Back to Journals » Clinical Interventions in Aging » Volume 12
Geroprotectors as a therapeutic strategy for COPD – where are we now?
Authors Miłkowska-Dymanowska J, Białas AJ ![]() , Makowska J, Wardzynska A, Górski P
, Makowska J, Wardzynska A, Górski P ![]() , Piotrowski WJ
, Piotrowski WJ ![]()
Received 23 May 2017
Accepted for publication 3 August 2017
Published 24 October 2017 Volume 2017:12 Pages 1811—1817
DOI https://doi.org/10.2147/CIA.S142483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Joanna Miłkowska-Dymanowska,1,2 Adam J Białas,1,2 Joanna Makowska,2,3 Aleksandra Wardzynska,2,4 Paweł Górski,1,2 Wojciech J Piotrowski1,2
1Department of Pneumology and Allergy, 1st Chair of Internal Medicine, 2Healthy Aging Research Centre, 3Department of Rheumatology, 4Department of Immunology, Rheumatology, and Allergy, Medical University of Lodz, Lodz, Poland
Abstract: Although current therapies in chronic obstructive pulmonary disease (COPD) improve the quality of life, they do not satisfactorily reduce disease progression or mortality. There are still many gaps in knowledge about the cellular, molecular, and genetic mechanisms contributing to pathobiology of this disease. However, increasing evidence suggests that accelerated aging, chronic systemic inflammation, and oxidative stress play major roles in pathogenesis in COPD, thus opening new opportunities in therapy. Therefore, the aim of our review was to describe and discuss some of the most widely used therapeutics that affect the root cause of aging and oxidative stress (metformin, melatonin, sirolimus, statins, vitamin D, and testosterone) in context of COPD therapy.
Keywords: COPD, metformin, melatonin, statins, vitamin D, testosterone
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex, multicomponent disease associated with pulmonary and extrapulmonary manifestations.1 Although current therapies in COPD improve the quality of life, they do not satisfactorily reduce disease progression or mortality. The reason is that there are still many gaps in knowledge about the cellular, molecular, and genetic mechanisms contributing to pathobiology of this disease.2 The evidence for the role of accelerated aging in COPD progression is growing, and senescence is one of the possible molecular pathways for the development of COPD.3
Likewise, the other well-documented theory suggests that chronic systemic inflammation plays the major role in pathogenesis of COPD. Inflammatory local response to inhaled particles and gases might spread out of the respiratory tract (the “spill-over” theory), or alternatively, one common trigger (like tobacco smoking) induces systemic inflammation first, and different organ manifestations result from this common root.3,4 Interestingly, inflammation persists years after cessation of the harmful exposure, for example, cigarette smoke.5,6 On the other hand, it is known that about 15%–20% of all smokers develop COPD, suggesting a role of genetic vulnerability.7–9 Oxidative stress crucially contributes to the pathogenesis of COPD, however, few studies have examined the effects of antioxidants in this condition.10
Pro inflammatory mediators such as C-reactive protein (CRP), fibrinogen, and interleukin 6 (IL-6) are also associated with ageing and comorbid diseases of COPD, such as cardiovascular disease (CVD), obesity, and diabetes and are believed to actively participate in the pathogenesis of these conditions.11–13
There are therapeutic possibilities targeting the root cause of aging and age-related diseases which slow down the aging process. Ito et al called them geroprotectors.2,14 Therefore, the aim of this narrative review was to describe and discuss some of such therapeutics of COPD context. These may include, at least metformin, melatonin, sirolimus, statins, vitamin D, and testosterone.
Materials and methods
The initial search was conducted using PubMed with the subject headings “COPD” and “geroprotectors.” Detailed headings in the area of metformin, statins, vitamin D, melatonin, and sirolimus were used, as provided in Table 1. Only articles written in English, with available abstracts, were retrieved. For relevant titles, the abstracts were reviewed, and if still relevant, the full versions of the articles were obtained. References within the selected articles were also reviewed for their relevance. Table 1 shows the number of hits and final selection for each thematic area. According to preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines, this review should be classified as a narrative systematic review.15
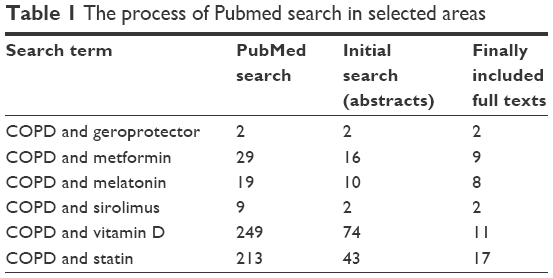 | Table 1 The process of Pubmed search in selected areas |
Metformin
Metformin (N,N-dimethylbiguanide) is an anti-glycemic, biguanide class drug, used in the treatment of diabetes mellitus and polycystic ovarian syndrome.2 However, metformin may offer additional benefits in COPD as well. Nowadays, we reconsidered the traditional contraindications for metformin.16 There is also no apparent reason why patients with CVD and COPD should discontinue metformin therapy.16 There is an evidence suggesting that the use of metformin correlates with a decreased risk of lung cancer, 39%–45%.17 On the other hand, Bodmer et al stated that long-term use of metformin (≥40 prescriptions) was not associated with an altered risk of lung cancer (adjusted OR 1.21, 95% CI 0.97–1.50).18
It was also shown that pretreatment with the use of metformin limits the growth of Staphylococcus aureus in the lungs. Hyperglycemia promotes respiratory S. aureus infection, and metformin modifies glucose flux across the airway epithelium to limit hyperglycemia induced bacterial growth. Garnett et al provided the new evidence that metformin reduces glucose flux into the lungs by reducing transepithelial permeability, independently of its known blood glucose-lowering effects.19 This highlights a new potential therapeutic benefit of metformin in the prevention and treatment of lung infection.
One of the latest retrospective research proves that patients with type 2 diabetes mellitus (T2DM) treated with metformin who had been admitted to hospital for COPD exacerbations were associated with a survival benefit, compared to those treated without it.20
A few studies demonstrated that metformin can minimize the rate of aging and decrease glucose, insulin, and IGF-1 level.21 Metformin may activate AMPK in several cells such as skeletal muscle, heart, endothelial, and hepatocytes. In this way it slows down glucose production in the liver and reduces insulin resistance in the muscle.4 However, as metformin cannot activate AMPK in respiratory system because lung tissue has a very low expression of a receptor responsible for metformin uptake in cells, it is unlikely to affect the lung epithelial cells directly, but possibly affect other types of cells such as alveolar macrophages and immune cells in the respiratory system.2
Sexton et al conducted a prospective open-label observational study. Participants with moderate or severe COPD, obese, and diabetes mellitus or impaired glucose tolerance took metformin twice daily for 6 months.22 Clinical results included St George’s Respiratory Questionnaire (SGRQ), transition dyspnea index, and incremental shuttle walk test. Physiological outcomes include pulmonary function tests, exhaled nitric oxide, respiratory mouth pressures, and handgrip strength. In total, 17 participants completed the study. SGRQ score improved by a median of 5 points, and transition dyspnea index scores improved by 2 points. Inspiratory mouth pressures increased by 7.5 cm H2O. There were trends to improvements in hyperinflation, gas trapping, and shuttle walk distance. Spirometry and exhaled nitric oxide were unchanged. In this proof-of-concept study, metformin may be related to increased inspiratory muscle strength which improves dyspnea and general quality of life in COPD. Those endpoints ought to be tested in a definitive study.23
Melatonin
Melatonin (N-acetyl-5-methoxytryptamine) is a pineal indole hormone. According to some studies, this hormone may extend the life span of mice, rats, fruit flies, and nematods.2,21 Melatonin, besides its function on the circadian rhythms, is also reported to exert a strong antioxidant activity by scavenging OH, O2–, and NO.
A few studies have shown that melatonin may do a lot for sleep quality in COPD. Two researches have shown that compared with placebo, melatonin administration significantly improved sleep quality evaluated by global Pittsburgh Sleep Quality Index (PSQI) score, and individual components of PSQI, such as sleep quality, sleep latency, sleep efficacy, and sleep duration improved significantly. No differences in daytime sleepiness, lung function, and functional exercise level were observed in both studies.23,24
Gumral et al suggest that the episodes of asthma or COPD might be associated with elevated levels of oxidative stress. Authors observed that oxidative stress in the exacerbation period of patients with asthma and COPD increased whereas the antioxidant enzymes and melatonin values reduced.25
Shin et al observed the effects of melatonin on the progress of COPD using cigarette smoke (CS) and lipopolysaccharide (LPS)-induced COPD model.26 The mice were exposed intranasally to LPS. Then, they were treated with CS for 1 hour per day (8 cigarettes per day) from day 1 to day 7. Melatonin (10 or 20 mg/kg) was injected intraperitoneally 1 hr before CS exposure. The drug significantly decreased the neutrophil count in the bronchoalveolar lavage fluid. Also the reduction of the pro inflammatory mediators was observed. Melatonin inhibited Erk phosphorylation and Sp1 expression induced by CS and LPS treatment. Melatonin also slowed down airway inflammation with a reduction in myeloperoxidase expression in lungs. In vitro experiments reported that melatonin suppressed the elevated expression of pro inflammatory mediators induced by cigarette smoke condensate (CSC) treatment. It reduced Erk phosphorylation and Sp1 expression in CSC-stimulated H292 cells. In addition, co-treatment of melatonin and Erk inhibitors significantly decreased the pro inflammatory mediators with greater reductions in Erk phosphorylation, and Sp1 expression than that observed in H292 cells treated with Erk inhibitor alone. Those results together, melatonin effectively inhibited the neutrophil airway inflammation induced by CS and LPS treatment, which was closely related to down regulation of Erk phosphorylation. These endpoints suggest that melatonin may have a therapeutic potential for the treatment of COPD.26
Melatonin has been tested on the effects of melatonin as antioxidant in COPD in randomized, double-blind, placebo-controlled study in clinically stable moderate to very severe COPD. Oxidative stress was evaluated by 8-isoprostane levels in exhaled breath condensate at baseline, and after 1, 2, and 3 months of 3 mg melatonin treatment. In addition, exhaled breath condensate levels of IL-8, dyspnea severity assessed in Medical Research Council scale, spirometry, and 6-minute walk test were compared at baseline and after treatment. Patients taking melatonin showed a decrease in 8-isoprostane with significant differences from baseline after 2 (P=0.03) and 3 months (P=0.01). Melatonin improved dyspnea (P=0.01), despite no significant changes in spirometry or 6-minute walk test.10
Furthermore, next studies revealed that α, β-unsaturated aldehyde acrolein in CS induces the production of IL-8, which is related to bronchitis, rhinitis, pulmonary fibrosis, and asthma.27–29 In addition, pulmonary fibroblasts secrete IL-8, which has a chemotactic effect on leukocytes, and which in turn, play a crucial role in lung inflammation. Melatonin effect antioxidant and anti-inflammatory by the reduced expressions of iNOS, IL-1β and IL-6, and increased glutathione (GSH) and superoxide dismutase activities. Kim et al tested whether melatonin suppresses acrolein-induced IL-8 secretion in human pulmonary fibroblasts (HPFs).27 It revealed that acrolein-induced IL-8 production was accompanied by increased levels of phosphorylation of Akt and extracellular signal-regulated kinases (ERK1/2) in HPFs, and in this way melatonin suppressed IL-8 production in HPFs. These findings suggest that melatonin suppresses acrolein-induced IL-8 production via ERK1/2 and phosphatidylinositol 3-kinase (PI3K)/Akt signal inhibition in HPFs.
The role of melatonin in the long-term management of COPD patients should be examined in further studies.27
Sirolimus
Sirolimus is an immunosuppressive agent used to prevent rejection in organ transplant patients. It is an inhibitor of mammalian target of rapamycin (mTOR). Recent findings has shown that it also extends the life span of yeast, Caenorhabditis elegans, Drosophila melanogaster, and mice.30 Long-term study of mTOR has not been planned in COPD yet.2 It should be considered because it regulates translation initiation, and elongation, ribosome biogenesis, cell-cycle progression, lipid synthesis, mitochondrial biogenesis, and autophagy.30
Vitamin D
Although vitamin D is traditionally related to bone turnover, in recent years there is increasing evidence that low vitamin D levels are associated with numerous autoimmune diseases,31 cancer,32 and infections.33
According to the meta-analysis performed by Zhu, the serum levels of 25-hydroxyvitamin D (25(OH)D), in COPD patients was comparable with controls in cohort studies but was significantly lower in case–control studies.34 The deficiency rate of 25(OH)D was comparable between COPD and controls both in cohort and case-control studies.35,36
Until now, five studies examining curative effect of vitamin D supplementation have been published. In 2012, Lehouck et al published data of randomized, double-blind placebo-controlled study, in which 91 patients on active treatment with 100,000 IU of vitamin D, and 91 on placebo were enrolled.37 Neither the median time to exacerbation nor exacerbation rate, forced expiratory volume in 1 second (FEV1) value, hospitalization rate, quality of life, nor mortality differ between two subgroups after 1 year of follow-up. However, when the post hoc analysis of 30 patients with severe vitamin D deficiency (25(OH)D levels <10 ng/mL at a baseline) was performed, it revealed that the rate of exacerbations per patient/year decreased by 43%, although the time to exacerbation did not differ in this subgroup. Also in 2012, Hornikx et al published a post-hoc analysis of the Lehouck study in which 50 subjects who entered the pulmonary rehabilitation program during the trial were studied.38 The influence of vitamin D supplementation on the outcome of rehabilitation program was studied. Patients receiving vitamin D (100,000 IU/month during 1 year) had larger improvements in inspiratory muscle strength and maximal oxygen uptake, but the quadriceps strength and 6 minutes walking did not differ.
Another short-time study (6 weeks) on relatively small group of patients (18 patients receiving vitamin D, and 18 on placebo) assessed the effect of supplementation with 2,000 IU of vitamin D daily on physical performance, which was assessed by Short Physical Performance Battery score.39 Patients also filled the SGRQ containing domains assessing respiratory symptoms, limitations due to breathlessness, and the impact of lung disease on social and psychological functioning. The study showed no effect of short-term treatment with vitamin D on physical performance. In the multicenter double-blind placebo-controlled study of Martineau, the effect of vitamin D was administered bimonthly for 1 year (120,000 IU each dose) on exacerbation rate and upper respiratory infections.40 There was no difference in the time to first moderate or severe exacerbation or time to first respiratory infection in the group with vitamin D versus placebo but vitamin D supplementation was protective for moderate to severe exacerbation only in the subgroup with baseline 25(OH)D level below 50 nmoL/mL.41
The study of Zendedel et al included 44 patients with COPD treated with 100,000 IU of vitamin D per month for 6 months, and 44 patients were included to placebo group.41 The exacerbation rate decreased significantly, and also the increase in FEV1 values was observed; however, it has to be noticed that baseline 25(OH)D levels were not assessed in the study.
To sum up, the beneficial effect of vitamin D on exacerbation rate is observed only in the group of COPD patients with deficiency of vitamin D. The results of the double-blind placebo-controlled studies suggest also that correction of vitamin D deficiency in patients with COPD reduces the risk of exacerbation, and can influence the outcomes of respiratory rehabilitation program.
Statins
Statins are the inhibitors of 3-hydroxy-3-methylgluteryl coenzyme A (HMG-CoA) reductase, and are the most potent cholesterol lowering agents. Currently the indications for use of statins include hypercholesterolemia, coronary heart disease, and diabetes.42 However, their pleiotropic activity has been stressed: a positive effect on vascular endothelium and oxidative stress as well as anti-proliferative and anti-inflammatory activity.43 There are several works concerning the impact of statins on chronic systemic inflammation in patients with COPD but the underlying mechanism has not been yet precisely defined.44 Data from both retrospective and randomized controlled trials (RCTs) has shown the reduction in CRP level, or in a concentration of a number of pro inflammatory cytokines in COPD patients.45 In a prospective study of Lee et al, 6 months of administration of pravastatin (40 mg/day) was associated with reduction of high sensitive CRP in a cohort of clinically stable COPD individuals.46 In a group of patients with stable COPD, a 4-week treatment with 20 mg daily simvastatin was connected with reduction of IL-17, IL-6, and IL-22, and up regulation of IL-10 in the induced sputum.47 The anti-inflammatory effect was also observed in a lung tissue. In a recent randomized study, Mroz et al demonstrated that 12-week treatment with atorvastatin 40 mg/day was associated with reduction of local lung inflammation in patients with mild to moderate COPD as compared with control group.48
There have been many attempts to prove that the anti-inflammatory effects of HMG-CoA reductase inhibitors demonstrated in COPD patients can be translated into major clinical outcomes.49 Reduced risk of COPD exacerbation in statin users was observed by Wang et al50 and by Ingebrigtsen et al51 however, in this study the positive effect was not seen in the most severe COPD cases without cardiovascular comorbidity. In a population-based cohort in New Zealand, statin treatment was associated with a reduction in all-cause mortality at 3–4 years after first admission for COPD, irrespective of comorbid conditions.52 Another retrospective analysis conducted in patients with COPD from Scotland showed positive effect of statins used in secondary prevention on cardiovascular events, and mortality.53 In a prospective study during 1 year follow-up of 245 patients admitted to hospital due to COPD exacerbations, the use of statins was associated with a lower risk for subsequent exacerbation but had no effect on mortality.54 Prospective observation from Taiwan showed that statins were associated with decreased hospitalization rate due to COPD in patients newly diagnosed with this disease.55 The all-cause mortality in statin users with COPD was also reduced in a follow-up of a population from Rotterdam study, and the result was related to the baseline hsCRP level.56
However, despite the promising results of retrospective and prospective observational studies, RCTs did not confirm the positive effect of statin therapy on the frequency of COPD exacerbations, COPD-related mortality, and other major clinical outcomes.
The simvastatin in the prevention of COPD exacerbations (STATCOPE) study, the largest published randomized controlled trial on the use of statins in COPD, was conducted in a population of 885 patients with a high risk of exacerbation without indication to cholesterol-lowering therapy. In this study, the use of simvastatin 40 mg/day was not associated with the reduction in exacerbation rate (primary outcome) or the in time to an exacerbation.57 Another RCT, radiation dose among different endovascular procedures (RODEO) study, showed no improvement of vascular function or ventilatory parameters in COPD patients treated with 10 mg/day rosuvastatin as compared to placebo group. Similar to STATCOPE, RODEO trial subjects with conventional indication to statin therapy were excluded.58
Despite all the large and constantly growing number of studies, there is not enough evidence for recommending the introduction of statins for the treatment of COPD. It has been suggested that the anti-inflammatory effect is dose-dependent, may be related to the type of HMG-CoA reductase inhibitor, and probably is more pronounced in individuals with cardiovascular comorbidities.45 However, statins still remain a promising therapeutic option for COPD patients, and there should be more research to establish their role in the treatment of COPD. Table 2 summarizes the geroprotectors described above.
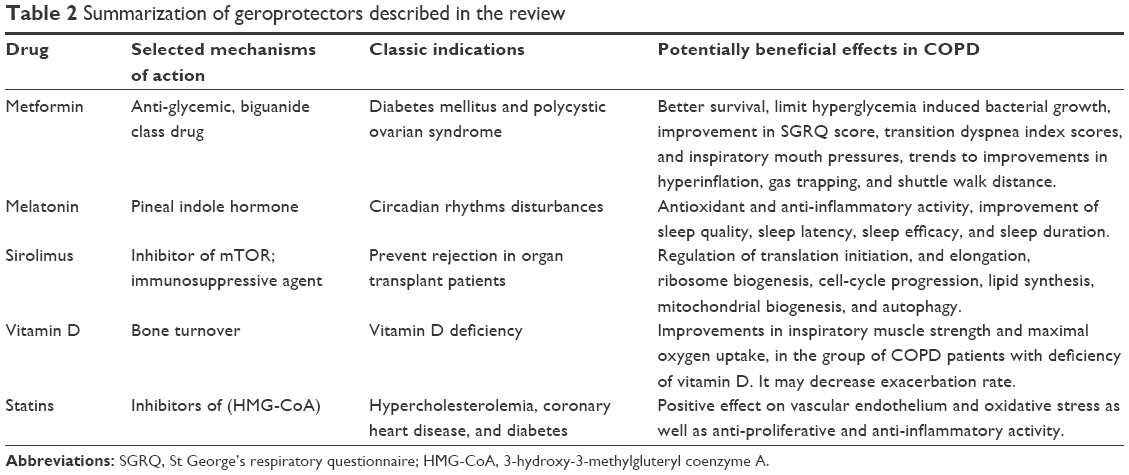 | Table 2 Summarization of geroprotectors described in the review |
Conclusion
Although there are numerous reports suggesting a promising place of geroprotectors in therapy of COPD, number of meta-analyses which provide best quality evidences is limited. However, present state of knowledge lets us to recognize them as a new therapeutic approach which may ameliorate prognoses of patients with COPD.
Disclosure
The authors report no conflicts of interest in this work.
References
Agusti A, Sobradillo P, Celli B. Addressing the complexity of chronic obstructive pulmonary disease: from phenotypes and biomarkers to scale-free networks, systems biology, and P4 medicine. Am J Respir Crit Care Med. 2011;183(9):1129–1137. | ||
Ito K, Mercado N. STOP accelerating lung aging for the treatment of COPD. Exp Gerontol. 2014;59:21–27. | ||
Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. | ||
Ito K, Barnes PJ. COPD as a disease of accelerated lung aging. Chest. 2009;135(1):173–180. | ||
Willemse BWM, ten Hacken NHT, Rutgers B, Lesman-Leegte IGAT, Postma DS, Timens W. Effect of 1-year smoking cessation on airway inflammation in COPD and asymptomatic smokers. Eur Respir J. 2005;26(5):835–845. | ||
Miller M, Cho JY, Pham A, Friedman PJ, Ramsdell J, Broide DH. Persistent airway inflammation and emphysema progression on CT scan in ex-smokers observed for 4 years. Chest. 2011;139(6):1380–1387. | ||
Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J. 1977;1(6077):1645–1648. | ||
Liu SF, Kuo HC, Tseng CW, et al. Leukocyte mitochondrial DNA copy number is associated with chronic obstructive pulmonary disease. PLoS One. 2015;10(9):e0138716. | ||
Cunningham TJ, Ford ES, Rolle IV, Wheaton AG, Croft JB. Associations of self-reported cigarette smoking with chronic obstructive pulmonary disease and co-morbid chronic conditions in the United States. COPD. 2015;12(3):276–286. | ||
de Matos Cavalcante AG, de Bruin PFC, de Bruin VMS, et al. Melatonin reduces lung oxidative stress in patients with chronic obstructive pulmonary disease: a randomized, double-blind, placebo-controlled study. J Pineal Res. 2012;53(3):238–244. | ||
Vanfleteren LEGW, Spruit MA, Groenen M, et al. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(7):728–735. | ||
Fu JJ, McDonald VM, Gibson PG, Simpson JL. Systemic inflammation in older adults with asthma-COPD overlap syndrome. Allergy Asthma Immunol Res. 2014;6(4):316–324. | ||
Garcia-Aymerich J, Gómez FP, Benet M, et al. Identification and prospective validation of clinically relevant chronic obstructive pulmonary disease (COPD) subtypes. Thorax. 2011;66(5):430–437. | ||
Ito K, Colley T, Mercado N. Geroprotectors as a novel therapeutic strategy for COPD, an accelerating aging disease. Int J Chron Obstruct Pulmon Dis. 2012;7:641–652. | ||
Panic N, Leoncini E, de Belvis G, Ricciardi W, Boccia S. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS One. 2013;8:e83138. | ||
Rachmani R, Slavachevski I, Levi Z, Zadok B, Kedar Y, Ravid M. Metformin in patients with type 2 diabetes mellitus: reconsideration of traditional contraindications. Eur J Intern Med. 2002;13(7):428. | ||
Lai SW, Liao KF, Chen PC, Tsai PY, Hsieh DPH, Chen CC. Antidiabetes drugs correlate with decreased risk of lung cancer: a population-based observation in Taiwan. Clin Lung Cancer. 2012;13(2):143–148. | ||
Bodmer M, Becker C, Jick SS, Meier CR. Metformin does not alter the risk of lung cancer: a case-control analysis. Lung Cancer Amst Neth. 2012;78(2):133–137. | ||
Garnett JP, Baker EH, Naik S, et al. Metformin reduces airway glucose permeability and hyperglycaemia-induced Staphylococcus aureus load independently of effects on blood glucose. Thorax. 2013;68(9):835–845. | ||
Hitchings AW, Archer JRH, Srivastava SA, Baker EH. Safety of metformin in patients with chronic obstructive pulmonary disease and type 2 diabetes mellitus. COPD. 2015;12(2):126–131. | ||
Anisimov VN. Metformin. Cell Cycle. 2013;12(22):3483–3489. | ||
Sexton P, Metcalf P, Kolbe J. Respiratory effects of insulin sensitisation with metformin: a prospective observational study. COPD. 2014;11(2):133–142. | ||
Halvani A, Mohsenpour F, Nasiriani K. Evaluation of exogenous melatonin administration in improvement of sleep quality in patients with chronic obstructive pulmonary disease. Tanaffos. 2013;12(2):9–15. | ||
Nunes DM, Mota RMS, Machado MO, Pereira EDB, de Bruin VMS, de Bruin PFC. Effect of melatonin administration on subjective sleep quality in chronic obstructive pulmonary disease. Braz J Med Biol Res. 2008;41(10):926–931. | ||
Gumral N, Naziroglu M, Ongel K, et al. Antioxidant enzymes and melatonin levels in patients with bronchial asthma and chronic obstructive pulmonary disease during stable and exacerbation periods. Cell Biochem Funct. 2009;27(5):276–283. | ||
Shin IS, Shin NR, Park JW, et al. Melatonin attenuates neutrophil inflammation and mucus secretion in cigarette smoke-induced chronic obstructive pulmonary diseases via the suppression of Erk-Sp1 signaling. J Pineal Res. 2015;58(1):50–60. | ||
Kim GD, Lee SE, Kim TH, Jin YH, Park YS, Park CS. Melatonin suppresses acrolein-induced IL-8 production in human pulmonary fibroblasts. J Pineal Res. 2012;52(3):356–364. | ||
Hales CA, Musto SW, Janssens S, et al. Smoke aldehyde component influences pulmonary edema. J Appl Physiol. 1992;72:555–561. | ||
Finkelstein EI, Nardini M, Van Der Vliet A. Inhibition of neutrophil apoptosis by acrolein: a mechanism of tobaccorelated lung disease? Am J Physiol Lung Cell Mol Physiol. 2001;281:L732–L739. | ||
Partridge L, Alic N, Bjedov I, Piper MDW. Ageing in drosophila: the role of the insulin/Igf and TOR signalling network. Exp Gerontol. 2011;46(5):376–381. | ||
Haroon M, Fitzgerald O. Vitamin D and its emerging role in immunopathology. Clin Rheumatol. 2012;31(2):199–202. | ||
Garland CF, Garland FC, Gorham ED, et al. The role of vitamin D in cancer prevention. Am J Public Health. 2006;96(2):252–261. | ||
Ginde AA, Mansbach JM, Camargo CA. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2009;169(4):384–390. | ||
Zhu B, Zhu B, Xiao C, Zheng Z. Vitamin D deficiency is associated with the severity of COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1907–1916. | ||
Kunisaki KM, Niewoehner DE, Connett JE. COPD Clinical Research Network. Vitamin D levels and risk of acute exacerbations of chronic obstructive pulmonary disease: a prospective cohort study. Am J Respir Crit Care Med. 2012;185(3):286–290. | ||
Quint JK, Donaldson GC, Wassef N, Hurst JR, Thomas M, Wedzicha JA. 25-hydroxyvitamin D deficiency, exacerbation frequency and human rhinovirus exacerbations in chronic obstructive pulmonary disease. BMC Pulm Med. 2012;12:28. | ||
Lehouck A, Mathieu C, Carremans C, et al. High doses of vitamin D to reduce exacerbations in chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2012;156(2):105–114. | ||
Hornikx M, Van Remoortel H, Lehouck A, et al. Vitamin D supplementation during rehabilitation in COPD: a secondary analysis of a randomized trial. Respir Res. 2012;13(1):84. | ||
Bjerk SM, Edgington BD, Rector TS, Kunisaki KM. Supplemental vitamin D and physical performance in COPD: a pilot randomized trial. Int J Chron Obstruct Pulmon Dis. 2013;8:97–104. | ||
Martineau AR, James WY, Hooper RL, et al. Vitamin D3 supplementation in patients with chronic obstructive pulmonary disease (ViDiCO): a multicentre, double-blind, randomised controlled trial. Lancet Respir Med. 2015;3(2):120–130. | ||
Zendedel A, Gholami M, Anbari K, Ghanadi K, Bachari EC, Azargon A. Effects of vitamin D intake on FEV1 and COPD exacerbation: a randomized clinical trial study. Glob J Health Sci. 2015;7(4):243–248. | ||
Pedro-Botet J, Climent E, Chillarón JJ, Toro R, Benaiges D, Flores-Le Roux JA. Statins for primary cardiovascular prevention in the elderly. J Geriatr Cardiol. 2015;12(4):431–438. | ||
McFarlane SI, Muniyappa R, Francisco R, Sowers JR. Clinical review 145: Pleiotropic effects of statins: lipid reduction and beyond. J Clin Endocrinol Metab. 2002;87(4):1451–1458. | ||
Young RP, Hopkins RJ. Update on the potential role of statins in chronic obstructive pulmonary disease and its co-morbidities. Expert Rev Respir Med. 2013;7(5):533–544. | ||
Carlson AA, Smith EA, Reid DJ. The stats are in: an update on statin use in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:2277–2284. | ||
Lee TM, Lin MS, Chang NC. Usefulness of C-reactive protein and interleukin-6 as predictors of outcomes in patients with chronic obstructive pulmonary disease receiving pravastatin. Am J Cardiol. 2008;101(4):530–535. | ||
Maneechotesuwan K, Wongkajornsilp A, Adcock IM, Barnes PJ. Simvastatin suppresses airway IL-17 and upregulates IL-10 in patients with stable COPD. Chest. 2015;148(5):1164–1176. | ||
Mroz RM, Lisowski P, Tycinska A, et al. Anti-inflammatory effects of atorvastatin treatment in chronic obstructive pulmonary disease. a controlled pilot study. J Physiol Pharmacol. 2015;66(1):111–128. | ||
Cao C, Wu Y, Xu Z, et al. The effect of statins on chronic obstructive pulmonary disease exacerbation and mortality: a systematic review and meta-analysis of observational research. Sci Rep. 2015;5:16461. | ||
Wang MT, Lo YW, Tsai CL, et al. Statin use and risk of COPD exacerbation requiring hospitalization. Am J Med. 2013;126(7):598–606.e2. | ||
Ingebrigtsen TS, Marott JL, Vestbo J, et al. Characteristics of undertreatment in COPD in the general population. Chest. 2013;144(6):1811–1818. | ||
Lawes CMM, Thornley S, Young R, et al. Statin use in COPD patients is associated with a reduction in mortality: a national cohort study. Prim Care Respir J. 2012;21(1):35–40. | ||
Sheng X, Murphy MJ, MacDonald TM, et al. Effect of statins on total cholesterol concentrations, cardiovascular morbidity, and all-cause mortality in chronic obstructive pulmonary disease: a population-based cohort study. Clin Ther. 2012;34(2):374–384. | ||
Bartziokas K, Papaioannou AI, Minas M, et al. Statins and outcome after hospitalization for COPD exacerbation: a prospective study. Pulm Pharmacol Ther. 2011;24(5):625–631. | ||
Huang CC, Chan WL, Chen YC, et al. Statin use and hospitalization in patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study in Taiwan. Clin Ther. 2011;33(10):1365–1370. | ||
Lahousse L, Loth DW, Joos GF, et al. Statins, systemic inflammation and risk of death in COPD: the Rotterdam study. Pulm Pharmacol Ther. 2013;26(2):212–217. | ||
Criner GJ, Connett JE, Aaron SD, et al. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med. 2014;370(23):2201–2210. | ||
Neukamm A, Høiseth AD, Einvik G, et al. Rosuvastatin treatment in stable chronic obstructive pulmonary disease (RODEO): a randomized controlled trial. J Intern Med. 2015;278(1):59–67. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.