Back to Journals » Clinical Ophthalmology » Volume 14
High-Resolution Wavefront-Guided Photorefractive Keratectomy and Accelerated Corneal Crosslinking for Stabilization and Visual Rehabilitation of Keratoconus Eyes
Authors Tamayo GE, Castell C, Vargas P, Polania E, Tamayo J
Received 7 February 2020
Accepted for publication 21 April 2020
Published 12 May 2020 Volume 2020:14 Pages 1297—1305
DOI https://doi.org/10.2147/OPTH.S248787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Gustavo E Tamayo, Claudia Castell, Pilar Vargas, Eduardo Polania, Juliana Tamayo
Bogota Laser Ocular Surgery Center, Bogota, Colombia
Correspondence: Gustavo E Tamayo Tel +1 305 987 0527
Email [email protected]
Purpose: To evaluate the visual and refractive outcomes after high-resolution wavefront-guided (HRWG) surface ablation with corneal crosslinking (CXL) in keratoconus eyes.
Patients and Methods: In this prospective, interventional case series, 47 eyes of 28 progressive keratoconus patients older than age 18 were enrolled. All patients underwent HRWG photorefractive keratectomy (PRK) with simultaneous accelerated CXL. The study parameters were manifest refraction spherical equivalent (MRSE), keratometric outcomes, uncorrected (UDVA) and corrected distance visual acuity (CDVA) at postoperative 6 and 12 months.
Results: There was improvement in mean MRSE from − 2.39± 1.89 D preoperatively to − 0.13 ± 0.68 D at 12 months, with corresponding improvement in UDVA from 0.77 ± 0.35 logMAR to 0.08 ± 0.12 logMAR and CDVA from 0.10 ± 0.11 logMAR to 0.02 ± 0.04 logMAR. Preoperative flat and steep keratometry (K) were 4wct 32.49 ± 1.67 D and 45.94 ± 2.10 D, respectively, and at postoperative 12 months were 41.36 ± 2.08 D and 42.65 ± 2.78 D, respectively. At postoperative 12 months, visual and refractive outcomes were maintained. Comparisons between preoperative and postoperative 12 month timepoints were statistically significant for all parameters.
Conclusion: Simultaneous wavefront-guided PRK followed by CXL is a promising treatment for the visual rehabilitation of keratoconus patients.
Keywords: keratoconus management, high-resolution wavefront-guided surface ablation with corneal crosslinking, wavefront-guided PRK with CXL
Introduction
Clinical management of keratoconus and other ectatic disorders involves a twofold challenge: halting the progression of the disease and visual rehabilitation.1 To achieve these goals, the combination of excimer laser surface ablation with corneal crosslinking (CXL) has been reported to be safe and effective.1–5 While CXL strengthens the biomechanics of the cornea to stop progression, the laser refractive surgery aims to improve vision.
Excimer laser surface ablation can be accomplished by either topography-guided or wavefront-guided photorefractive keratectomy (PRK) in conjunction with simultaneous CXL.6–8 Topography-guided PRK + CXL has been reported to yield promising results in ectatic eyes.1–5 Since topographers measure the anterior corneal surface, a topography-guided treatment may substantially reduce surface irregularity and therefore, refractive error; however, topography-guided treatment does not consider the refractive component, the posterior corneal anatomy, or any internal aberrations, potentially reducing its refractive predictability.9
In keratoconus and other ectatic disorders, increased high order aberrations (HOA) play an important role in deteriorating the quality of vision.10 Correcting low and high order aberrationswould increase retinal image resolution and contrast,11 which would, in turn, be expected to improve the visual performance of keratoconus eyes. In addition, the potential of a wavefront-guided procedure to correct the aberrations measured from the anterior as well as posterior cornea may theoretically yield better visual and refractive outcomes than a topography-guided procedure, which measures and corrects only the topography (anterior cornea). Therefore, when feasible, a wavefront-guided approach may be a better option to manage keratoconus.
The development of high-resolution aberrometry technology has allowed wavefront-guided procedures to be performed on more highly aberrated corneas in patients with keratoconus, post laser-assisted in situ keratomileusis (LASIK) ectasia, or prior history of radial keratotomy.6,7,12 The new iDesign System (Johnson & Johnson Vision, Santa Ana, CA) is a high-resolution Hartmann-Shack aberrometer that can capture up to 1257 data points, depending on the pupil size. It uses Fourier mathematical algorithms to reconstruct the wavefront map.
Our pilot study on the use of high-resolution wavefront-guided (HRWG) surface ablation with CXL in mild cases of keratoconus and post-LASIK ectasia found good safety and efficacy.12 In the present study, we evaluated the visual and refractive outcomes following HRWG surface ablation with CXL in a larger data set of early keratoconus eyes.
Patients and Methods
This prospective, interventional case series included 47 keratoconus eyes of 28 patients (11 female/17 male) who planned to undergo HRWG PRK with simultaneous accelerated CXL at Bogota Laser Ocular Surgery Center, Bogota, Colombia between July 2014 and December 2015. The mean age of the patients was 30.3 ± 8.2 years (range 18 to 51 years). The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Bogota Laser Ocular Surgery Center. After the nature of the procedure was explained, all patients provided written informed consent.
The inclusion criteria were age 18 years or more, presence of keratoconus with a clear cornea in the visual axis (absence of scar and Vogt striae) and estimated residual stromal bed thickness of at least 350 µm (without epithelium). The diagnosis of keratoconus was based on Pentacam (Oculus Optikgeräte Inc., Wetzlar, Germany) parameters. The Pentacam descriptors analyzed were steep, flat and mean keratometry (K), corneal thickness progression indices, anterior and posterior elevation maps, anterior surface topometric indices, normalized deviation indices and overall deviation of normality (Belin/Ambrosio Enhanced Ectasia Display-Final D index). In addition, pachymetry (central, thinnest and apex) was measured using Pentacam, as it is considered more accurate than ultrasonic measurements.13,14
Exclusion criteria were dry eye syndrome, a history of herpetic eye disease, history of LASIK, pregnancy or lactation during the course of the study, active anterior and posterior segment pathologies, autoimmune disease and delayed epithelial healing. Patients with very thin corneas, corneal scarring or opacification within the pupillary area preventing a reliable acquisition with the aberrometer, or very poor corrected distance visual acuity (CDVA) were not included in the study. Contact lens wearers were instructed to discontinue contact lens use for a minimum of 2 weeks before the preoperative eye examination for soft contact lenses and 4 weeks for rigid contact lenses.
All patients had a complete preoperative ophthalmic examination including manifest and cycloplegic refraction, uncorrected distance visual acuity (UDVA) and CDVA testing, slit-lamp anterior segment examination, corneal topography and anterior segment imaging using the Pentacam-HR system, iDesign aberrometry, applanation tonometry and fundoscopy. The wavefront examination was performed under scotopic conditions in order to obtain measurements with the largest possible pupil diameter.
The Visx Star S4-IR excimer laser platform (Johnson & Johnson Vision, Santa Ana, CA) was used to perform all treatments. The default optical zone diameter was 6 mm (9 mm with transition zone); however, the treatment plan was individualized for each eye to achieve residual bed thickness of at least 350 µm (without epithelium).
All surgical procedures were performed under topical anesthesia. The corneal epithelium was removed with 20% alcohol for 20 to 40 seconds and the laser ablation was then applied, followed by accelerated CXL with the KXL System and Vibex Rapid (Avedro Inc., Waltham, MA, USA). The riboflavin drops were instilled for 6 to 10 minutes followed by UV light irradiation of 3 minutes at 30 mW/cm2. Mitomycin-C (0.02%) was applied for 1 minute at the end of the procedure and rinsed thoroughly with balanced salt solution. A bandage contact lens (BCL) was then placed. Patients were examined at postoperative Day 3 and Week 1 to assess the status of corneal epithelial healing. If complete epithelialization was present, the BCL was removed.
The patients were examined at 1, 3, 6 and 12 months after surgery. UDVA and CDVA testing, manifest refraction, corneal topography and anterior segment imaging using the Pentacam-HR system, ocular aberrometry and biomicroscopic examination were performed at these 4 visits. The postoperative treatment regimen consisted of the combination of dexamethasone and moxifloxacin (Vigadexa, Alcon Laboratories, Inc., Fort Worth, TX), 4 times a day for 10 days followed by fluorometholone with gradual tapering over 2 months. The BCL was removed after complete epithelialization, within a period of 4 to 10 days.
Statistical Analysis
Data analysis was performed using Microsoft Excel (Microsoft, Redmond, WA) and SPSS version 17.0 (SPSS, Inc., Chicago, IL). The standard graphs for reporting outcomes in refractive surgery were plotted. Normality of data samples was evaluated by the Shapiro–Wilk test and Q–Q plots. For normally distributed data, the Student’s t-test for paired data was used for comparisons between the preoperative and postoperative 12 months data, whereas the Wilcoxon rank sum test was applied to assess the significance of such differences when data were not normally distributed. Differences were considered statistically significant when the associated p-value was <0.05.
Results
Preoperative characteristics of 47 eyes of 28 patients are presented in Table 1. Twenty eyes were lost to follow up; accordingly, analysis at 12 months included 27 eyes.
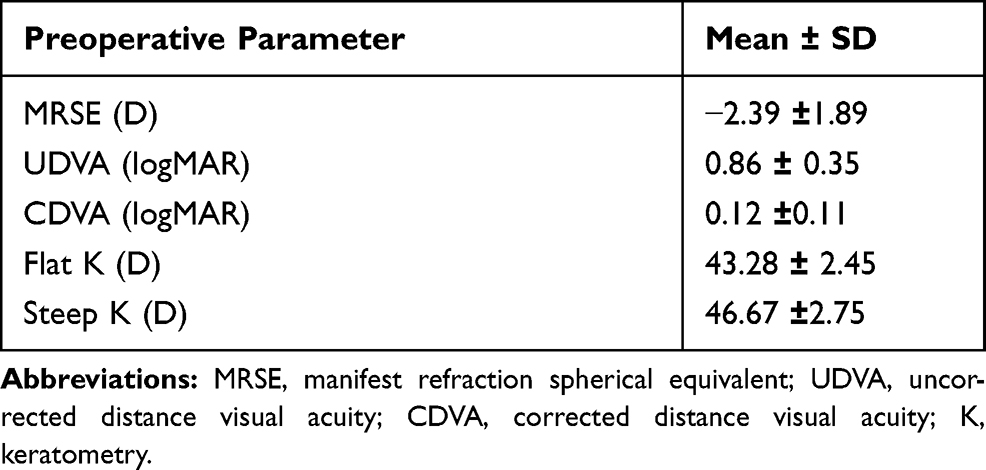 |
Table 1 Mean and Standard Deviation of the Preoperative Parameters of 47 Eyes of 28 Patients |
At postoperative 12 months, a statistically significant improvement was observed in mean MRSE as compared to preoperative levels (−1.99 ± 1.49 vs 0.13 ± 0.68; p<0.01). A linear regression of the attempted versus achieved MRSE had a slope of 1.0905 and intercept of 0.0501 (Figure 1). MRSE within ±1.0 D was achieved in 92.6% of eyes (Figure 2). Figure 3 shows good stability of the spherical equivalent refraction over time. The percentage of eyes with residual refractive cylinder within ±1.0 D was 81.5%. (Figure 4).
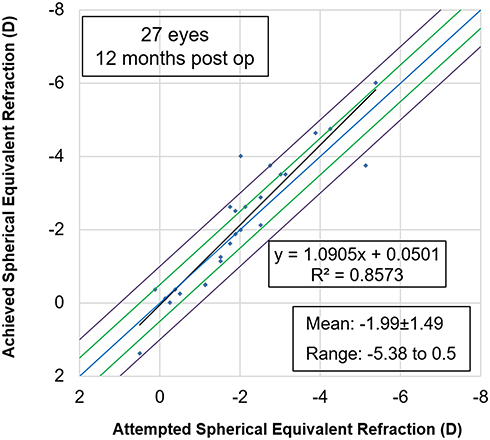 |
Figure 1 Scatterplot showing the relationship between the attempted and achieved spherical equivalent correction at postoperative 12 months. |
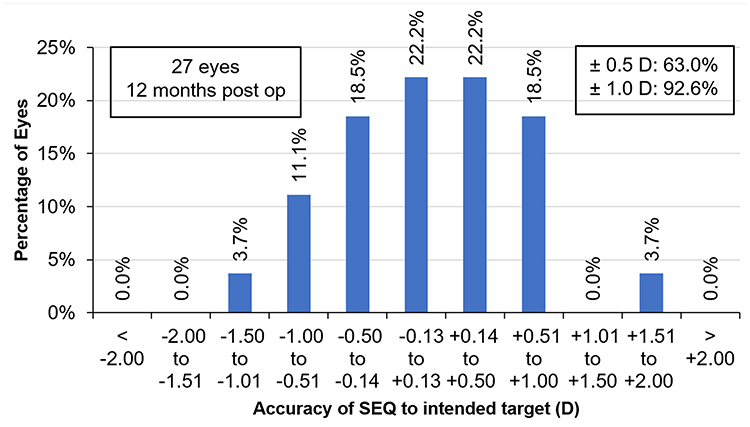 |
Figure 2 Spherical equivalent refraction accuracy after high-resolution wavefront-guided PRK plus accelerated CXL at postoperative 12 months. |
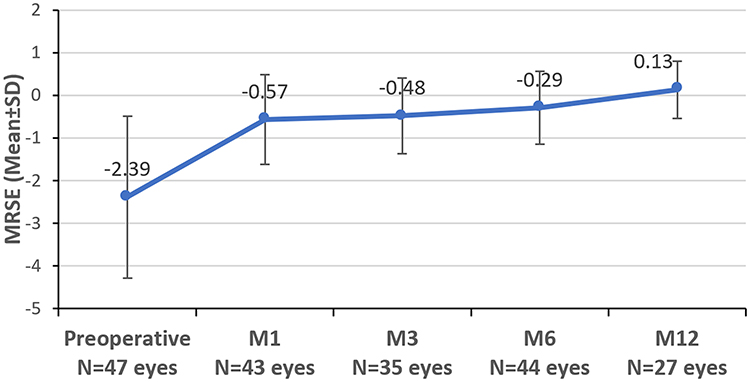 |
Figure 3 Manifest refraction spherical equivalent (MRSE) at different timepoints, demonstrating refractive stability over time. |
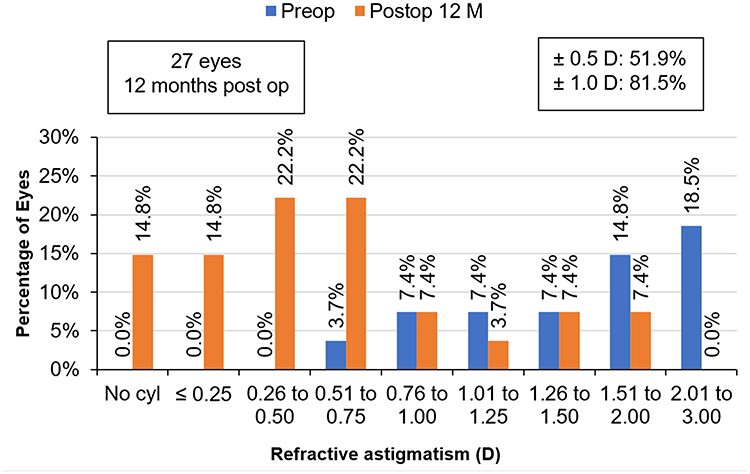 |
Figure 4 Refractive astigmatism accuracy after high-resolution wavefront-guided PRK plus accelerated CXL in comparison with pre-operative refractive astigmatism at postoperative 12 months. |
A statistically significant improvement in both mean UDVA (0.77 ± 0.35 vs 0.08 ± 0.12) and mean CDVA (0.10 ± 0.09 vs 0.02 ± 0.04 logMAR) was observed postoperatively (p<0.01) (Figure 5A and B). The percentage of eyes with UDVA of 20/40 or better was 92.6%. (Figure 6).
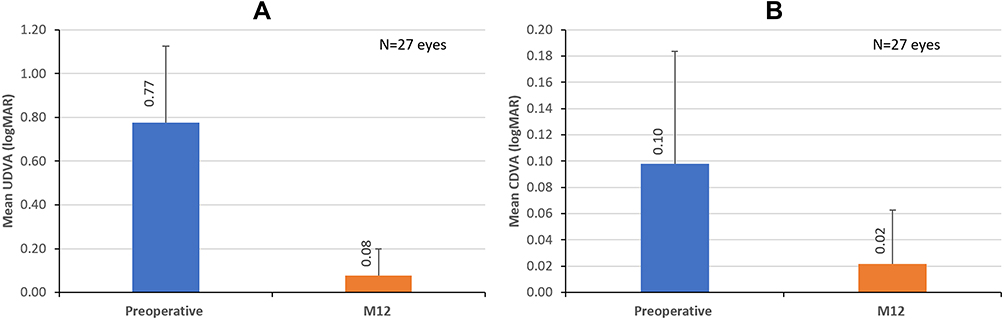 |
Figure 5 Mean uncorrected and corrected distance visual outcomes of high-resolution wavefront-guided PRK plus accelerated CXL at preoperative and postoperative month 12. (A) UDVA, (B) CDVA. |
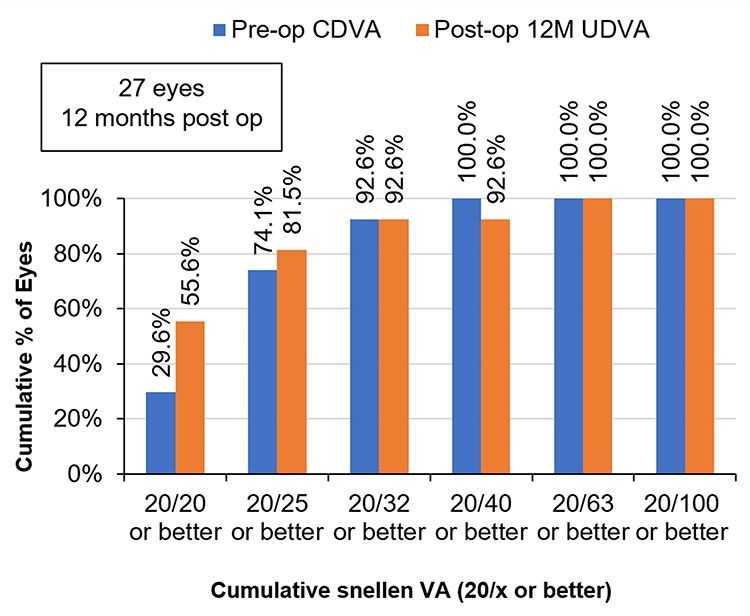 |
Figure 6 Cumulative percent of eyes achieving post-operative UDVA of 20/x or better after high-resolution wavefront-guided PRK plus accelerated CXL as compared to pre-operative CDVA of 20/x or better at postoperative 12 months. |
No change in lines of CDVA was reported in 40.7% eyes (Figure 7). While 40.7% of eyes gained one or more lines of CDVA, 18.5% of eyes had a gain of 2 or more lines of CDVA at 12 months. There was no loss of any lines of CDVA.
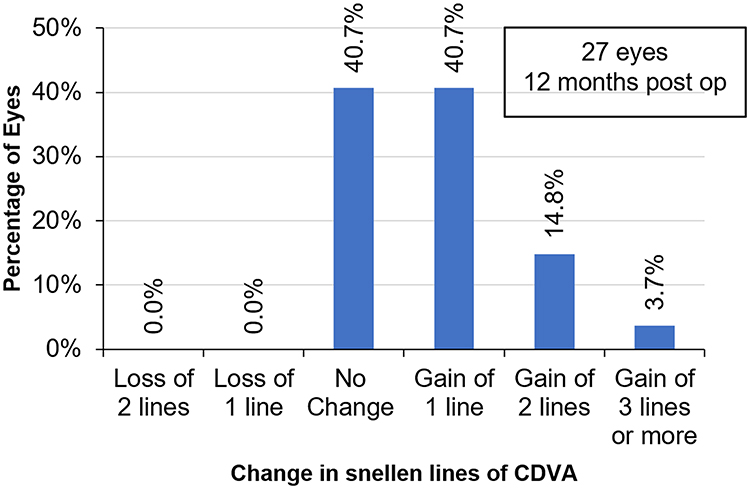 |
Figure 7 Change in Snellen’s line of visual acuity after high-resolution wavefront-guided PRK plus accelerated CXL at postoperative 12 months. |
Preoperative mean flat (42.49 ± 1.67 D) and steep Ks (45.94 ± 2.10 D) were significantly reduced postoperatively to 41.36 ± 2.08 D and 42.65 ± 2.78 D, respectively (p=0.002 for flat K and p<0.01 for steep K) (Figure 8A and B).
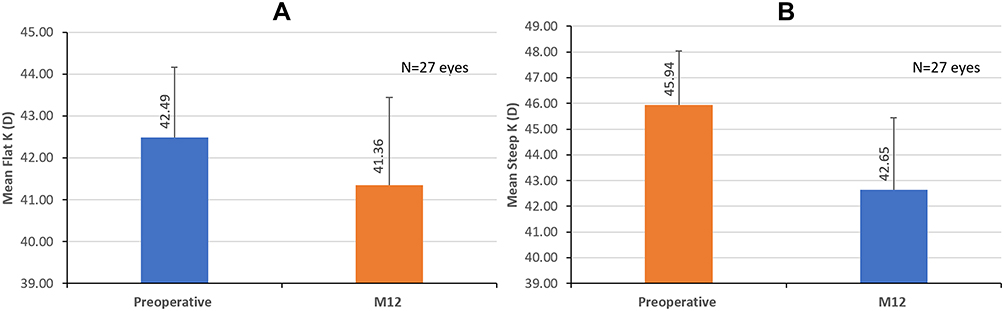 |
Figure 8 Keratometric outcomes of high-resolution wavefront-guided PRK plus accelerated CXL at preoperative and postoperative month 12. (A) Flat K, (B) steep K. |
Preoperatively, mean coma, spherical aberration and total root mean square (RMS) were 0.26 ± 0.26, −0.05 ± 0.13 and 1.21 ± 0.98, respectively. The corresponding HOAs at postoperative 12 months were 0.19 ± 0.18, −0.03 ± 0.15 and 0.91 ± 0.55, respectively.
No clinically significant haze was observed postoperatively in any of the eyes.
Discussion
CXL is a well-established treatment to halt the progression of keratoconus. It aims to improve the intrinsic biomechanical characteristics of corneal stroma in order to stabilize progressive keratoconus.15 Since visual rehabilitation for keratoconus eyes requires improvement in corneal aberrations, photoablation therapies in combination with CXL treatment have been proposed to not only arrest progression of the underlying disease but also to improve functional vision.16 Promising results have been reported with topography-guided or wavefront-guided PRK with CXL in keratoconus eyes.1–3,6,7,17,18
The present study analyzed the outcomes of HRWG PRK combined with CXL in keratoconus eyes and found statistically significant improvements in visual acuity, refraction, and keratometry at postoperative 12 months, which are either consistent with or better than the findings of our previous pilot study. The refractive predictability in the present study (92.6% eyes within ±1.0 D of MRSE) was found to be better than our previous study (87.7% eyes within ±1.0 D of MRSE). Likewise, in the present study, 92.6% eyes had UDVA of 20/32 or better compared with 81.3% in the pilot study, which included eyes with post-refractive surgery ectasia in addition to keratoconus. The keratometric outcomes were comparable between our two studies. As such, the present study validates our previous results of good visual and refractive outcomes after combined HRWG PRK + CXL for the management of keratoconus.
Shaheen et al studied the outcomes of wavefront-guided PRK in aberrated eyes with previous CXL treatment using the same aberrometer as in the present study.6,7 In their pilot study, the authors reported 45.5% eyes within ±1.0 D of attempted correction.6 In their second study,7 this value improved to 76.5%, probably due to adjustments to the ablation profile to change the maximum ablation depth to 15% of the corneal thickness at the thinnest location, which was limited to 50 µm in their pilot study. As such, they could ablate more tissue, which improved refractive predictability in the later study. The refractive predictability found in the present study is even better than that reported in the two studies by Shaheen et al.6,7 In the present study, 92.6% eyes were within ±1.0 D of the attempted correction, which is higher than the corresponding values of 45.5% and 76.5% reported in by Shaheen et al.6,7 This may be due to the fact that the treatment plan in the current study was targeted to achieve residual bed thickness of at least 350 μm. The patients in our study might have had greater corneal thickness than those in the earlier studies. Moreover, the mean preoperative MRSE of the subjects in the Shaheen et al studies (−3.43 ± 1.85 D and −3.22 ± 1.32 D)6,7 were higher than the present study (−2.39 ± 1.89 D).
We performed simultaneous (same day) PRK and CXL, that is, PRK followed by CXL in the same session. The simultaneous (same day) versus sequential (second procedure at a later date) approach for performing PRK + CXL in keratoconus eyes has been debated in the literature. Performing both procedures in the same session has been reported to be beneficial in terms of the minimization of PRK-associated haze and preserving the crosslinked corneal tissue.2,17 In concordance with the results of previous studies of simultaneous topography-guided PRK and CXL in keratoconus eyes, the present study outcomes suggest that simultaneous PRK + CXL is safe and effective.1–5,17,19–21 In previously crosslinked keratoconus eyes that may benefit from wavefront-guided PRK, the sequential procedure (PRK at a later date) as previously documented by Shaheen et al6,7 is a valid option.
We have not compared our study outcomes to the published literature on topography-guided laser treatment. There are significant differences in the magnitude of corneal ectasia (from early to advanced keratoconus) across studies; as such, it may be futile to compare the current study results with the topography-guided ablation literature. In addition, the topography-guided ablations are centered on the corneal vertex, whereas wavefront-guided ablations are centered on the pupil. The authors consider topography-guided treatments only when the severity of the irregularity precludes reliable wavefront measurements.
Several factors, including the depth of CXL into the stroma, sequence/timing of PRK/CXL, the amount of keratocyte loss or activation and excessive production of extracellular material from the activated keratocytes may be responsible for the development of postoperative haze.1 In the present study, we did not observe any cases of clinically significant haze, which corresponds to the finding of no loss of lines of CDVA at 12 months. As previously mentioned, performing both procedures in the same session minimizes the risk of post-PRK corneal haze.18 Crosslinking of the ablated stroma offers the advantage of depopulating keratocytes in the anterior stroma, which could reduce the possibility of haze formation.17 Furthermore, the use of mitomycin-C immediately after crosslinking as well as post-surface ablation prevents the development of haze.22,23 According to John Marshall, when performing combined surface ablation and CXL (personal communication), mitomycin-C should be used only at the end of the combined procedure, after CXL has already been performed. The presence of mitomycin-C when the UV light is applied could increase the risk of scarring (haze formation). The fact that we applied mitomycin-C for one minute at the end of the combined procedure might have contributed to the absence of clinically significant haze.
It is well-known that any ablation of the ectatic cornea reduces the thickness of the already weak structure. This is likely to further weaken the cornea and may lead to progression of the disease. Although the authors have some experience performing PRK in mild keratoconus without damage or progression, we recommend that CXL be performed to increase corneal biomechanical stability whenever tissue is removed from a keratoconus cornea. Although we did not evaluate parameters in this study to measure corneal biomechanics, good refractive stability over 12 months is indicative of good biomechanical stability.
The repeatability of the aberrometer used in the present study has been evaluated previously for lower- as well as higher-order aberrations and has been found to be similar in both normal and keratoconus eyes.10 However, it is important to note that in patients with advanced keratoconus, wavefront measurements may not be repeatable. The subjects in the current study had mild to moderate keratoconus; as such, we did not encounter any problem with the measurement of wavefront repeatability. We also saw a trend towards improved HOA, but differences in pupil size between preoperative and postoperative aberrometry measurements make this parameter difficult to analyze. We believe that in advanced keratoconus eyes, topography-guided PRK with CXL may be an excellent option.
This study was designed as a prospective, interventional, non-comparative case series. Not having a control group is a limitation. However, there are inherent challenges in studying treatments for irregular corneas in a prospective controlled study. The potential study population is limited. Recruiting a control group is difficult and may be unethical if treatment to stabilize the ectatic cornea is withheld. It may be possible in the future to design a study in which two comparison groups both receive crosslinking, but only one undergoes PRK. Alternatively, given the paucity of information in the literature on wavefront-guided versus topography-guided approaches for such patients, a study comparing these two interventions (along with CXL) may be warranted.
In conclusion, simultaneous wavefront-guided PRK followed by accelerated CXL seem to be a promising treatment for patients with keratoconus. Administering this technique with careful observance of safety could offer patients with keratoconus an opportunity to gain functional vision, avoid complications associated with long-term contact lens use and reduce the need for corneal transplantation. Improvement in visual outcomes, no loss of lines of CDVA and the stability of refractive outcomes during the postoperative follow-up indicate that the simultaneous HRWG PRK and CXL may offer an alternative solution for mild to moderate keratoconus.
Acknowledgments
Raman Bedi, MD (IrisARC - Analytics, Research & Consulting, Chandigarh, India) and Jan Beiting (Wordsmith Consulting, Cary, North Carolina) provided research, statistics and editorial assistance in the preparation of this manuscript. Johnson & Johnson Vision, Santa Ana, CA, USA, provided an unrestricted research grant.
Disclosure
GET is a consultant to Johnson & Johnson Vision. He also reports grants from J&J Vision, during the conduct of the study; grants from Avedro-Glaukos and non-financial support from Keramed Corp, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Kymionis GD, Portaliou DM, Kounis GA, Limnopoulou AN, Kontadakis GA, Grentzelos MA. Simultaneous topography-guided photorefractive keratectomy followed by corneal collagen cross-linking for keratoconus. Am J Ophthalmol. 2011;152(5):748–755. doi:10.1016/j.ajo.2011.04.033
2. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. J Refract Surg. 2009;25(9):S812–S818. doi:10.3928/1081597X-20090813-10
3. Kanellopoulos AJ, Binder PS. Management of corneal ectasia after LASIK with combined, same-day, topography-guided partial transepithelial PRK and collagen cross-linking: the Athens protocol. J Refract Surg. 2011;27(5):323–331. doi:10.3928/1081597X-20101105-01
4. Krueger RR, Kanellopoulos AJ. Stability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reports. J Refract Surg. 2010;26(10):S827–832. doi:10.3928/1081597X-20100921-11
5. Tuwairqi WS, Sinjab MM. Safety and efficacy of simultaneous corneal collagen cross-linking with topography-guided PRK in managing low-grade keratoconus: 1-year follow-up. J Refract Surg. 2012;28(5):341–345. doi:10.3928/1081597X-20120316-01
6. Shaheen MS, El-Kateb M, Hafez TA, Piñero DP, Khalifa MA. Wavefront-guided laser treatment using a high-resolution aberrometer to measure irregular corneas: a pilot study. J Refract Surg. 2015;31(6):411–418. doi:10.3928/1081597X-20150521-08
7. Shaheen MS, Shalaby Bardan A, Piñero DP, et al. Wave front–guided photorefractive keratectomy using a high-resolution Aberrometer after corneal collagen cross-linking in Keratoconus. Cornea. 2016;35(7):946–953. doi:10.1097/ICO.0000000000000888
8. Shetty R, D’Souza S, Srivastava S, Ashwini R. Topography-guided custom ablation treatment for treatment of keratoconus. Indian J Ophthalmol. 2013;61(8):445. doi:10.4103/0301-4738.116067
9. Lin DT, Holland S, Tan JC, Moloney G. Clinical results of topography-based customized ablations in highly aberrated eyes and keratoconus/ectasia with cross-linking. J Refract Surg. 2012;28(11):S841–S848. doi:10.3928/1081597X-20121005-06
10. Shetty R, Kochar S, Grover T, et al. Repeatability of a commercially available adaptive optics visual simulator and aberrometer in normal and keratoconic eyes. J Refract Surg. 2017;33(11):769–772. doi:10.3928/1081597X-20170718-02
11. Wygledowska-Promienska D, Zawojska I. Changes in higher order aberrations after wavefront-guided PRK for correction of low to moderate myopia and myopic astigmatism: two-year follow-up. Eur J Ophthalmol. 2007;17(4):507–514. doi:10.1177/112067210701700405
12. Tamayo GE, Castell C, Vargas P, Polania E, Tamayo J. high-resolution wavefront-guided surface ablation with corneal cross-linking in ectatic corneas: a pilot study. Clin Ophthalmol. 2017;11:1777. doi:10.2147/OPTH.S140627
13. De Bernardo M, Rosa N, Hersh R, et al. U.S. multicenter clinical trial of corneal collagen crosslinking for treatment of corneal ectasia after refractive surgery (Ophthalmology. 2017; 124:1475–1484). Ophthalmology. 2018;125(6):e39. doi:10.1016/j.ophtha.2018.01.037
14. De Bernardo M, Vitiello L, Abbinante G, Rosa N. Vector analysis and Pentacam to compare standard cross-linking and photorefractive keratectomy combined with accelerated cross-linking in keratoconus management. Acta Ophthalmol. 2019;97(5):e808. doi:10.1111/aos.14037
15. Iqbal M, Elmassry A, Tawfik A, et al. Evaluation of the effectiveness of cross-linking combined with photorefractive keratectomy for treatment of keratoconus. Cornea. 2018;37(9):1143. doi:10.1097/ICO.0000000000001663
16. Andreanos KD, Hashemi K, Petrelli M, Droutsas K, Georgalas I, Kymionis GD. Keratoconus treatment algorithm. Ophthalmol Ther. 2017;6(2):245–262. doi:10.1007/s40123-017-0099-1
17. Kymionis GD, Kontadakis GA, Kounis GA, et al. Simultaneous topography-guided PRK followed by corneal collagen cross-linking for keratoconus. J Refract Surg. 2009;25(9):S807–S811. doi:10.3928/1081597X-20090813-09
18. Samra A, Ali W, El Emam DS, Farag RK, Abouelkheir HY. Simultaneous versus sequential accelerated corneal collagen cross-linking and wave front guided PRK for treatment of keratoconus: objective and subjective evaluation. J Ophthalmol. 2016;2016.
19. KAnElloPoUloS AJ. Preventing ectasia with cross-linking after PRK or LASIK. Cataract Refract Surg Today. 2012:50–54.
20. Kanellopoulos AJ, Binder PS. Collagen cross-linking (CCL) with sequential topography-guided PRK: a temporizing alternative for keratoconus to penetrating keratoplasty. Cornea. 2007;26(7):891–895. doi:10.1097/ICO.0b013e318074e424
21. Cennamo G, Intravaja A, Boccuzzi D, Marotta G, Cennamo G. Treatment of keratoconus by topography-guided customized photorefractive keratectomy: two-year follow-up study. J Refract Surg. 2008;24(2):145–149. doi:10.3928/1081597X-20080201-04
22. Xu L, Tao X, Li Z, et al. Clinical Study of Mitomycin C in Reducing Haze Formation After Ultraviolet A/Riboflavin Crosslinking for Keratoconus. Eye Contact Lens. 2018;44(Suppl 2):S81–S86. doi:10.1097/ICL.0000000000000422
23. Majmudar PA, Schallhorn SC, Cason JB, et al. Mitomycin-C in corneal surface excimer laser ablation techniques: a report by the American Academy of Ophthalmology. Ophthalmology. 2015;122(6):1085–1095. doi:10.1016/j.ophtha.2015.01.019
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.