Back to Journals » International Journal of Women's Health » Volume 11
Generational differences in current sexual behavior among Georgian reproductive-aged women
Authors Abzianidze T, Butsashvili M ![]() , Kajaia M, DeHovitz JA, Kamkamidze G
, Kajaia M, DeHovitz JA, Kamkamidze G
Received 8 December 2018
Accepted for publication 21 February 2019
Published 6 May 2019 Volume 2019:11 Pages 301—308
DOI https://doi.org/10.2147/IJWH.S197473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Tinatin Abzianidze,1 Maia Butsashvili,1 Maia Kajaia,1 Jack A DeHovitz,2 George Kamkamidze1
1Health Research Union (HRU), Tbilisi, Georgia; 2Department of Medicine, SUNY Downstate Medical Center, Brooklyn, NY, USA
Background: Following the collapse of the Soviet Union, there was a pronounced change in the availability of modern contraceptive methods and an accompanying shift in the knowledge and attitudes of Georgian women related to sexual behaviors. This study describes differences in sexual behaviors, condom use and family planning practices among several generations of reproductive-aged Georgian women.
Methods: Study participants were recruited from three large cities in Georgia. Women >25 years were recruited from the Cervical Cancer Screening National Program by consecutive sampling; those <25 years were recruited from universities using random sampling. Data collection included self-administered, anonymous surveys. Bivariate analyses were conducted and adjusted prevalence ratios (PR) with 95% confidence intervals were computed.
Results: Among the 350 participants, independent predictors of age at first sexual intercourse were age (aPR 0.27; 95% CI 0.12–0.57), level of education (aPR 0.23; 95% CI: 0.11–0.44), marital status (aPR 2.8;95% CI:1.3–6.0) and religion (aPR 4.01; 95% CI:1.17–13.68). Younger women were more likely to have a premarital sexual relationship compared to older women (RR=0.85; 95% CI: 0.80–0.89); older women were also significantly more likely to use family planning methods with a current partner (RR=2.15; 95% CI: 1.48–3.13). Similarly, advanced education was associated with family planning (RR=1.66; CI: 1.13–2.45).
Conclusions: This study describes clear generational differences in current sexual behavior among Georgian women of reproductive age and these differences, especially in age at first sexual intercourse, premarital sexual relationship and use of contraceptive methods, are influenced by age, level of education, marital status and religion. This information is vital to designing contextually appropriate strategies to prevent sexually transmitted infections.
Keywords: Georgia, generation, sexual behavior, sexual partners contraception, reproductive age, women
Introduction
Following the collapse of the Soviet Union in 1991, Russia and its former republics experienced profound changes in political and economic development, which were accompanied by shifts in traditional cultural norms induced by some assimilation of Western influence. For example, this conservative society has seen a subtle shift in sexual behaviors, the primary determinants of reproductive health,1–3 in the past several decades following the introduction of modern contraceptive methods.4,5 The landscape of Georgian public health has also changed with the introduction of private health care providers, western pharmaceutical companies, mass media, and international foundations and agencies. In addition, new nongovernmental organizations began to play a role in changing sexual behavior and promoting family planning methods. Although systematic sexual education is still not taught in Georgian schools, the younger generation has been exposed to sexual information via a variety of media, such as television, journals and magazines, in contrast to the older generation of women, raised under the strictures of the Soviet Union where public discussion of sexuality was taboo.6
The declining abortion rate is one indicator of change. In the former Soviet countries, including Georgia, induced abortion was the most prevalent method of controlling fertility.7,8 Between 2005 and 2010, the abortion rate declined dramatically from 3.7 to 1.6 (abortions per woman), but still remains high. The increased awareness about reproductive health has supported a shift from abortion to contraception among young women.9 However, the typical Georgian family remains fairly reticent to discuss sexuality, inadvertently leaving the education of young women to the void filled by peers and liberal media influence, which is perhaps moderated by shifting conservative forces. In the former Soviet Union, most youth aged 14–28 were compelled to join the young Communists’ union “Komsomol” which opposed pre-marital sex. Today, religious influences are supplanting Communist principles, wielding a steady conservative influence on the youth, particularly young women. The Orthodox Church is Georgia’s dominant religious institution, one which believes the only appropriate and morally appropriate place for sexual relations is marriage.
This transformation of society has undoubtedly influenced reproductive health in ways which have not yet been quantified. The very limited published data on Georgian women’s sexual behavior are mostly conducted among adolescents. Information on the sexual practices of older generations are not available and there are thus no comparative studies describing trends in sexual behaviors across different age groups. The goal of the study was to assess generational differences in sexual behavior and family planning practices among reproductive-aged Georgian women in response to a dramatically altered social, political and technological milieu. This knowledge will help to shape public health policy and resource allocation.
Methods
Ethics
Before enrollment, each study participant was provided with the information about the purpose, methods, procedures, risks and benefits of the study. Those individuals who agreed to participate signed informed consent form before enrollment in the survey. Prior to the start of the survey, the study protocol was approved by SUNY Downstate Medical Center IRB and Privacy Board (FWA# 00003624) and the Institutional Review Board of Health Research Union (IRB00009520; IORG0005619). The study was conducted in accordance with the Declaration of Helsinki.
Sampling
The majority of the population is ethnic Georgians with Armenians and Azeri representing the largest ethnic minorities.9 Study participants were recruited from the three largest cities in Georgia: Tbilisi (the capital), Batumi (western Georgia), and Rustavi (eastern Georgia). Women over 25 years were recruited from The National Program of Cervical Cancer Screening, operating throughout the country and targeting all female Georgian citizens aged 25–60 years. The largest screening center from each participating city was selected and a consecutive sample of women at each site was included in the study. Younger women (<25 years) were recruited from the universities. A complete list of universities and total enrollment was obtained from the Ministry of Science and Education of Georgia. The names of universities were rearranged at random in a new list. A probability proportional to size (PPS) sampling technique was used for the selection of universities; and from each selected university, complete lists of students were obtained and rearranged at random in a new list. From this new list, study subjects were selected by a simple random sampling approach. Eligibility criteria for study enrollment were: women aged 18–44 years, Georgian or Russian speaking, competency to read the study information sheet and provide informed consent to volunteer for the study.
Data collection
Data collection included a self-administered, anonymous survey. The questionnaire was specifically developed for this study and, prior to administration, it was piloted with 28 women of reproductive age. The questionnaire was used to obtain detailed demographic and reproductive health information. The social-demographic characteristics included age, residence, ethnicity, marital status, birth place, education, employment, family and personal income, living arrangement, religion, etc. Sexual behavior information included the number of sexual partners (lifetime and during the last three months), partner’s status (spouse, boyfriend, random partner etc.) at first sexual intercourse, age at first intercourse and safe sex practices. Reproductive health information included family planning methods, age at menarche, age at first pregnancy and delivery, age at first marriage, time period between first sexual intercourse and first pregnancy, availability and access to family planning methods, and finally, available and preferred sources of information on sexual health, including the role of parents in providing this information.
At the Cervical Cancer Screening Centers, study participants were recruited by nurses. Selected women completed questionnaires in a specially designated space, such as the physician’s office, after which the completed questionnaires were placed in sealed envelopes. At the selected universities, potential participants were approached by the study coordinator. Randomly selected students meeting the eligibility criteria were provided with study information sheets, self-administered and anonymous questionnaires and envelopes. Willing individuals completed the questionnaires in auditoriums and dropped them in sealed envelopes in a special box placed in the lobby. This approach shielded the students from undue influence and/or coercion to take part in the survey.
Statistical analysis
SPSS (IBM) version 23 was used for data management and statistical analysis. Participants were divided into two age groups: less than or equal to 27 years (those born after the collapse of the Soviet Union) and older than 27 years. The main outcome variable was age at first sexual intercourse <21 years. Bivariate analysis was conducted to measure the association between different socio-demographic/behavioral characteristics and having sexual intercourse at a younger age. Logistic regression was used to estimate adjusted prevalence ratios (PR) with 95% confidence intervals.
Results
Out of 385 women approached, 350 agreed to participate (refusal rate 9.1%). Among study participants, 205 (59%) were from Tbilisi, 93 (27%) from Batumi and 52 (15%) from Rustavi. The median age of the respondents was 29 years (range 18–44) and more than half of them (57%) were married. Two-thirds of surveyed women (68%) had a high level of education (University or post-graduate). The proportion of employed women was 55.7% with more than half having a monthly personal income ≤500 Gel (about 200 USD). The distribution of respondents according to ethnicity was as follows: 314 Georgian (90%), 14 Armenian (4%) and 22 Azeri (6%) (Table 1). Most of the respondents (90.3%) were orthodox Christians and 66% among them mentioned that they often (at least once a month) attend religious services. The vast majority of study participants (97.4%) stated that religion is an important issue in their lives. One in 5 women (21.4%) reported past history of tobacco use and 17.7% currently smoke cigarettes. Current alcohol consumption (more than 1 drink 2–3 times per week) was reported by 12.9% of the respondents (Table 2).
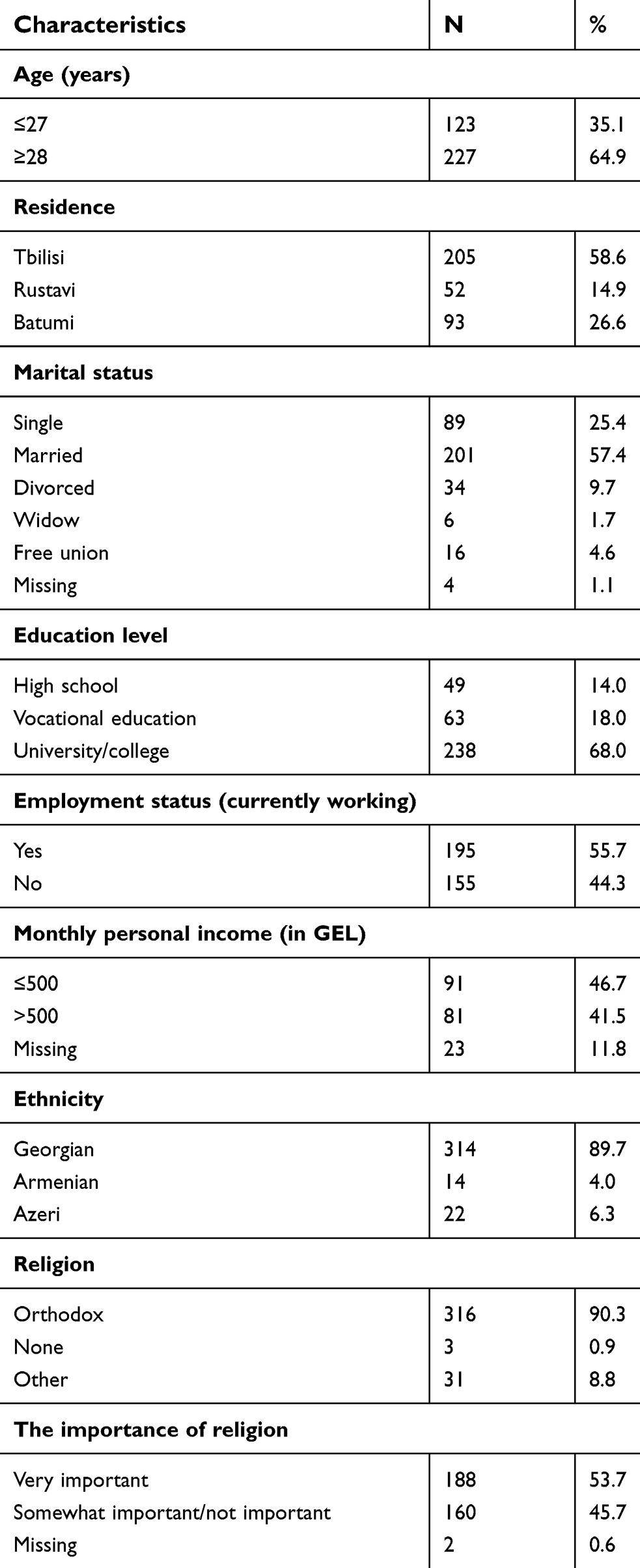 | Table 1 Sociodemographic characteristics of study participant women |
 | Table 2 Behavioral characteristics of study participant women |
The median age of the respondents at menarche was 13. Ever having sexual intercourse was reported by 78.0% of the women. Among those who never had sex the most frequently stated reasons were that having sex before marriage is unacceptable for moral (39.0%) or religious (32.5%) reasons. Of these women, 75.3% will wait until marriage and 25.7% until engagement to have first sexual intercourse. Nearly two-thirds (65.4%) of surveyed women had a spouse or regular sex partner. The median age of study participants at first sexual contact was 21 years and their partners’ median age was 25 years. Two-thirds (66.9%) of surveyed women ever having sex reported that the first sexual intercourse was with their spouse. Respondent’s median age at first marriage, first pregnancy and first delivery was 21 years. Most of the survey participants (60.3%) had one lifetime sexual partner. Among women who ever had sexual intercourse, 53.7% had an induced abortion; the median number of induced abortions was 3 (range 1–13). History of induced abortion was twice as prevalent among women ≥28 years old (61.7%) compared to younger women (31.8%). The median number of days from last sexual intercourse was 7 days and the vast majority of surveyed women (98.4%) had one sex partner during the last 3 months (Table 2).
Using any type of contraceptive method was reported by two thirds (61.7%) of the study participants. The most common family planning method that the respondents ever used was condoms (60.6%), followed by pills (40.3%), intrauterine devices (25.9%) and natural (withdrawal, fertility awareness) methods (13.0%). Among those who reported not using any family planning method, the reasons were desire to have children (42.2%), religious opposition (15.6%), partner refusal (8.9%), fear of health problems associated with contraception (6.7%) and lack of sufficient information about contraceptive methods (4.3%). The vast majority of surveyed women (99.7%) have ever heard about male condoms, but only 36.9% used it with the current partner. The majority of women (83.4%) knew that the purpose of condom use is to avoid unwanted pregnancies as well as prevent HIV and other sexually transmitted infections (STIs). The primary reasons for condom use the last time was to prevent unwanted pregnancies for 32.0% of women. The most common explanations for not using condoms with the current partner was desire to have children (24.4%), followed by not willing to use condoms (20.9%), not feeling at risk of HIV and other STIs from their partners (11.6%), using another contraceptive method (9.3%), and less pleasure (8.1%). Among study participant women, 42.9% never discussed family planning methods with their current partners.
Awareness about STIs was very high among surveyed women (98.6 stated that ever heard about STIs), and 7.7% of the respondents reported that they at least once had STI in their lifetime. Among those with past history of STI, 74.1% were treated at health center and 7.4% conducted self-treatment (either traditional or medical). Only 39.4% of study participants had ever discussed STIs with their partners. The reasons for not discussing STIs were not feeling at risk of STIs (19%), didn’t want to discuss STIs with their partners (14.1%) and trusted their partners (12.7%).
The majority of the respondents (79.7%) reported usually consulting her mother about important matters, while only 48.9% noted that they ever talked with the mother about sex-related issues. Many (27.9%) study subjects stated that it’s difficult or very difficult to talk with the father about important things in their lives and the vast majority (76.9%) have never talked about sex-related issues with their fathers. Physicians (67.4%) and friends (29.7%) were identified as the favored sources of information on sexual and reproductive topics.
In bivariate analysis, younger age (PR=1.68; 95% CI:1.37–2.06), high level of education (PR=1.76; 95% CI:1.43–2.14); non-marital relationships (PR=1.8; 95% CI:1.22–2.64); partner’s status at first intercourse (PR=2.95; 95% CI:1.41–6.18); multiple lifetime partners (PR=1.84; 95% CI:1.06–3.18); and non-orthodox religion (PR=2.47; 95% CI:1.19–5.12) were associated with early sexual intercourse. Earlier first sexual contact was not statistically associated with place of residence (urban vs rural). After adjustment, independent predictors of age at first sexual intercourse were: age, level of education, marital status and religion. (Table 3) Younger women were more likely to have a premarital sexual relationship compared to older women (100% of older women had first sexual intercourse with spouse compared to 85.3% of younger women; RR=0.85; 95% CI: 0.80–0.89).
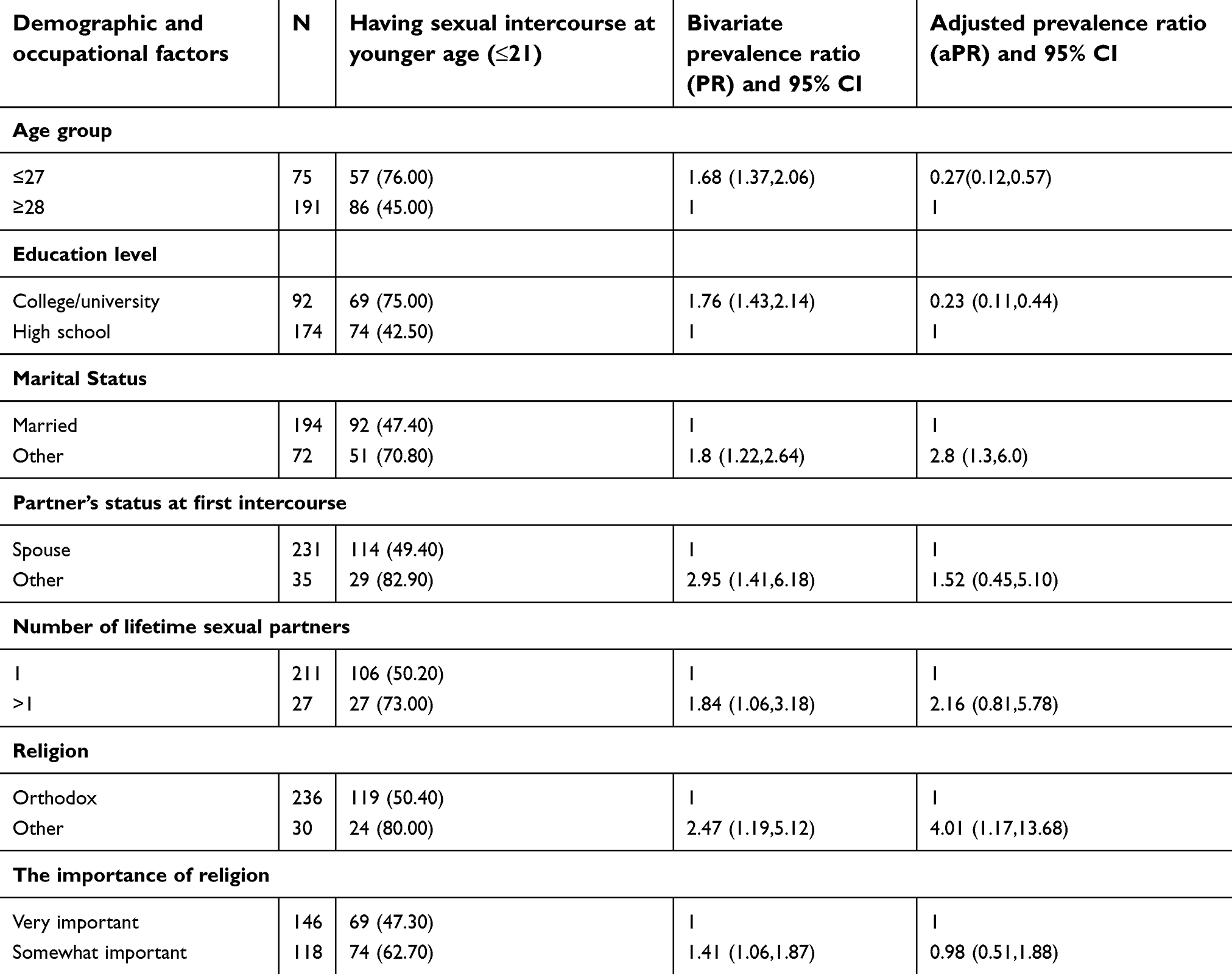 | Table 3 Association of early sexual intercourse with different factors among women of reproductive age in Georgia |
Using family planning methods with current partner was associated with age and education level. A higher proportion of the older women (81.1%) were using family planning methods with the current partner compared to younger women (18.9%) (RR=2.15; 95% CI: 1.48–3.13). Women with a high school level of education were less likely to use family planning methods with their current partners than women with advanced education (RR=1.66; CI: 1.13–2.45).
Discussion
Our study results suggest that first sexual intercourse at an early age is more common among women born after the 1990s than among women born before the collapse of the Soviet Union. This is consistent with other studies conducted elsewhere showing that sexual behaviors and attitudes are changing across the generations.10 Our study further elucidates that premarital sex remains the exception rather than the norm, and while sexual activity appears to commence earlier among younger Georgian women compared to their older peers, the first sexual intercourse remains most likely to be with the woman’s husband. Our findings depart from other study with respect to rural residence and an increased likelihood of earlier first sexual intercourse:11 we did not find any statistically significant difference in age of first intercourse by urban VS rural residence.
In former Soviet countries, including Georgia, induced abortion was the most prevalent method of controlling fertility.7,8 In Georgia, abortion rates remain high with a median number 3 per woman, but increased awareness about sexual and reproductive health has prompted a shift away from abortion to contraception among young women. Two-thirds of our study participants reported ever using any type of contraception, a proportion that remains lower compared to the USA where 99% of women who have ever had sexual intercourse have ever used contraception.12 Proportion of women using modern methods of contraception is alarmingly low in many countries of the Eastern Europe-Central Asia region.13 In five countries of the region (Albania, Azerbaijan, Bosnia and Herzegovina, The Republic of Macedonia and Serbia) this rate is below 22% (the average for the least developed countries)14 and lower than 55% in other 11 countries (the average for the less developed regions).13 Using contraception is important in countries like Georgia which have a high incidence of STIs (24.8% Incidence per 100,000 population)15. In our study young women are more likely to use condoms, but we did not find any association between age and STI history. This is likely due to a persistent lack of awareness that condoms can prevent both unwanted pregnancies and STIs in Georgia compared to other countries.16
A major limitation of this study is self-reported history of sexual behavior ptentially leading to information bias. In addition, the women were well-educated and recruited from either cervical cancer screening clinics or universities. The recruitment strategies employed may thus overestimate the typical knowledge and behaviors about reproductive options. This is relevant to the development of public health strategies to reduce the transmission of STIs.
Conclusion
This study describes clear generational differences in current sexual behavior among Georgian women of reproductive age and these differences, especially in age at first sexual intercourse, premarital sexual relationship and use of contraceptive methods, are influenced by age, level of education, marital status and religion. This information is vital to designing contextually appropriate strategies to prevent sexually transmitted infections. Generation differences in knowledge and attitudes should be taken into account when planning educational interventions.
Key points
- In Georgia, first sexual intercourse at an early age is more common among women born after the 1990s than among women born before the collapse of the Soviet Union.
- Premarital sex remains the exception rather than the norm in Georgia
- Abortion rates remain high with a median number 3 per woman.
Acknowledgment
This study was supported by the NIH Fogarty International Center, Research Grant # 3D43TW0000233.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boyce W, Doherty M, Fortin C, MacKinnon D. Canadian Youth, Sexual Health and AIDS/HIV Study Factors Influencing Knowledge, Attitudes and Behaviors. Canada: Council of Ministers of Education; 2003:
2. Khajehei M, Ziyadlou S, Ghanizadeh A. Knowledge of and attitudes towards sexual and reproductive health in adults in Shiraz: a need for further education. East Mediterr Health J. 2013;19(12):982–989.
3. Rogers C, Earnest J. A cross-generational study of contraception and reproductive health among Sudanese and Eritrean women in Brisbane, Australia. Health Care Women Int. 2014;35(3):334–356. doi:10.1080/07399332.2013.857322
4. Contraceptive use in the countries of the former Soviet union: two decades of transition. Russia Longitudinal Monitoring Survey (RLMS) Perlman and McKee 2009. Available from:
5. Perlman F, McKee M. Trends in family planning in Russia, 1994–200. Perspect Sex Reprod Health. 2009;41(1):40–50. doi:10.1363/psrh.2009.41.issue-1
6. Štulhofer A, Sandfort T. Sexuality and Gender in Postcommunist Eastern Europe and Russia. Routledge, NY. 2008.
7. Mitrofanova E. Demographic behavior of Russians: family and fertility patterns across generations. Macrotheme Rev. 2013;2(3):71–80.
8. Serbanescu F, Stupp P, Westoff C. Contraception matters: two approaches to analyzing evidence of the abortion decline in Georgia. Int Perspect Sex Reprod Health. 2010;36(2):099–110. doi:10.1363/33609910
9. Reproductive health survey, Georgia 2010. National Center for Disease Control and Public Health (NCDC). Available from:
10. Finer LB, Philbin JM. Trends in ages at key reproductive transitions in the United States, 1951–2010. Womens Health Issues. 2014;24(3):e271–e279. doi:10.1016/j.whi.2014.02.002
11. Daniels K, Martinez GM, Nugent CN. Urban and rural variation in fertility-related behavior among U.S. women, 2011–2015. NCHS Data Brief; 2017 January;(297):1–8.
12. Daniels K, Daugherty J, Jones J, Mosher W. Current contraceptive use and variation by selected characteristics among women aged 15–44: United States, 2011–2013. Natl Health Stat Report; 2015 November 10;(86):1–14.
13. Key factors influencing contraceptive use in Eastern Europe and Central Asia 2012.UNFPA. Available from:
14. State of the world population report, 2012. UNFPA. Available from:
15. Gamkrelidze A, Kereselidze M, Tsintsadze M. Health Care Statistical Yearbook 2016, Georgia. Ministry of Labour, Health and Social Affairs of Georgia; National Center for Disease Control and Public Health. Available from:
16. Åkerman E, Östergren PO, Essén B, Fernbrant C, Westerling R. Knowledge and utilization of sexual and reproductive healthcare services among Thai immigrant women in Sweden. BMC Int Health Hum Rights. 2016;16(1):25. doi:10.1186/s12914-016-0100-4
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.