Back to Journals » Clinical Interventions in Aging » Volume 13
Good overall morbidity prediction with the POSSUM scoring system in patients having a total hip or knee replacement – a prospective study in 227 patients
Authors Hildén M, Wretenberg P, Ekström W
Received 15 February 2018
Accepted for publication 12 June 2018
Published 13 September 2018 Volume 2018:13 Pages 1747—1754
DOI https://doi.org/10.2147/CIA.S165698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Mattias Hildén, Per Wretenberg, Wilhelmina Ekström
Karolinska Institutet, Department of Molecular Medicine and Surgery, Karolinska University Hospital Solna, Stockholm, Sweden
Purpose: The Physiological and Operation Severity Score for the enUmeration of Mortality and Morbidity (POSSUM) and P (Portsmouth)-POSSUM predict the risks of complications and mortality 30 days after surgery. The purpose of this study was to evaluate the POSSUM and P-POSSUM scoring systems in patients who underwent surgery for a total hip or knee replacement.
Patients and methods: A total of 227 patients with an elective primary total hip or knee replacement were included. The predicted postoperative morbidity was analyzed in these patients and compared with the observed value 30 days after surgery. Logistic regression analysis was used to assess the correlation of variables and outcome.
Results: The number of patients undergoing total hip or knee replacement was equally distributed with a mean age of 66.4±12.5 years; 57% of patients were females. Postoperative complications occurred in 49 patients, and POSSUM predicted 49 cases with an observed-over-expected ratio of 1.0. The average total POSSUM score was 27.4±4.4 in patients with complications and 26.8±3.5 in patients without complications (P=0.340). Wound infection (n=18), urinary tract infection (n=7), and pulmonary embolus (n=5) were the most common complications. The operation magnitude variable had the highest mean POSSUM score making it the most relevant variable. Age and blood loss and echocardiogram had the largest variance among the assessed variables.
Conclusion: POSSUM accurately predicted morbidities in patients undergoing elective primary total hip or knee replacement. The risk for wound infection, urinary retention, and pulmonary embolus should be considered during hospitalization. The computerized POSSUM system provides case-mix-adjusted morbidity predictions for groups and, hence, serves as a useful tool for surgical audits and large-scale benchmarking.
Keywords: physical status, operation severity, case-mix, prediction, total joint replacement
Introduction
In recent years, quality variables reflecting surgical outcome and care of the patient have become increasingly important. To counteract complications and early postoperative mortality, an instrument or system that can identify individuals at risk before surgery is needed. It is also important that the system allows comparison on equal terms, that is, accounting for the specific case mix of the clinic.1 This could be achieved by using systems with predictive physiological and operative variables that are not too demanding in terms of data collection.2,3
The Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM) provides a quantification of the risks of surgical intervention adjusted both to physical status and operation severity.4 The American Society of Anesthesiologists Physical Status score (ASA),5 the Cardiac Risk Index (RCRI),6 the Acute Physiology and Chronic Health Evaluation II (APACHE II),7 and the Surgical Apgar Score (SAS)8 are other validated surgical risk scoring systems that are based on either physiological and/or operative variables to different extents. Since the introduction of the POSSUM scoring system in 1991, it has been among the most frequently validated tools in heterogeneous surgical cohorts9–11 and has also been studied within different specialties.12 In 1998, the Portsmouth POSSUM (P-POSSUM) was developed when the POSSUM mortality prediction failed in patients with low mortality risks.13 This was due to POSSUM’s rather unique method of statistical analysis, which gives a minimum mortality risk of 1.08% that is considered too high in its representation of healthy patients in low-risk operations.14 Mohamed et al validated an orthopedic model with a specified operation severity scale suiting general orthopedics15 that later was confirmed suitable for patients with femoral neck fractures.16 The new model also changed the variable definition of wound contamination and the timing of operation. As total hip and knee replacements are performed on increasingly elderly individuals with additional increased comorbidity, there is a need to objectively assess the patient’s risks before elective surgery. This assessment could be a basis for decision making for the surgeon as well as provide the patient more specific information enabling him/her to participate in the proposed treatment. POSSUM has been validated within general surgery and surgical specialties, but its predictive ability in primary elective total hip or knee replacement is not well known. There are very few studies evaluating how a surgeon can assess a risk scenario using any POSSUM version for his or her patient prior an elective primary total joint replacement (TJR). Zhou et al have reported an accurate 30-day morbidity prediction with POSSUM in a cohort of patients undergoing arthroplastic surgery.17 However, the study sample was small and not detailed, and the results were not statistically significant. In another study, the P-POSSUM model with its alternative mortality prediction equation accurately predicted mortality (P>0.05) while POSSUM tended to over-predict mortality in patients undergoing total hip replacement (THR).18 It is not known whether the included patients in this study were elective or mixed with trauma patients, and the study sample was considered small as well.
The purpose of this study was to evaluate the POSSUM and P-POSSUM scoring systems in terms of predicting mortality and morbidity 30 days after surgery in patients undergoing surgery for a total hip or knee replacement.
Patients and methods
This was a prospective observational cohort study of patients who underwent elective primary total hip or knee replacement surgery. All patients admitted for elective primary TJR from January 1 to December 31 in 2013, at the Karolinska University Hospital in Solna, were included in the study.
All POSSUM scoring was calculated prospectively. The model includes 12 physiological parameters and six surgical parameters. The physiological severity parameters are age, cardiac signs, respiratory signs, systolic blood pressure, pulse, Glasgow Coma Scale, blood urea or creatinine, blood sodium, blood potassium, hemoglobin, white cell count, and echocardiogram (ECG). The operative severity parameters are magnitude of the operation, number of operations in the last 30 days, blood loss per operation, surgical wound contamination, presence of malignancy, and timing of operation. Each parameter in the two groups is divided into four grades with an exponentially increasing score: 1, 2, 4, and 8 (Table 1). The minimum score is 8, and the maximum score is 88. If any variable is missing, a score of 1 is applied. Four variables in the physiological scoring (cardiac and respiratory signs, ECG, and surgical wound contamination) were determined by an orthopedic surgeon when assessing the patient’s health condition prior to surgery. The operation severity was assessed after completion of the operation by the orthopedic surgeon. The collection of all other POSSUM variables was automated using an integrated software. The software retrieved ICD-10 codes, surrogate variables, and personal information such as sex and age from the patient’s medical record. Observed outcomes were recorded by the software as complications, death, and cause of death 30 days post-surgery. Miscellaneous complications included non-categorized complications with relevance to the surgery noted.
 | Table 1 Physiological and operative severity assessment in POSSUM scoring system |
Statistical method
Descriptive statistics included several variables. Continuous data were presented as the mean value ± standard deviation (SD) with a 95% confidence interval (CI) and as median values with range. Categorical data were analyzed as frequencies and proportions. Statistical significance was calculated using a t-test in continuous variables and a chi-squared test for binary variables; a P-value<0.05 was considered statistically significant. Descriptive statistics are presented in contingency tables. Logistic regression analysis was used to assess the correlation of variables and outcome. The observed-over-expected (O/E) ratios were analyzed to specify the risk prediction accuracy for the whole sample as a group and for certain risk bands of 10%. The O/E ratio for risk bands displays whether the model’s prediction accuracy is different for low- or high-risk groups. The study was approved by the Regional Ethical Review Board in Stockholm, Dnr. 2010/783-31/1. The regional Ethical Review Board has approved research on follow-up on complications and mortality after surgery without any other intervention as equal to quality monitoring. Patient data has been handled with total confidentiality and, as such, the regional Ethical Review Board has decided that written consent is not required.
Results
A total of 247 patients with elective THRs and total knee replacements (TKR) were initially included in this study. As 20 patients were living outside the county and were not able to be fully monitored for 30 days, they were considered lost to follow-up. Complete follow-up was therefore performed in 227 patients. The proportion of TKR and THR operations was even. The study population is presented in detail in Table 2. Mean age was 66.4 years, and the mean total POSSUM score was 27.0. There was a slight overrepresentation of females (57%).
 | Table 2 Description of patients having surgery with total hip or knee replacement (n=227) |
No patient died within 30 days post-surgery. The POSSUM mortality equation predicted 0 deaths, and the P-POSSUM equation predicted one death in this cohort. As there was no mathematically valid denominator, it was therefore not possible to calculate an O/E ratio.
The predicted number of patients with complications made by the POSSUM morbidity equation was 49, giving an O/E ratio of 1.00. A comparison of the patients with and without complications is presented in Table 3. In total, there were 52 complications in 49 patients. The most common complications were wound infection (n=18), urinary retention (n=6), and pulmonary embolus (n=5) (Table 4). Infectious disease contributed to 47% of the total number of complications. Wound infections were significantly more common after TKR operations (n=14) compared to THR (n=4) (P=0.015).
 | Table 3 Descriptive data of study population (n=227) categorized by patients with complications (n=49) and without complications (n=178) |
 | Table 4 Number of complications (n=52) and type of complications in patients having a TJR (n=49) |
The case with the highest predicted morbidity risk and mortality risks suffered an acute myocardial infarction, the most severe form of the included complications. The group of miscellaneous complications included cases of pericarditis, esophagitis, duodenal ulcer, and ileus. Three patients suffered multiple complications.
The POSSUM scoring results are displayed as the mean for each scoring variable in Figure 1. Within the scoring results, age, blood loss, and ECG variables had the largest SDs from the mean and, hence, the largest variance. The mean blood loss scores differed significantly between the surgical methods (275 mL in THR and 127 mL in TKR [P=0.000]).
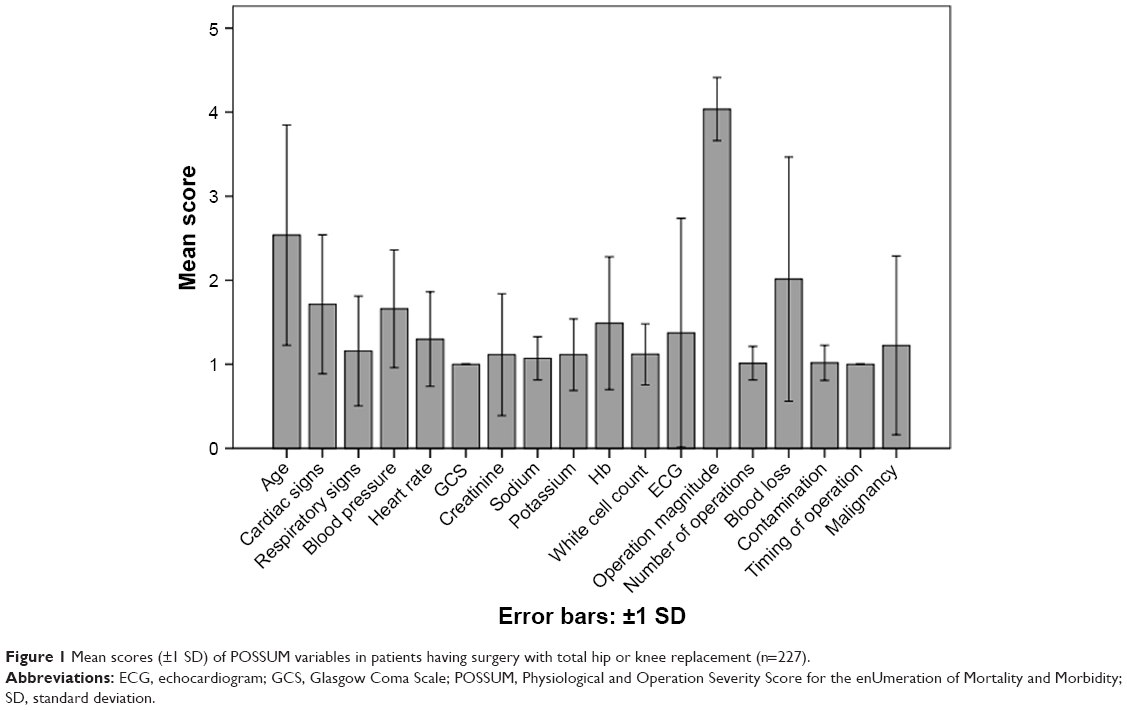 | Figure 1 Mean scores (±1 SD) of POSSUM variables in patients having surgery with total hip or knee replacement (n=227). |
Males had a higher relative risk ratio for a 30-day postoperative complication, OR 1.47 (95% CI: 0.86–2.48) but without significant difference compared to females. No significant difference could be seen between the sexes regarding age, ASA score, and total POSSUM score.
The highest O/E ratio (1.56) was found in patients with a predicted 10%–20% risk for a complication compared to an O/E below 1.0 in patients with a complication risk above 20% (Table 5).
 | Table 5 Morbidity risk bands and comparison of the observed and expected number of complications in patients with primary total hip and knee replacement (n=227) |
Discussion
The aim of this study was to evaluate the POSSUM and P-POSSUM scoring systems in terms of predicting mortality and morbidity 30 days after surgery in patients scheduled for a primary TJR. No deaths occurred among the patients in the study population; thus, the mortality prediction could not be evaluated. POSSUM accurately predicted morbidities in patients undergoing elective primary TJR. The most common complication was wound infection, followed by urinary retention, and pulmonary embolus. The computerized POSSUM system offers case-mix-adjusted morbidity prediction for groups and, hence, is a useful tool for surgical audits and large-scale benchmarking.
Earlier studies on primary TJR identified several preoperative mortality predictors such as emergency admission, advanced age, presence of cardiovascular disease, metastatic cancer, fluid and electrolyte disturbances, coagulopathy, respiratory diseases, dementia, renal disease,19 and male sex.20–22 Jämsen et al reported additional predictors such as ASA>2, preoperative anemia, and use of blood transfusions, but they did not find any association of blood loss and duration of operation with higher mortality.23 Many of these predictors are found within the POSSUM instrument, but a further evaluation of these predictors was not possible since no deaths occurred during the study period.
The frequency of complications was correctly predicted by POSSUM, which indicates that case mix had been taken into account. The present study demonstrates an overall morbidity rate of 21.6%, which is rather high compared to the rates reported in the literature. Provided that POSSUM predictions are accurate in orthopedic surgery,15 this complication rate can be expected in an average-performing clinic with this case mix. Postoperative morbidity statistics in elective TJR are challenging to discuss and depend on definitions of complications, surveillance level, and study types.24,25 A 30-day complication in elective operations could be seen in 4.9% of primary THR cases (22), 5.6% of primary TKR cases,26 and 3.6% of primary TJR cases.27 Mohamed et al found a 30-day complication rate of 4.4% in general elective orthopedic surgery where POSSUM had good prediction accuracy.15 Reports from the Swedish Hip Arthroplasty Register (SHAR) indicate that the proportion of relatively healthy patients is considerably smaller in university hospitals, and our results may thus be due to the case mix rather than poor hospital performance.28 Further, the SHAR for 2012–2014 reported a frequency of 30-day adverse events in Sweden of 1.9% in THR patients aged 55–84 with primary osteoarthritis, ASA class I or II, and a BMI between 18.5 and 29.9.28 The definition of adverse events in the SHAR reports included all forms of reoperation of the hip as well as cardiovascular, cerebrovascular, and thromboembolic complications; pneumonia; ulcers; and death if these complications resulted in hospitalization.
In the specific risk bands, POSSUM predicted a too-low number of complications in low-risk patients. This can be due to a too-low prediction by the surgeon or poor prediction performance by POSSUM, or the clinic could also underperform in this risk band. This question cannot be solved without more extensive validation of the instrument and of other factors that may affect the result on these patients regarding TJR surgery.
In the present study, infectious complications were the most common complication (51%). Mohamed et al reported an even higher infectious complication rate of 71% in elective orthopedic surgery; they likewise used the same complication template as did this study.15
There are known significant predictors of postoperative complications in elective primary THR such as age over 80 years, ASA>2, cardiac diseases, COPD, and diabetes.22 Pulido et al found that patients undergoing surgery for primary TKR had a higher risk for postoperative systemic complications in contrast to the higher risk for local complications found in patients having a THR; this is in line with our results.29 We found that TKR surgery had a statistically significantly higher risk of postoperative wound infections compared to THR surgery without any significant difference between male and female sex. In earlier studies, male sex was associated with a higher risk for postoperative major systemic complications, but female sex was associated with a higher risk for minor local complications22 and cardiac and thromboembolic events.25 However, Pulido et al could not find a significant association of sex and morbidity risk,29 and it is difficult to find a general consensus on this matter. The overall importance in the clinical setting is, of course, to reduce the risk for postoperative complications both in men and women. We could not find any significant difference between the sexes concerning age, ASA, and total POSSUM score that could be relevant for preoperative guidance and information predicting complications. The main postoperative complications in this study were wound infection, urinary retention, and pulmonary embolus. The patient’s lifestyle affects the risk of complications and this may be a topic for discussion before surgery. Smoking and alcohol cessation up to 4–8 weeks before surgery should be recommended to both men and women before surgery to optimize patient outcomes.30,31
In the present study, in line with the literature, physiological variables had a stronger correlation to morbidity outcome than did operative variables.13,15 The operative variable blood loss had the strongest correlation to morbidity, although none of the correlations were statistically significant. The blood loss, ECG, and age variables had the highest variance within the cohort, making them the most significant variables for case mix discrimination (Figure 1).
Today, TJR is one of the most common elective major surgical interventions in the elderly. However, even if mortality risk is low despite the severity of the operation, a substantial number of deaths occur. Elective primary TJR surgery has a reported in-hospital mortality rate of 0.10%–0.15%19,29 and a 30-day mortality rate of 0.18%–0.65%.21,22,26 In this study, the predicted number of deaths of one by P-POSSUM and zero by POSSUM appears reasonable regarding the reported rates of 0.10%–0.65%.19,21,22,26,29
At present, the individual morbidity risk prediction should be used with caution. However, using POSSUM in a broad surgical field such as orthopedic surgery may suit the system better.15 Nevertheless, with the POSSUM system, the patient in a certain risk band can obtain quite exact risks for mortality and specific types of complications (ie, pulmonary embolism and wound infection) that may offer the patient a more explicit awareness of the surgical risks before the procedure.
There are some limitations in the present study. The sample size was too low to assess mortality in the statistical analysis of this low-risk cohort. With more patients, it is possible that this could have been analyzed within the system, and, thus, we could have been able to test the POSSUM system further considering the mortality aspect. The POSSUM and P-POSSUM systems could hence not be compared in this matter. This study included patients undergoing an elective primary TJR, excluding traumatic and emergency cases that are otherwise commonly included in POSSUM studies. Including these cases would also have contributed to a greater variation in the other variables seen in emergency cases. This consequently makes it more difficult to compare our results with those of other studies.
The study sample consisted of patients undergoing only two types of highly standardized operations, resulting in a much reduced, and sometimes nonexistent, scoring parameter variability. The sample size was 227 cases, including an expanded number of patients might have been an advantage.
Conclusion
POSSUM accurately predicted morbidities in patients undergoing elective primary TJR. Measures to counteract wound infection, urinary retention, and pulmonary embolus should be considered during hospitalization. The computerized POSSUM system provides case-mix-adjusted morbidity predictions for groups and, hence, is a useful tool for surgical audits and large-scale benchmarking.
Acknowledgment
The authors would like to thank statistician Gunnar Edman for support in statistical calculations and discussions.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Neary WD, Heather BP, Earnshaw JJ. The Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM). Br J Surg. 2003;90(2):157–165. | ||
Shah N, Hamilton M. Clinical review: can we predict which patients are at risk of complications following surgery? Crit Care. 2013;17(3):226. | ||
Jones HJ, de Cossart L. Risk scoring in surgical patients. Br J Surg. 1999;86(2):149–157. | ||
Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78(3):355–360. | ||
Barnett S, Moonesinghe SR. Clinical risk scores to guide perioperative management. Postgrad Med J. 2011;87(1030):535–541. | ||
Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043–1049. | ||
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. | ||
Gawande AA, Kwaan MR, Regenbogen SE, Lipsitz SA, Zinner MJ. An Apgar score for surgery. J Am Coll Surg. 2007;204(2):201–208. | ||
Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med. 2010;152(1):26–35. | ||
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. | ||
Moonesinghe SR, Mythen MG, Das P, Rowan KM, Grocott MP. Risk stratification tools for predicting morbidity and mortality in adult patients undergoing major surgery: qualitative systematic review. Anesthesiology. 2013;119(4):959–981. | ||
Richards CH, Leitch FE, Horgan PG, McMillan DC. A systematic review of POSSUM and its related models as predictors of post-operative mortality and morbidity in patients undergoing surgery for colorectal cancer. J Gastrointest Surg. 2010;14(10):1511–1520. | ||
Prytherch DR, Whiteley MS, Higgins B, Weaver PC, Prout WG, Powell SJ. POSSUM and Portsmouth POSSUM for predicting mortality. Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity. Br J Surg. 1998;85(9):1217–1220. | ||
Whiteley MS, Prytherch DR, Higgins B, Weaver PC, Prout WG. An evaluation of the POSSUM surgical scoring system. Br J Surg. 1996;83(6):812–815. | ||
Mohamed K, Copeland GP, Boot DA, et al. An assessment of the POSSUM system in orthopaedic surgery. J Bone Joint Surg Br. 2002;84(5):735–739. | ||
van Zeeland ML, Genovesi IP, Mulder JW, Strating PR, Glas AS, Engel AF. POSSUM predicts hospital mortality and long-term survival in patients with hip fractures. J Trauma. 2011;70(4):E67–E72. | ||
Zhou M, Sm Z, Fu J, et al. Effects of POSSUM score system and its modification in evaluating post-operative risk for arthroplasties. J Clin Rehab Tissue Eng Res. 2011;15(39):7396–7398. | ||
Gu GS, Zhang DB, Zhang BH, Sun NK. Evaluation of P-POSSUM scoring system in predicting mortality in patients with hip joint arthroplasty. Chin J Traumatol. 2006;9(1):50–55. | ||
Memtsoudis SG, Pumberger M, Ma Y, et al. Epidemiology and risk factors for perioperative mortality after total hip and knee arthroplasty. J Orthop Res. 2012;30(11):1811–1821. | ||
Memtsoudis SG, González della Valle A, Besculides MC, Esposito M, Koulouvaris P, Salvati EA. Risk factors for perioperative mortality after lower extremity arthroplasty: a population-based of 6,901,324 patient discharges. J Arthroplasty. 2010;25(1):19–26 | ||
Singh JA, Kundukulam J, Riddle DL, Strand V, Tugwell P. Early postoperative mortality following joint arthroplasty: a systematic review. J Rheumatol. 2011;38(7):1507–1513. | ||
Belmont PJ Jr, Goodman GP, Hamilton W, Waterman BR, Bader JO, Schoenfeld AJ. Morbidity and mortality in the thirty-day period following total hip arthroplasty: risk factors and incidence. J Arthroplasty. 2014;29(10):2025–2030. | ||
Jämsen E, Puolakka T, Eskelinen A, et al. Predictors of mortality following primary hip and knee replacement in the aged. Acta Orthop. 2013;84(1):44–53. | ||
Kirksey M, Chiu YL, Ma Y, et al. Trends in in-hospital major morbidity and mortality after total joint arthroplasty: United States 1998–2008. Anesth Analg. 2012;115(2):321–327. | ||
Singh JA, Jensen MR, Harmsen WS, Gabriel SE, Lewallen DG. Cardiac and thromboembolic complications and mortality in patients undergoing total hip and total knee arthroplasty. Ann Rheum Dis. 2011;70(12):2082–2088. | ||
Belmont PJ, Goodman GP, Waterman BR, Bader JO, Schoenfeld AJ. Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. J Bone Joint Surg Am. 2014;96(1):2. | ||
Bozic KJ, Grosso LM, Lin Z, et al. Variation in hospital-level risk-standardized complication rates following elective primary total hip and knee arthroplasty. J Bone Joint Surg Am. 2014;96(8):640–647. | ||
Swedish Hip Arthroplasty Register. 2015. Available from: https://shpr.registercentrum.se/shar-in-english/the-swedish-hip-arthroplasty-register/p/ryouZwaoe. Accessed March 16, 2015. | ||
Pulido L, Parvizi J, Macgibeny M, et al. In hospital complications after total joint arthroplasty. J Arthroplasty. 2008;23(6 Suppl 1):139–145. | ||
Grønkjær M, Eliasen M, Skov-Ettrup LS, et al. Preoperative smoking status and postoperative complications: a systematic review and meta-analysis. Ann Surg. 2014;259(1):52–71. | ||
Eliasen M, Grønkjær M, Skov-Ettrup LS, et al. Preoperative alcohol consumption and postoperative complications: a systematic review and meta-analysis. Ann Surg. 2013;258(6):930–942. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.