Back to Journals » Patient Preference and Adherence » Volume 13
How Much Information and Participation Do Patients with Inflammatory Rheumatic Diseases Prefer in Interaction with Physicians? Results of a Participatory Research Project
Authors Mattukat K ![]() , Boehm P
, Boehm P ![]() , Raberger K, Schaefer C, Keyszer G
, Raberger K, Schaefer C, Keyszer G ![]() , Mau W
, Mau W ![]()
Received 19 March 2019
Accepted for publication 25 October 2019
Published 17 December 2019 Volume 2019:13 Pages 2145—2158
DOI https://doi.org/10.2147/PPA.S209346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Kerstin Mattukat,1 Peter Boehm,2 Katja Raberger,1 Christoph Schaefer,3 Gernot Keyszer,3 Wilfried Mau1
1Institute of Rehabilitation Medicine, Martin Luther University Halle-Wittenberg, Halle (Saale), Germany; 2Federal Association of the German League Against Rheumatism, Bonn, Germany; 3Clinic for Internal Medicine II, Department of Internal Medicine, University Hospital Halle, Halle (Saale), Germany
Correspondence: Kerstin Mattukat
Institute of Rehabilitation Medicine, Martin Luther University Halle-Wittenberg, Magdeburger Street 8, Halle (Saale) 06112, Germany
Tel +49 345 557-7646
Fax +49 345 557-4206
Email [email protected]
Objective: Patient preferences for information and participation in medical decision-making are important prerequisites to realize a shared decision between patients and physicians. This paper aims at exploring these preferences in German patients with inflammatory rheumatic diseases and at identifying relevant determinants of these preferences.
Methods: In a cross-sectional survey, adult patients with rheumatoid arthritis (RA), spondyloarthritis (SA) or different connective tissue diseases (CTS) filled out a questionnaire. Data were collected via a written questionnaire (1) sent to members of a regional self-help group or (2) handed out to patients at their rheumatologist’s appointment, and (3) via an online questionnaire available nationwide. Measurements included information and participation preferences (Autonomy Preference Index; API: 0–100), as well as health-related and sociodemographic variables. Analyses included ANOVAs (group differences) and multiple regression analyses (determinants of preferences). To ensure the analysis was patient-centered we involved a trained representative of the German League Against Rheumatism as a research partner.
Results: 1616 patients returned questionnaires [44% response, 79% female, mean age 54 years, diagnoses 63% RA, 28% SA, 19% CTS]. Participants reported a concurring major preference for information but vastly different preferences for participation. A greater preference for participation was associated with female sex, younger age, higher household income, and self-help group membership. Conversely, a lower preference for participation was linked to blue-collar workers, retirement, higher confidence in the rheumatologist, and poorer health literacy.
Conclusion: Whereas patients consistently welcome comprehensive information about their disease and its different treatment options, not all patients wish to be involved in therapeutic decisions. Especially older patients with lower education status and lower health literacy, but higher confidence in their rheumatologist tend to leave the decisions rather to the physician. Different preferences should be considered in the doctor–patient communication.
Keywords: doctor–patient communication, decision making, health care, outpatient, patient-reported outcomes
Introduction
Due to early diagnosis and improved treatment options, today’s patients with an inflammatory rheumatic disease have a good chance of living lives without major impairments of their daily activities or social participation.1,2 These treatment options are pharmacological and non-pharmacological as well as aids and remedies offered by an interdisciplinary network including the rheumatologist, other medical specialists, health professionals, and patient organizations.3 Within the framework of the German health care system, patients can receive state-of-the-art treatment regardless of age, sex, location, socioeconomic status, or ethnic background. However, the decision as to which available treatment option is the best for the individual patient is mostly a matter of physician-patient communication. Usually, the choice of treatment should be based upon a shared decision between patient and rheumatologist.4,5 In clinical practice, shared decision-making (SDM) includes the physician’s explanation of the different treatment options, the exchange of views on their pros and cons with the patient, and finally, a joint decision that leaves both satisfied.6,7 Furthermore, the patient’s personal values, preferences, opinions, and background should play a crucial role in these decision processes.7
Unfortunately, SDM requires time that is routinely not available in the outpatient (or acute) clinical setting. As the German Society for Rheumatology recently noted, only about half of the required internal rheumatologists are getting involved in outpatient care.3 Because of this undersupply, the time-per-patient is limited and so are the possibilities to implement SDM in everyday clinical practice.
Previous studies have found that the fit between participation preferences and experiences is fundamentally important for improving treatment outcomes, such as treatment adherence, patient satisfaction, and other patients’ reported outcomes.8,9 Unfortunately, the patient’s individual preferences are often ignored during medical decision-making.10,11 In a recent review, the mean of congruence between preference for and perceived participation in medical decision-making was 60% across 52 patient samples, most of them suffering from cancer.12 Despite widespread belief that greater participation in health decisions is associated with better health-related outcomes for patients, systematic reviews revealed that positive effects of SDM were available for less than half of the analyzed patient-reported outcomes (PROs).13,14 Positive associations with SDM were found for psychosocial and affective-cognitive outcomes, respectively, compared to behavioral and health outcomes.13,14 The neglect of patient preferences may play a crucial role in this context.
In the field of rheumatology, previous research has mainly been focusing on therapeutic decisions regarding pharmacological treatment options.15–25 Hence, patients’ preferences for SDM on non-pharmacological treatment options (eg, physiotherapy, occupational therapy, rehabilitation services) or recommended lifestyle changes remain unclear. Given the high degree of non-adherence in these important fields of disease management, it would be crucial to explore these preferences, identify important influencing factors, and develop interventions oriented towards improving patient participation in medical decision-making.
On a more global level, only few studies focused on rheumatic patients’ need for information and for involvement in decision-making, and the quality of SDM communication between providers and rheumatic patients, respectively.26–29 Rheumatoid arthritis (RA) patients were almost exclusively the target group of rheumatologic studies, while patients with other inflammatory rheumatic diseases were rarely included. In previous studies, the need for (specific) information of RA patients was high while their need for involvement in (specific) decision-making was low(er).16,19,20,24,26,30 From an international perspective, different health care systems may “generate” different patient preferences on the surface. Influencing factors of these preferences might in turn recreate comparability on the individual level. However, so far, no study analyzed the preferences for information and participation of patients with RA and various other inflammatory rheumatic diseases at the same time, in the same language and with the same assessment instruments. This approach enables global analysis on patient preferences as well as more detailed analysis to estimate the influence of different diseases on the individual level of patient preference.
Regarding influencing factors of patient preferences, the most investigated factors were sex, age, and education level. Higher preference for information was associated with female sex, current employment, and higher education level.24,26 Higher participation preference was associated with female sex, younger age, and greater knowledge of RA.16,23,26 However, not all associations of preferences with age were significant.16,19 Instead, the duration of disease might play a role in the decision-making process: After living with RA for many years, many patients reported that their involvement had evolved from a paternalistic decision-making to a shared decision-making.18 These patients attributed the change in involvement to the development of a trusting relationship with their physician, as well as to becoming educated about the disease.18 An international finding approved that good doctor-patient communication regarding treatment cannot be taken for granted: While 90% of the physicians were satisfied with their communications with their patients regarding RA treatment, 61% of the patients felt uncomfortable raising concerns or fears with their physician.31 Suboptimal SDM communication from the patient perspective was associated with a lack of confidence in the physician, older age, poor English-language proficiency, and low health literacy.28 Active patient participation in the medical consultation and higher levels of confidence in the physician were positively linked to various patient-reported outcomes (eg, lower disease activity, better global health, greater treatment satisfaction, and more positive beliefs about control of the disease).32 In our study, we included most of the previous detected covariates on patient preferences in RA to examine their associations with the preferences while controlling for different rheumatic diseases. Furthermore, we included some promising covariates that to our knowledge have never been analyzed in this context before, such as the patients’ social background, illness perception or self-help group membership.
To summarize previous findings, we know that
- patients with inflammatory rheumatic diseases have a high preference for information, but a low(er) preference for participation in decision-making regarding pharmacological treatment options,
- women, younger and higher educated patients tend to report higher preferences for participation, and
- a more active role in the decision-making process is associated with better patient-reported outcomes.
It is important to bear in mind that most of these findings relate to surveys with RA patients and pharmacological treatment decisions only.
We do not know
- how much information and participation in decision-making do patients with different inflammatory rheumatic diseases prefer in the context of pharmacological as well as non-pharmacological treatment decisions,
- if there are similar associations of preferences with sex, age, and education level for patients with other inflammatory rheumatic diseases except RA, and
- if there are other important environmental and personal factors relating to preferences of patients with different inflammatory rheumatic diseases that can be identified and that were partly not considered before.
To close these research gaps, our survey targeted at German patients with different inflammatory rheumatic diseases in different care contexts. As usual in exploratory research, we used various assessments to detect important influencing factors on the main target variables, ie, the patients’ preference for information and participation. Detailed knowledge about preferences could lead to new opportunities to enhance patient empowerment and involvement in treatment decisions. This, in turn, might lead to improved treatment satisfaction and adherence in the short-term and better health outcomes for all patients in the long term.
Materials and Methods
Study Design and Patient Research Partnership
This study was conducted in cooperation with the University Hospital of the Martin Luther University Halle-Wittenberg and the patient self-help association German League Against Rheumatism (GLAR). To help keep our study patient-oriented, we asked the Federal Association of the GLAR for support by a patient research partner (PRP). The Association’s PRPs are persons with rheumatic musculoskeletal diseases who are involved in research projects. The EULAR (European League Against Rheumatism = European organisation of scientists, physicians, other health care professionals and patients) defines PRPs as
Persons with a relevant disease who operate as active research team members on an equal basis with professional researchers, adding the benefit of their experiential knowledge to any phase of the project. (p. 722)33
According to the EULAR,
Patient participation ensures better representation of their needs and uncertainties, and helps preventing a potential mismatch between their preferences and the scientific focus in research. (p. 722)33
PRPs can be involved in the development and planning of a research project, the realization of research, the analysis of data, and the interpretation and distribution of research results. There are four levels of participation: consultation, contribution, collaboration, and control.34
In this project, the PRP of the GLAR participated in:
- implementation of research and analysis of data; interpreting the outcomes (on the levels of consultation, contribution, and collaboration),
- distribution (publication) and implementation of the research results (on the levels of contribution and collaboration).
Participants
Inclusion criteria for participants were:
- diagnosis of an inflammatory rheumatic disease according to the International Statistical Classification of Diseases and Related Health Problems (ICD-10-GM), ie, rheumatoid arthritis (RA; M05, M06), juvenile arthritis (M08), spondyloarthritis (L40.5/M07 [psoriatic arthritis], M45 [ankylosing spondylitis]), or connective tissue diseases (M32 [systemic lupus eythematosus], M33 [dermatomyositis/polymyositis], M34 [scleroderma/systemic sclerosis], M35.0 [Sjögren’s syndrome], M35.1 [mixed connective tissue disease]),
- minimum age of 18 years,
- residence in Germany with access to the German health care system.
Patients were contacted in three different ways:
- Members of a regional self-help group (GLAR Saxony-Anhalt) received a letter with a written questionnaire (mail group; first study phase).
- An online questionnaire was introduced to patients via different online forums and social media platforms, eg, www.rheuma-online.de, facebook groups (online group; first study phase).
- Patients at their rheumatologist’s appointment received the questionnaire along with a study information, a return envelope, and the request to participate in the study (outpatient group; second study phase).
Dropouts
The response rate for the initial 800 mailings to GLAR members was 45% (n = 363). As for the online survey, 657 people started to fill out the questionnaire, though only 436 completed it. Mean fill-out time was 27 mins and most participants (90%) completed the questionnaire within 46 mins. Dropouts broke off the online questionnaire within 7 mins (25%), 11 mins (50%), and 16 mins (75%) or after 55 mins at the latest. Online dropouts and online participants reported no differences regarding information and participation preferences or regarding health and sociodemographic-related variables. Another 46 persons were excluded for various reasons (other diagnosis, residence outside Germany). In the end, complete data sets were available for 390 online participants. The response rate for the outpatient survey was 46% (n=863), varying between the different rheumatologists from 5% to 96%. Figure 1 depicts the flow of participants in the study.
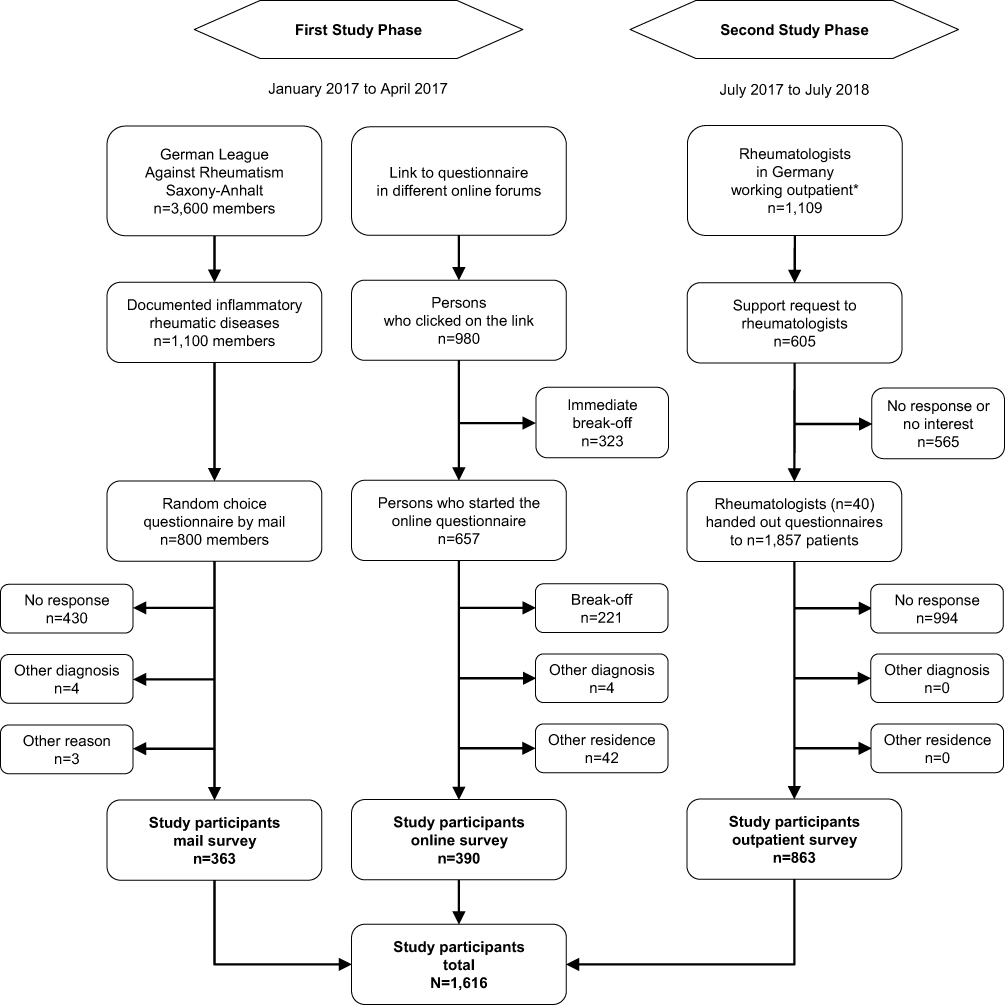 |
Figure 1 Flow of participants.Note: *Data from reference 35. |
Assessments
The 18-page questionnaire (DIN A4) included items on information and participation preferences (main outcomes), different health-related and sociodemographic variables. Standardized assessments were administered where possible. A copy of the (German) questionnaire is available from the authors on request.
Main Outcomes
The German version of the Autonomy Preference Index (API-Dm) was administered to measure the patient’s preferences for information (7 items) and participation (4 items) in medical decision-making.11 Items were scored on a 5-point Likert-scale from 1 (totally disagree) to 5 (totally agree). Mean sum scores were transformed into total scores ranging from 0 to 100, with higher scores indicating a greater preference for information or participation.
Health-Related Variables
Health status, pain, and fatigue were assessed as 1-item scores with numeric rating scales (NRS) ranging from 0 (worst) to 10 (best) for the health status and 0 (no pain/no fatigue) to 10 (total pain/total fatigue) for the symptoms, respectively. Disease-related information included the kind of inflammatory rheumatic disease(s), time since diagnosis, and other chronic diseases.
The patient’s confidence in their rheumatologist was assessed with only one item of the German Trust in Physician Scale (TPS; “I feel my rheumatologist does everything he/she should for my medical care”) scored from 1 (not at all true) to 5 (absolutely true).36,37 The authors chose this item due to its high correlation with the sum score of the TPS, aiming at limiting the total length of the questionnaire.36
The German Arthritis Impact Measurement Scales 2 - Short Form (AIMS2-SF) assessed functional status and quality of life with 26 items forming five subscales (“physical functioning”, “symptoms”, “affect”, “social interaction”, and “role function”).38 Scores ranged from 0 to 10, with higher scores indicating a worse outcome.
The Brief Illness Perception Questionnaire (BIPQ) is a 9-item scale designed to assess the cognitive and emotional representations of illness.39 In this study, participants were asked to answer the first eight questions on numeric rating scales from 0 to 10, while the ninth item asking for the assumed causes of the disease was skipped.
The Health Education Literacy of Patients with chronic musculoskeletal diseases (HELP) questionnaire comprises 18 items.40 Patients stated their difficulties in consultations with physicians regarding their “comprehension of medical information” (6 items), “applying medical information” (5 items), and “communicative competence in provider interactions” (7 items) on a 5-point scale from 1 (no difficulties) to 5 (strong difficulties). Means are reported for each subscale, with higher values indicating more difficulties/lower health literacy.
Symptoms of depression were assessed with the Patient Health Questionnaire (PHQ-8).41 Patients were asked to rate their symptoms of depression from the previous two weeks according to the ICD-10-GM. Items were answered on a 4-point scale from 0 (not at all) to 3 (almost every day). The analysis of a summarized severity score (0–24) allows the level of depression to be graded (0–4 = minimal, 5–9 = mild, 10–14 = moderate, 15–19 = moderately severe, 20–24 = severe).
Sociodemographics
Finally, participants stated their age, gender, education level, employment status, most recent work position, and net household income.
Statistical Methods
Differences between study participants in the three groups (mail, online and outpatient) were analyzed with analyses of variance (ANOVA; normal distribution) and Kruskal–Wallis tests (ANOVAs; no normal distribution), respectively, for metric variables, and with Chi-square tests for categorical variables. We depict the level of significance (p-values) for single analyses.
Determinants of the preference for information and participation were analyzed in three steps: First, univariate linear regression analyses were computed with one possible determinant as a predictor. The effect size f is displayed for variables at the 5%-level. By convention, f effect sizes of 0.10, 0.25, and 0.40 are regarded as small, medium, and large, respectively. Second, variables at the 5%-level were tested for collinearity (r > 0.5) and excluded if necessary. Finally, the remaining variables served as predictors in a multiple linear regression analysis with a stepwise forward approach (considering variables at the 5%-level in every step). All analyses were conducted with IBM SPSS 25.0.
Results
Participants
The sample included 1616 patients with one (83.5%), two (14.6%), three (1.7%) or four (0.2%) inflammatory rheumatic diseases (M = 1.2, SD = 0.4). Participants were mainly female and ranged from 18 to 85 years of age. Sample characteristics are shown in Table 1.
 |
Table 1 Sample Characteristics as Means (M) and Standard Deviations (SD) Unless Otherwise Stated |
Sociodemographic differences between the mail, online and outpatient participants were observed across almost all variables: Online participants were younger, almost exclusively female, more often employed, and had a higher education level and household income. Online participants reported a diagnosis of RA less often, but more often a diagnosis of Sjögren’s syndrome or systemic lupus erythematosus. Mail participants reported a longer duration of disease and higher comorbidity. However, the burden of the disease(s) seemed to be highest in the online group as indicated by symptoms of depression and impairments to physical, mental and social functioning (eg, AIMS2-SF scores, fatigue, pain, and BIPQ scores), while outpatient participants reported the best functional scores. Regarding their health literacy, mail participants reported greater problems understanding medical information while online participants reported more problems in the communication with physicians.
Preference for Information
The preference for information in medical decision-making was assessed with 7 items summed and transformed to a score ranging from 0 to 100. The internal consistency (Cronbach’s alpha) of this score was α = 0.813. The preference for information was very high for almost all participants (M = 92.4, SD = 10.8). The box plots in Figure 2A show the distribution and variability of the preferences for information of the three study groups (including minimum, first quartile, median, third quartile, and maximum; points characterize statistical outliers). Participants reported comparable preferences for information (mail group: M = 93.3, SD = 10.8; online group: M = 92.1, SD = 9.9; outpatient group: M = 92.1, SD = 11.2; ANOVA: not significant).
 |
Figure 2 Preference for information (A) and participation (B) in medical decision-making of the three study groups.Note: The Autonomy-Preference-Index (API) was used to assess the main outcomes.11 |
In the univariate analysis, a higher preference for information correlated to a higher age of the participants. Accordingly, people with an old age pension reported a higher preference for information. Preferences were also higher for participants with a higher confidence in their rheumatologist, and for persons with less difficulty to apply medical information and to communicate with their physicians, ie, for persons with a higher health literacy. Illness perceptions according to a higher concern and a higher coherence correlated positively to a higher preference for information. Persons with a higher preference for participation and employed people tended to have a lower preference for information. Effect sizes were small to medium.
In the multivariate regression analysis, age and illness perceptions explained the variance in preference for information (corrected R2 = 0.040; see Table 2).
 |
Table 2 Predictors of the Preference for Information (API: 0–100)11 (Univariate and Multivariate Analyses) |
Preference for Participation
The preference for participation in medical decision-making was assessed with 4 items summed and transformed to a score ranging from 0 to 100. The internal consistency (Cronbach’s alpha) of this score was α = 0.845. The preference for participation varied substantially between study participants (M = 43.9, SD = 24.7; see box plots in Figure 2B). Online participants (M = 57.4, SD = 21.9) reported a higher preference for participation compared to the mail group (M = 41.8, SD = 24.3) and the outpatient group (M = 38.4, SD = 23.8; ANOVA: p < 0.001).
In the univariate analysis, the online group reported a higher preference and the outpatient group reported a lower preference for participation (dichotomous dummy variables; Table 3). Preference for participation was positively correlated with younger age, female gender, high household income, higher education level, and current working status. Old-age pension and blue-collar work were associated with a lower preference for participation. RA patients reported a lower preference for participation, while SA and Sjögren’s patients reported a higher preference for participation. Poor health status, as indicated by more severe fatigue, depressive and rheumatic symptoms, as well as by worse AIMS2-SF scores of affect and social interaction, was associated with a higher preference for participating in medical decision-making. Higher confidence in the rheumatologist and in the control of the disease by the rheumatologic treatment correlated to a lower preference for participation. This preference was also lower for individuals who found comprehension of medical information more difficult and for individuals who had less problems to communicate with their physicians. Finally, members of self-help groups reported a higher preference for participation. Effect sizes were small to medium (f ≤ 0.34).
 |
Table 3 Predictors of the Preference for Participation (API: 0–100)11 (Univariate and Multivariate Analyses) |
In the multivariate regression analysis, online participation, age, sex, household income, old-age pension, blue-collar work, confidence in rheumatologist, problems to understand medical information and membership in self-help group were independent predictors of the preference for participation (R2 = 0.210; see Table 3).
Discussion
International treatment guidelines and recommendations of patient organizations refer to the informed and autonomous patient who decides which therapy is best for him or her in consultation with the attending physician.42 In terms of rheumatologic care research, investigators recently looked at RA patient preferences with respect to pharmaceutical treatment and their experiences with SDM communication. However, rheumatologic research had not extensively addressed the patient’s perspective on their treatment or their preferences for information or involvement in medical decisions in general. Furthermore, patients with other inflammatory rheumatic diseases besides RA are rarely investigated regarding patient preferences and SDM. This study explored the preferences for information and participation in adult patients with RA as well as other inflammatory rheumatic diseases. In addition, we examined important determinants of these preferences that had in part not yet been considered before.
Summary of Findings
In this observational study, questionnaire data were collected from 363 members of a regional self-help group using mailed letters, from 390 patients participating in a nationwide online survey, and from 863 outpatients recruited at the visit to their rheumatologist. These three groups differed largely in terms of sociodemographic and health-related characteristics including rheumatic disease entities.
Almost all participants reported a high preference for information on their inflammatory rheumatic disease and different treatment options as it was found in recent studies.19,24,26 No differences occurred between the three study groups. Due to the small overall variance of this preference, determinants explaining this variance were not detectable. Univariate significant variables (age, concern for and understanding of the disease) explained only 4% of the variance in the multiple regression analysis.
In contrast to the homogeneous preference for information, participants reported varying preferences regarding the participation in medical decision-making. This result is comparable to samples with other chronic conditions and to findings of RA patients as well.26,43 In this study, online participants reported a higher preference for participation compared to the mail group and the outpatient group. Women and younger patients preferred more involvement, which is in line with recent studies and other study samples.12,16,23,26 Consequently, old-age pensioners reported a lower preference for involvement, while employed people preferred more involvement. Patients with a higher household income reported a higher preference, while blue-collar workers reported a lower preference for participation. Both characteristics may serve as indicators of education that was positively associated with a higher preference for participation in this study as well as in other samples.12 In this sample, RA patients reported a lower preference for participation while patients with Spondylarthritis and patients with Sjögren’s syndrome reported a higher need for participation compared to the study sample. However, these rather small effects of the univariate analyses did not persist in the multivariate analysis where other factors remained significant. For example, higher confidence in the rheumatologist correlated to a lower preference for participation in our sample. In line with that, previous researcher had found an association between suboptimal patient-provider SDM communication and low patient confidence in the physician in RA patients.28 Other findings suggested a correlation between growing confidence in the physician and increasing participation in medical decisions.18 The preference for participation was higher for persons with higher health literacy and for members of self-help organizations. As health literacy involves the ability to understand medical facts, to communicate with the physician competently, and to make medical decisions, low health literacy had been associated with suboptimal provider-patient SDM communication in RA before.28 Involvement and activity in self-help communities might provide knowledge of the disease and might as well be helpful to enhance communication skills and health literacy. Interventions that positively influence the provider-patient communication and enhance the autonomous role of the patients in medical decision-making are of interest. An improved participation in medical decision-making might be helpful to increase the patient’s adherence in the long run.44,45
Limitations of the Study
This exploratory study generated, rather than tested, hypotheses about preferences for information and participation. Due to a lack of previous studies in this research area, an observational study was conducted at one time of measurement. Since cross-sectional data are not suitable for discovering causal pathways, our findings display relationship trends and correlations rather than influencing factors or predictors. Furthermore, the results of this study must be interpreted with caution, as all investigated groups are highly self-selective: the mail group due to their GLAR membership, the online participants due to their engagement in online forums, and the outpatients due to selection by the rheumatologists and their staff. Influencing factors played a negligible role in the explained variance of the preference for information and still a rather small role in explaining the preference for participation. The participants’ preference for involvement in medical decision-making may be influenced by factors other than those assessed in our questionnaire, such as different aspects of doctor-patient communication. Furthermore, different assessments of patient preferences might have generated different findings regarding preferences and their determinants.43
Strengths of the Study
This was the first exploration of preferences for information and participation according to the principles of SDM regarding various treatment modalities in a large sample (n=1616) of patients with RA and various other inflammatory rheumatic diseases. Due to the different means of access, we were able to include very different groups of patients as study participants. The findings of this study provide an important insight (i) into the very high preference for information across all patient groups, (ii) into different preferences for participation according to the principles of SDM between these patient groups, and (iii) into partly new, important determinants of these preferences after controlling for the inflammatory rheumatic disease(s).
Conclusions
All patients – regardless of age, sex, education level, and duration of disease – should receive adequate information on their disease and treatment options. Potential providers of information are physicians, receptionists, and other healthcare professionals, as well as the staff of regional and national self-help groups. Types of information may vary as well as level of detail. A layered approach might be helpful so that the patients can access the level of information that they want. Accessing information online is now easy, especially for younger patients. However, patients still value their attending physician as important advisor to provide new information on the disease and its treatment as well as to discuss and evaluate information from the internet and other sources.46,47
Beneath their high preference for information, not all patients prefer being involved in medical decision-making. Hence, shared decision-making might not be suitable for every individual. To consider individual preferences for participation in the consultation, physicians could just ask the patients to express their needs and wishes. This patient-oriented approach is in line with the aforementioned time-limited possibilities to implement SDM in everyday clinical care for all patients.3
Based on these results, we would like to give specific recommendations for clinicians:
- Give your patients comprehensive, evidence-based information about their disease and related facts of interest, eg, its medical and non-medical treatment options and important lifestyle recommendations.
- Use plain language and consider patient-preferred media for providing these information (eg, print media like brochures, trustworthy websites, useful smartphone apps).
- Recommend local self-help groups to your patients if they are interested in interacting with other patients.
- Consider your patients’ preferences for participation in all pending decisions. Attention: The best decision for the individual may not exactly be in line with the most highly recommended options of the treatment guidelines. It rather depends on the patients’ individual situations including their individual backgrounds, wishes, and preferences.
Regarding future considerations, the preference for participation cannot be increased until important determinants are improved, particularly individual health literacy.28,48 Patient education programs (e.g., communication training) might be important especially for patients with a lower education level and those who have difficulties understanding medical information. Interested providers might consider the EULAR recommendations for patient education for people with inflammatory arthritis.49 Furthermore, communication skills training for physicians particularly if they wish to share decisions with their patients can improve physician empathy and patient satisfaction.50
In order to provide best fitting interventions to patients with different rheumatic diseases, further questions should be answered by future research:
- Do different assessments of patient preferences meet the quality criteria of reliability and validity? Which assessment can be recommended for application in future research and interventions?
- Which other important influencing factors can be detected for the preference for participation (eg, kind of decision to be made, communication skills of the physician, self-esteem of the patients)?
- Which factors may change, and which ones do constantly predict patient preferences for information and participation in a longitudinal study design?
- Which means can improve response and reduce selection bias of participants (eg, incentives for study participation of patients, repeated reminders for non-responders, reduction of assessments to shorten the total questionnaire)?
Based on the knowledge of what inhibits and what facilitates patient involvement in medical decision-making, further research should lead to the consideration of these factors in future interventions (eg, patient training, a greater role for specialist nurses, and self-help groups) in order to improve patient-centered rheumatologic care. Finally, the investigation of potentially different target groups of these interventions (eg, newly diagnosed patients, patients with severe symptoms) may be of particular interest.
Abbreviations
AIMS2-SF, Arthritis Impact Measurement Scales 2 - Short Form; ANOVA, analysis of variance; API, Autonomy Preference Index; BIPQ, Brief Illness Perception Questionnaire; CI, confidence interval; CTS, connective tissue diseases; eg, for example; EULAR, European League Against Rheumatism; GLAR, German League Against Rheumatism; ICD, International Statistical Classification of Diseases and Related Health Problems; ie, that means; HELP, Health Education Literacy of Patients with chronic musculoskeletal diseases; M, mean (statistics); NA, not applicable; NRS, numeric rating scale; PHQ, Patient Health Questionnaire; PRO, patient-reported outcome; PRP, patient research partner; RA, rheumatoid arthritis; SA, spondyloarthritis; SD, standard deviation (statistics); SDM, shared decision-making; TPS, Trust in Physician Scale.
Ethics Approval and Informed Consent
The study was performed in accordance with the principles outlined in the Declaration of Helsinki. The Ethics Committee of the Medical Faculty of the Martin Luther University Halle-Wittenberg approved the study protocol (2016-139). Participation in the study was voluntary. Eligible patients received written or online information about study aims, participation requirements, and the right to refuse. Completion and return of the questionnaire implied informed consent. We registered the study in the German Clinical Trials Register (DRKS00011554; http://www.drks.de).
Data Sharing Statement
Selected research data are available by request from the Institute of Rehabilitation Medicine, Martin Luther University Halle-Wittenberg. Please state the title of the project, its funding number (30/09), and the aim and purpose of your request.
Acknowledgments
First, our sincere thanks go to the participants of our study. Furthermore, we would like to thank our partners in this research project, amongst them all of the engaged rheumatologists and nurses across Germany, the Deutsche Rheuma-Liga Landesverband Sachsen-Anhalt e.V. (German League Against Rheumatism Saxony-Anhalt), the Deutsche Rheuma-Liga Bundesverband (Federal Association of the German League Against Rheumatism), our diligent research assistants, and our supportive colleagues at the Medical Faculty of the Martin Luther University Halle-Wittenberg for their valuable collaboration.
Authors’ Information
PB is the research partner from the Federal Association of the German League Against Rheumatism; KR is research fellow and KM is the leader of the research project. CS is the president of the German League Against Rheumatism Saxony Anhalt. GK is the speaker of the Rheumazentrum Halle at the University Hospital Halle (RZH); CS, WM and KM are members of the RZH.
Author Contributions
All authors contributed to conception and design, acquisition of data or data analysis, drafting or revising the article, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
Peter Boehm reports financial fees for employment from Deutsche Rheuma-Liga Berlin e. V., financial fees for lectures from Wannseeschule e. V. and Schule für Gesundheits- und Krankenpflege and non-financial support from Deutsche Rheuma-Liga e. V. and Deutsche Vereinigung Morbus Bechterew e. V. The authors report no other financial or non-financial conflicts of interest in this work.
References
1. Versteeg GA, Steunebrink LMM, Vonkeman HE, et al. Long-term disease and patient-reported outcomes of a continuous treat-to-target approach in patients with early rheumatoid arthritis in daily clinical practice. Clin Rheumatol. 2018;37:1189–1197. doi:10.1007/s10067-017-3962-5
2. Toledano E, Ortiz AM, Ivorra-Cortes J, et al. Are rheumatologists adhering to the concepts window of opportunity and treat-to-target? Earlier and more intense disease-modifying anti-rheumatic drug treatment over time in patients with early arthritis in the PEARL study. Clin Exp Rheumatol. 2018;36:382–388.
3. Zink A, Braun J, Gromnica-Ihle E, et al. Memorandum of the German society for rheumatology on the quality of treatment in rheumatology – update 2016. Z Rheumatol. 2017;76:195–207. doi:10.1007/s00393-017-0297-1
4. Smolen JS, Landewe R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76:960–977. doi:10.1136/annrheumdis-2016-210715
5. Singh JA, Saag KG, Bridges SL, et al. 2015 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken). 2016;68:1–25. doi:10.1002/acr.22783
6. Elwyn G, Laitner S, Coulter A, et al. Implementing shared decision making in the NHS. BMJ. 2010;341:c5146. doi:10.1136/bmj.c5146
7. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27:1361–1367. doi:10.1007/s11606-012-2077-6
8. Lee -Y-Y, Lin JL. Do patient autonomy preferences matter? Linking patient-centered care to patient-physician relationships and health outcomes. Soc Sci Med. 2010;71:1811–1818. doi:10.1016/j.socscimed.2010.08.008
9. Barratt A. Evidence based medicine and shared decision making: the challenge of getting both evidence and preferences into health care. Patient Educ Couns. 2008;73:407–412. doi:10.1016/j.pec.2008.07.054
10. Ende J, Kazis L, Ash A, et al. Measuring patients’ desire for autonomy: decision making and information-seeking preferences among medical patients. J Gen Intern Med. 1989;4:23–30. doi:10.1007/BF02596485
11. Simon D, Kriston L, Haerter M. The German modified version of the autonomy preference index (API-Dm). Klin Diagn Eval. 2011;4:5–14.
12. Brom L, Hopmans W, Pasman HRW, et al. Congruence between patients’ preferred and perceived participation in medical decision-making: a review of the literature. BMC Med Inform Decis Mak. 2014;14:25.
13. Clayman ML, Bylund CL, Chewning B, et al. The impact of patient participation in health decisions within medical encounters: a systematic review. Med Decis Making. 2016;36:427–452. doi:10.1177/0272989X15613530
14. Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Making. 2015;35:114–131. doi:10.1177/0272989X14551638
15. Fraenkel L, Matzko CK, Webb DE, et al. Use of decision support for improved knowledge, values clarification, and informed choice in patients with rheumatoid arthritis. Arthritis Care Res (Hoboken). 2015;67:1496–1502. doi:10.1002/acr.v67.11
16. Chilton F, Collett RA. Treatment choices, preferences and decision-making by patients with rheumatoid arthritis. Musculoskeletal Care. 2008;6:1–14. doi:10.1002/(ISSN)1557-0681
17. Li LC, Shaw CD, Lacaille D, et al. Effects of a web-based patient decision aid on biologic and small-molecule agents for rheumatoid arthritis: results from a proof-of-concept study. Arthritis Care Res (Hoboken). 2018;70:343–352. doi:10.1002/acr.v70.3
18. Mathews AL, Coleska A, Burns PB, et al. Evolution of patient decision-making regarding medical treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken). 2016;68:318–324. doi:10.1002/acr.v68.3
19. Nota I, Drossaert CHC, Taal E, et al. Patient participation in decisions about disease modifying anti-rheumatic drugs: a cross-sectional survey. BMC Musculoskelet Disord. 2014;15:333. doi:10.1186/1471-2474-15-333
20. Aoki A, Suda A, Nagaoka S et al. Matching of patients’ actual and desired roles in treatment decision making and trust in physicians.
21. Fraenkel L, Bogardus ST, Concato J, et al. Patient preferences for treatment of rheumatoid arthritis. Ann Rheum Dis. 2004;63:1372–1378. doi:10.1136/ard.2003.019422
22. Qu H, Shewchuk RM, Alarcon G, et al. Mapping perceptions of lupus medication decision-making facilitators: the importance of patient context. Arthritis Care Res (Hoboken). 2016;68:1787–1794. doi:10.1002/acr.22904
23. Dilla T, Rentero ML, Comellas M, et al. Patients’ preferences for rheumatoid arthritis treatments and their participation in the treatment decision-making process. a systematic review of the literature. Value Health. 2015;18:A652. doi:10.1016/j.jval.2015.09.2348
24. Fraenkel L, Bogardus S, Concato J, et al. Preference for disclosure of information among patients with rheumatoid arthritis. Arthritis Rheum. 2001;45:136–139. doi:10.1002/(ISSN)1529-0131
25. Fraenkel L, Gulanski B, Wittink D. Patient treatment preferences for osteoporosis. Arthritis Rheum. 2006;55:729–735. doi:10.1002/(ISSN)1529-0131
26. Neame R, Hammond A, Deighton C. Need for information and for involvement in decision making among patients with rheumatoid arthritis: a questionnaire survey. Arthritis Rheum. 2005;53:249–255. doi:10.1002/(ISSN)1529-0131
27. Schildmann J, Grunke M, Kalden JR, et al. Information and participation in decision-making about treatment: a qualitative study of the perceptions and preferences of patients with rheumatoid arthritis. J Med Ethics. 2008;34:775–779. doi:10.1136/jme.2007.023705
28. Barton JL, Trupin L, Tonner C, et al. English language proficiency, health literacy, and trust in physician are associated with shared decision making in rheumatoid arthritis. J Rheumatol. 2014;41:1290. doi:10.3899/jrheum.131350
29. Aoki A, Ohbu S. Japanese physicians’ preferences for decision making in rheumatoid arthritis treatment. Patient Prefer Adherence. 2016;10:107–113. doi:10.2147/PPA.S95346
30. Garcia-Gonzalez A, Gonzalez-Lopez L, Gamez-Nava JI, et al. Doctor-patient interactions in Mexican patients with rheumatic disease. J Clin Rheumatol. 2009;15:120–123. doi:10.1097/RHU.0b013e31819d89bf
31. Gibofsky A, Galloway J, Kekow J, et al. Comparison of patient and physician perspectives in the management of rheumatoid arthritis: results from global physician- and patient-based surveys. Health Qual Life Outcomes. 2018;16:211. doi:10.1186/s12955-018-1035-3
32. Georgopoulou S, Prothero L, D’Cruz DP. Physician–patient communication in rheumatology: a systematic review. Rheumatol Int. 2018;38:763–775. doi:10.1007/s00296-018-4016-2
33. de Wit MPT, Berlo SE, Aanerud GJ, et al. European league against rheumatism recommendations for the inclusion of patient representatives in scientific projects. Ann Rheum Dis. 2011;70:722. doi:10.1136/ard.2010.135129
34. Sweeney A, Morgan L. Chapter 3: levels and stages. In: Wallcraft J, Schrank B, Amering M, editors. Handbook of Service User Involvement in Mental Health Research. Chichester: Wiley-Blackwell; 2009:25–36.
35. Kassenaerztliche Bundesvereinigung. Statistische Informationen aus dem Bundesarztregister. Available from: https://www.kbv.de/media/sp/2017_12_31_BAR_Statistik.pdf.
36. Glattacker M, Guelich M, Farin E, et al. Trust in the physician - psychometric testing of the German version of the “trust in physician scale”. Phys Med Rehab Kuror. 2007;17:141–148. doi:10.1055/s-2007-940008
37. Freburger JK, Callahan LF, Currey SS, et al. Use of the trust in physician scale in patients with rheumatic disease: psychometric properties and correlates of trust in the rheumatologist. Arthritis Rheum. 2003;49:51–58. doi:10.1002/(ISSN)1529-0131
38. Rosemann T, Koerner T, Wensing M, et al. Evaluation and cultural adaptation of a German version of the AIMS2-SF questionnaire (German AIMS2-SF). Rheumatology (Oxford). 2005;44:1190–1195. doi:10.1093/rheumatology/keh718
39. Broadbent E, Petrie KJ, Main J, et al. The brief illness perception questionnaire. J Psychosom Res. 2006;60:631–637. doi:10.1016/j.jpsychores.2005.10.020
40. Farin E, Ullrich A, Nagl M. Health education literacy in patients with chronic musculoskeletal diseases: development of a new questionnaire and sociodemographic predictors. Health Educ Res. 2013;28:1080–1091. doi:10.1093/her/cyt095
41. Spangenberg L, Braehler E, Glaesmer H. Identifying depression in the general population - a comparison of PHQ-9, PHQ-8 and PHQ-2. Z Psychosom Med Psychother. 2012;58:3–10. doi:10.13109/zptm.2012.58.1.3
42. Smolen JS, Aletaha D, Bijlsma JWJ, et al. Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2010;69:631–637. doi:10.1136/ard.2009.123919
43. Chewning B, Bylund CL, Shah B, et al. Patient preferences for shared decisions: a systematic review. Patient Educ Couns. 2012;86:9–18. doi:10.1016/j.pec.2011.02.004
44. Joosten EAG, DeFuentes-Merillas L, de Weert GH, et al. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77:219–226. doi:10.1159/000126073
45. Lofland JH, Johnson PT, Ingham MP, et al. Shared decision-making for biologic treatment of autoimmune disease: influence on adherence, persistence, satisfaction, and health care costs. Patient Prefer Adherence. 2017;11:947–958. doi:10.2147/PPA
46. Tan SS-L, Goonawardene N. Internet health information seeking and the patient-physician relationship: a systematic review. J Med Internet Res. 2017;19:e9. doi:10.2196/jmir.5729
47. Clarke MA, Moore JL, Steege LM, et al. Health information needs, sources, and barriers of primary care patients to achieve patient-centered care: a literature review. Health Informatics J. 2015;22:992–1016. doi:10.1177/1460458215602939
48. Hirsh JM. Can shared decision making help eliminate disparities in rheumatoid arthritis outcomes? J Rheumatol. 2014;41:1257. doi:10.3899/jrheum.140479
49. Zangi HA, Ndosi M, Adams J, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015;74:954. doi:10.1136/annrheumdis-2014-206807
50. Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016;31:755–761. doi:10.1007/s11606-016-3597-2
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.