Back to Journals » Clinical Ophthalmology » Volume 14
Horizontal Extraocular Muscle Insertion Site in Relation to Axial Length Using Swept-Source Anterior Segment OCT
Authors El-Fayoumi D, Bahgat N, Khafagy M ![]() , Hatata R, Sabry D
, Hatata R, Sabry D ![]() , Allam G, Kasem MA
, Allam G, Kasem MA ![]() , Sadek S
, Sadek S ![]()
Received 30 May 2020
Accepted for publication 1 October 2020
Published 29 October 2020 Volume 2020:14 Pages 3583—3589
DOI https://doi.org/10.2147/OPTH.S262916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Dina El-Fayoumi,1 Nermeen Bahgat,1 Mohamed Khafagy,1 Ragai Hatata,2 Dalia Sabry,3 Ghada Allam,3 Manal Ali Kasem,3 Sherin Sadek2
1Ophthalmology Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 2Ophthalmology Department, Faculty of Medicine, Fayoum University, Fayoum, Egypt; 3Mansoura Ophthalmic Centre, Faculty of Medicine, Mansoura University, Mansoura, Egypt
Correspondence: Sherin Sadek
Faculty of Medicine, Fayoum University, 2/7 Zahraa EL Maadi, 4th Floor, Dep. 45, Fayoum 11435, Egypt
Tel +20 1006232012
Email [email protected]
Purpose: The purpose of this study was to correlate between the axial length of the globe and the insertion site of horizontal extraocular muscles using swept-source anterior segment optical coherence tomography (SS-ASOCT), with posing an equation to calculate the muscle insertion site from the axial length.
Methods: The study design was observational and cross-sectional. It was performed on 157 eyes of 157 healthy subjects. The distance of the medial rectus (MR) and the lateral rectus (LR) insertion sites from the limbus were measured using SS-ASOCT. The insertion sites’ distances were correlated to the axial length (hypermetropes < 22.5 mm, myopes > 24.5). Correlation between numerical variables was done by Pearson’s correlation coefficient and confirmed by linear regression analysis and scatter diagrams.
Results: The mean MR insertion site was 5.47 ± 0.19 mm in hypermetropes versus 5.68 ± 0.23 mm in myopes, whereas the mean LR insertion site was 6.81± 0.23 mm in hyperopes versus 7.08 ± 0.16 mm in myopes. The axial length showed a moderate positive, but significant, correlation to the insertional position for the medial and lateral rectus muscles (MR: r=0.417, p< 0.001; LR: r=0.410, p< 0.001).
Conclusion: Comparing the horizontal extraocular muscle insertion site to axial length using SS-ASOCT showed a significant positive correlation. The model equation for MR insertion: MR (mm) = 4.522 + 0.045 (AXL in mm) with an R = 0.437, R2= 0.191, F=12.071, P< 0.001. The model equation for LR insertion: LR (mm) = 5.72 + 0.048 (AXL in mm) with an R = 0.438, R2= 0.192, F=12.116, P< 0.001.
Keywords: AS-OCT, axial length, extraocular muscle insertion site, swept-source OCT
Introduction
Preoperative planning for strabismus surgery depends on the insertion site of the extraocular muscles from the limbus, such distances cannot be precisely detected prior to surgery.1 Many techniques were used to measure these distances, as magnetic resonance imaging (MRI), and computed tomography (CT) scans.2–4 But, these methods were inaccurate in determining the insertion of the muscle or for measuring the distance from the limbus to the insertion site. The high cost and the risk of exposure to radiation decrease the feasibility of its use.
B-scan ultrasonography (U/S) provides better visualization but with a low-resolution image.5–7 Ultrasound biomicroscopy (UBM) produces better images than U/S but it needs contact with the globe so, it difficult to perform in children.8,9 Optical coherence tomography (OCT) is a non-contact technique allowing high-resolution imaging.
Many studies used OCT in visualizing extraocular muscles (EOMs) insertions.10–12 Liu et al were the first to use OCT to detect the insertion distance and showed good agreement with intraoperative measurements.10 A study was done by De-Pablo-Gómez-de-Liaño L et al, in 2016, to measure the distance of the horizontal rectus muscle insertion site from the limbus, using spectral domain optical coherence tomography (SD-OCT). Moreover, they correlated their results with axial length, sex, and age.13
In the current study, we used swept-source anterior segment optical coherence tomography (SS-ASOCT) to identify the horizontal muscle insertion site and to compare it with the axial length in normal subjects. We aimed at finding a correlation between the site of horizontal muscle insertion and the axial lengths in three groups (emmetropes, myopes and hypermetropes) using an equation.
Patients and Methods
This cross-sectional, descriptive study included 157 right eyes of normal individuals who were seeking correction of refractive errors or were just having minor ocular complaints, such as infective or allergic conjunctivitis. Our study group was collected from the ophthalmic investigative unit of Mansoura University.
The research was approved by the ethical committee of Mansoura Faculty of Medicine (R/17.11.54), with adherence to the tenets of Declaration of Helsinki. All participants provided informed consent.
Ophthalmological Examination
A full history was taken, and ophthalmological examination was done for all participants. Cover test was performed and patients who had any manifest deviation were excluded. Also, any of the participants with previous intraocular surgery or surgery for strabismus was excluded from the study. Demographic data including the age and the sex were also recorded.
Measurement of Axial Length
Each subject underwent axial length measurement using A-scan biometry (US Nidek 4000). After instillation of topical anesthetic eye drops, axial length reading was taken 3 times then the average was taken and recorded using contact ultrasound probe.
Based on that the mean adult values for axial length range from 22 to 25 mm,14 the participants were further subdivided according to their axial length into three groups, emmetropes (22.5–24.5 mm), myopes (AXL >24.5mm) and hypermetropes (AXL <22.5).
Measurement of EOM Insertion Site by AS-OCT
AS-OCT scan was done using Swept-Source OCT, Topcon DRI OCT (Triton plus ver.10.11, 16 mm line scan) with a special anterior segment attachment. The examination was done while the patient is sitting. Horizontal cross-section line scans with axial resolution of 7 µm center scan at 3 and 9 o’clock to visualize the horizontal rectus muscles were taken using a fixation light. The patients were asked to look at extreme temporal gaze to scan MR muscle and to look at extreme nasal gaze for the LR muscle. Horizontal line scans were taken passing through the muscle tendon parallel to the axis of the muscle (0–180) and the root of the iris. Five consecutive scans were taken and the most central one was taken. The distance from the muscle insertion (the point where the muscle tendon ends) to the anterior chamber angle (root of the iris) was measured using software caliper provided by the device. One mm was added to our measurements to compensate for the distance between the angle and the limbus, based on previous studies reported that anatomically the iris root (the anterior chamber angle) lying nearly 1.0 mm behind the limbus in the horizontal meridian.15
The scans were taken by a well-trained examiner (GA) and analyzed by another examiner (MK). The demographic data and the axial lengths measurements of the participants were masked from both examiners. To ensure interobserver reproducibility two examiners (GA, MK) measured the distance on the same image but on different days. The intra-observer reproducibility was also ensured by comparing 2 OCT images performed for each participant taken one week apart by the same examiner.
Statistical Analysis
Statistical analysis was done using IBM SPSS v21.0 statistical software (IBM corporation, USA). Descriptive statistics were calculated, and the data were summarized as range (maximum to minimum), and mean ± SD for continuous variables, while frequency and percentages were used for categorical variables. Comparisons between groups were carried out using one-way ANOVA with Bonferroni correction for post hoc analysis. Correlation between numerical variables was done by Pearson’s correlation coefficient and confirmed by linear regression analysis and scatter diagrams. The results were considered statistically significant if p-value ≤ 0.05.
Results
The right eyes of 157 normal subjects were included in the study. The data collected from all patients were summarized (Table 1). On subgroup analysis according to refractive error distribution, a significant difference in muscle insertion was detected between the three refractive error groups (One-way ANOVA, P-value <0.001, Table 2). The MR muscle insertion was farther from the limbus as the axial length progressed (Figure 1), the same was found with the LR muscle insertion. The myopic group was the farthest from the limbus, while the hyperopic group was the nearest (Table 2). These relations were statistically significant in post hoc analysis (P-value <0.05)
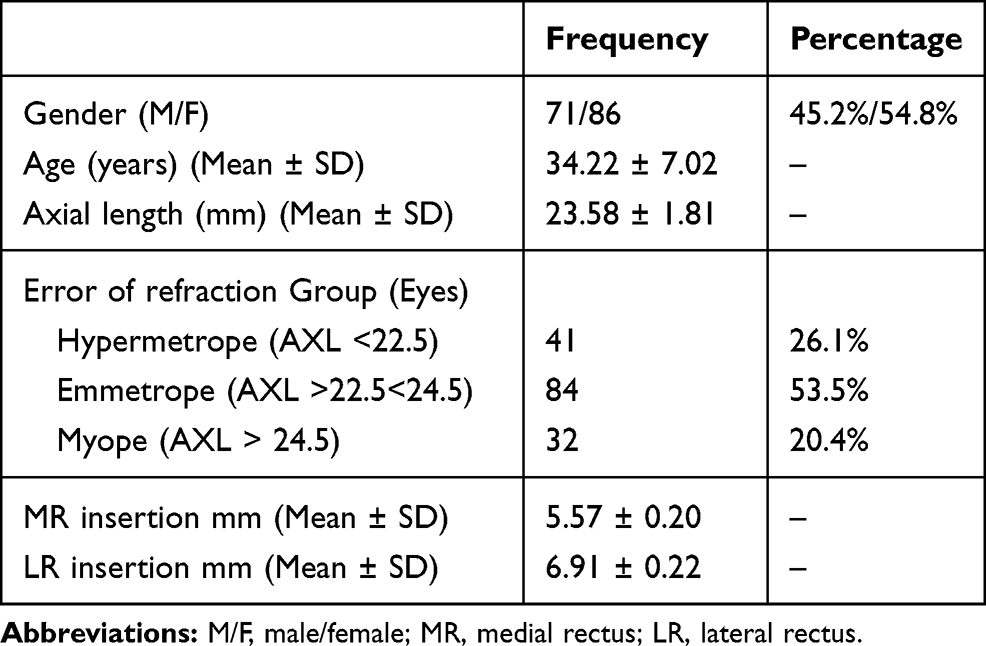 |
Table 1 Summary of the Demographic and OCT Data Obtained from the Participants in the Study (n=157) |
 |
Table 2 Summary and Comparison Between the Muscle Insertion Measured by OCT and the Refractive Error Groups (n=157) |
 |
Figure 1 (A) SS AS-OCT image for lateral rectus muscle of the right eye. The distance from the site of insertion to the iris root of hyperopic eye (AL 21mm) was measured using the caliper (5.38mm). (B) Emmetropic eye (6.06mm, AL 24.3) and (C) Myopic eye (6.40mm, AL 25.2mm). |
Correlations
On analysis of the relation between the axial length, gender and age with the muscle insertion of each muscle, we found no significant correlation between both age and gender with the insertion length for both muscles in our study group (P>0.05). The axial length correlated significantly with both insertions with a moderate positive correlation (MR: r=0.417, p<0.001; LR: r=0.410, p<0.001). Figures 2 and 3 show the scatter diagram and the regression formula between the axial length and the MR and LR muscle insertion, respectively.
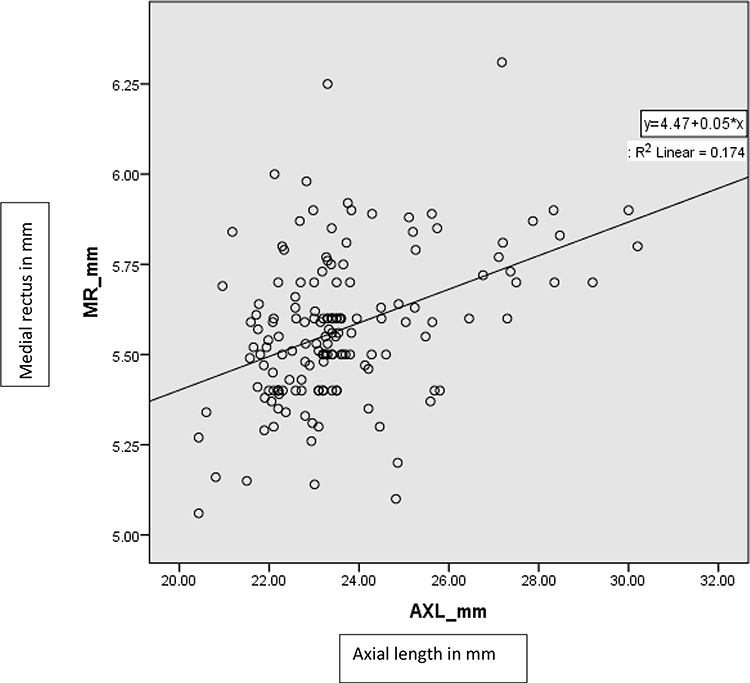 |
Figure 2 Scatter plot between MR insertion and axial length. |
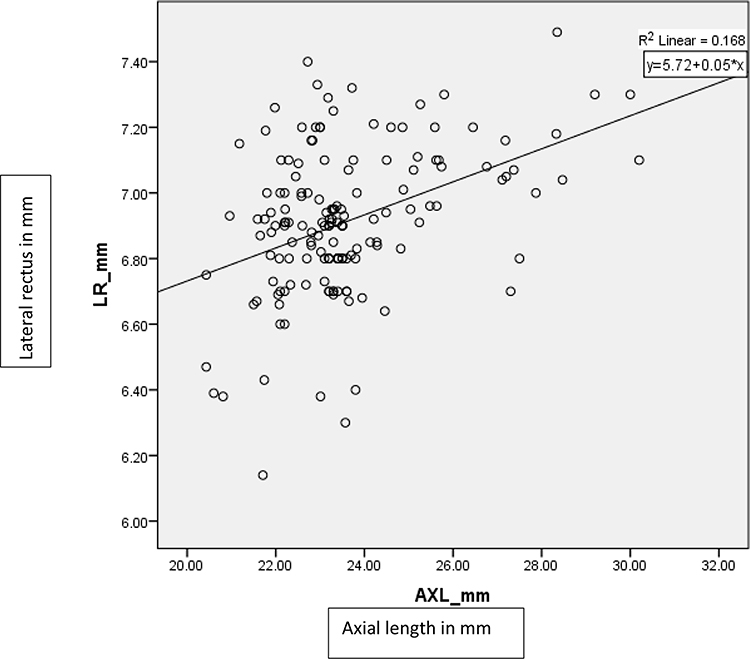 |
Figure 3 Scatter plot between LR insertion and axial length. |
Regression Analysis was carried out to predict the length of MR and LR insertion from axial length (AXL). As mentioned, the weight of the age and gender on Muscle insertion was found to be not significant (P>0.05) and only the axial length was the significant factor to be included in the model (P < 0.05). For the MR insertion the model equation was MR (mm) = 4.522 + 0.045 (AXL in mm) with an R = 0.437, R2 = 0.191, F=12.071, P<0.001. For the LR insertion the model equation was: LR (mm) = 5.72 + 0.048 (AXL in mm) with an R = 0.438, R2 = 0.192, F=12.116, P<0.001.
The models are statistically significant with an increasing trend seen in the diagrams (Figures 2 and 3), which indicates a positive relationship between the insertion of the EOM and the axial length of the eye.
Discussion
The site of the extraocular muscles’ insertion has been taken as a landmark for estimating the amount of surgery. However, it might vary in some strabismus patients depending on the axial length, age or sex of the patient. This can affect the new site of a recessed muscle.16–19
In our study, we used swept-source OCT to precisely identify the site of insertion of the horizontal extraocular muscles in 157 eyes of different axial lengths, in an adult population with a mean age of 34.22 ± 7.02 years. We correlated the insertion sites with age, sex and axial length. Our study group was divided according to axial length into 3 subgroups; emmetropes, hyperopes and myopes. The mean insertion distance of MR to the limbus was 5.57 ± 0.20 mm, and for LR was 6.91 ± 0.22 mm. These results matched with what Tillaux described that the MR and LR were inserted at 5.5 mm and 6.9 mm from the limbus, respectively.1
Watts et al used (ultrasound biomicroscopy) UBM, they found LR at an average distance of 6.4± 0.7 mm, and MR at 5.2± 0.9 mm in children.8 These numbers are much less than our results using SS-OCT, may be because of the difference in the age group, as our study included adults only.
Previous studies, using OCT for visualization of EOM showed results comparable to our results. Liu et al reported that the mean LR insertion distance was 6.80 ±0.6 mm, and the mean of MR insertion distance was 5.72 ±0.6 mm.10 Their results were very close to ours, but slightly higher for the MR.
The mean distances obtained by OCT were higher than the distances conducted by De-Pablo-Gomez-de-Liano et al. In their study they used SD-OCT, the mean LR insertion site was 6.47± 0.5 mm and MR mean insertion site was 5.22 ± 0.5 mm.13 This discrepancy is probably because in our study and in Liu et al study as well as other studies11,12 the distance was measured from the insertion site to the angle of anterior chamber, and then added 1.0 mm. However, in De Pablo-Gomez-de-liano, the distance was measured directly from the posterior limbus.13
Moreover, Liu et al found the measurements by OCT overestimated the insertion-limbus distance when compared to intra-operative measurements.10
This study is the first to use the swept-source OCT to measure the horizontal rectus muscle insertion site, and comparing it to the axial length in emmetropes, myopes and hyperopes. De-Pablo-Gomez-de-Liano et al used SD-OCT. They found the correlation between LR and MR insertion distance and sex, age, or axial length showing a longer distance in men. In their multivariate study, they stated that axial length and age were statistically nonsignificant with either LR or MR insertion distance. Their study included 187 eyes with the mean axial length was of 23.9 ± 1.6 mm in which the representation of different axial lengths was not clarified. In the present study 157 eyes were included, 53.5% emmetropes, 26.1% myopes and 20.4% hypermetropes.
On regression analysis of the relation between the axial length, gender and age with the muscle insertion of each muscle, we found no significant correlation between both age and gender with the insertion length for both muscles in our study group (P>0.05). The Axial length correlated significantly with both insertions with a moderate positive correlation (MR: r=0.417, p<0.001; LR: r=0.410, p<0.001).
Regression Analysis was used to predict the length of MR and LR insertion from axial length (AXL). For the MR insertion the model equation was MR (mm) = 4.522 + 0.045 (AXL in mm) with an R = 0.437, R2= 0.191, F=12.071, P<0.001. For the LR insertion the model equation was: LR (mm) = 5.72 + 0.048 (AXL in mm) with an R = 0.438, R2= 0.192, F=12.116, P<0.001. These equations need further validation, through intra-operative confirmation of the horizontal rectus muscle insertion site and correlating it with the axial length.
Our study had some limitations; we could not measure the insertion sites of the vertical recti muscles. As for the technique, we measured the distance from the insertion site of the muscle to the angle of anterior chamber then added 1.0 mm, as had proven by previous studies that reported the root of the iris approximately lies 1.0 mm behind the limbus. These measurements can be taken from the posterior corneoscleral limbus, and this might make the measurements more accurate.
In conclusion, the current study used SS-ASOCT to measure the limbus-insertion distance which will help in strabismus preoperative planning. In addition, the study showed that the axial length correlated positively with the EOM insertion sites for the horizontal recti. It also posed an equation to calculate the muscle insertions sites from the axial length. We recommend taking the axial length into consideration prior to any strabismus surgery. We also recommend performing other future studies on re-do strabismus cases to confirm the preoperative SS-OCT findings to the intraoperative findings.
Disclosure
The authors declare that they have no financial interest and no conflicts of interest regarding this work.
References
1. Dahlmann-Noor AH. P. J. Tillaux: of the way the muscles insert onto the sclera. Strabismus. 2008;16(4):174–175. doi:10.1080/09273970802637558
2. Ozgen A, Ariyurek M. Normative measurement of orbital structures using CT. AJR Am J Roentgenol. 1998;170(4):1093–1096. doi:10.2214/ajr.170.4.9530066
3. Ettl A, Kramer J, Daxer A, Koornneef L. High resolution magnetic resonance imaging of the normal extraocular musculature. Eye. 1997;11(6):793–797. doi:10.1038/eye.1997.207
4. Tian S, Nishida Y, Isberg B, Lennerstrand G. MRI measurements of normal extraocular muscles and other orbital structures. Graefes Arch Clin Exp Ophthalmol. 2000;238(5):393–404. doi:10.1007/s004170050370
5. Tamburrelli C, Salgarello T, Vaiano AS, Scullica L, Palombi M, Bagolini B. Ultrasound of the horizontal rectus muscle insertion sites: implications in preoperative assessment of strabismus. Invest Ophthalmol Vis Sci. 2003;44:618–622. doi:10.1167/iovs.02-0112
6. Gillies WE, McIndoe A. The use of ultrasonography in determining the amount of extraocular muscle surgery in strabismus. Aust J Ophthalmol. 1982;10:191–194.
7. Pierro L, Zaganelli E, Tavola A, Muraglia M. Extraocular muscle size comparison between normal and myopic eyes using standardized A-scan echography. Ophthalmologica. 1998;212(Suppl 1):22–24. doi:10.1159/000055415
8. Watts P, Smith D, Mackeen L, Kraft S, Buncic JR, Abdolell M. Evaluation of the ultrasound biomicroscope in strabismus surgery. J AAPOS. 2002;6(3):187–190. doi:10.1067/mpa.2002.122365
9. Solarte CE, Smith DR, Buncic JR, Tehrani NN, Kraft SP. Evaluation of vertical rectus muscle using ultrasound biomicroscopy. J AAPOS. 2008;12(2):128–131. doi:10.1016/j.jaapos.2007.06.019
10. Liu X, Wang F, Xiao Y, Ye X, Hou L. Measurement of the limbus- insertion distance in adult strabismus patients with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2011;52:8370–8373.
11. Park KA, Lee JY, Oh SY. Reproducibility of horizontal extraocular muscle insertion distance in anterior segment optical coherence tomography and the effect of head position. J AAPOS. 2014;18(1):15–20. doi:10.1016/j.jaapos.2013.11.005
12. Ngo CS, Smith D, Kraft SP. The accuracy of anterior segment optical coherence tomography (AS-OCT) in localizing extraocular rectus muscles insertions. J AAPOS. 2015;19:233–236.
13. De-Pablo-Gómez-de-Liaño L, Fernández-Vigo JI, Ventura-Abreu N, et al. Spectral domain optical coherence tomography to assess the insertion of extraocular rectus muscles. J AAPOS. 2016;20(3):201–205. doi:10.1016/j.jaapos.2016.02.011
14. Bhardwaj V, Rajeshbhai GP. Axial length, anterior chamber depth-A study in different age groups and refractive errors. J Clin Diagn Res. 2013;7(10):2211–2212.
15. Park DJJ, Karesh JW. Chapter 1. Topographic anatomy of the eye: an overview. In: Tasman W, Jaeger EA, editors. Duane’s Foundations of Clinical Ophthalmology. Vol. 1.
16. Apt L, Call NB. An anatomical re-evaluation of rectus muscle insertions. Ophthalmic Surg. 1982;13:108–112.
17. Sevel D. The origins and insertions of the extraocular muscles: development, histologic features, and clinical significance. Trans Am Ophthalmol Soc. 1986;84:488–526.
18. Barsoum-Homsy M. Medial rectus insertion site in congenital esotropia. Can J Ophthalmol. 1981;16:181–186.
19. Keech RV, Scott WE, Baker JD. The medial rectus muscle insertion site in infantile esotropia. Am J Ophthalmol. 1990;109(1):79–84. doi:10.1016/S0002-9394(14)75584-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.