources had no involvement in collection, analysis, interpretation of data, and in the writing of the report. In addition, we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme Open Access Publishing, by the Baden-Württemberg Ministry of Science, Research and the Arts and by Ruprecht-Karls-Universität Heidelberg.
Disclosure
The authors report no conflicts of interest in this work.
References
Castro EM, Van Regenmortel T, Vanhaecht K, Sermeus W, Van Hecke A. Patient empowerment, patient participation and patient-centeredness in hospital care: A concept analysis based on a literature review. Patient Educ Couns. 2016;99(12):1923–1939. | ||
de Boer D, Delnoij D, Rademakers J. The importance of patient-centered care for various patient groups. Patient Educ Couns. 2013;90(3):405–410. | ||
Robinson JH, Callister LC, Berry JA, Dearing KA. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract. 2008;20(12):600–607. | ||
Náfrádi L, Galimberti E, Nakamoto K, Schulz PJ. Intentional and Unintentional Medication Non-Adherence in Hypertension: The Role of Health Literacy, Empowerment and Medication Beliefs. J Public Health Res. 2016;5(3):762. | ||
Elliott M, Liu Y. The nine rights of medication administration: an overview. Br J Nurs. 2010;19(5):300–305. | ||
Haefeli WE. Verabreichungsfehler – welche Informationen braucht ein Patient um seine Arzneimittel-Therapie sicher durchzuführen? [Drug administration errors-what information is required to enable patients to safely take their drugs? Ther Umsch. 2006;63(6):363–365. German. | ||
Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. | ||
de Vries ST, Keers JC, Visser R, et al. Medication beliefs, treatment complexity, and non-adherence to different drug classes in patients with type 2 diabetes. J Psychosom Res. 2014;76(2):134–138. | ||
Duggan C, Bates I. Medicine information needs of patients: the relationships between information needs, diagnosis and disease. Qual Saf Health Care. 2008;17(2):85–89. | ||
EPatient RSD GmbH. Press conference. EPatient Survey 2016; March 3; 2016; Berlin, Germany. Available from: https://dl.health-it-portal.de/topics/860/files/pressemappe_fachmedien_epatientsurvey2016.pdf. Accessed October 25, 2018. | ||
Botermann L, Krueger K, Eickhoff C, Kloft C, Schulz M. Patients’ handling of a standardized medication plan: a pilot study and method development. Patient Prefer Adherence. 2016;10:621–630. | ||
Crunkhorn C, van Driel M, Nguyen V, Mcguire T. Children’s medicine: What do consumers really want to know? J Paediatr Child Health. 2017;53(2):155–162. | ||
Pijpers EL, Kreijkamp-Kaspers S, Mcguire TM, Deckx L, Brodribb W, van Driel ML. Women’s questions about medicines in pregnancy – An analysis of calls to an Australian national medicines call centre. Aust N Z J Obstet Gynaecol. 2017;57(3):334–341. | ||
Benetoli A, Chen TF, Spagnardi S, Beer T, Aslani P. Provision of a Medicines Information Service to Consumers on Facebook: An Australian Case Study. J Med Internet Res. 2015;17(11):e265. | ||
Kloosterboer SM, Mcguire T, Deckx L, Moses G, Verheij T, van Driel ML. Self-medication for cough and the common cold: information needs of consumers. Aust Fam Physician. 2015;44(7):497–501. | ||
Van De Belt TH, Hendriks AF, Aarts JW, Kremer JA, Faber MJ, Nelen WL. Evaluation of patients’ questions to identify gaps in information provision to infertile patients. Hum Fertil. 2014;17(2):133–140. | ||
Huber M, Kullak-Ublick GA, Kirch W. Drug information for patients – an update of long-term results: type of enquiries and patient characteristics. Pharmacoepidemiol Drug Saf. 2009;18(2):111–119. | ||
Pohjanoksa-Mäntylä MK, Antila J, Eerikäinen S, et al. Utilization of a community pharmacy-operated national drug information call center in Finland. Res Social Adm Pharm. 2008;4(2):144–152. | ||
Maywald U, Schindler C, Krappweis J, Kirch W. First patient-centered drug information service in Germany – a descriptive study. Ann Pharmacother. 2004;38(12):2154–2159. | ||
Assemi M, Torres NM, Tsourounis C, Kroon LA, Mccart GM. Assessment of an online consumer “Ask Your Pharmacist” service. Ann Pharmacother. 2002;36(5):787–792. | ||
Weersink RA, Taxis K, Mcguire TM, van Driel ML. Consumers’ questions about antipsychotic medication: revealing safety concerns and the silent voices of young men. Soc Psychiatry Psychiatr Epidemiol. 2015;50(5):725–733. | ||
Marvin V, Park C, Vaughan L, Valentine J. Phone calls to a hospital medicines information helpline: analysis of queries from members of the public and assessment of potential for harm from their medicines. Int J Pharm Pract. 2011;19(2):115–122. | ||
Bouvy ML, van Berkel J, de Roos-Huisman CM, Meijboom RH. Patients’ drug-information needs: a brief view on questions asked by telephone and on the Internet. Pharm World Sci. 2002;24(2):43–45. | ||
Sage A, Carpenter D, Sayner R, et al. Online Information-Seeking Behaviors of Parents of Children With ADHD. Clin Pediatr. 2018;57(1):52–56. | ||
Abraham O, Brothers A, Alexander DS, Carpenter DM. Pediatric medication use experiences and patient counseling in community pharmacies: Perspectives of children and parents. J Am Pharm Assoc. 2017;57(1):e32:38–46. | ||
Twigg MJ, Bhattacharya D, Clark A, et al. What do patients need to know? A study to assess patients’ satisfaction with information about medicines. Int J Pharm Pract. 2016;24(4):229–236. | ||
Mamen AV, Håkonsen H, Kjome RL, Gustavsen-Krabbesund B, Toverud EL. Norwegian elderly patients’ need for drug information and attitudes towards medication use reviews in community pharmacies. Int J Pharm Pract. 2015;23(6):423–428. | ||
Yi ZM, Zhi XJ, Yang L, et al. Identify practice gaps in medication education through surveys to patients and physicians. Patient Prefer Adherence. 2015;9:1423–1430. | ||
Kazaryan I, Sevikyan A. Patients in need of medicine information. Int J Risk Saf Med. 2015;27(Suppl 1):S21–S22. | ||
Mahler C, Jank S, Hermann K, Haefeli WE, Szecsenyi J. Information zur Medikation – wie bewerten chronisch kranke Patienten das Medikationsgespräch in der Arztpraxis? [Information on medications – How do chronically ill patients assess counselling on drugs in general practice?] Dtsch Med Wochenschr. 2009;134(33):1620–1624. German. | ||
Ho CH, Ko Y, Tan ML. Patient needs and sources of drug information in Singapore: is the Internet replacing former sources? Ann Pharmacother. 2009;43(4):732–739. | ||
Newby DA, Hill SR, Barker BJ, Drew AK, Henry DA. Drug information for consumers: should it be disease or medication specific? Results of a community survey. Aust N Z J Public Health. 2001;25(6):564–570. | ||
van Geffen EC, Kruijtbosch M, Egberts AC, Heerdink ER, van Hulten R. Patients’ perceptions of information received at the start of selective serotonin-reuptake inhibitor treatment: implications for community pharmacy. Ann Pharmacother. 2009;43(4):642–649. | ||
Zwaenepoel L, Bilo R, De Boever W, et al. Desire for information about drugs: a survey of the need for information in psychiatric in-patients. Pharm World Sci. 2005;27(1):47–53. | ||
Lamberts EJ, Bouvy ML, van Hulten RP. The role of the community pharmacist in fulfilling information needs of patients starting oral antidiabetics. Res Social Adm Pharm. 2010;6(4):354–364. | ||
Nair K, Dolovich L, Cassels A, et al. What patients want to know about their medications. Focus group study of patient and clinician perspectives. Can Fam Physician. 2002;48:104–110. | ||
Raynor DK, Savage I, Knapp P, Henley J. We are the experts: people with asthma talk about their medicine information needs. Patient Educ Couns. 2004;53(2):167–174. | ||
Borgsteede SD, Karapinar-Çarkit F, Hoffmann E, Zoer J, van den Bemt PM. Information needs about medication according to patients discharged from a general hospital. Patient Educ Couns. 2011;83(1):22–28. | ||
Ziegler DK, Mosier MC, Buenaver M, Okuyemi K. How much information about adverse effects of medication do patients want from physicians? Arch Intern Med. 2001;161(5):706–713. | ||
Meredith C, Symonds P, Webster L, et al. Information needs of cancer patients in west Scotland: cross sectional survey of patients’ views. BMJ. 1996;313(7059):724–726. | ||
Tarn DM, Paterniti DA, Williams BR, Cipri CS, Wenger NS. Which providers should communicate which critical information about a new medication? Patient, pharmacist, and physician perspectives. J Am Geriatr Soc. 2009;57(3):462–469. | ||
Herber OR, Gies V, Schwappach D, Thürmann P, Wilm S. Patient information leaflets: informing or frightening? A focus group study exploring patients’ emotional reactions and subsequent behavior towards package leaflets of commonly prescribed medications in family practices. BMC Fam Pract. 2014;15:163. | ||
Barnett GC, Charman SC, Sizer B, Murray PA. Information given to patients about adverse effects of radiotherapy: a survey of patients’ views. Clin Oncol (R Coll Radiol). 2004;16(7):479–484. | ||
Tarn DM, Wenger A, Good JS, Hoffing M, Scherger JE, Wenger NS. Do physicians communicate the adverse effects of medications that older patients want to hear? Drugs Ther Perspect. 2015;31(2):68–76. | ||
Hirsh D, Clerehan R, Staples M, Osborne RH, Buchbinder R. Patient assessment of medication information leaflets and validation of the Evaluative Linguistic Framework (ELF). Patient Educ Couns. 2009;77(2):248–254. | ||
Berry DC, Knapp P, Raynor DK. Provision of information about drug side-effects to patients. Lancet. 2002;359(9309):853–854. | ||
Büchter RB, Fechtelpeter D, Knelangen M, Ehrlich M, Waltering A. Words or numbers? Communicating risk of adverse effects in written consumer health information: a systematic review and meta-analysis. BMC Med Inform Decis Mak. 2014;14:76. | ||
Laaksonen R, Duggan C, Bates I. Desire for information about drugs: relationships with patients’ characteristics and adverse effects. Pharm World Sci. 2002;24(5):205–210. | ||
Hamrosi KK, Raynor DK, Aslani P. Pharmacist and general practitioner ambivalence about providing written medicine information to patients-a qualitative study. Res Social Adm Pharm. 2013;9(5):517–530. | ||
McGrath JM. Physicians’ perspectives on communicating prescription drug information. Qual Health Res. 1999;9(6):731–745. | ||
Lamb GC, Green SS, Heron J. Can physicians warn patients of potential side effects without fear of causing those side effects? Arch Intern Med. 1994;154(23):2753–2756. | ||
Krag A, Nielsen HS, Norup M, Madsen SM, Rossel P. Research report: do general practitioners tell their patients about side effects to common treatments? Soc Sci Med. 2004;59(8):1677–1683. | ||
Liseckiene I, Liubarskiene Z, Jacobsen R, Valius L, Norup M. Do family practitioners in Lithuania inform their patients about adverse effects of common medications? J Med Ethics. 2008;34(3):137–140. | ||
Tarn DM, Heritage J, Paterniti DA, Hays RD, Kravitz RL, Wenger NS. Physician communication when prescribing new medications. Arch Intern Med. 2006;166(17):1855–1862. | ||
Krska J, Morecroft CW, Poole H, Rowe PH. Issues potentially affecting quality of life arising from long-term medicines use: a qualitative study. Int J Clin Pharm. 2013;35(6):1161–1169. | ||
Mutebi A, Warholak TL, Hines LE, Plummer R, Malone DC. Assessing patients’ information needs regarding drug-drug interactions. J Am Pharm Assoc. 2013;53(1):39–45. | ||
Mody SK, Haunschild C, Farala JP, Honerkamp-Smith G, Hur V, Kansal L. An educational intervention on drug interactions and contraceptive options for epilepsy patients: a pilot randomized controlled trial. Contraception. 2016;93(1):77–80. | ||
Young A, Tordoff J, Smith A. “What do patients want?” Tailoring medicines information to meet patients’ needs. Res Social Adm Pharm. 2017;13(6):1186–1190. | ||
Indermitte J, Reber D, Beutler M, Bruppacher R, Hersberger KE. Prevalence and patient awareness of selected potential drug interactions with self-medication. J Clin Pharm Ther. 2007;32(2):149–159. | ||
Dohle S, Dawson IG. Putting knowledge into practice: Does information on adverse drug interactions influence people’s dosing behaviour? Br J Health Psychol. 2017;22(2):330–344. | ||
Waters EA, Weinstein ND, Colditz GA, Emmons K. Explanations for side effect aversion in preventive medical treatment decisions. Health Psychol. 2009;28(2):201–209. | ||
Myers ED, Calvert EJ. Information, compliance and side-effects: a study of patients on antidepressant medication. Br J Clin Pharmacol. 1984;17(1):21–25. | ||
Howland JS, Baker MG, Poe T. Does patient education cause side effects? A controlled trial. J Fam Pract. 1990;31(1):62–64. | ||
Adam TJ, Vang J. Content and Usability Evaluation of Patient Oriented Drug-Drug Interaction Websites. AMIA Annu Symp Proc. 2015;2015:287–296. | ||
Gustafsson J, Kälvemark S, Nilsson G, Nilsson JL. Patient information leaflets – patients’ comprehension of information about interactions and contraindications. Pharm World Sci. 2005;27(1):35–40. | ||
Wali H, Grindrod K. Don’t assume the patient understands: Qualitative analysis of the challenges low health literate patients face in the pharmacy. Res Social Adm Pharm. 2016;12(6):885–892. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Med. 2009;3(3):e123–e130. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.