")
Back to Journals » Drug Design, Development and Therapy » Volume 13
The safety, pharmacodynamics, and pharmacokinetics of immediate-release formulation containing esomeprazole 20 mg/sodium bicarbonate 800 mg in healthy adult male
Authors Kim D, Park MS , Yoo BW , Hong T, Park SJ, Kim CO
Received 17 April 2019
Accepted for publication 11 June 2019
Published 3 September 2019 Volume 2019:13 Pages 3151—3159
DOI https://doi.org/10.2147/DDDT.S212491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianbo Sun
Dasohm Kim1,2, Min Soo Park1,2, Byung Won Yoo2, Taegon Hong2, Shin Jung Park3, Choon Ok Kim2
1Department of Pharmaceutical Medicine and Regulatory Sciences, College of Medicine and Pharmacy, Yonsei University, Incheon, Korea; 2Department of Clinical Pharmacology and Clinical Trials Center, Severance Hospital, Yonsei University Health System, Seoul, Korea; 3Chong Kun Dang Research Institute, Chong Kun Dang Pharmaceutical Corporation, Seoul, Korea
Correspondence: Choon Ok Kim
Department of Clinical Pharmacology and Clinical Trials Center, Severance Hospital, Yonsei University Health System, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea
Tel +82 22 228 0455
Fax +82 22 227 7890
Email [email protected]
Background: Esomeprazole is the most effective treatment for acid-related disorders and is widely used with enteric coating due to rapid degradation in the acidic environment. However, the enteric-coated formulation delays absorption and onset of action. To overcome this limitation, an immediate-release formulation containing esomeprazole 20 mg and sodium bicarbonate 800 mg (IR-ESO) was developed.
Purpose: To evaluate the safety, pharmacokinetics (PK), and pharmacodynamics of IR-ESO compared to those of esomeprazole 20 mg (ESO).
Methods: A randomized, open-label, multiple-dose, two-treatment, two-sequence crossover study was conducted in 40 healthy male subjects. Subjects received either IR-ESO or ESO for 7 days. After single and multiple dosing, blood samples were collected for PK analysis, and intragastric pH was assessed by 24-hr pH monitoring.
Results: Plasma esomeprazole exposure of IR-ESO was similar to that of ESO after single and multiple dosing. Time to peak concentration of IR-ESO (0.50–0.75 hr) was shorter than that of ESO (1.25–1.50 hr). Percentage changes in 24-hr integrated gastric acidity from baseline for IR-ESO were similar to those for ESO. In addition, mean time to maintain gastric pH >4 for 24 hr was similar for both drugs (IR-ESO 55.5–69.9% vs ESO 56.8–70.2%). Evaluation of time to first reach pH 4 after dosing indicated that IR-ESO showed a faster onset than ESO. All subjects found the drug tolerable, and there were no significant differences in adverse events between two drugs.
Conclusion: This study showed that IR-ESO produced a rapid, safe and sustained gastric acid suppression (ClinicalTrials.gov: NCT03211143).
Keywords: sodium bicarbonate, immediate-release esomeprazole, esomeprazole, 24-hr pH monitoring
Introduction
Gastro-esophageal reflux disease (GERD) is the most common acid-related disorder, and its typical symptoms include heartburn and/or regurgitation.1 The goal of treatment for GERD is to achieve symptomatic relief.2 The severity and frequency of these symptoms significantly correlate with the degree of esophageal exposure to acid and the pH of the refluxate.3 It is necessary to suppress gastric acid for relieving the symptoms.
Proton pump inhibitors (PPIs) are widely used for the treatment of GERD, and they act by suppressing gastric acid secretion and raising intragastric pH.4 Esomeprazole is one of the most frequently prescribed PPI and provides more rapid and effective relief than other PPIs.5 However, esomeprazole is prone to degradation by gastric acid in the stomach.6,7 To overcome this shortcoming and protect it from rapid degradation, esomeprazole was improved via enteric coating.8,9 The enteric-coated formulation of esomeprazole enhanced the stability of active ingredients in the stomach; however, it also led to delayed absorption and onset of action.8,9
Some studies have indicated that a single dose might not be sufficient to achieve maximum effectiveness due to delayed absorption of enteric-coated esomeprazole.10,11 Esomeprazole with enteric coating showed therapeutic efficacy of approximately 68.3% after 8 weeks of treatment; however, the efficacy was about 45.3% after single dose.12 Despite remarkable effects with respect to the management of GERD, lack of an immediate response might contribute to patient dissatisfaction with treatment and could lead to unnecessary increases in dosage or inappropriate switching to alternate members of this class.10
The sodium bicarbonate is a chemical compound which can be used as an antacid. It raises the pH of the stomach and creates a chemical umbrella that protects the esomeprazole and allows it to pass safely to the duodenum where it is absorbed.13 An immediate-release (IR) formulation containing esomeprazole 20 mg and sodium bicarbonate 800 mg (IR-ESO; Chong Kun Dang Pharmaceutical Corp., Seoul, Korea) was developed to mitigate the delayed onset of action. This study was designed to compare the pharmacokinetics (PK) and pharmacodynamics (PD) of IR-ESO with those of an enteric-coated formulation of esomeprazole.
Materials and methods
Ethics
The protocol was approved by the Institutional Review Board (IRB) of Severance Hospital (Seoul, South Korea, IRB number 4-2017-0310) and the Ministry of Food and Drug Safety. It is also registered at the ClinicalTrials.gov (Identifier: NCT03211143). This study was carried out in accordance with the Declaration of Helsinki and the Korean Good Clinical Practice (KGCP). All subjects provided written informed consent before enrolment in this study.
Subjects
Healthy male subjects aged 19–50 years with body mass index (BMI) between 18.5 and 25.0 kg/m2 were considered for participation in the study. The volunteers were determined as healthy based on medical history, physical examinations, 12-lead electrocardiography (ECG), and laboratory tests such as hematology, serum chemistry, urinalysis, and serology (negative for hepatitis B surface antigen, anti-hepatitis C virus antibody, human immunodeficiency virus serology, and syphilis reagin test). In addition, subjects who met the following criteria were excluded: current smoker, medical history of disease that might influence the PK or PD evaluation in this study, history of clinically significant hypersensitivity reaction to drugs, or positive results in urine drug screening. During the study period, all the subjects were prohibited to take any drugs, herbals, or over-the-counter drugs that could affect PK or PD evaluation. Additionally, subjects were not allowed to smoke or consume alcohol, caffeine, any beverage, or food except the ones provided.
Study design
This was a randomized, open-label, multiple-dose, two-treatment, and two-sequence crossover study design. The two treatments administered were as follows: a fixed dose combination tablet consisting of 20 mg of esomeprazole and 800 mg of sodium bicarbonate once daily for 7 days (test treatment, T), and a tablet of esomeprazole 20 mg once daily for 7 days (reference treatment, R). Forty subjects were randomly assigned to one of the two sequence groups (T-R or R-T) in 1:1 ratio. Each treatment period was separated by a 7-day washout period.
All subjects were hospitalized in the clinical trials center during each treatment period (from Day −2 to Day 8). They underwent 24-hr gastric pH monitoring at baseline, after single administration and after multiple administrations of test or reference treatment in each period. The pH measurement and recording started 30 mins before study drug administration (at approximately 08:00) and were continuously conducted for 24 hrs. During the 24-hr intragastric pH monitoring, all subjects were required to maintain similar posture to minimize its effect on gastric pH. They were required to lie down on the bed during nighttime (23:00 to 07:00) and maintain upright posture with at least 45 degrees during daytime (07:00 to 23:00).
In addition, all the participants received each treatment with 150 mL water under fasting conditions at approximately 08:00 on Day 1 through 7 of each period. During every dose administration and 24-hr intragastric pH monitoring, they ate breakfast at approximately 09:00 for 20 mins and were served lunch and dinner at 13:00 and 18:00, respectively. All meals were nutritionally equivalent (700–800 kcal, containing 5–25% fat content) and were provided at the same time scheduled throughout the study period.
On Days 1 and 7 during each period, blood samples were collected for PK analysis in sodium heparin tubes prior to dose administration, and after 0.17 (=10 mins), 0.33 (=20 mins), 0.5, 0.75, 1, 1.25, 1.5, 2, 2.5, 3, 3.5, 4, 5, 6, 8, 10, and 12 hrs on Days 1 and 7 during each period. The collected blood samples were centrifuged at 3,000 rpm at 4°C for 10 mins and stored below −70°C until analysis.
Plasma esomeprazole assay
The plasma samples for esomeprazole concentration measurement were analyzed using a high-performance liquid chromatography assay, coupled with triple quadrupole mass spectrometer (API 4000, AB SCIEX, USA) equipped with electrospray ionization in positive ion mode. A 50 μL plasma sample was prepared by protein precipitation by mixing with 10 μL of esomeprazole-d3 (500 ng/mL) and 600 μL of acetonitrile. After centrifugation at 13,500 rpm for 10 mins, 2 μL supernatant was injected into the column (Hypersil GOLD, 150*2.1 mm, 5 μm) in the mobile phase, which consisted of 10 mM ammonium formate:acetonitrile with 0.1% formic acid (50:50, v/v). The lower limit of quantification was 1 ng/mL, and precision and accuracy were less than 15% coefficient of variation. The calibration curves had adequate linearity as r >0.9959 in the ranges of 1 to 3,000 ng/mL of sample concentration.
Pharmacokinetic analysis
The PK parameters for esomeprazole were calculated by non-compartmental analysis using Phoenix WinNonlin version 7.0 (Certara, Princeton, NJ, USA). The maximum plasma concentration (Cmax) and time to reach maximum plasma concentration (Tmax) were determined directly from the observed data. The area under the plasma concentration–time curve (AUC) within a dose interval (τ) (AUCτ) and AUC to the last measurable time (AUClast) was calculated using the linear trapezoidal rule. The terminal elimination rate constant (ke) was estimated by log-linear regression analysis. The elimination half-life (t1⁄2) and the apparent plasma clearance (CL/F) were calculated from the equation, t1⁄2=ln(2)/ke and CL/F=dose/AUC, respectively. AUC from 0 to infinity (AUCinf) was obtained by summation of AUClast and Clast/ke. The apparent volume of distribution (Vd/F) was calculated from the equation, Vd/F=Dose/(ke∙AUCinf).
Intragastric pH monitoring
Intragastric pH monitoring was performed using an impedance-pH recorder (Ohmega R, Enschede, Netherlands). Before each 24-hr intragastric pH monitoring, the pH catheter and catheter-based ambulatory pH monitoring system were calibrated using standard buffer solutions (pH 4.0 and 7.0). On Day 1, a pH catheter was inserted into the stomach, and the point (cm) where the pH dropped abruptly to <2.5 for each subject was recorded. The catheter was inserted at the same point for each subject during all 24-hr intragastric pH monitoring. The measurements were taken every second for 24 hrs.
Pharmacodynamic analysis
The primary PD parameters were percentage decrease in integrated gastric acidity from baseline over a 24-hr interval (%IA24hr) after multiple administrations (Day 7). Additionally, PD parameters included %IA24hr after single administration (Day 1), percentage of time with gastric pH >4 for 24-hr interval, and mean gastric acid concentration after single and multiple administrations. Integrated gastric acidity was calculated using the following method.14 Baseline integrated gastric acidity was calculated as the mean of baseline intragastric pH measured between two periods.
- Acid concentration (mmol/L) =1,000×10−pH
- Acidity (mmol∙hr/L) = (acid in mmol/L at time “t” + acid in mmol/L at time “t−1”)/2×(t-t−1)
- Acidity values were summed cumulatively per second. Integrated acidity is expressed as mmol/L×time, ie, mmol∙hr/L
- Integrated gastric acidity was analyzed for each hour of the recording
%IA24hr after single or multiple administrations was calculated using the following method.
%IA24hr after single or multiple administrations (%) = [(Baseline – Day 1 or Day 7)/Baseline] ×100
Safety evaluation
Adverse events (AE) were monitored throughout the study. Safety evaluation was performed as follows: physical examination, monitoring of vital signs, 12-lead ECG, and laboratory tests including hematology, serum chemistry, and urinalysis. All AEs were collected using MedDRA® (Ver. 19.0) dictionary.
Statistical analyses
The PK and PD data were analyzed to compare the treatment groups. The primary PK parameter (AUCτ) and PD parameter (%IA24hr after multiple administrations) were log-transformed and analyzed by analysis of variance using a mixed-effects model. To compare the primary PK and PD parameters, point estimates and 90% confidence intervals (CI) for the geometric mean ratios (T/R) were also presented. Demographic characteristics were analyzed using the independent two sample t-test and chi-square test for comparison of two sequence groups (T-R and R-T). Safety data were presented using descriptive statistics. All statistical analyses were conducted using SAS statistical software version 9.3 (SAS Institute Inc. Cary, NC, USA) and Phoenix WinNonlin version 7.0 (Certara, Princeton, NJ, USA).
Results
Study participants
A total of 40 subjects were enrolled in this study and received at least one dose of study drugs. One subject withdrew from the study after completing the schedule of period 1 and was not included in the PK and PD analysis set. Two subjects completed all schedules in this study but were excluded from the PD analysis set because the missing rate for the pH monitoring measurements was more than 5%. All the subjects were men, and there were no significant differences in demographics between the two sequence groups (T–R and R–T) (Table 1).
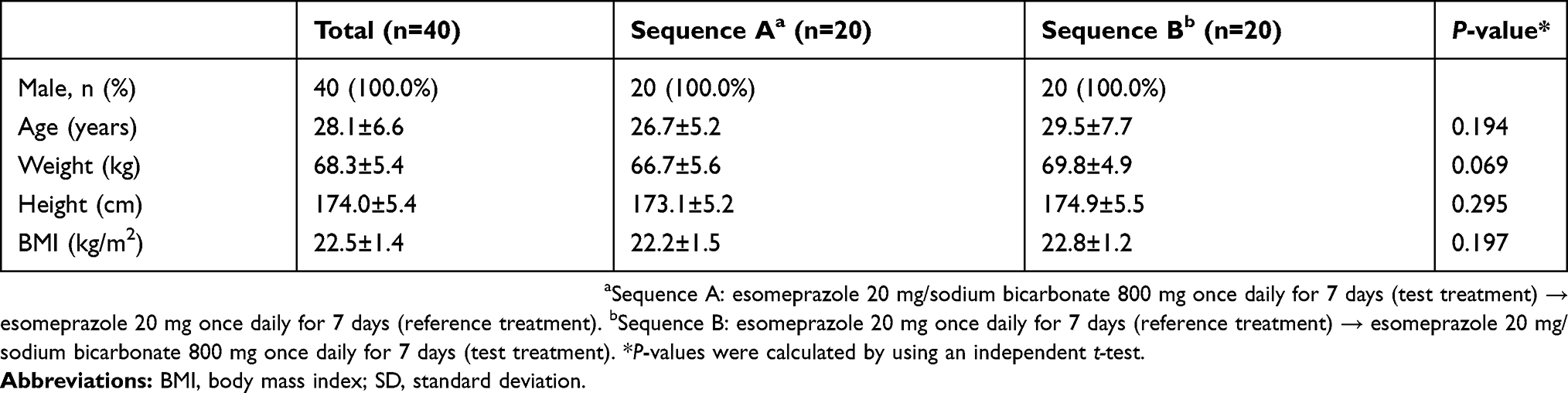 |
Table 1 Demographic characteristics of subjects |
Pharmacokinetics
The details of PK parameters of esomeprazole in each group are summarized in Table 2. After single or multiple administrations, the plasma concentration of esomeprazole in the test group showed a rapid increase, while those in the reference group increased gradually (Figure 1). Median Tmax of esomeprazole for the test group was shorter than that for the reference group upon both single and multiple administrations. The Tmax was 0.50 hr and 0.75 hr for the test group after single and multiple administrations, respectively, while the values were 1.50 and 1.25 hr for the reference group in each administration.
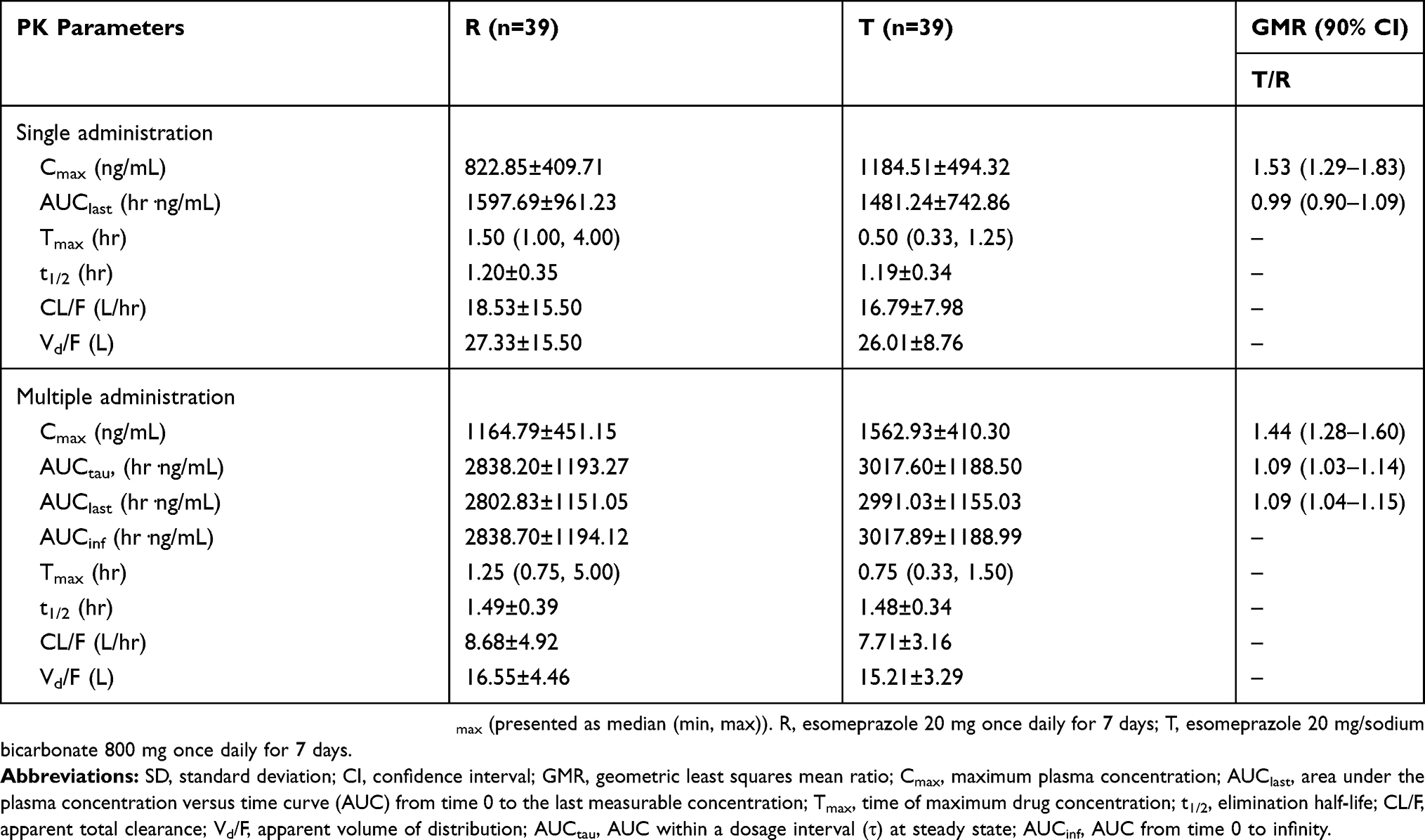 |
Table 2 PK parameters and comparison of esomeprazole after single and multiple administrations |
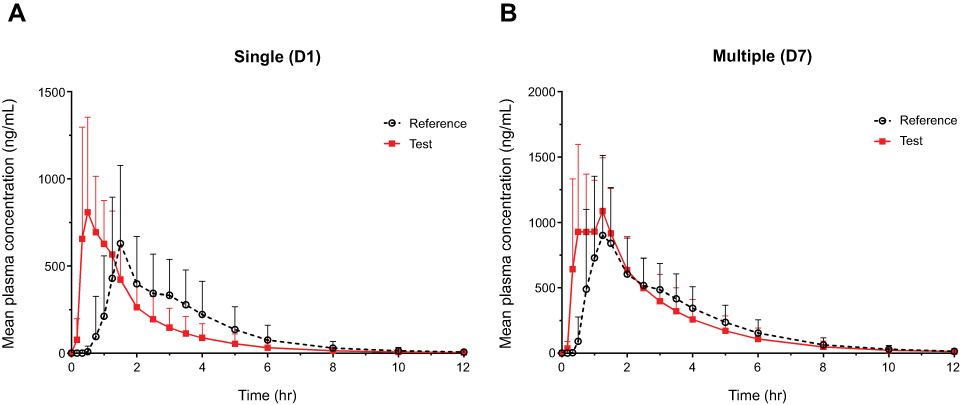 |
Figure 1 Mean plasma concentration-time profiles (A) after a single administration on day 1 and (B) after multiple administrations on day 7. Notes: The vertical bars represent SD. Reference, esomeprazole 20 mg once daily for 7 days. Test, esomeprazole 20 mg/sodium bicarbonate 800 mg once daily for 7 days. |
The Cmax of the test group demonstrated an approximately 1.53-fold and 1.44-fold increase as compared to that of the reference group after single and multiple administrations, respectively. However, the AUC of esomeprazole after single or multiple administrations was similar between the two formulations, and the t1/2, CL/F, and Vd/F of esomeprazole in the test group were similar to those of the reference group.
Pharmacodynamics
The intragastric pH over 24 hrs (median pH per 15 mins) at baseline, after single and multiple administrations is illustrated in Figure 2. Meal times and time of supine position are also indicated in Figure 2. The profiles of intragastric pH over 24 hrs for both single and multiple administrations were generally similar between the two treatment groups. The intragastric pH within 2 hrs (median pH per 1 min) after single and multiple administrations is shown in Figure 3. The first time to reach pH >4 after single and multiple administrations was about 55 and 27 mins in the test group, and 67 and 46 mins in the reference group, respectively.
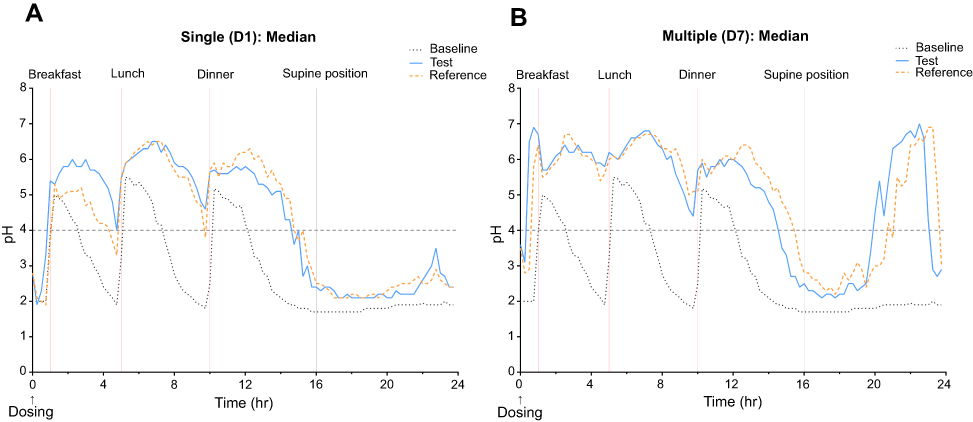 |
Figure 2 Median intragastric pH over a 24-hr interval with esomeprazole 20 mg/sodium bicarbonate 800 mg (test) or esomeprazole 20 mg (reference) at baseline, (A) after a single administration on day 1 and (B) after multiple administrations on day 7. Notes: Reference, esomeprazole 20 mg once daily for 7 days. Test, esomeprazole 20 mg/sodium bicarbonate 800 mg once daily for 7 days. |
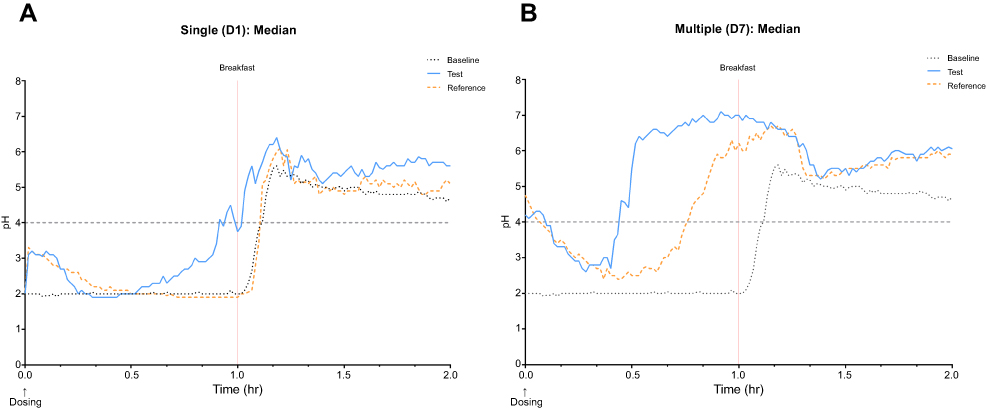 |
Figure 3 Median intragastric pH within 2 hrs with esomeprazole 20 mg/sodium bicarbonate 800 mg (test) or esomeprazole 20 mg (reference) at baseline, (A) after a single administration on day 1 and (B) after multiple administrations on day 7.Notes: Reference, esomeprazole 20 mg once daily for 7 days. Test, esomeprazole 20 mg/sodium bicarbonate 800 mg once daily for 7 days. |
The mean percentage times observed for gastric pH >4 at baseline, on Day 1 and Day 7 are presented in Figure 4. The mean (SD) percentage time for gastric pH >4 on Day 1 was 56.8% (22.8%) for test group compared with 55.5% (21.6%) for reference group (P=0.806). The mean (SD) percentage time for gastric pH >4 on Day 7 was 69.9% (15.9%) for the test group compared to 70.2% (16.6%) for reference group (P=0.951). The time to maintain pH >4 was similar between the two groups on both Day 1 and Day 7.
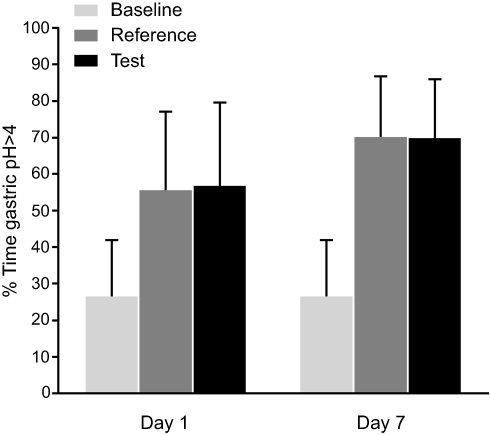 |
Figure 4 Mean percentage (%) of time with gastric pH >4 over a 24-hr period following treatment with esomeprazole 20 mg/sodium bicarbonate 800 mg (test) or esomeprazole 20 mg (reference) or at baseline.Notes: The vertical bars represent SD. Reference, esomeprazole 20 mg once daily for 7 days. Test, esomeprazole 20 mg/sodium bicarbonate 800 mg once daily for 7 days. |
The 24-hr integrated intragastric acidity and %IA24hr after single and multiple administrations are summarized in Table 3. The 24-hr integrated intragastric acidity decreased significantly from the baseline after administration of the study drugs. Mean %IA24hr in test group as compared to the baseline was similar to those of reference group after single or multiple administrations. The point estimates (with 90% CI) of the geometric mean ratios for %IA24hr after single and multiple administrations were 1.01 (0.93–1.09) and 1.00 (0.95–1.04), respectively.
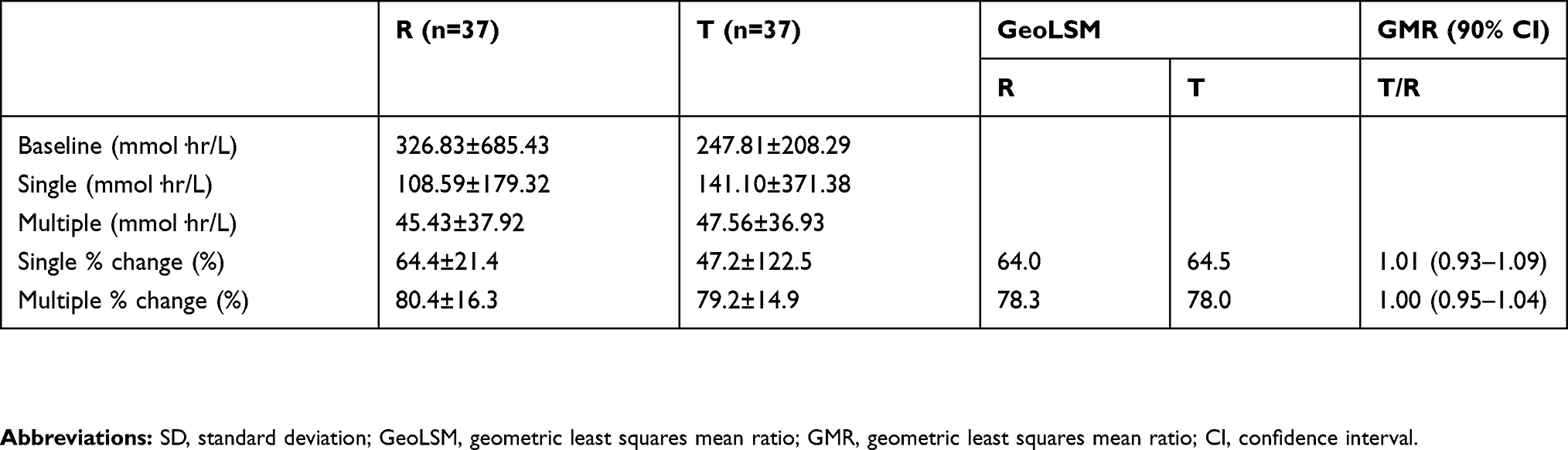 |
Table 3 Summary of 24-hr integrated gastric acidity and comparison of percent change from baseline in integrated gastric acidity over a 24-hr interval after single and multiple administrations |
Safety
There were no serious AEs observed during the study. Adverse drug reactions (ADR) occurred in seven subjects (10 cases) in the test group and two subjects (3 cases) in the reference group. The most common AEs were dyspepsia, pyrexia, and headache. All the AEs were mild, and all subjects recovered without any complications. During the study, there was no statistically significant difference in the frequency of ADRs between the test group and reference group (P=0.106). Furthermore, there were no clinically significant changes in physical examination, vital signs, ECG, or clinical laboratory results.
Discussion
This randomized, open-label, multiple-dose study compared the PK and PD of esomeprazole between IR-ESO and a tablet of enteric-coated esomeprazole 20 mg in healthy male subjects. In this study, the two drugs showed similar PK and PD profiles, indicating that the two drugs have a similar extent of absorption and acid inhibitory effects.
Esomeprazole, the S-isomer of omeprazole, is widely used for the treatment of acid-related disorders.7 In previous studies, esomeprazole showed more efficacy in maintaining the intragastric pH and exhibited greater inhibition of gastric acid secretion compared to omeprazole.15 To ensure its stability in the stomach, like other PPIs, esomeprazole was also developed to a delayed-release enteric coating formulation.16–18 However, the enteric-coated esomeprazole delayed the onset time of therapeutic effect due to delayed absorption.19 Therefore, IR-ESO was developed to overcome this limitation of delayed onset, to facilitate a rapid effect.
The first time to reach pH >4 after single and multiple administrations was faster in the IR-ESO group than in the enteric-coated esomeprazole group. The pH profiling within 2 hrs after each drug administration showed that pH increased abruptly after IR-ESO administration, but after the administration of enteric-coated esomeprazole, the pH was maintained around 2, and then increased after breakfast. This rapid pH increase by IR-ESO might be due to the immediate release of esomeprazole. In addition, sodium bicarbonate acts as a buffer to protect esomeprazole from gastric acid degradation, and it stimulates the temporary release of gastrin.20 The increase in gastrin levels allows parietal cells to absorb esomeprazole before degradation by the gastric acid.10 In addition, sodium bicarbonate acts as an antacid and rapidly neutralizes gastric acid and may provide faster symptomatic relief independent of accelerated esomeprazole effect. This IR esomeprazole formulation with sodium bicarbonate may have an advantage of relieving symptoms rapidly and efficiently in acid-related disorders.
Maintenance of intragastric pH above 4.0 has been considered a reliable surrogate marker for relieving the symptoms of acid-related disorders and healing GERD.21 The severity and frequency of heartburn or pain in GERD correlate with the duration of esophageal exposure to the refluxate with pH <4.0.22 However, the value of intragastric pH <4.0 is considered the same whether the pH is 3.9 or 1.0 for the same period of time, which is a major limitation in the identification of actual intragastric acidity.21 In order to overcome this, the integrated intragastric acidity has been used as a more precise method to assess the intragastric acid control.21 In this study, we measured both the mean percentage time for the intragastric pH >4.0 and integrated intragastric acidity for a 24-hr interval to evaluate the antacid effect. After treatment with IR-ESO, the mean percentage times observed with gastric pH >4.0 were about 56.8–69.9%, and percentage decrease in the 24-hr integrated intragastric acidity from baseline was about 64.4–80.4%. Both these parameters were similar to those in the group with administration of enteric-coated esomeprazole, suggesting that IR-ESO has a similar potency as enteric-coated esomeprazole to treat GERD.12
Zegerid approved by the FDA is similar to IR-ESO formulation of this study, since it contained sodium bicarbonate and immediate-release formulation of PPI.6 In a previous study to compare Zegerid and enteric-coated omeprazole, the Tmax for Zegerid was much lower than that of enteric-coated omeprazole (0.50 vs 1.38 hrs).20 Comparative symptom relief in patients with GERD showed that patients who consumed Zegerid demonstrated a remarkable and rapid symptom relief within 30 mins, while patients with treated with enteric-coated omeprazole did not show the same effect.20 These observations suggest that absorption of IR formulation PPI occurs rapidly due to the buffer effect of sodium bicarbonate and treatment also works rapidly because of the antacid effect of sodium bicarbonate in addition to accelerated effects of rapidly absorbed PPI.20 Based on these results, IR-ESO, which showed shorter Tmax than enteric-coated esomeprazole, is expected to cause faster symptomatic relief of GERD because of rapid absorption and increased antacid effects.
The Cmax values for IR-ESO were about 1.4- to 1.5-fold higher than those of enteric-coated esomeprazole; however, the AUC of esomeprazole was similar between the two groups. As observed in a previous study, wherein the AUC of esomeprazole predicts the efficacy of acid inhibition more precisely, the acid inhibitory effect of IR-ESO was comparable to that of enteric-coated esomeprazole, similar to the results of AUC.23 There are safety concerns of IR-ESO resulting from higher Cmax values than those of enteric-coated esomeprazole. However, the frequency or severity of ADR was similar between the two groups, and the ADRs were not clinically significant. On the basis of these results, IR-ESO is considered to be safe irrespective of higher plasma peak concentration.
Despite these findings, this study has several limitations. First, it included only healthy adult male subjects, and the results cannot be generalized for patients with GERD. However, the main objective of this study was to compare the PK/PD of esomeprazole between the two drugs, and it is important to control any factors that may affect the PK/PD such as concomitant medication, disease status, lifestyles, and so on. Therefore, it was reasonable to conduct the study only in healthy subjects for controlling these factors strictly. In the future, further studies in patients with acid-related disorders might be needed to evaluate the acid inhibitory effect and clinical efficacy by observation of symptom control or rate of healing of IR-ESO. Second, the serum gastrin concentrations were not analyzed in this study. Since the serum gastrin level can be elevated depending on the degree of acid inhibition, there is a good correlation between serum gastrin and gastric acid suppression.23 However, in this study, 24-hr pH monitoring and 24-hr integrated intragastric acidity monitoring were considered sufficient to evaluate the degree of acid inhibition.
Conclusion
Results from the present study suggested that IR-ESO showed similar PK/PD profiles as enteric-coated esomeprazole in healthy male adults. Furthermore, this study demonstrates that IR-ESO exhibited a faster onset compared with enteric-coated esomeprazole, such that median Tmax and the initial time to reach pH >4 were shorter. During the course of the study, IR-ESO and enteric-coated esomeprazole were well tolerated and safe. All ADRs were mild and recovered without any complications. As the study population was limited to healthy male Korean population, further studies are required to evaluate whether there is a difference of PK/PD profiles of IR-ESO between both gender, a wider age range and patient with acid-related disorders.
Data availability
The raw data of this study will not be shared because of confidentiality.
Acknowledgments
We would like to thank the staff at Severance Hospital Clinical Trials Center for assistance for conducting this study. This study was sponsored by Chong Kun Dang Pharmaceutical Corp., Seoul, Korea, and supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C1913).
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Shin Jung Park is a full-time employee of Chong Kun Dang Pharmaceutical Corp. The authors report no other conflicts of interest in this work.
References
1. Joelsson B, Johnsson F. Heartburn–the acid test. Gut. 1989;30(11):1523–1525. doi:10.1136/gut.30.11.1523
2. Miner P. Relief of symptoms in gastric acid‐related diseases–correlation with acid suppression in rabeprazole treatment. Aliment Pharmacol Ther. 2004;20:20–29. doi:10.1111/j.1365-2036.2004.02162.x
3. Huang J-Q, Hunt RH. pH, healing rate, and symptom relief in patients with GERD. Yale J Biol Med. 1999;72(2–3):181.
4. Vanderhoff BT, Tahboub RM. Proton pump inhibitors: an update. Am Fam Physician. 2002;66(2):273–280.
5. Castell DO, Kahrilas PJ, Richter JE, et al. Esomeprazole (40 mg) compared with lansoprazole (30 mg) in the treatment of erosive esophagitis. Am J Gastroenterol. 2002;97(3):575. doi:10.1111/j.1572-0241.2002.05560.x
6. Castell D. Review of immediate-release omeprazole for the treatment of gastric acid-related disorders. Expert Opin Pharmacother. 2005;6(14):2501–2510. doi:10.1517/14656566.6.14.2501
7. Shi S, Klotz U. Proton pump inhibitors: an update of their clinical use and pharmacokinetics. Eur J Clin Pharmacol. 2008;64(10):935–951. doi:10.1007/s00228-008-0538-y
8. Horn J, Howden C. Review article: similarities and differences among delayed-release proton-pump inhibitor formulations. Aliment Pharmacol Ther. 2005;22:20–24. doi:10.1111/apt.2005.22.issue-s3
9. Small RE. Advances in proton pump inhibitor therapy: an immediate-release formulation of omeprazole. Pharmacol Ther. 2005;30:698–715.
10. Howden C. immediate‐release proton‐pump inhibitor therapy–potential advantages. Aliment Pharmacol Ther. 2005;22:25–30. doi:10.1111/j.1365-2036.2005.02709.x
11. McQuaid KR, Laine L. Early heartburn relief with proton pump inhibitors: a systematic review and meta-analysis of clinical trials. Clin Gastroenterol Hepatol. 2005;3(6):553–563.
12. Richter JE, Kahrilas PJ, Johanson J, et al. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am J Gastroenterol. 2001;96(3):656–665. doi:10.1111/j.1572-0241.2001.3600_b.x
13. Abdel-Hamid H. Modified PPIs (a search for the better). Al-Azhar Assiut Med J. 2016;14(1):8. doi:10.4103/1687-1693.180455
14. Gardner J, Perdomo C, Sloan S, et al. Integrated acidity and rabeprazole pharmacology. Aliment Pharmacol Ther. 2002;16(3):455–464. doi:10.1046/j.1365-2036.2002.01158.x
15. Lind T, Rydberg L, Kylebäck A, et al. Esomeprazole provides improved acid control vs. omeprazole In patients with symptoms of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2000;14(7):861–867. doi:10.1046/j.1365-2036.2000.00813.x
16. Missaghi S, Young C, Fegely K, Rajabi-Siahboomi AR. Delayed release film coating applications on oral solid dosage forms of proton pump inhibitors: case studies. Drug Dev Ind Pharm. 2010;36(2):180–189. doi:10.3109/03639040903468811
17. Röhss K, Lind T, Wilder-Smith C. Esomeprazole 40 mg provides more effective intragastric acid control than lansoprazole 30 mg, omeprazole 20 mg, pantoprazole 40 mg and rabeprazole 20 mg in patients with gastro-oesophageal reflux symptoms. Eur J Clin Pharmacol. 2004;60(8):531–539. doi:10.1007/s00228-004-0804-6
18. Miner P
19. Benetti C, Flammini L, Vivo V, et al. Esomeprazole immediate release tablets: gastric mucosa ex vivo permeation, absorption and antisecretory activity in conscious rats. J Control Release. 2016;239:203–210. doi:10.1016/j.jconrel.2016.08.032
20. Walker D, Shing RNK, Jones D, Gruss H-J, Reguła J. Challenges of correlating pH change with relief of clinical symptoms in gastro esophageal reflux disease: a phase III, randomized study of Zegerid versus Losec. PLoS One. 2015;10(2):e0116308. doi:10.1371/journal.pone.0116308
21. Tutuian R, Castell D, Xue S, Katz P. The acidity index: a simple approach to the measurement of gastric acidity. Aliment Pharmacol Ther. 2004;19(4):443–448. doi:10.1111/apt.2004.19.issue-4
22. Hunt RH. Importance of pH control in the management of GERD. Arch Intern Med. 1999;159(7):649–657.
23. Robinson M. current perspectives on hypergastrinaemia and enterochromaffin-like-cell hyperplasia. Aliment Pharmacol Ther. 1999;13:5–10. doi:10.1046/j.1365-2036.1999.00033.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.