")
Back to Journals » Journal of Asthma and Allergy » Volume 17
Usefulness of Computed Tomography for Evaluating the Effects of Bronchial Thermoplasty in Japanese Patients with Severe Asthma
Authors Abe S, Yasuda M, Tobino K, Harada S, Sasano H, Tanabe Y, Sandhu Y, Takeshige T, Matsuno K , Asao T , Sueyasu T, Nishizawa S, Yoshimine K, Ko Y, Yoshimatsu Y , Tsuruno K, Ide H, Takagi H, Ito J, Nagaoka T, Harada N , Takahashi K
Received 1 December 2023
Accepted for publication 21 March 2024
Published 6 April 2024 Volume 2024:17 Pages 325—337
DOI https://doi.org/10.2147/JAA.S452865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Sumiko Abe,1 Mina Yasuda,1,2 Kazunori Tobino,1,2 Sonoko Harada,1,3 Hitoshi Sasano,1 Yuki Tanabe,1 Yuuki Sandhu,1 Tomohito Takeshige,1 Kei Matsuno,1 Tetsuhiko Asao,1 Takuto Sueyasu,2 Saori Nishizawa,2 Kohei Yoshimine,2 Yuki Ko,2 Yuki Yoshimatsu,2 Kosuke Tsuruno,2 Hiromi Ide,2 Haruhi Takagi,1 Jun Ito,1 Tetsutaro Nagaoka,1 Norihiro Harada,1,3,4 Kazuhisa Takahashi1,4
1Department of Respiratory Medicine, Juntendo University Faculty of Medicine and Graduate School of Medicine, Tokyo, Japan; 2Department of Respiratory Medicine, Iizuka Hospital, Fukuoka, Japan; 3Atopy (Allergy) Research Center, Juntendo University Faculty of Medicine and Graduate School of Medicine, Tokyo, Japan; 4Research Institute for Diseases of Old Age, Juntendo University Faculty of Medicine and Graduate School of Medicine, Tokyo, Japan
Correspondence: Norihiro Harada, Department of Respiratory Medicine, Juntendo University Faculty of Medicine and Graduate School of Medicine, 3-1-3 Hongo, Bunkyo-ku, Tokyo, 113-8431, Japan, Tel +81-3-5802-1063, Fax +81-3-5802-1617, Email [email protected]
Background: Bronchial thermoplasty (BT) improves clinical outcomes and quality of life for patients with severe asthma and has shown sustained reductions in airway narrowing and air trapping in previous CT studies. However, there is a lack of a comprehensive analysis, including CT evaluation, of clinical outcomes in Japanese patients who have undergone BT for severe asthma. This study aimed to evaluate the impact of BT in Japanese asthma patients, with a focus on the CT metric “WA at Pi10” to assess airway disease.
Methods: Twelve patients with severe persistent asthma who underwent BT were assessed using ACQ6, AQLQ, pulmonary function tests, FeNO measurement, blood sampling, and chest CT before BT and one year after the third procedure for the upper lobes.
Results: The median age of the patient was 62.0 years, 7/12 (58.3%) were male, 4/12 (33.3%) used regular oral corticosteroids, and 8/12 (66.7%) received biologics. Median FEV1% was 73.6%, and median peripheral eosinophil count was 163.8/μL. After one year of BT, ACQ6 scores improved from 2.4 to 0.8 points (p = 0.007), and AQLQ scores improved from 4.3 to 5.8 points (p < 0.001). Significant improvements were also observed in asthma exacerbations, unscheduled visits due to exacerbations, FeNO, and √WA at Pi10 (p < 0.05). The baseline mucus score on the CT findings was negatively correlated with FEV1 (r = − 0.688, p = 0.013) and with the maximum mid-expiratory flow rate (r = − 0.631, p = 0.028), and positively correlated with the peripheral blood eosinophil count (r = − 0.719, p = 0.008). Changes in √WA at Pi10 after one year were positively correlated with changes in the mucus score (r = 0.742, p = 0.007).
Conclusion: This study has limitations, including its single-arm observational design and the small sample size. However, BT led to a symptomatic improvement in patients with severe asthma. The validated “√WA at Pi10” metric on CT effectively evaluated the therapeutic response in Japanese asthma patients after BT.
Keywords: asthma, bronchial thermoplasty, chest computed tomography, asthma control questionnaire, √WA at Pi10
Introduction
Despite the availability of effective long-term control medications for asthma, such as inhaled corticosteroids (ICS) and biologics, certain asthma patients continue to experience poor control and some exhibit resistance to biologics.1 The presence of such patients has led to recognition of the diversity of airway inflammation that exists in severe asthma.2 Excessive contraction and hypertrophy of the airway smooth muscle layer play a role in exacerbating asthma and contribute to the key characteristics of severe asthma, regardless of the heterogeneity of airway inflammation.3,4 Bronchial thermoplasty (BT) is a catheter-based, bronchoscopic, non-pharmacological interventional therapy approved for patients aged 18 years and older who have persistent severe asthma that remains poorly controlled despite appropriate treatment. During bronchoscopy, BT delivers radiofrequency energy that heats the wall of the airway and leads to a sustained decrease in the smooth muscle mass of the airway and the ends of the bronchial nerves, as evidenced by histological studies on thermal ablation.5 Randomized controlled clinical trials and real-world clinical registries have provided evidence of significant improvements in the symptoms of severe asthma after BT, as well as improved clinical outcomes, including a reduction in severe asthma exacerbations, hospital emergency visits, and hospital admissions, as well as a better quality of life.5,6 A long-term study conducted in 16 hospitals in the United States, the United Kingdom, Canada, Brazil, and the Netherlands followed a large group of participants treated with BT for 10 years or more. The study demonstrated the safety of BT and provided evidence of the sustained functional stability and clinical benefits experienced by these patients.6 However, despite these improvements, there was a limited correlation between the values of the lung function tests between before and after BT. The physiological mechanisms through which alterations in the smooth muscle layer translate into clinical benefits, including improvement in symptoms and reduced asthma exacerbations, remain unclear in patients who undergo BT.
Computed tomography (CT) provides highly valuable morphometric data in chronic obstructive pulmonary disease.7 Bronchial wall thickening on CT is present in approximately 60% of asthma patients and is therefore a potentially useful indicator to assess the therapeutic response.8 Multiple studies have examined the effects of BT by analyzing CT findings within a 6-week to 2-year post-procedure timeframe.9,10 These studies consistently demonstrated that BT led to sustained reductions in airway narrowing and air trapping among patients with severe asthma.9,10 Such improvements are closely associated with relief of symptoms and decreased airway resistance. Chest CT in asthma patients can also reveal the presence of mucus plugs, which are linked to the deterioration of airflow limitation.11,12 It is crucial to address mucus plugs to effectively manage asthma symptoms. Despite the fact that BT has been accessible in Japan since 2015, there remains a lack of a comprehensive analysis of clinical outcomes, including evaluation of chest CT scans, in Japanese patients with severe asthma who have undergone BT. The potential for improved accuracy with the recently introduced “square root of the airway wall area (WA) of a theoretical airway with an internal perimeter (Pi) of 10 mm” (√WA at Pi10) as a standardized measure of airway wall thickness. However, to date, no studies have utilized this method to assess clinical response after BT.9,13,14 √WA at Pi10 is a surrogate measure of airway wall thickness and is calculated from numerous measurements of airway lumen and airway wall throughout the lung that can be seen on chest CT. CT airway measurements are expressed in terms of airway wall thickness and lumen area of specific segmental and subsegmental bronchioles, which require a set of accurately labeled airway branches and are difficult to perform in routine clinical practice. √WA at Pi10 provides a useful summary score of airway wall thickness for individual patients, conveniently derived from CT images obtained in routine clinical practice. Therefore, the present study aimed to evaluate the association between CT findings and the effects of BT, focusing on the metrics of √WA at Pi10 and mucus score as promising candidates to evaluate the state of airway disease, in Japanese asthma patients who underwent BT.
Methods
Patients
In this prospective non-interventional observational cohort study, patients diagnosed with asthma were enrolled and scheduled to undergo BT. Participants were recruited from among patients aged ≥18 years with a diagnosis of severe asthma and who experienced uncontrolled symptoms despite current treatment options and received treatment at Juntendo University Hospital (Tokyo, Japan) and Iizuka Hospital (Fukuoka, Japan). The diagnosis of asthma was confirmed based on a clinical history of episodic symptoms accompanied by airflow limitation, along with variations in lung function assessed by forced expiratory volume in 1 s (FEV1) or peak expiratory flow rate measurements, following the guidelines provided by the Global Initiative for Asthma (GINA).15 Patients who met any of the following criteria were excluded from the study: (1) diagnosis of infectious disease or cancer; (2) presence of an implanted electrical device such as a pacemaker; (3) history of asthma exacerbation within the last 14 days; (4) inability to undergo bronchoscopy; and (5) cases judged inappropriate by the study investigators.
BT Procedure
BT was performed using the Alair System (Boston Scientific, Tokyo, Japan), which administers radiofrequency energy, a combination of magnetic and electrical energy, as previously described.5,9 The electrode array is introduced and expanded to contact the airway walls under direct visualization through the working channel of a high-frequency compatible flexible bronchoscope (Supplementary Figure 1). Activation of the Alair radiofrequency controller occurs only when the electrodes are in suitable contact with the airway walls, leading to the delivery of radiofrequency energy. This energy is transmitted from the electrode through the airway wall and is converted to thermal energy upon absorption by high-resistance tissue such as smooth muscle. Patients received a daily dose of 50 mg prednisolone for 5 days: 3 days before BT, on the day of BT, and the day after BT. All BT procedures were performed under sedation, with a minimum interval of 3 weeks between treatment of the right lower lobe as the initial step, followed by the left lower lobe, and finally both upper lobes. During BT, thermal energy (radiofrequency ablation) was delivered to the airway wall of subsegmental bronchi of diameter 3–10 mm, specifically targeting the third to fourth generation of airways.
The following assessments were conducted before BT and one year after the third procedure: asthma control questionnaire 6 (ACQ6), asthma quality of life questionnaire (AQLQ), pulmonary function tests, fractional exhaled nitric oxide (FeNO) levels, blood sampling and chest CT. FeNO levels were measured using an electrochemical handheld NO analyzer (NIOX VERO®; Aerocrine AB, Solna, Sweden) according to the recommendations of the American Thoracic Society. The measurements were taken at a constant flow rate of 0.05 L/s against an expiratory resistance of 20 cm of water.
Criteria for Responsiveness to BT
The patients were categorized as responders according to the criteria used in various previous studies, taking into consideration alterations in ACQ6 score, lung function, and asthma exacerbations.16–21 A patient was considered a responder if he met at least two of the following three criteria one year after BT: (1) improvement of at least 0.5 points in the ACQ6 score, (2) reduction in the number of asthma exacerbations, and (3) improvement in FEV1 of at least 100 mL.
Quantification of Serum Cytokine and Chemokine Levels
After centrifugation of blood samples, sera from patients were collected and subsequently frozen at –80 °C. The MILLIPLEX multiplex assay was used for analysis of the collected sera, following the manufacturer’s instructions (Merck Millipore, Burlington, MA, USA). The working range of the assay was determined between the lower and upper limits of quantification, as indicated in Supplementary Table 1. The measurement of serum periostin levels was carried out using ELISA (Shino-Test, Kanagawa, Japan), following the established protocol.22 To quantify serum tenascin-C and regulated on activation, normal T cell expressed and secreted (RANTES), thawed serum samples were simultaneously assessed using the human tenascin-C ELISA kit (IBL, Gunma, Japan) and the human RANTES ELISA kit (R&D Systems, Minneapolis, MN, USA), respectively.
CT Techniques and Airway Analysis
Thoracic thin-section CT scans were obtained at 120 kVp and 250 mA using LightSpeed VCT (GE Medical Systems, Milwaukee, WI, USA) in 3 patients and Aquilion ONE (Toshiba, Tokyo, Japan) in 9 patients. CT was performed with the patient in the supine position and with full inspiration, and acquired within one month prior to BT and 12 months after the third BT procedure. For each patient, all CT examinations were obtained using the same CT scanner. No contrast media were used. Axial images were obtained at 0.5 mm thickness with the lung algorithm for airway analysis (STANDARD for LightSpeed VCT, FC03 for Aquilion ONE). Airway dimension analysis was performed using Airway Inspector (Airway Inspector, Brigham and Women’s Hospital, Boston, MA, USA) [www.airwayinspector.org].23,24 The inner and outer airway walls were identified using full width at half maximum and phase congruency edge detection methods.25 The airway parameters WA and airway Pi were investigated for all airways visible in CT as tangential cross sections (with an internal diameter length/shortness ratio of approximately 0.9–1.1). For each measured airway, the square root of WA was plotted against Pi and the regression line of this plot was used to determine the square root of the wall area of a “theoretical airway” with a 10 mm inner circumference, defined as √WA at Pi1013 (Supplementary Figure 2). All examinations were visually inspected by a senior chest respiratory physician for the absence of significant motion artifacts and inclusion of the entire chest.
Mucus Score
The presence of mucus plugs was assessed by CT images, defined as complete airway obstruction, using the visual lung segment-based scoring system developed by Dunican et al.11 Twenty lung segments were visually inspected and scored for the presence (score 1) or absence (score 0) of one or more mucus plugs. The scores for individual lung segments were summed to produce an overall lung mucus score from 0 to 20 for each participant. Segmental mucus plugs were scored on CT by two senior chest respiratory physicians, and a segment was scored as plugged only if both readers independently agreed.
Statistical Analysis
The D’Agostino–Pearson test was used to assess the normality of the samples. To determine the significance of parameter differences before BT and one year after the third BT procedure, the paired t-test and Wilcoxon signed rank test were used as appropriate. Pearson’s correlation coefficient and Spearman’s rank correlation coefficient were used to analyze the correlations between √WA at Pi10 and mucus score and each parameter, and among each change the √WA at Pi10 and mucus score and parameters from pre-BT values to one year after BT. Statistical significance was considered for p values < 0.05. GraphPad Prism version 6 software (GraphPad Software, San Diego, CA, USA) was used to perform all statistical analyzes.
Ethics
The present study, aligned with the Declaration of Helsinki, underwent review and approval by the Juntendo University Research Ethics Committee (Tokyo, Japan), receiving approval number 15–128. Before participating in the study, each patient gave his written informed consent. The study was registered in the UMIN Clinical Trial Registry on 6 January 2016 (UMIN000020443) (http://www.umin.ac.jp/).
Results
Baseline Characteristics
A total of 12 patients with severe asthma, whose asthma symptoms were not adequately controlled by their current treatment regimens, including the biologic agents available for each patient, were enrolled in the study and underwent BT. Eight patients underwent treatment with the following biologics during the BT treatment period: omalizumab (n = 6), mepolizumab (n = 1), and benralizumab (n = 1) (Table 1). The remaining four patients did not use biologics for their asthma during this period. Of these, a patient had previously experienced anaphylaxis due to biologics and was unable to continue his usage, a patient was being treated with biologics for connective tissue disease, and two voluntarily opted not to receive biologics as part of their treatment for financial reasons. Table 1 lists the baseline characteristics of the patients. The median age (interquartile range) was 62.0 (41.3–70.5) years, the median duration of asthma was 23.0 (7.3–50.3) years (Table 1), 7 (58.3%) were male, and 4 (33.3%) were on regular oral corticosteroids (OCS) (Table 1). The median percentage of FEV1 (FEV1%), which is the ratio of FEV1/forced vital capacity (FVC) and is calculated by dividing FEV1 by FVC, was 73.6% (60.6–82.2), and the median peripheral eosinophil count was 163.8/μL (81.8–397.0) (Table 2). Among the CT findings, the mucus score was negatively correlated with FEV1 (r = −0.688, p = 0.013) and with the maximum mid-expiratory flow rate (MMF) (r = −0.631, p = 0.028), and positively correlated with peripheral blood eosinophil count (r = −0.719, p = 0.008) (Table 3).
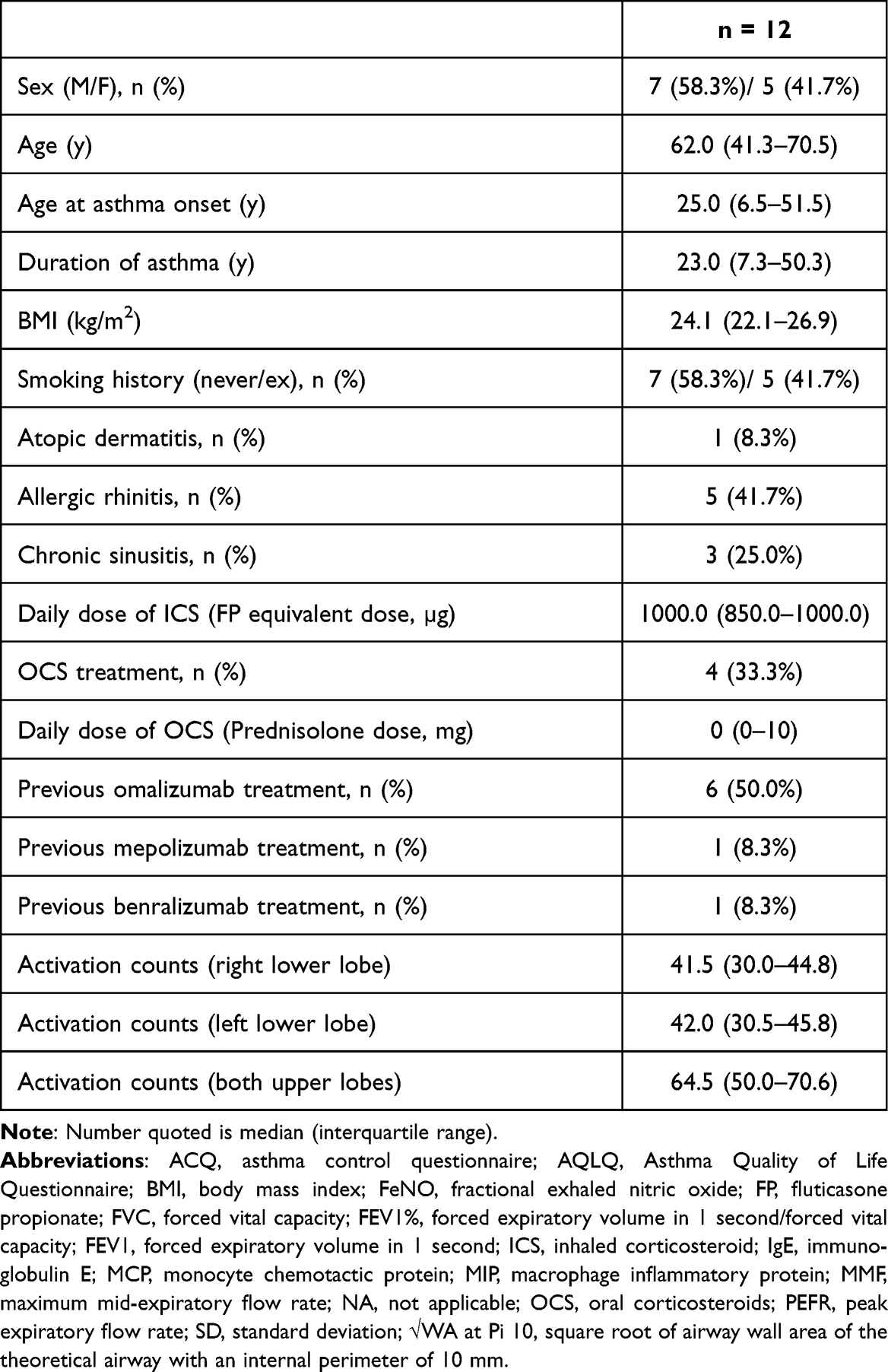 |
Table 1 Baseline Characteristics of the Study Population |
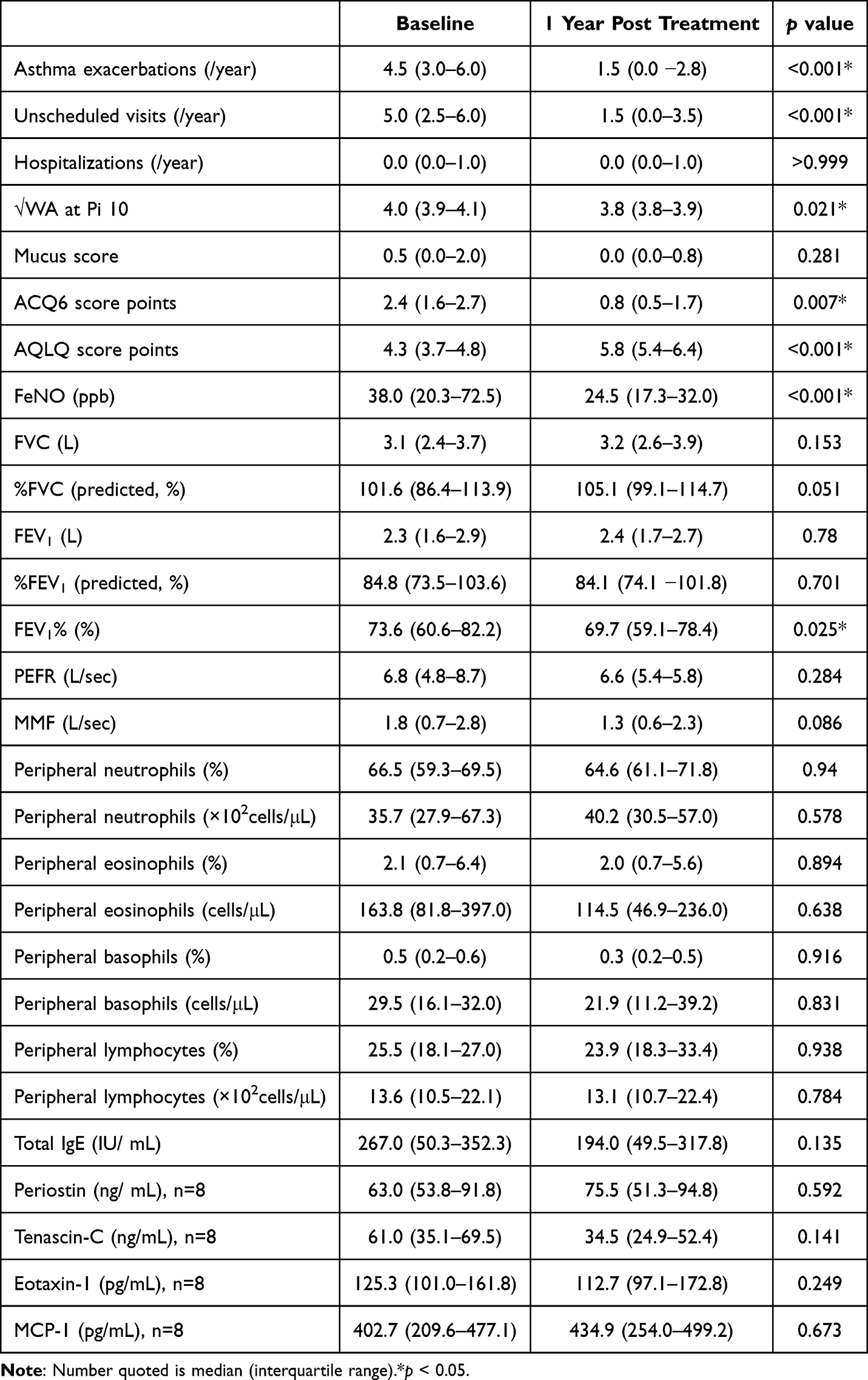 |
Table 2 Baseline Characteristics of the Study Population and Kinetics of Parameters in Patients Treated with BT |
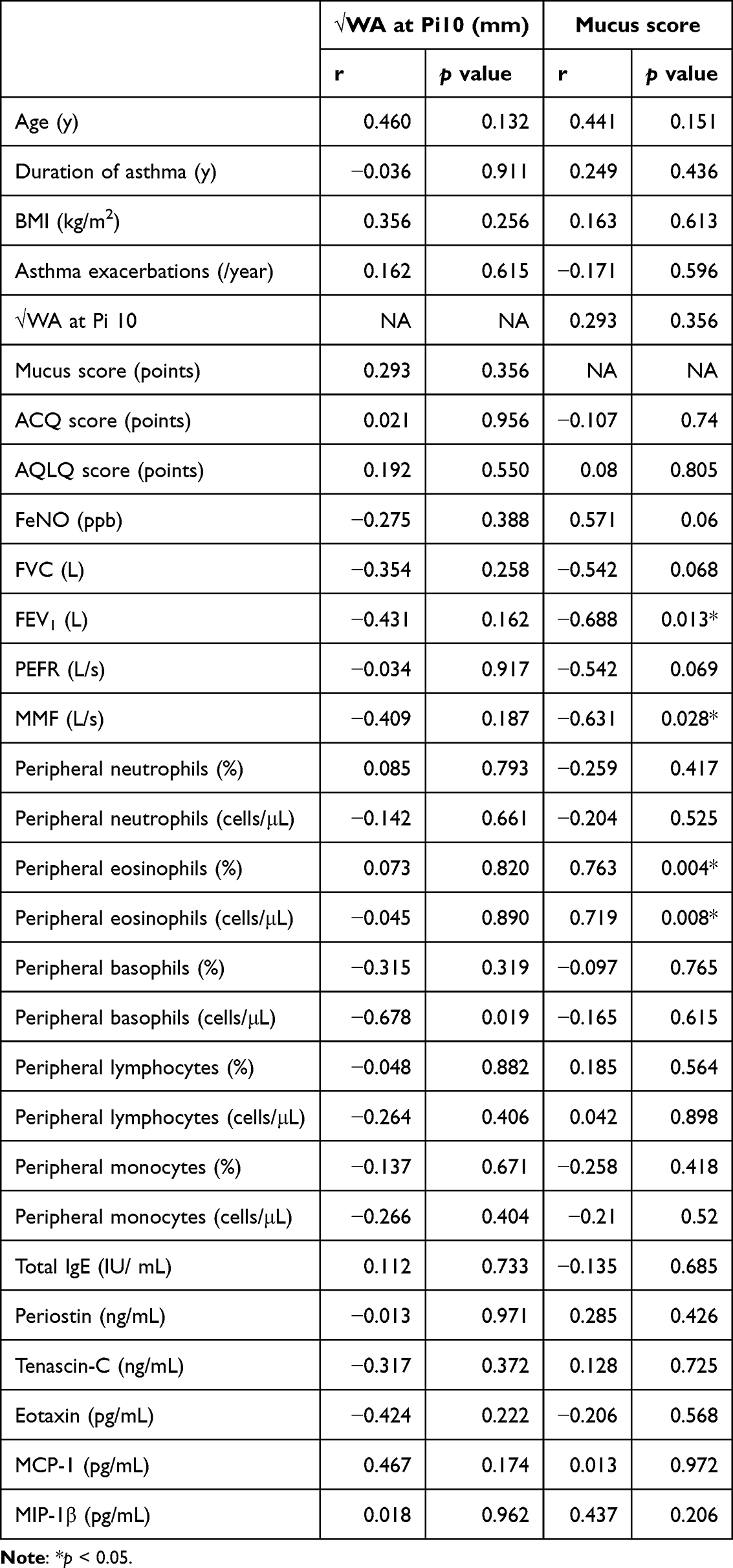 |
Table 3 The Correlation Coefficients Between CT Findings and Baseline Characteristics |
Complications were observed immediately after BT in 11 out of 12 patients (91.7%). Among them, consolidation or atelectasis was detected on X-ray and CT in 9 patients (75.0%), while exacerbation of asthma occurred in 2 patients (1 duplicate case). Seven (58.3%) of these patients required short-term OCS. Furthermore, a patient (8.3%) developed pneumonia and received oral antimicrobial treatment.
Change in Parameters 1 Year After BT
In 9/12 patients (75%), ACQ6 and AQLQ scores at one year after BT demonstrated an improvement of at least 0.5 points compared to the pre-BT values, which is considered the minimal clinically important difference.26,27 Specifically, the ACQ6 scores showed a significant decrease from 2.4 to 0.8 points (p = 0.007), and the AQLQ scores showed a significant increase from 4.3 to 5.8 points (p < 0.001) (Table 2). Furthermore, there was a considerable reduction in the frequency of asthma exacerbations and unscheduled visits due to exacerbations (p < 0.001). Additionally, FeNO levels (p < 0.001) and √WA at Pi10 (p = 0.021) improved significantly (Table 2 and Figure 1). There was no significant change in airflow limitation, except for a significant decrease in the median FEV1% from 73.6% to 69.7% after one year (p = 0.025) (Table 2 and Figure 1). Supplementary Figure 3 presented an example of bronchial wall thinning and lumen expansion resulting from BT. Serum levels of total IgE, periostin, tenascin-C, eotaxin-1, and MCP-1 did not show statistically significant changes between baseline and BT 1 year later (Table 2).
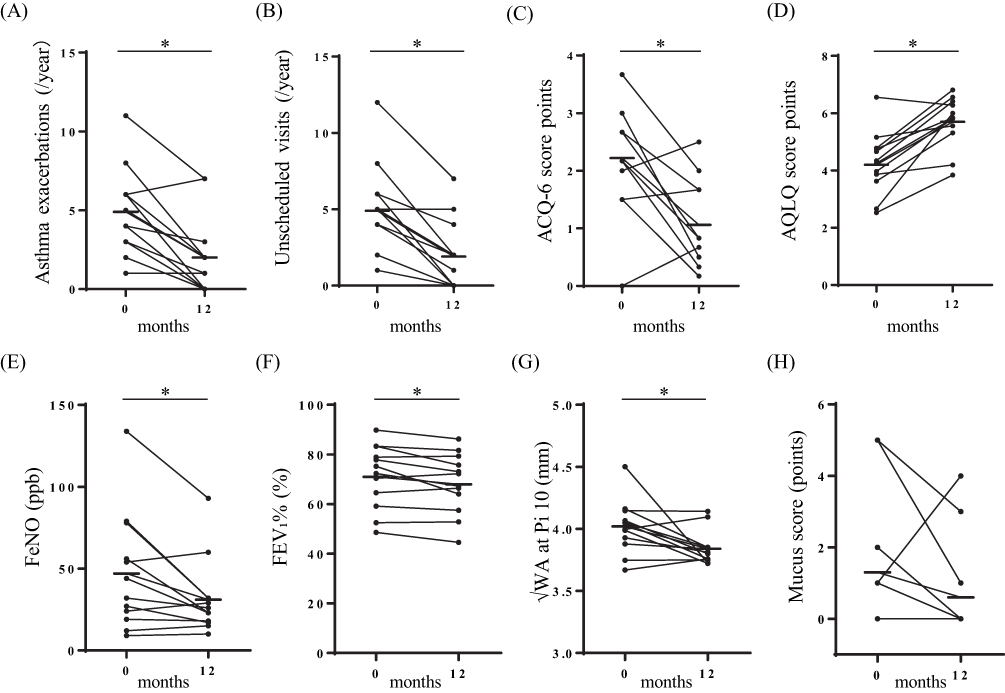 |
Figure 1 Change in parameters between before BT and one year after the third BT procedure. There was a significant decrease in the number of asthma exacerbations (A), unscheduled visits due to exacerbations (B), and ACQ6 score (C) after one year. There was a significant increase in the AQLQ score (D), along with a decrease in FeNO (E), FEV1% (F), √WA at Pi10 (G) after one year. There was no significant change in the mucus score (H) during the same period. The bars indicate the median values. *p < 0.05. |
According to the criteria for the responders observed in the method of this study, 9 (75%) of 12 patients were categorized as responders. All those responders showed a significant improvement in √WA at Pi10, ACQ6 score, AQLQ score, and number of exacerbations at one year after BT.
Patients who showed improvement one year after BT were included, including those who decreased or completely stopped taking OCS and biologics. Of the four patients who regularly took OCS, one patient discontinued their use, two patients reduced their dose of prednisolone from 5 to 3 mg, and one patient continued with the same dose. Among patients receiving biologics, a patient successfully stopped benralizumab treatment.
The change in a parameter between the pre-BT value and the year after BT was denoted as Δ. We evaluated the correlation of the change in √WA at Pi10 (Δ√WA at Pi10) and the change in the mucus score (ΔMucus score) with each baseline parameter, as well as with each other (Table 4). Δ√WA at Pi10 was negatively correlated with baseline √WA at Pi10 (r = −0.673, p = 0.019) and baseline mucus score (r = −0.752, p = 0.008) (Table 4 and Figure 2). ΔMucus score exhibited a negative correlation with the baseline mucus score (r = −0.713, p = 0.009) and a positive correlation with Δ√WA at Pi10 (r = 0.742, p = 0.007) (Table 4 and Figure 2).
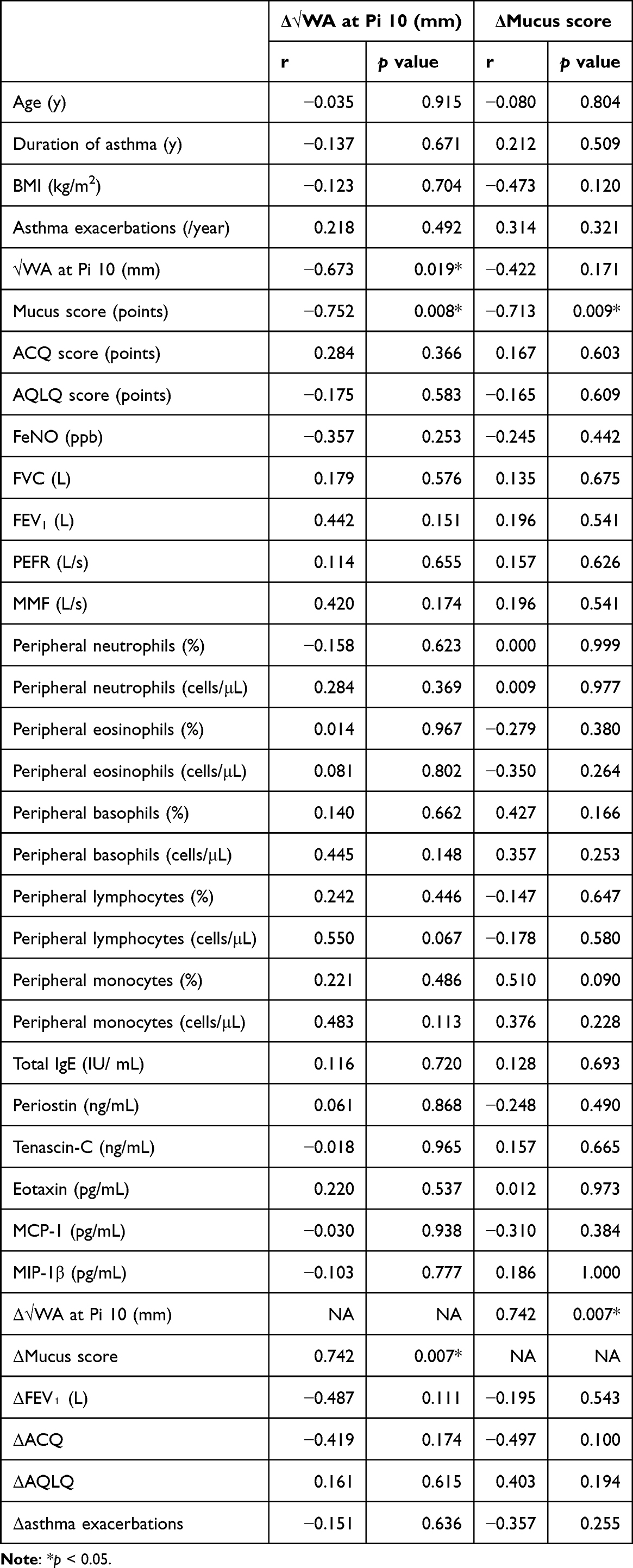 |
Table 4 The Correlation Coefficients Between Δ√WA at Pi 10 and Δmucus Score |
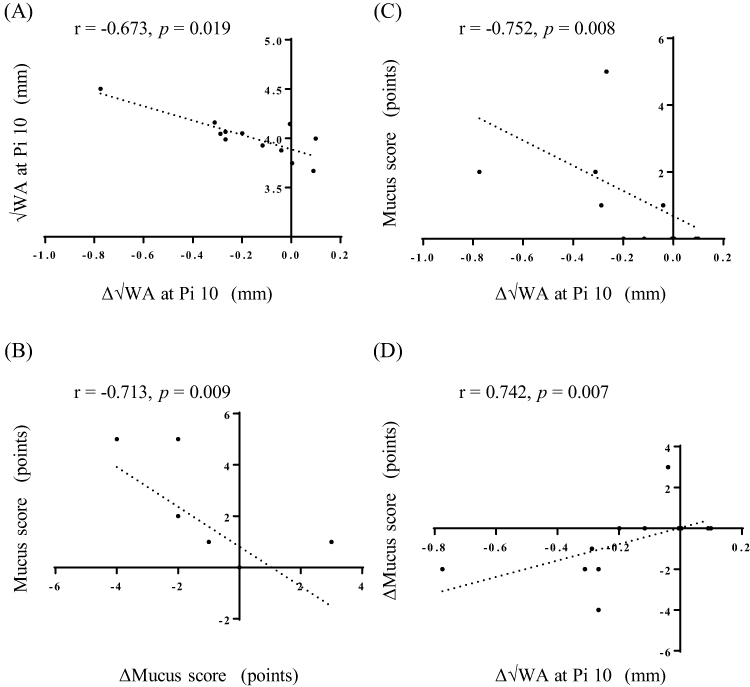 |
Figure 2 Correlation between √WA at Pi10 and mucus score. There were significant negative correlations between pre-BT values and changes from pre-BT values to those recorded one year after the third BT procedure in √WA at Pi10 (Δ√WA at Pi10) (A) and in the mucus score (ΔMucus score) (B), respectively. Δ√WA at Pi10 was negatively correlated with the baseline mucus score (C) and positively correlated with ΔMucus score (D). |
Discussion
One year after the BT procedure, patients with severe asthma had improved √WA at Pi10 as measured by CT, improved ACQ6 and AQLQ scores, FeNO values, and fewer asthma exacerbations and unscheduled hospital visits, compared to before BT. The amount of change in √WA at Pi10 after one year was positively correlated with the change in mucus score. To our knowledge, this study is the first to mention a positive effect of BT on √WA at Pi10 and mucus score. In addition, the results indicate that √WA at Pi10 can be used to evaluate the dimensions of the standardized airways on CT and effectively assess the therapeutic response in Japanese asthma patients undergoing BT. Konietzke et al compared airway changes between 17 patients with severe asthma who underwent BT and 11 patients with severe asthma who did not undergo BT, and found that the average thickness of the wall, the percentage of the wall, and √WA at Pi10 were significantly reduced throughout the whole lung in those who underwent BT.9 Limited information is available on CT analysis of Japanese asthma patients who received BT; however, the results of evaluation using expiratory CT (n = 10) and xenon ventilation CT (n = 4) demonstrated improvements in expiratory volume and air trapping at 6 and 4 weeks, respectively, after BT.28,29 Only one case report has documented airway lumen dilatation and reduction in bronchial wall thickness following the BT procedure, in a Japanese patient with asthma.30 In the present study of Japanese patients with severe asthma, BT improved √WA at Pi10, which was correlated with an improvement in the mucus score. These findings suggest a possible decrease in airway wall thickness and mucus score in Japanese patients treated with BT and that √WA at Pi10 may provide an accurate assessment of the status of small airway disease. Moreover, the √WA at Pi10 and the mucus score presented distinct differences as biomarkers. The mucus score exhibited correlations with FEV1 and eosinophils, whereas the √WA at Pi10 did not show such associations. These findings might indicate the potential importance of √WA at Pi10, distinguishing it from other biomarkers.
A study that followed patients for ten years after the BT procedure showed no deterioration in quality of life or respiratory function in 136 patients who underwent BT, suggesting that the efficacy of BT persists for more than ten years and has an acceptable safety profile.6 Therefore, BT is indicated for patients aged 18 years or older who experience severe asthma, particularly when treatment remains insufficient despite optimal medical intervention. This includes treatment with high-dose ICS, long-acting beta2-agonists, leukotriene receptor antagonists, long-acting anticholinergics, theophylline, OCS, and biologics. However, due to the prevalence of biologics, which are a safer treatment than BT, the actual indications of BT tend to be limited to patients who cannot achieve symptom control even with biologics and those who cannot tolerate biologic therapy. We observed a similar trend among patients in this study, indicating that there is a certain number of patients with severe asthma for whom BT is a necessary therapeutic tool. A patient in the present study experienced anaphylaxis with three biologics, improved markedly after BT, and now participates in amateur swimming.31 In addition, the success of some of our patients in discontinuing systemic steroids and benralizumab one year after BT indicates the potential of BT to alleviate the side effects associated with systemic steroids, as well as the financial and overall burden of the disease burden experienced by individuals with severe asthma.
Although this study had certain limitations, including being a single-arm open-label observational study with a small sample size, it is important to note that all patients underwent a thorough evaluation, including consideration of biologic treatment options, prior to the initiation of BT. Consequently, we have confidence that the observed clinical improvements in patients with uncontrolled severe asthma after the BT procedure are truly attributable to the effectiveness of BT and not a result of optimized previous background therapy. Furthermore, more research is necessary to determine the utility of √WA at Pi10, as this study did not provide a correlation with CT measurements indicative of an improvement in asthma.
In conclusion, one year after BT treatment, Japanese patients with severe asthma showed significant improvements in multiple aspects. These included a decrease in √WA at Pi10 as measured by CT, improvements in ACQ6 and AQLQ scores and FeNO values, and a decrease in the number of asthma exacerbations and unscheduled hospital visits. Notably, the improvement in √WA at Pi10 at the one-year mark showed a positive correlation with an improvement in the mucus score. √WA at Pi10, a validated quantification method for evaluating standardized airway dimensions on CT scans, might be an effective means of assessing therapeutic response in Japanese asthma patients who underwent BT.
Abbreviations
ACT, asthma control questionnaire; ACQ, asthma control questionnaire; AQLQ, asthma quality of life questionnaire; BT, bronchial thermoplasty; FeNO, fractional exhaled nitric oxide; FP, fluticasone propionate; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; FEV1%, forced expiratory volume in 1 s/forced vital capacity; ICS, inhaled corticosteroid; MIP, macrophage inflammatory protein; MMF, maximum mid-expiratory flow rate; OCS, oral corticosteroids; PEFR, peak expiratory flow rate; RANTES, regulated on activation, normal T cell expressed and secreted; SD, standard deviation; √WA at Pi10, square root of airway wall area of the theoretical airway with an internal perimeter of 10 mm.
Acknowledgments
The authors would like to thank FORTE Science Communications (https://www.forte-science.co.jp/) for English language editing.
Disclosure
NH reports personal fees from AstraZeneca, GlaxoSmithKline, Kyorin, Novartis, and Sanofi; and grants from AstraZeneca, Daikin, and TOSOH, outside of the submitted work. KTa reports grants and personal fees from Chugai Pharmaceutical Co., Ltd.; and grants from Nippon Boehringer Ingelheim Co., Ltd., Bristol-Myers K.K., Eli Lilly Japan K.K., KYORIN Pharmaceutical Co., Ltd., MSD K.K., ONO PHARMACEUTICAL CO., LTD., Sanofi K.K., TEIJIN PHARMA LIMITED, and TAIHO PHARMACEUTICAL CO., LTD.; and personal fees from AstraZeneca, outside of the submitted work. All other authors declare that they have no conflicts of interest.
References
1. Chung KF, Wenzel SE, Brozek JL, et al.. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–373. doi:10.1183/09031936.00202013
2. Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012;18:716–725. doi:10.1038/nm.2678
3. James AL, Bai TR, Mauad T, et al.. Airway smooth muscle thickness in asthma is related to severity but not duration of asthma. Eur Respir J. 2009;34:1040–1045. doi:10.1183/09031936.00181608
4. Langton D, Banks C, Noble PB, Plummer V, Thien F, Donovan GM. The effect of bronchial thermoplasty on airway volume measured 12 months post-procedure. ERJ Open Res. 2020;2020:6.
5. Dombret MC, Alagha K, Boulet LP, et al.. Bronchial thermoplasty: a new therapeutic option for the treatment of severe, uncontrolled asthma in adults. Eur Respir Rev. 2014;23:510–518. doi:10.1183/09059180.00005114
6. Chaudhuri R, Rubin A, Sumino K, et al.. Safety and effectiveness of bronchial thermoplasty after 10 years in patients with persistent asthma (BT10+): a follow-up of three randomised controlled trials. Lancet Respir Med. 2021;9:457–466. doi:10.1016/S2213-2600(20)30408-2
7. Wielputz MO, Eichinger M, Weinheimer O, et al.. Automatic airway analysis on multidetector computed tomography in cystic fibrosis: correlation with pulmonary function testing. J Thorac Imaging. 2013;28:104–113. doi:10.1097/RTI.0b013e3182765785
8. Gupta S, Siddiqui S, Haldar P, et al.. Qualitative analysis of high-resolution CT scans in severe asthma. Chest. 2009;136:1521–1528. doi:10.1378/chest.09-0174
9. Konietzke P, Weinheimer O, Wielputz MO, et al.. Quantitative CT detects changes in airway dimensions and air-trapping after bronchial thermoplasty for severe asthma. Eur J Radiol. 2018;107:33–38. doi:10.1016/j.ejrad.2018.08.007
10. Langton D, Noble PB, Donovan GM. Response of individual airways in vivo to bronchial thermoplasty. J Appl Physiol. 2021;130:1205–1213. doi:10.1152/japplphysiol.00959.2020
11. Dunican EM, Elicker BM, Gierada DS, et al.. Blood institute severe asthma research P. Mucus plugs in patients with asthma linked to eosinophilia and airflow obstruction. J Clin Invest. 2018;128:997–1009. doi:10.1172/JCI95693
12. Tang M, Elicker BM, Henry T, et al.. Mucus Plugs Persist in Asthma, and Changes in Mucus Plugs Associate with Changes in Airflow over Time. Am J Respir Crit Care Med. 2022;205:1036–1045. doi:10.1164/rccm.202110-2265OC
13. Grydeland TB, Dirksen A, Coxson HO, et al.. Quantitative computed tomography: emphysema and airway wall thickness by sex, age and smoking. Eur Respir J. 2009;34:858–865. doi:10.1183/09031936.00167908
14. Kim SS, Jin GY, Li YZ, Lee JE, Shin HS. CT quantification of lungs and airways in normal Korean Subjects. Korean J Radiol. 2017;18:739–748. doi:10.3348/kjr.2017.18.4.739
15. Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and prevention; 2006. Available from: http://www.ginasthma.org/.
16. Eger K, Kroes JA, Ten Brinke A, Bel EH. Long-term therapy response to Anti-IL-5 biologics in severe asthma-a real-life evaluation. J Allergy Clin Immunol Pract. 2021;9:1194–1200. doi:10.1016/j.jaip.2020.10.010
17. Hamada K, Oishi K, Murata Y, Hirano T, Matsunaga K. Feasibility of discontinuing biologics in severe asthma: an algorithmic approach. J Asthma Allergy. 2021;14:1463–1471. doi:10.2147/JAA.S340684
18. Liu MC, Chipps B, Munoz X, et al.. Benefit of switching to mepolizumab from omalizumab in severe eosinophilic asthma based on patient characteristics. Respir Res. 2021;22:144. doi:10.1186/s12931-021-01733-9
19. Mummler C, Munker D, Barnikel M, et al.. Dupilumab improves asthma control and lung function in patients with insufficient outcome during previous antibody therapy. J Allergy Clin Immunol Pract. 2021;9:1177–1185 e1174. doi:10.1016/j.jaip.2020.09.014
20. Sandhu Y, Harada N, Sasano H, et al.. Pretreatment frequency of circulating Th17 Cells and FeNO levels predicted the real-world response after 1 year of benralizumab treatment in patients with severe asthma. Biomolecules. 2023;14:13. doi:10.3390/biom14010013
21. Sasano H, Harada N, Harada S, et al.. Pretreatment circulating MAIT cells, neutrophils, and periostin predicted the real-world response after 1-year mepolizumab treatment in asthmatics. Allergol Int. 2023;2023:1.
22. Okamoto M, Hoshino T, Kitasato Y, et al.. Periostin, a matrix protein, is a novel biomarker for idiopathic interstitial pneumonias. Eur Respir J. 2011;37:1119–1127. doi:10.1183/09031936.00059810
23. Diaz AA, Hardin ME, Come CE, et al.. Childhood-onset asthma in smokers. association between CT measures of airway size, lung function, and chronic airflow obstruction. Ann Am Thorac Soc. 2014;11:1371–1378. doi:10.1513/AnnalsATS.201403-095OC
24. Oguma T, Niimi A, Hirai T, et al.. Assessment of small airways with computed tomography: mosaic attenuation or lung density?. Respiration. 2015;89:539–549. doi:10.1159/000381553
25. Gierada DS, Guniganti P, Newman BJ, et al.. Quantitative CT assessment of emphysema and airways in relation to lung cancer risk. Radiology. 2011;261:950–959. doi:10.1148/radiol.11110542
26. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific quality of life questionnaire. J Clin Epidemiol. 1994;47:81–87. doi:10.1016/0895-4356(94)90036-1
27. Juniper EF, Svensson K, Mork AC, Stahl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99:553–558. doi:10.1016/j.rmed.2004.10.008
28. Ishii S, Iikura M, Shimoda Y, Izumi S, Hojo M, Sugiyama H. Evaluation of expiratory capacity with severe asthma following bronchial thermoplasty. Respirol Case Rep. 2019;7:e00387. doi:10.1002/rcr2.387
29. Dokuni R, Kobayashi K, Ohno Y, et al.. Effect of bronchial thermoplasty on air trapping assessed by xenon ventilation computed tomography. Intern Med. 2021;60:2027–2032. doi:10.2169/internalmedicine.6493-20
30. Ishii S, Iikura M, Hojo M, Sugiyama H. Use of 3D-CT airway analysis software to assess a patient with severe persistent bronchial asthma treated with bronchial thermoplasty. Allergol Int. 2017;66:501–503. doi:10.1016/j.alit.2016.12.008
31. Jingo K, Harada N, Nishioki T, et al.. Anaphylaxis to three humanized antibodies for severe asthma: a case study. Allergy Asthma Clin Immunol. 2020;16:46. doi:10.1186/s13223-020-00446-w
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.