Back to Journals » Journal of Healthcare Leadership » Volume 13
Health Professional Frontline Leaders’ Experiences During the COVID-19 Pandemic: A Cross-Sectional Study
Authors Hølge-Hazelton B ![]() , Kjerholt M
, Kjerholt M ![]() , Rosted E
, Rosted E ![]() , Thestrup Hansen S
, Thestrup Hansen S ![]() , Zacho Borre L
, Zacho Borre L ![]() , McCormack B
, McCormack B ![]()
Received 19 October 2020
Accepted for publication 14 December 2020
Published 19 January 2021 Volume 2021:13 Pages 7—18
DOI https://doi.org/10.2147/JHL.S287243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Bibi Hølge-Hazelton,1,2 Mette Kjerholt,3 Elizabeth Rosted,2,4 Stine Thestrup Hansen,5 Line Zacho Borre,1 Brendan McCormack6
1Research Support Unit, Zealand University Hospital, Roskilde 4000, Denmark; 2Department of Regional Health Research, University of Southern Denmark, Odense C 5000, Denmark; 3Department of Hematology, Zealand University Hospital, Roskilde 4000, Denmark; 4Department of Oncology and Palliative Care, Zealand University Hospital, Roskilde 4000, Denmark; 5Department of Plastic Surgery and Breast Surgery, Zealand University Hospital, Roskilde 4000, Denmark; 6Centre for Person-Centred Practice Research, Queen Margaret University Edinburgh, Musselburgh, East Lothian EH21 6UU, UK
Correspondence: Bibi Hølge-Hazelton
Zealand University Hospital, Research Support Unit, Munkesøvej 14, Roskilde 4000, Denmark
Tel +45 27124286
Email [email protected]
Purpose: The aim was to identify the differences in experiences of Danish healthcare leaders in the beginnning of the coronavirus (COVID-19) pandemic and to generate knowledge for future leadership during and post crises.
Background: The global spread of COVID-19 has affected healthcare systems worldwide and has forced healthcare leaders to face challenges few were prepared for. It is expected that the pandemic may hit in several waves within the next year and therefore healthcare leaders must be prepared for these waves.
Methods: An online survey was developed, and comparative analyses were performed.
Results: One hundred and sixty hospital leaders were invited, and 72% completed the questionnaire. Significant differences were found within three selected characteristics: 1) Management level: significantly more heads of departments experienced taking complex decisions (P=0.05), being able to work in a way consistent with their beliefs and values (P=0.05), and they were less likely to experience that collaboration with other leaders was adversely affected by the COVID-19 situation compared to ward managers (P=0.04). On the other hand, ward managers were significantly more often worried about both their own health (P=0.01) and their family’s health (P=0.04). 2) Management education: those with a formal management education more often experienced having the managerial competences to effectively manage the COVID-19 situation (P=0.00), and performing meaningful tasks during the situation (P=0.04). 3) Years of experience: significantly more leaders with more than five years of experience identified having the managerial competences to effectively manage the situation (P=0.01).
Conclusion: Leadership support during a healthcare crisis like the COVID-19 pandemic should strategically focus on ward managers, leaders with no formal management education and leaders with less than two years of experience. Hospital leaders may use this knowledge to re-contextualize what is already known about targeted leadership support during healthcare crises and to act accordingly.
Keywords: assessment, clinical leadership, management, communication
Plain Language Summary
Immediately after the first COVID-19 case was confirmed in Denmark, this study was initiated in order to document and learn from the hospital leaders experiences. 160 clinical and paraclinical healthcare leaders with staff responsibility were invited to participate in a survey and of those, 72% completed the questionnaire. The questionnaire consisted of 27 items that focused on four overall themes – concerns (including values and beliefs), coordination and decision-making, collaboration (internal and external) and communication. The results demonstrate that despite it being known for some time that the pandemic was on its way, it was difficult for the frontline leaders to be fully prepared for the situation and act according to their values and beliefs about leadership. Particularly, leaders with less than two years of experience, with no formal leadership education and ward-managers were challenged. Our findings suggest the need for targeted leadership support of leaders with less education and experience and ward managers to enhance their capacity to manage effectively in times of crisis.
Introduction
Healthcare systems worldwide are currently facing major challenges due to the global spread of coronavirus (COVID-19). It is expected that the pandemic may hit in several waves in the coming year and healthcare systems have to be prepared for these waves.1
On February 27, 2020, the first COVID-19 case was confirmed at a regional acute University hospital in Denmark. This resulted in an immediate organizational response coordinated according to the national and WHO 4-phase pandemics strategy.2 This included an emergency leadership committee that was in full charge of coordination and modification of the infrastructure at the hospital on a daily basis. Two COVID-19 units and a test center were established, resulting in re-organizing and moving units and staff, as well as recruiting and training staff in intensive care. Frontline leaders across the hospital had to face major challenges in order to postpone all non-acute operations, secure patients the best possible care and treatment, and to ensure a safe environment because a focus on employees during a pandemic is crucial.3
Healthcare leaders are familiar with continuous change and developments, but the COVID-19 situation has forced leaders to face challenges many have never experienced before.4–6 There is still a lack of leadership literature regarding healthcare leaders experiences in the present situation, but learning from the SARS pandemic highlights that when no standard procedures exists, effective leadership is key to successful crisis management and vital for staff commitment to their professional responsibilities.7–9 This includes, but is not limited to, effective communication, coordination and decision-making, collaboration, and collective behavior.10,11 Leadership under such circumstances is difficult and may lead to feelings of role overload, conflict or ambiguity if the leader’s values and beliefs are compromised.12 However, leaders may also gain unintended positive experiences and acquire leadership competencies that could not have been gained elsewhere, for instance those regarding virtual leadership.12,13
Purpose
This study aims to identify the differences in experiences of leaders in the beginning of the coronavirus (COVID-19) pandemic and to generate knowledge for future leadership during and post crises.
Methods
Design
The study was a cross-sectional descriptive study using questionnaires.14 It was based on the principles of applied research.15 An on-line survey was developed for this study, as no validated questionnaire appropriate for our purposes was available. An EQUATOR-checklist for cross-sectional studies (STROBE checklist) was applied (Appendix 1).16
Sample and Setting
The setting was the regional acute University hospital in Denmark where the first COVID-19 case was confirmed. The hospital has 18 clinical and six paraclinical departments with a total of 738 beds. The hospital covers departments across four different settings in four different cities.
All clinical and paraclinical leaders with staff responsibility, in total 160, were invited to complete the survey, including physiotherapists, doctors, nurses, biomedical laboratory technicians, medical secretaries, radiographers, midwives and dentists. Leaders were defined as employees from clinical and paraclinical departments having staff responsibility.
Paraclinical departments are those that provide a service for patients without direct involvement in care. Even though these leaders did not have direct responsibility for patient care, they were included in the study because they represented an important part of the totality of the COVID-19 organization, including clinical lab tasks and coordination.
Development of the Survey
Initially, national leading management researchers were contacted for advice regarding a useful and validated tool to examine leaders’ experiences during the COVID-19 situation, but no tool was recommended. Rather, a number of papers were suggested as sources of knowledge.17–20 Reading these papers lead to further searches for literature including the terms disaster management and healthcare crisis leadership.10,21–23 In addition, a Google-scholar alert “COVID-19 leaders experiences, hospital care” was set up on April 28 2020, securing daily notifications presenting new studies, but none was found that focused on COVID-19 leaders’ experiences in hospitals at the time of completing the development of the survey. Thus, an expert committee consisting of two nursing professors, a clinical nurse research leader, a postdoc nurse, and a PhD nurse specialist developed the questionnaire, consisting of twenty-seven questions.
Firstly, the dimensionality of the construct was identified as equal for all answers and an on-line questionnaire was chosen, according to the situation where social distance was recommended.24 Items were developed to be simple, short, and written in a language familiar to the respondents. In the process, the questionnaire was reduced to the final 27 items that were found adequate to represent the construct.24 The items focused on four overall themes – concerns (including values and beliefs), coordination and decision-making, collaboration (internal and external) and communication.10,17–23 Subsequently, an expert panel consisting of two nurse leaders and a medical doctor assessed the content validity and evaluated the clarity of the questions, including identification of any gaps and that the questions addressed the four themes.24
Face validity of the questionnaire was achieved by pilot-testing the survey with a group of four healthcare leaders and subsequently the wording of four questions were adjusted. The survey was developed in Danish and then translated for academic purposes by a native English-speaking senior researcher.
Both the expert panel and the pilot-group were chosen from within the hospital in which the main study took place, as knowledge of the setting was found to have significant importance when evaluating the usefulness and relevance of the developed questions.
Initial validation, test–retest reliability and internal consistency were not performed due to the necessity to capture the here and now experience in a time frame of two weeks.24
Survey Structure
The survey consisted of questions about the participants’ professional background, management level, years of experience as a leader, leadership education and whether the participant had management responsibility for staff.
Subsequently, 27 questions focused on the leaders own experiences in the beginning of the COVID-19-situation. Responses were placed on a five-point Likert-scale (Always, Often, Sometimes, Seldom, Never/Almost never). In addition, the participants had the opportunity to expand on their responses in a column for open-ended answers for every 5th question. Finally, the participants were asked to evaluate whether the management of COVID-19 had helped to develop them as leaders.
Data Collection
Participants were leaders employed at the hospital and recruited through data supplied by the Human Resources Department who identified the population by focusing on job title and responsibility.
The survey was distributed via an online program, SurveyXact, a secure data management application, with a specific hyperlink.25 The survey was distributed on April 24th 2020, six weeks after the first national lockdown, and reminders were sent at weekly follow-ups, with the survey being closed three weeks after it was first distributed. Completing the questionnaire was voluntary.
Data Analysis
Participants’ characteristics are presented as numbers and means. Differences in relation to participants management level, management education and years of experience as leaders (<2y/>5 Y) were assessed using Mann Whitney U-test as all data were non-normal distributed. Data were investigated for normal distribution using the Shapiro–Wilk test.26
When comparing years of experience as a leader representing more than two groups, one-way non-parametric ANOVA (Kruskal–Wallis H-test) including Bonferroni corrections was used, as it is appropriate when analysing ordinal variables, including Likert-scales.26 As these analyses revealed no differences between the three groups, we compared the leaders with the least experience (0–2 years) to those with the most experience (>5 years), using Mann Whitney U-test.
A P-value < 0.05 was considered significant for all analyses. The outcomes from the comparative analyses will be presented as a P-value and a mean rank. Mean rank is the sum of ranks divided by numbers of participants in the group (n). The group with the lowest mean rank is the group with the greatest number of lower scores. Similarly, the group with the highest mean rank have a greater number of high scores.
The survey data were analyzed with descriptive statistics using IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Only fully completed questionnaires were included in the analyses.
Grouping of Data
Several analysis were performed and results were reviewed for relevancy to the purpose of this study. Groupings, which showed significant differences in experiences of the participants were selected and results analysed and discussed. The three relevant groupings were:
- Management level: Head of department or ward manager.
- Formal management education: Yes or no.
- Years of experience as leader: Less than two years vs more than five years.
Results
Sample Characteristics
One hundred and sixty leaders from 18 clinical and six paraclinical departments were invited to complete the questionnaire. Forty-one did not open the survey, one opened, but did not approve content, one did not have staff responsibility, and one did not complete the questionnaire. Eventually 115 (72%) leaders completed the survey and 45 were dropouts (28%). As only one questionnaire was not fully completed this was excluded from analyses.
Table 1 shows demographic data for those who completed the survey and the 45 dropouts. Where data were available, the two groups were compared and no significant differences were found.
 |
Table 1 Demographic Data for Leaders Who Were Invited to Participate in the Survey (n= 160) |
Comparative Analyses
Results are presented in sections of the selected characteristics: management level, management education, and years of experience as a leader. Responses to the 27 questions are divided into the four key themes concern, coordination and decision-making, collaboration and communication. This section both summarizes the results with significant differences, and cases representing substantial difference and thus worth discussing. All results of the comparative analyses can be seen in Table 2.
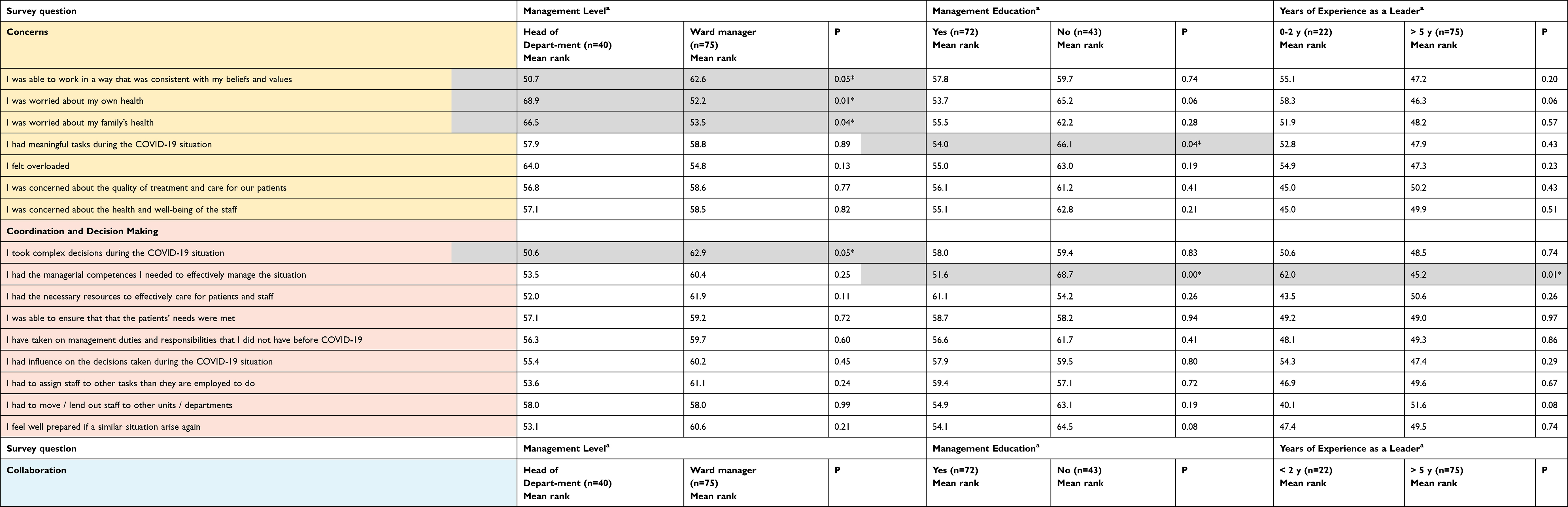 |
Table 2 Results from the Comparative Analyses of the Characteristics Management Level, Management Education and Years of Experience as a Leader. All Results are Divided into the Four Key Themes |
In addition to the above-mentioned analyses, several other group analyses were performed, but the results were not associated with the purpose of this study. The following analyses were excluded from presentation:
- Clinical vs paraclinical positions (paraclinical positions provide a service for patients without direct involvement in care): All significant differences found between these groups were related to whether the group had direct patient contact or not. Eg staff with paraclinical positions experienced rarely or never to be able to answer questions from patients and staff with clinical positions more often experienced to be concerned about quality of treatment and care for the patients.
- Professions (nurses, doctors, physiotherapists, midwives, medical secretaries, radiographers, biomedical laboratory technicians and dentist): Results in analyses comparing these groups tended same results as clinical vs paraclinical positions. Results were affected by whether the profession group had clinical or paraclinical positions, which was related to whether the group had direct patient contact or not.
- Years of duty as a leader: When comparing the three groups, 0–2 y, 3–5 y and > 5y, no significant differences where found between the group 3–5 y and the remaining two groups. Therefore, 0–2 y and > 5y where compared singularly. These are the results presented in Table 2.
Management Level
Within the key theme concerns, heads of departments more often experienced being able to work in a way consistent with their beliefs and values (P=0.05). On the other hand, compared with heads of departments, ward managers were significantly more often worried about both their own health (P=0.01) and their family’s health (P=0.04).
Within the key theme coordination and decision-making, significantly more heads of departments experienced taking complex decisions compared to ward managers (P=0.05).
Concerning the key theme collaboration, leaders who were head of department were less likely to experience that collaboration with other leaders in their own department was adversely affected by the COVID-19 situation (P=0.04).
No significant differences were found in the key theme communication. However, it seems that the heads of departments were more often prepared for the next phase and able to clearly communicate. They felt more prepared for answering staff and patients’ questions.
Management Education
It was found that significantly more leaders with a formal management education experienced performing meaningful tasks during the COVID-19 situation (P=0.04) within the key theme concerns.
In coordination and decision-making, those with a management education more often experienced having the managerial competences they needed to effectively manage the COVID-19 situation (P=0.00).
No significant differences were found for this characteristic in the key themes communication and collaboration.
Years of Experience as a Leader
Significantly more leaders with more than five years of experience indicated having the managerial competences to effectively manage the situation (P=0.01) within the theme coordination and decision-making compared to the group having 0–2 years of experience.
Open-Ended Answers
The participants had the opportunity to expand on their responses in a column for open-ended answers for every fifth question. In all, 294 open-ended responses were given from all professions together. In Table 3, examples of these responses are presented according to the key themes. A forthcoming publication will present an in-depth thematic analysis of these responses.
 |
Table 3 Examples of the Open Answers from the Leaders, Related to the Four Key Themes |
Discussion
In management level, head of department and ward manager, significant differences were found in five questions. Between the leaders with or without management education, significant differences were found in two questions. Concerning years of experience, significant difference were found between the group with less than two years of experience and the group with more than five years of experience, in one question.
The results of the leader survey are discussed focusing on the characteristics of management level, formal leader education and years of experience as leader.
Management Level
Regarding coordination and decision-making, the heads of departments significantly more often replied that they made complex decisions, compared to the ward managers. The data also indicate that they more often experienced having influence on decisions during the COVID-19 situation. Further, more heads of departments reported that they had the resources they needed to effectively care for patients and staff, that they had the competences needed in the situation and that they felt prepared for a similar situation in the future, compared with ward managers. These results raise concerns about the nature of the ward managers’ work in a role that is seen to be squeezed between frontline staff, patients and strategic leaders.27 It is a position that demands confidence and self-efficacy and if this is not in place, it may impact on patient care as well as the wellbeing of staff and the leaders themselves.28,29 The challenging role of ward managers has been extensively studied in nursing and this evidence with a focus on “clinical leadership” highlights the daily dilemmas that ward managers face in balancing operational effectiveness with strategic demands.30 The fact that these two agendas are not always compatible is brought into sharp focus at the time of crisis such as a pandemic, and it raises critical questions to be addressed in future work to clarify the roles of ward managers, identification of an essential supportive infrastructure and the need for appropriate and relevant leadership education.
In the context of collaboration, the ward managers significantly more often replied that collaboration with leaders in their own departments was adversely affected by the COVID-19 situation compared with the head of department leaders, who on the other hand did not feel well informed by their nearest leaders (the hospital management). In a study of Taiwanese nurse leaders during the SARS epidemic, significant support from other leaders was found to be an important factor in ensuring quality of care.7 Therefore, our study indicates that interpersonal actions among ward managers and their nearest leaders, and among the heads of departments and hospital leaders were experienced as less supportive and compassionate.31 This is a worrying finding and it further highlights the need for consistency in leadership behaviors and practices at all levels. In that context, the importance of “shared values” among leaders at all levels of an organization has been previously highlighted.32,33 The existence of such shared values provides a benchmark for leadership practices across an organization and at all levels.
No significant differences were found relating to management level and communication. However, the data indicate that the heads of departments felt better prepared for the next phase, felt more able to communicate clearly and more able to answer staff and patients questions more often than the ward managers. This may indicate that leaders closer to the top management were better informed and prepared for their role, than the ward managers who were closer to the patients and staff in the everyday frontline. As effective health communication has been described as a key factor in fighting the COVID-19 pandemic, securing access by the ward managers to the information they need, must be a priority when preparing for a similar situation in the future.10,34
Formal Leader Education
In the key theme concerns, significantly more leaders with a formal leader education experienced that their tasks during the COVID-19 situation were meaningful, compared with those who did not have such an education. Interestingly, despite their tasks seeming meaningful to them, the leaders who had a leadership education felt more overloaded and were more concerned about the health and wellbeing of patients, staff, own and own family’s health. This is an interesting finding, as it highlights the role that leadership education plays in helping leaders to balance task assignment/achievement with the wellbeing of persons. In particular, this finding opens a space for exploring the place of person-centred leadership in times of crisis.28 At such times, task achievement inevitably becomes the key priority. However, the welfare and well-being of persons who are affected by such crises is of equal concern, but is often relegated to a lower level of priority. Person- centred educated leaders have the expertise to integrate these concerns, recognizing that the well-being of all persons is a key strategy in effective task achievement and leadership effectiveness.28,35
Regarding coordination and decision-making, significantly more leaders with formal management education experienced that they had the necessary management competences to handle the situation compared with the leaders who did not have formal education. Despite evidence of the value of management education, some health professionals are still promoted to leadership positions on the basis of their clinical expertise without having the specific management competence.36,37 The results of our research is an important message to hospital leaders, to prioritize raising the education level of existing leaders, as well as setting a requirement for a higher level of educational preparation in the appointment of future leaders.
No significant differences were found in collaboration when comparing the leaders who had formal management education, with those who did not. However, the results indicate that the leaders with no formal education experienced less support from their leader colleagues in the rest of the organization compared with the leaders who had formal education. The capacity to establish networks has been described as an important competence in management training and education.36 In the COVID-19 situation, lack of support among leaders may lead to missed opportunities to coordinate and collaborate and consequently lead to potential inefficient use of resources, compromised patient safety, and lack of support among leaders.
No significant differences were found in communication when comparing the two groups. However, the results indicate that the leaders who had formal education were more likely to feel able to communicate quickly, clearly and transparently to colleagues and collaborators compared with those who did not have management education. Poor communication in health care has been found to result in inefficient use of resources and compromised patient safety.38 For this reason, our survey results should lead to organizational considerations of being extra attentive and supportive in the reconstruction phase with the leaders who have no formal education. These leaders may be extra vulnerable due to their experiences of not being able to communicate in a manner in which they would have liked to.39,40
Years of Experience as a Leader
Despite a preunderstanding that years of experience as a leader would lead to significant differences in all investigated key themes, the only significant difference was found in the question regarding perception of own managerial competencies in the theme coordination and decision making.41 Here the leaders with less than two years of experience, not surprisingly, replied that they never or almost never experienced they had the necessary competencies to effectively manage the COVID-19 situation, compared with leaders with more than five years of experience. This highlights the need to provide extra support to this group of new leaders when a new health crisis occurs.31 One step could be securing mentors who, directly or via telementoring, are able and willing to provide the emotional support frontline leaders rarely receives, particularly in a situation like COVID-19.42
Figure 1 illustrates the main points in the discussion.
 |
Figure 1 Core findings presented outside-in: Context, Survey Issues, Areas of Attention, and in the middle Core Attention Areas for Supporting Hospital Leadership During a Pandemic. |
Study Limitations
The main limitations are that the data were collected from only one hospital and that the questionnaire could have been further developed and psychometrically tested. Further, the validation methods used experts and pilot participants from the same hospital as where the study took place which could also be a limitation. A strength on the other hand is that 72% responded, representing all invited professions.
Conclusion
This study contributes to the evidence of the impact of the COVID-19 epidemic on hospital leaders, by highlighting the importance of organizations having a thorough understanding of the knowledge, skills and experience of leaders in the organization and their needs for support at times of crisis.
Organizations may use the results from this study to prioritize its leadership-support at times of crises by focusing on its ward managers, leaders with no formal management education and leaders with less than two years of experience as a leader, so these leaders may be able to better handle complex decision-making, collaborate with other leaders, and navigate concerns effectively in times of crisis. From a longer-term perspective, the findings give credence to organizational investment in management training and leadership mentoring to boost junior/novice manager confidence.
The COVID-19 pandemic situation is unique, but the experiences of the leaders in this study affirms and enlarges existing dynamics and resilience. Hospital leaders may use this knowledge to re-contextualize what is already known about targeted leadership support during healthcare crises and act accordingly.
Data Sharing Statement
Anonymized data can be obtained by contacting the authors.
Ethics Approval and Informed Consent
Permission to conduct the study was received from the hospital management and the Danish Data Protection Agency (REG-026-2020) and The National Committee on Health Research Ethics approved the study (J.nr. 20-000013). This study was conducted in accordance with the principles of the Declaration of Helsinki.43 Informed consent was obtained from each participant at the opening page of the online questionnaire.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
There were no sources of funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Situation update worldwide, as of 10 April 2020. European Centre for Disease Prevention and Control; April 11, 2020. Available from: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases.
2. Sundhedsstyrelsen. COVID-19 - risk assessment, strategy and action in epidemics in Denmark [COVID-19 - Risikovurdering, strategi og tiltag ved epidemi i Danmark]. Sundhedsstyrelsen; 2020:22. Available from: https://www.sst.dk/-/media/Udgivelser/2020/Corona/Strategi-for-COVID-19.ashx?la=da&hash=067BF6AF0A95D88B3E0A329ABB3C8935E12DDDFF.
3. Ruderman C, Tracy CS, Bensimon CM, et al. On pandemics and the duty to care: whose duty? Who cares? BMC Med Ethics. 2006;7:E5. doi:10.1186/1472-6939-7-5
4. Kester K, Wei H. Building nurse resilience. Nurs Manag (Harrow). 2018;49(6):42–45. doi:10.1097/01.NUMA.0000533768.28005.36
5. Daly J, Jackson D, Anders R, Davidson PM. Who speaks for nursing? COVID‐19 highlighting gaps in leadership. J Clin Nurs. 2020;29(15–16):2751–2752. doi:10.1111/jocn.15305
6. Dinibutun SR. Factors associated with burnout among physicians: an evaluation during a period of COVID-19 pandemic. J Healthc Leadersh. 2020;12:85–94. doi:10.2147/JHL.S270440
7. Shih F-J, Turale S, Lin Y-S, et al. Surviving a life-threatening crisis: Taiwan’s nurse leaders’ reflections and difficulties fighting the SARS epidemic. J Clin Nurs. 2009;18(24):3391–3400. doi:10.1111/j.1365-2702.2008.02521.x
8. Tseng H-C, Chen T-F, Chou S-M. SARS: key factors in crisis management. J Nurs Res. 2005;13(1):58–65. doi:10.1097/00134372-200503000-00008
9. Wu D, Yang L-C, Wu -S-S. Crisis management of SARS in a hospital. J Safety Res. 2004;35(3):345–349. doi:10.1016/j.jsr.2003.11.010
10. Finset A, Bosworth H, Butow P, et al. Effective health communication – a key factor in fighting the COVID-19 pandemic. Patient Educ Couns. 2020;103(5):873–876. doi:10.1016/j.pec.2020.03.027
11. Lloyd-Smith M. The COVID-19 pandemic: resilient organisational response to a low-chance, high-impact event. BMJ Lead. 2020;1–4. doi:10.1136/leader-2020-000245
12. Rakowsky S, Flashner BM, Doolin J, et al. Five questions for residency leadership in the time of COVID-19: reflections of chief medical residents from an internal medicine program. Acad Med J Assoc Am Med Coll. 2020;95(8):1152–1154. doi:10.1097/ACM.0000000000003419
13. Saltman DC. Is COVID-19 an opportunity to improve virtual leadership? Aust J Gen Pract. 2020;49. doi:10.31128/AJGP-COVID-12.
14. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice.
15. Thorne S. Toward methodological emancipation in applied health research. Qual Health Res. 2011;21(4):443–453. doi:10.1177/1049732310392595
16. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
17. Boin A, McConnell A. Preparing for critical infrastructure breakdowns: the limits of crisis management and the need for resilience. J Contingencies Crisis Manag. 2007;15(1):50–59. doi:10.1111/j.1468-5973.2007.00504.x
18. Evans S. HRM and front line managers: the influence of role stress. Int J Hum Resour Manag. 2017;28(22):3128–3148. doi:10.1080/09585192.2016.1146786
19. Hartge T, Callahan T, King C. Leaders’ behaviors during radical change processes: subordinates’ perceptions of how well leader behaviors communicate change. Int J Bus Commun. 2019;56(1):100–121. doi:10.1177/2329488415605061
20. Hills A. Revisiting institutional resilience as a tool in crisis management. J Contingencies Crisis Manag. 2000;8(2):109–118. doi:10.1111/1468-5973.00130
21. Guan W, Ni Z, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
22. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
23. Tierney K. Disasters: A Sociological Approach. Polity Press; 2019.
24. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–S89. doi:10.4103/sja.SJA_203_17
25. SurveyXact by Ramboll. 2018. Available from: https://www.surveyxact.com/.
26. Verma JP, Abdel-Salam A-SG. Testing Statistical Assumptions in Research. John Wiley & Sons; 2019.
27. Orvik A, Vagen SR, Axelsson SB, Axelsson R. Quality, efficiency and integrity: value squeezes in management of hospital wards. J Nurs Manag. 2015;23(1):65–74. doi:10.1111/jonm.12084
28. Cardiff S, McCormack B, McCance T. Person-centred leadership: A relational approach to leadership derived through action research. J Clin Nurs. 2018;27(15–16):3056–3069. doi:10.1111/jocn.14492
29. Van Dyk J, Siedlecki SL, Fitzpatrick JJ. Frontline nurse managers’ confidence and self-efficacy. J Nurs Manag. 2016;24(4):533–539. doi:10.1111/jonm.12355
30. Pegram AM, Grainger M, Sigsworth J, While AE. Strengthening the role of the ward manager: a review of the literature. J Nurs Manag. 2014;22(6):685–696. doi:10.1111/jonm.12047
31. Vogus TJ, McClelland LE. Actions, style and practices: how leaders ensure compassionate care delivery. BMJ Lead. 2020:
32. Chen Y-R-R, Hung-Baesecke C-JF, Bowen SA, Zerfass A, Stacks DW, Boyd B. The role of leadership in shared value creation from the public’s perspective: A multi-continental study. Public Relat Rev. 2020;46(1):101749. doi:10.1016/j.pubrev.2018.12.006
33. Porter ME, Kramer MR Creating shared value. Harv Bus Rev; 2011 (January–February 2011). Available from: https://hbr.org/2011/01/the-big-idea-creating-shared-value.
34. Torani S, Majd PM, Maroufi SS, Dowlati M, Sheikhi RA. The importance of education on disasters and emergencies: A review article. J Educ Health Promot. 2019;8. doi:10.4103/jehp.jehp_262_18.
35. Lynch BM, McCance T, McCormack B, Brown D. The development of the person-centred situational leadership framework: revealing the being of person-centredness in nursing homes. J Clin Nurs. 2017. doi:10.1111/jocn.13949
36. Sonnino RE. Health care leadership development and training: progress and pitfalls. J Healthc Leadersh. 2016;8:19–29. doi:10.2147/JHL.S68068
37. Pfeffermann G, Kurth A. Value of management education to enhance health systems. Lancet Glob Health. 2014;2(9):
38. Vermeir P, Vandijck D, Degroote S, et al. Communication in healthcare: a narrative review of the literature and practical recommendations. Int J Clin Pract. 2015;69(11):1257–1267. doi:10.1111/ijcp.12686
39. Greenberg N, Tracy D. What healthcare leaders need to do to protect the psychological well-being of frontline staff in the COVID-19 pandemic. BMJ Lead. 2020;
40. Walton M, Murray E, Christian MD. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur Heart J Acute Cardiovasc Care. 2020;9(3):2048872620922795. doi:10.1177/2048872620922795
41. Johansson B, Fogelberg-Dahm M, Wadensten B. Evidence-based practice: the importance of education and leadership. J Nurs Manag. 2010;18(1):70–77. doi:10.1111/j.1365-2834.2009.01060.x
42. Mentoring during a crisis. Harv Bus Rev; 2020. Available from: https://hbr.org/2020/10/mentoring-during-a-crisis.
43. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects; 2020:4. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.