Back to Journals » Clinical Ophthalmology » Volume 9
Glaucoma-service provision in Scotland: introduction and need for Scottish Intercollegiate Guidelines Network guidelines
Authors Syrogiannis A, Rotchford A, Agarwal PK, Kumarasamy M, Montgomery D, Burr J, Sanders R
Received 5 July 2015
Accepted for publication 30 July 2015
Published 29 September 2015 Volume 2015:9 Pages 1835—1843
DOI https://doi.org/10.2147/OPTH.S91818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andreas Syrogiannis,1 Alan P Rotchford,2 Pankaj Kumar Agarwal,1 Manjula Kumarasamy,1 Donald Montgomery,1 Jennifer Burr,1 Roshini Sanders1,2
On behalf of the SIGN working group
1SIGN Working Group, SIGN Guidelines for Glaucoma Referral and Safe Discharge, 2Healthcare Improvement Scotland, Edinburgh, Scotland
Purpose: To describe the pattern of glaucoma-service delivery in Scotland and identify areas for improvement, taking into account Scottish General Ophthalmic Services (GOS) arrangements and the Eye Care Integration project, and to design Scottish Intercollegiate Guidelines Network (SIGN) guidelines to refine the primary and secondary interface of glaucoma care.
Materials and methods: A glaucoma-survey questionnaire was sent to all consultant glaucomatologists in Scotland. The design of SIGN guidelines was based on the results of the questionnaire using SIGN methodology.
Results: Over 90% of Scottish glaucoma care is triaged and delivered within hospital services. Despite GOS referral, information is variable. There are no consistent discharge practices to the community. These results led to defined research questions that were answered, thus formulating the content of the SIGN guidelines. The guideline covers the assessment of patients in primary care, referral criteria to hospital, discharge criteria from hospital to community, and monitoring of patients at risk of glaucoma.
Conclusion: With increasing age and limitations to hospital resources, refining glaucoma pathways between primary and secondary care has become a necessity. Scotland has unique eye care arrangements with both the GOS and Eye Care Integration project. It is hoped that implementation of SIGN guidelines will identify glaucoma at the earliest opportunity and reduce the rate of false-positive referrals to hospital.
Keywords: glaucoma, referral, community care, SIGN guidelines
Introduction
Glaucoma is a leading cause of preventable global blindness,1 and disease prevalence in the UK is 2.0% in those aged over 40 years.2 It is estimated that over two-thirds of this patient population is undiagnosed.3 Case detection in the UK is by community optometrists, with onward referral for further assessment in shared care and hospital eye services (HES). The optometrists in the UK and especially in Scotland, in addition to prescribing glasses, may act as primary care ophthalmic practitioners, giving them opportunities to diagnose and monitor disease, and also treat ophthalmic diseases if they possess a postgraduate qualification in independent prescribing. Once a diagnosis of ocular hypertension (OHT) or glaucoma is made, patients are referred to the HES that are operating inside most of the 14 regional National Health Service (NHS) boards throughout Scotland. Following referral, they are seen into a general ophthalmology clinic, where a diagnosis is made and a management plan is established. In cases of advanced glaucoma, challenging management, or if they require an operation, patients are referred internally to the consultant glaucomatologist with a special interest in glaucoma for an expert opinion. This process is fraught with challenges, ranging from disparate detection strategies and lack of well-defined criteria for referral to HES to delayed time for hospital appointments.4
A unique feature in Scotland, felt at the time to potentially aid glaucoma detection, was the introduction of the General Ophthalmic Services (GOS)5 contract in 2006, which had two major objectives: first to facilitate easy access to an eye test in order to improve early diagnosis and initiate prompt treatment for newly diagnosed diseases, and second to reduce the burden of false-positive referrals to the HES.5
Within the GOS, every adult between the age of 16 and 59 years is entitled to a free eye test biennially, with the exception of those above the age of 40 years with a first-degree relative diagnosed with glaucoma, who can attend annually. Those diagnosed with OHT or glaucoma are also entitled to yearly tests independently of their age-group. In addition to performing refraction, the test includes intraocular pressure (IOP) measurement, visual field tests, and dilated fundoscopy to assess the optic nerve head, and also allows for repeat testing.5
Another unique element to the Scottish eye care services is the Eye Care Integration project,6 launched in 2013, which aims to electronically connect all community optometrists to HES to allow electronic referrals with attached digital ophthalmic images. The key feature is that referral is based on five disease-specific forms (glaucoma, macula, cataract, pediatric, and general) with electronic feedback to optometry. The electronic referral system hopes to reduce time from referral to treatment, allocate each patient to the correct clinic at the first hospital visit, reduce unscheduled attendances, and finally identify patients suitable for community care. This system therefore stands potentially to impact glaucoma services significantly, particularly as this process is sensitively dependent on accurate referral information, including detail of the optic disk appearance, which is best captured through images.6
Following the introduction of the GOS contract, the number of patients receiving free eye tests in Scotland between 2006 and 2007 was 613,000, and this increased every year by 10%–12% to over 1.8 million in 2011, with a consequent direct increase in the number of referrals, also by 10%–15% every year, despite a stable Scottish population.7,8 In addition, although not directly quantifiable in Scotland, the publication of the National Institute for Health and Care Excellence (NICE) glaucoma guideline CG85 in 20092 was felt to increase further the number of referrals to HES, especially in the ocular hypertensive group of patients. The representative optometrist bodies advised that regardless of any suggested solutions made by their local primary care organization or local ophthalmologists, for legal defense purposes, all patients with IOP over 21 mmHg should be referred to HES.
Therefore, in Scotland, despite the GOS and Eye Care Integration project, the interface between primary and secondary glaucoma care was left with inconclusive guidance on which patients to refer from community to HES, in the face of increasing eye tests and hospital referrals. It was felt that specific guidelines for Scotland were required in order to maximize the potential of the existing service infrastructure. Additionally, there was possible scope to have low-risk glaucoma suspects and ocular hypertensives monitored in the community within agreed guidance without the risk of visual loss.
The aim of this paper is to describe the current pattern of glaucoma-service delivery in Scotland and highlight areas for potential improvement and refinement, thus leading to the need and process of Scottish Intercollegiate Guidelines Network (SIGN) guidelines. The former was achieved through a questionnaire survey and the latter through the SIGN process, established for over 20 years in Scotland.9
Materials and methods
Survey of consultant glaucomatologists
In 2013, we sought responses from all Scottish consultant glaucomatologists, identified through the Scottish Glaucoma group, to a questionnaire developed to ascertain current needs and glaucoma-service provision in Scotland. The consultants were asked to supply information on the source of new referrals, triage processes, where and by whom new and follow-up patients are seen, and discharge processes. They were also asked for information on the allocation of appointments and any improvements with referral information that could refine the triage process. Where possible, information on case mix and shared care practice was also ascertained.
Scottish Intercollegiate Guidelines Network
SIGN develops evidence-based clinical practice guidelines for the NHS in Scotland. Guideline development is undertaken by a multidisciplinary team with national representation. The first stage of the SIGN process is to identify the key questions to be addressed in the guideline, which are then developed within small subgroups of the SIGN committee facilitated by the guideline coordinator. Recommendations are explicitly linked to supporting evidence from a critical evaluation of systematic reviews relevant to the key questions. An initial guideline is presented at an open forum and then sent for global peer review. The final guideline incorporates all feedback and makes evidence-based scientific recommendations and good clinical practice points that have specific relevance to the region and existing health service infrastructure. The current guideline was influenced by the responses received from the glaucoma questionnaire and the SIGN peer-review process. Account was also taken of consultation with the College of Optometrists, Royal College of Ophthalmologists, NICE guidelines on management of patients with suspected glaucoma and OHT, and other key stakeholders.9
Results
Glaucoma survey
Of the 16 consultant glaucomatologists, 13 responded across the 14 Scottish health boards. Although three did not fill in the questionnaire, they cited colleagues who worked in the same health board, so we had a response from all Scottish health boards. Apart from Fife, all other health boards gave estimates for the questionnaire survey.
In 2013, there were approximately 15,000 referrals to the HES glaucoma services from community optometry. This result concurs with the Information Services Division, which has a similar figure of between 14,500 and 16,000.7
Nearly, all referrals (90%) are triaged by consultants, and the remainder by specialist nurses or hospital optometrists. When information on missing referral information was asked for, the estimated absence of referral information varied from 10% to 40%, with visual field most commonly cited as being absent, followed by optic disc assessment and finally IOP. The Fife Health Board was able to return accurate information by interrogating a glaucoma electronic patient record.10 In one Fife hospital, analysis of 787 consecutive referrals between 2006 and 201211 showed that 597 (75.9%) patients had IOP measurement, 614 (78%) optic disc assessment, and 640 (81.3%) visual field testing.
The majority of all new referrals (>95%) were allocated an appointment. Once patients were allocated an HES appointment, approximately 90% of new patients and 80% of follow-up patients were seen in a consultant-led service in hospital. The remainder were seen in hospital in an optometrist-, specialist nurse-, or orthoptist-led service, with the exception of one health board that had service arrangements with community optometry.
Across the health boards, 70%–80% of referrals were felt to be appropriate, with about one in five patients being categorized as normal. The Fife Health Board was able to give exact figures of 197 (25%) normal and 590 (75%) glaucoma suspects, and glaucoma or ocular hypertensive patients over a 6-year period in one hospital between 2006 and 2012 by extracting data from a glaucoma electronic patient record.11
It was the practice to discharge to a named optometrist in about a third of cases, and to any optometrist with a generic letter in two-thirds of discharges. One health board had service-level arrangements with a shared care community optometry service for formalized discharge processes and continued monitoring.
Two health boards returned detail on shared care services. Grampian has a glaucoma shared care service unique to Scotland, whereby a group of community optometrists received training and accreditation to improve diagnostic accuracy, reduce unnecessary referrals to HES, and initiate glaucoma medication promptly, avoiding delays associated with referral to HES. This initiative also has arrangements in place for discharge of patients from HES to community.12 The South Glasgow Shared Care Service runs within the HES. It is delivered by a team of trained glaucoma practitioners (orthoptists, optometrists, and specialist nurses) and undertakes monitoring of stable glaucoma patients. The service is overseen but not directly run by consultants, and functions using strict diagnostic criteria and protocols.13
In summary, the questionnaire showed the need to refine referral information and reduce the false-positive referral rate to HES. Additionally, there were no consistent arrangements for discharge from primary to secondary care or shared care services in primary care, except for the Grampian model.12
SIGN guidelines
The broad remit of this process was to provide a clinical guideline for primary care assessment and referral of glaucoma suspects of any subtype from community to HES and guidance for safe discharge of patients back to primary care after HES assessment with and without treatment. Full details of the process and the guideline can be found on the SIGN website.9 In brief, the main recommendations and good practice points are described in the following sections.
Primary care examination of glaucoma-suspect and OHT patients
In connection with referral from community to HES, the following examination techniques are recommended before referral.
- Measurement of IOP. A minimum of two IOP readings on a single occasion are measured using the same tonometer. To promote consistency across primary and secondary care services, Goldmann or Perkins tonometry is considered good practice.
- Optic disc assessment. Discs should be examined following dilation of pupils, unless there is a risk of angle closure. Detailed evaluation is recommended, taking into account disc size and narrowest rim:disc ratio in line with Spaeth’s disc damage likelihood scale, cup:disc ratio asymmetry, and all other signs of glaucoma. When referring patients to HES, transmission of optic disc images with the electronic referral letter is recommended.
- Visual field assessment. Standard automated perimetry or frequency-doubling technique with a minimum of two visual fields is recommended, unless the first test is unequivocal. The use of the same technology across primary and secondary care promotes direct comparison and consistency.
- Measurement of central corneal thickness (CCT).
- Van Herick method to assess depth of anterior chamber. Gonioscopy should be performed only if within the clinical experience and competence of the practitioner.
Guidance criteria for referral to HES of glaucoma-suspect and OHT patients
Following the assessment of patients in primary care, guidance on referral criteria are outlined in Figure 1. There was no systematic review evidence that studied the effectiveness of referral criteria. The following are good clinical practice points based on the Health Technology Assessment program on surveillance for OHT,14 NICE glaucoma-treatment guideline CG85,2 joint guidance from the Royal College of Ophthalmologists and College of Optometry,15 and the expertise of the SIGN group.9
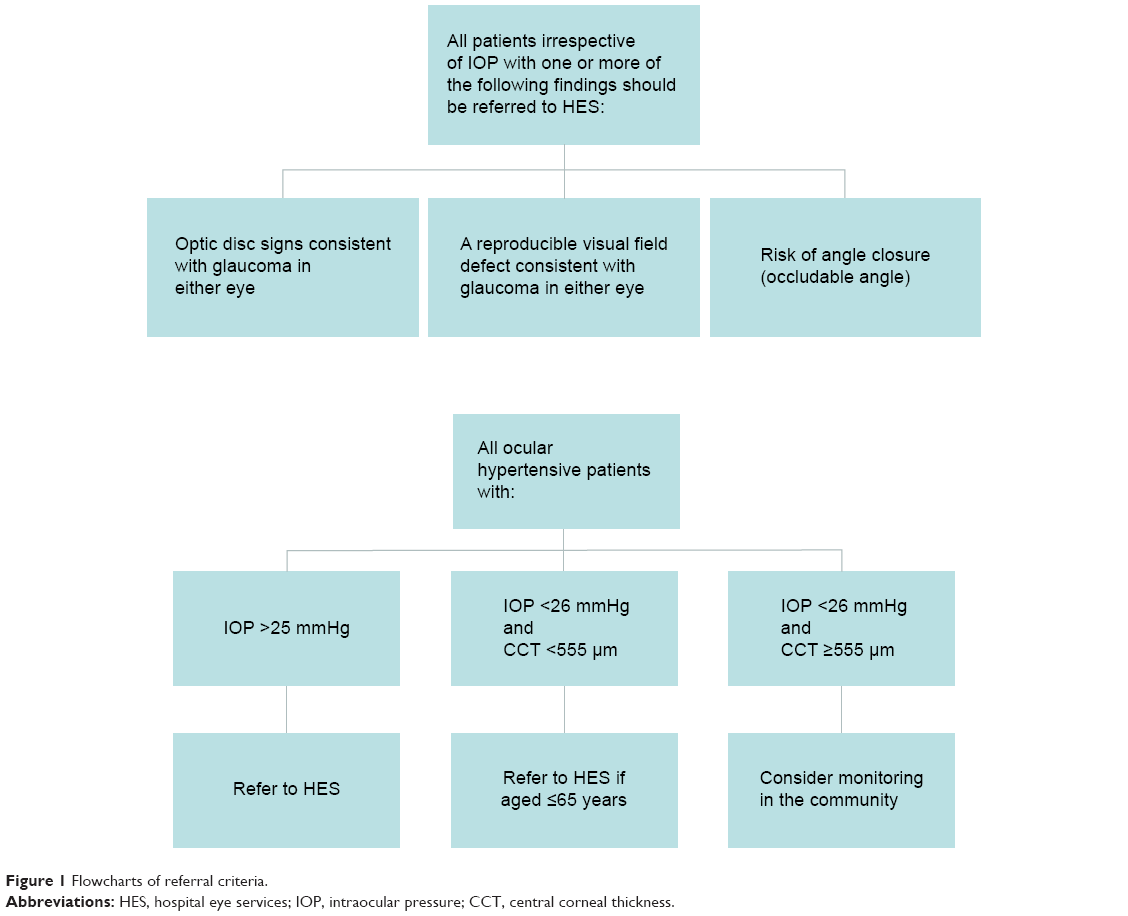 | Figure 1 Flowcharts of referral criteria. |
- Irrespective of IOP, patients with one or more of the following clinical signs should be referred to HES:
- Optic disc signs consistent with glaucoma
- Reproducible visual field defect consistent with glaucoma
- Risk of angle closure (using Van Herick technique if the peripheral anterior chamber width is one quarter or less of corneal thickness, or using gonioscopy if ≥270° of posterior pigmented trabecular meshwork is not visible)
- OHT >25 mmHg may be considered for referral to HES, irrespective of CCT
- OHT with IOP <26 mmHg and CCT <555 μm should be referred to HES if the patient is aged ≤65 years
- OHT <26 mmHg and CCT ≥555 μm may be monitored in the community.
Guidance criteria for possible discharge from HES to primary care
This guidance resulted from evidence based information, and its summary points mirror the guidance for referral into HES, and are outlined in Figure 2.
 | Figure 2 Flowchart of discharge criteria. |
- Untreated OHT of <26 mmHg, CCT ≥555 μm, and otherwise normal examination
- Untreated OHT of >25 mmHg, otherwise normal examination, and low lifetime risk of visual disability
- Treated OHT where rereferral criteria are documented
- Postprophylactic iridotomy for primary angle closure, with open angles, not on glaucoma medication, and with no evidence of glaucoma
- Patients with treated glaucoma should be monitored in HES. Discharge to locally accredited glaucoma optometrists should only be considered at the discretion of the consultant ophthalmologist, when this is in the best interests of the patient and with mutual consent. Robust arrangements should be in place for follow-up and frequency of monitoring, and criteria for rereferral to HES should be individualized.
For all of these discharge criteria, discussion and consent with the patient is required, with detailed discharge letters and rereferral to HES criteria.
An exemplar discharge summary is included in the guideline, outlining all the information required for safe discharge. Close liaison with the patient’s optometrist is required, and qualitative studies suggest that patients value continuity of care with the same professional.16
Monitoring patients at risk of glaucoma in the community
Finally, guidance is given on monitoring patients at risk of glaucoma with methods and frequency of examination in patients with OHT, postprophylactic iridotomy secondary to primary angle closure, pseudoexfoliation, pigment dispersion, and optic disc anomalies to include myopic, tilted, and disc drusen.
Discussion
This is the first survey to provide information on the pattern of glaucoma-service delivery across Scotland. The collective feedback across all health boards highlighted the areas that could be improved, potentially to refine the primary and secondary glaucoma ophthalmic care interface. The survey was only able to collate estimated information, apart from one health board that provided accurate electronic information. Nevertheless, the responses revealed collaborative trends between health boards and Information Services Division data that were helpful in formulating the guideline.
Responses to the survey identified that glaucoma services in Scotland are largely consultant-led and delivered within hospitals. The majority of referral triaging is carried out by consultants, and both new and return patients are largely seen in consultant-led clinics. Apart from Grampian and Glasgow, there are currently no other formally structured shared care schemes for glaucoma. This situation will be difficult to sustain, given the rising age of the Scottish population and consequent increasing incidence of glaucoma disease, in addition to the increasing number of community eye tests and referrals to hospital.
The findings of the survey also revealed that there were major concerns over inadequate referral information. The NHS Fife glaucoma electronic patient record had less than satisfactory referral information in approximately 25% of referrals. This is widely held to be a major contributor to false-positive referrals, but may also risk advanced disease being missed. False-positive referral rates in a glaucoma service are a major resource burden, as once a patient is given an HES appointment, there may follow a considerable resource-intensive clinical path of repeated investigation until disease is ruled out, sometimes prolonged over several years.
We identified that once a referral is made, almost 95% of patients are seen in hospital regardless of referral information. Also, there was no consistent discharge policy across the health board units.
The GOS contract and more recently the Eye Care Integration program both stand to refine the interface between community and HES, but lack guidance on how best to use the service infrastructure. The Scottish GOS arrangements are unique within any public ophthalmic service provision. Not only is a comprehensive ophthalmic examination supported but it also allows for repeat testing. We know that the latter in particular has a significant impact on reducing false-positive referrals. Ang et al compared glaucoma referrals pre- and postintroduction of the GOS contract, and found that there was a significant increase in the number of true-positive referrals.17 However, the study also showed that there were significant deficits in referral information.
The Eye Care Integration project is also unique to Scotland, facilitating referral based on a specific electronic glaucoma referral form (Figure 3) that includes all information required for a comprehensive glaucoma-screening and diagnosis service together with the ability to attach digital images of the disc. The form also includes characterization of the urgency of referral by the optometrist, which is usually defined as urgent where the patients are seen within 2 weeks, soon where they are seen within 4 weeks, and routine. The project is currently designing electronic feedback to community optometry and following on from the recent joint college recommendation on sharing information with optometrists, and plans to share HES clinic letters with optometry electronically.18 Apart from informing the optometrist of referral outcome, it has the enormous potential of educational feedback, which will add to continuous referral refinement.
 | Figure 3 Glaucoma form for direct referral to hospital eye services. |
Despite these two Scottish ophthalmic infrastructures, there is little in the way of shared care services in Scotland. A significant factor, we believe, is the specific lack of guidance on identifying which patients should be referred, which patients should be seen, and which patients may be considered for safe discharge to the community. This is in contrast to England, where according to a paper by Vernon and Adair in 2010,19 at least 50% of ophthalmic departments were running shared care schemes for glaucoma, both within and outside the HES.
The SIGN guidance criteria incorporate recommendations made by NICE guidelines and the joint recommendations of the College of Optometrists and Royal College of Ophthalmologists.2–15 Therefore, they afford clearer, nonconflicting guidance to Scottish glaucoma practitioners. The guideline does not address treatment of glaucoma and OHT, as these are covered in the NICE CG85 guideline.2
While there are several guidelines dealing with glaucoma,2,20,21 none specifically addresses referral into and out of the HES and within the existing Scottish ophthalmic service provisions.
It is hoped that all professionals connected with glaucoma care delivery will find this a helpful guideline. It aims to promote consistent clinical application across Scotland with regard to equipment, testing strategies and frequency, and standardization of skills and referral practices, all to enhance a high standard of collaborative care among professionals dealing with glaucoma. A degree of flexibility, without putting patients at risk of visual loss, is incorporated, thus keeping the patient’s interests central to the guideline, acknowledging that one size does not fit all. The guideline is set out systematically, addressing glaucoma-risk assessment first, followed by criteria for referral into and out of HES and safe clinical processes for discharge to community optometry.
There are direct resource implications both within optometry and ophthalmology. Approximately 90% of Scottish optometrists have the equipment for applanation tonometry, computerized visual fields, and fundus photography, known through the Eye Care Integration project survey.6 However, not all practices have corneal pachymetry equipment, and this was only present in 36% of Scottish practices when last surveyed in 2012.6 The Scottish optometry body through NHS Education Scotland acknowledges that optometrists will require further training in optic disc assessments and interpretation of visual fields, especially in instances of isolated visual field defects in the absence of any other abnormal signs.
Both optometry and ophthalmology will have to liaise more closely and consider such processes as a glaucoma register to ensure patients are appointed and followed up as merited by the clinical condition. This is a new work-flow stream for optometry, where robust auditable patient clinical pathways have to be in place. Hospitals have traditionally had medical record departments that ensure patients are followed up as they should, albeit with acknowledged inefficiencies within the system. Ultimate legal responsibility for “missed” patient appointments are borne by the hospital, whereas in optometry, this will have to be the responsibility of individual practices.
Following the introduction of the SIGN guideline, a process of audit and patient-satisfaction rates would be useful. Evaluation of the proportion of referrals from community optometrists to secondary eye care services with complete information, the number of patients with OHT and IOP <25 mmHg who are referred to secondary eye care services, and the number of patients who are discharged from secondary eye care services to the community and subsequently rereferred would all be useful audit measures.
Conclusion
In summary, once the guideline is embedded within Scottish glaucoma practice, it is hoped that more detailed community assessment of patients will see glaucoma detected at a much earlier stage of disease. It is also hoped that the false-positive rate of referral to HES will be reduced. This should ultimately help with the HES volume of glaucoma care and ensure that all resources are directed toward patients truly requiring hospital attention, with the capacity to be seen, treated, and followed up in a timely fashion within dedicated glaucoma services.
Disclosure
The authors report no conflicts of interest in this work.
References
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. | ||
National Institute for Health and Care Excellence. Diagnosis and Management of Chronic Open Angle Glaucoma and Ocular Hypertension. Manchester: NICE; 2009. Available from: http://www.nice.org.uk/guidance/cg85/resources/guidance-glaucoma-pdf. Accessed July 5, 2015. | ||
Burr JM, Mowatt G, Hernández R, et al. The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation. Health Technol Assess. 2007;11:1–190. | ||
National Patient Safety Agency. Preventing delay to follow-up for patients with glaucoma. 2009. Available from: http://www.nrls.npsa.nhs.uk/resources/?EntryId45=61908. Accessed July 5, 2015. | ||
Scottish Government. The NHS (General Ophthalmic Services) (Scotland) amendment regulations. 2010. Available from: http://www.sehd.scot.nhs.uk/pca/PCA2010(O)01.pdf. Accessed July 5, 2015. | ||
NHS Scotland. Eye care integration: programme resources for NHS Scotland. Available from: http://www.eyecareintegration.scot.nhs.uk. Accessed July 5, 2015. | ||
Information Services Division (ISD) Scotland. Data tables. 2015. Available from: http://www.isdscotland.org/Health-Topics/Eye-Care/Publications/data-tables.asp. Accessed July 5, 2015. | ||
Association of Optometrists. The Economic Impact of Free Eye Examinations in Scotland. London: AOP; 2012. Available from: http://www.aop.org.uk/uploads/Scotland/the_economic_impact_of_free_eye_examinations_in_scotland.pdf. Accessed July 5, 2015. | ||
Scottish Intercollegiate Guidelines Network. Glaucoma Referral and Safe Discharge. Edinburgh: SIGN; 2015. Available from: http://www.sign.ac.uk/pdf/SIGN144.pdf. Accessed July 5, 2015. | ||
Imrie F, Blaikie A, Cobb C, et al. Glaucoma electronic patient record – design, experience and study of high-risk patients. Eye (Lond). 2005;19:956–962. | ||
Foulds J, Dobson S, Sanders R. The analysis of referral data from community to a hospital glaucoma service with a glaucoma patient electronic record. Poster presented at: Congress of the Royal College of Ophthalmologists; May 21–23, 2013; Liverpool, UK. | ||
Azuara-Blanco A, Burr J, Thomas R, Maclennan G, McPherson S. The accuracy of accredited glaucoma optometrists in the diagnosis and treatment recommendation for glaucoma. Br J Ophthalmol. 2007;91: 1639–1643. | ||
Jamison A, McKay L, Rotchford A. The South Glasgow Shared Care Glaucoma Clinic – now entering its teenage years. Poster presented at: Scottish Ophthalmological Club Meeting; September 19, 2014; Edinburgh, UK. | ||
Burr JM, Botello-Pinzon P, Takwoingi Y, et al. Surveillance for ocular hypertension: an evidence synthesis and economic evaluation. Health Technol Assess. 2012;16:1–271. | ||
College of Optometrists, Royal College of Ophthalmologists. Guidance on the referral of glaucoma suspects by community optometrists. 2010. Available from: http://www.college-optometrists.org/en/utilities/document-summary.cfm/B7251E0C-2436-455A-B15F1E43B6594206. Accessed July 5, 2015. | ||
Waibel S, Henao D, Aller MB, Vargas I, Vázquez ML. What do we know about patients’ perceptions of continuity of care? A meta-synthesis of qualitative studies. Int J Qual Health Care. 2012;24:39–48. | ||
Ang GS, Ng WS, Azuara-Blanco A. The influence of the new general ophthalmic services (GOS) contract in optometrist referrals for glaucoma in Scotland. Eye (Lond). 2009;23:351–355. | ||
College of Optometrists. Agreement reached on the sharing of patient information between ophthalmologists and optometrists [press release]. London: College of Optometrists; 2015 [March 4]. Available from: http://www.college-optometrists.org/en/college/news/index.cfm/sharing_patient_information_following_referral. Accessed July 5, 2015. | ||
Vernon SA, Adair A. Shared care in glaucoma: a national study of secondary care lead schemes in England. Eye (Lond). 2010;24:265–269. | ||
European Glaucoma Society. Terminology and Guidelines for Glaucoma. 4th ed. 2014. Available from: http://www.eugs.org/eng/EGS_guidelines4.asp. Accessed July 5, 2015. | ||
White A, Goldberg I. Guidelines for the collaborative care of glaucoma patients and suspects by ophthalmologists and optometrists in Australia. Clin Experiment Ophthalmol. 2014;42:107–117. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.