")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 15
The Effect of School-Linked Module-Based Friendly-Health Education on Adolescents’ Sexual and Reproductive Health Knowledge, Guji Zone, Ethiopia - Cluster Randomized Controlled Trial
Authors Boku GG, Garoma Abeya S, Ayers N, Abera Wordofa M
Received 9 November 2023
Accepted for publication 16 January 2024
Published 23 January 2024 Volume 2024:15 Pages 5—18
DOI https://doi.org/10.2147/AHMT.S441957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gobena Godana Boku,1,2 Sileshi Garoma Abeya,2,3 Nicola Ayers,4 Muluembet Abera Wordofa5
1Population and Family Health Department, Faculty of Public Health, Jimma University, Jimma, Oromia, Ethiopia; 2Medical Services Lead Executive Office, Federal Ministry of Health, Addis Ababa, Ethiopia; 3Public Health Department, Adama Hospital Medical College, Adama, Oromia, Ethiopia; 4School of Nursing, BPP University, London, UK; 5Population & Family Health Department Faculty of Public Health, Jimma University, Jimma, Ethiopia
Correspondence: Gobena Godana Boku, Medical Services Lead Executive Office, MoHE, P.O. Box 1234, Addis Ababa, Ethiopia, Tel +251911545441, Email [email protected]
Background: Although access to sexual and reproductive health information is the right and a critical component of health policy, it is not well addressed in pastoral communities. This study assessed the effect of School-Lined Module-based friendly health education on adolescents’ sexual and reproductive health knowledge in the pastoral community of Guji Zone, Ethiopia.
Methods: A two-arm cluster Randomized control trial study with pre-post evaluation was conducted among interventions (n=375) compared with control (n=384) in Gorodola and Wadara high schools. Comparing an intervention to a control group, pre-posttests, and post-posttests were used to evaluate the effectiveness of the intervention. The data was collected using 25 Self-administered questionnaires and analyzed using paired-sample independent t-tests and linear regressions to study the relationship between the outcome and independent variables.
Results: We collected the data from 759 adolescents among 15 intervention and 15 control clusters. The results have shown that as compared to control arms, the mean sexual and reproductive health Knowledge score was significant higher in the intervention clusters (375) 73.3%, vs (384) 66.5%%, p< 0.001, 95% CI, (0.05395– 0.08347). Information (β: 0.038, 95% CI: 0.028– 0.052), confidence (β: 0.045, 95% CI: 0.033– 0.057), knowledge (β: 0.05, 95% CI: 0.035– 0.066), and compassionate care (β: 0.107, 95% CI: 0.092– 0.122) were significantly associated with SRH knowledge prediction. The proportion of SRH knowledge increased from 168(44%) baseline to 244(65%) end line in the intervention versus 235(60% to 238(62%) in control arms.
Conclusion: The execution of school-linked module-based friendly health education has proved to have a significant effect on mean SRH knowledge. Individual-level and behavioral-level factors significantly explain variability in enhancing SRH knowledge in the pastoral community. We recommend scaling up the School-Linked Module-based friendly health education intervention.
Trial Registration: We registered clinical trial PACTR202107905622610 on 16 July 2021.
Keywords: adolescent, SRH knowledge, education, intervention, pastoral community
Introduction
Modern scientific evidence broadly supports the view that a friendly health education intervention program is indispensable for enhancing adolescents’ sexual and reproductive health knowledge to make informed decisions and promote sexual and reproductive health (SRH) services utilization through interactive learning.1–3 Module-based friendly health education is a multidimensional construct that involves an instructional unit within a designed trial curriculum, usually organized by chronology, topic, or theme. The module has a title and includes questions, discussions, assignments, and quizzes. We designed the module to enable adolescent students to deal effectively with demands and challenges and make informed decisions. It provides strengths and capabilities that help adolescents develop a positive attitude and handle issues effectively with confidence.4,5
Various studies have proven the effectiveness of implementing Sexual and reproductive health education intervention programs in general education.6,7 However, SRH education is far from institutionalized in most developing countries. Early adolescents in sub-Saharan African countries were sexually active, although their RH knowledge is deficient. For instance, only about 24.5% of in-school adolescents have comprehensive HIV/AIDS knowledge.8 In contradiction to this finding, 88% of Mekelle High School students were highly knowledgeable about various family planning methods.9 In Ethiopia, the perception of being at risk of acquiring HIV is only about 21.6% to 24.5% of in-school adolescents and females less likely to have comprehensive knowledge.8,10,11
Poor access to SRH knowledge had a significant cause of poor self-confidence among adolescents.12 In line with this, in north India, the awareness of contraceptive health services was considerably less in rural adolescents 33.5%.13 Significant efforts have been undertaken in Ethiopia to increase ASRH expertise. However, high child marriage and adolescent childbearing rates persist in rural areas, particularly in the pastoral community. However, reaching rural adolescents with SRH information-relevant services remains a significant challenge in Ethiopia.14 School-linked and school-based sexual and reproductive health education and life skills intervention programs have shown positive effects in contributing to an improvement in SRH knowledge and skills.14–16 Moreover, school-based sexual and reproductive health education trial studies and a systematic review and meta-analysis on school-based sexual health education interventions in Ethiopia and Sub-Saharan Africa showed significant effectiveness on SRH knowledge outcome among school students compared to the control groups.2,17,18
Evidence from high schools in Ethiopia showed that about 35% to 59.6% of adolescents knew about SRH issues. It indicated that higher-level grade students had more SRH knowledge than low-level students,19–21 Continued provision of RH information has increased SRH knowledge. Thus, Knowledgeable adolescents have developed strong self-efficacy and are assertive toward sexuality. Self-efficacy and SRH knowledge are directly associated, and the effect has contributed significantly to healthy sexual behaviors.22,23 Attractive AFSRH services provided by compassionate providers positively affect SRH knowledge.24
Continuous provision of Comprehensive SRH information for adolescents has lifelong protective benefits.25 However, the health system must disseminate complete and timely information.26 Moreover, broad inequities in accessing quality SRH services and information have continued as challenges.27 The National Youth Policy of Ethiopia has stated that favorable conditions could create proper access to information and counseling on RH issues. Moreover, Increasing access to Adolescent health information and age-appropriate Sexual Education is one of the national priority areas of action.28 Providing SRH educational intervention has successfully improved SRH knowledge among adolescent students.29
Since module-based friendly health education intervention programs are essential for adolescents’ development, a school-linked module-based friendly health education was designed and implemented within trials clustered high school sections. It helps adolescents to be more logical and plan choices sexually so that there are fewer unintended pregnancies, rarer sexually transmitted diseases, and stronger interactions.30 The school-linked friendly health education program (MBFHE) approach enhances SRH knowledge in pastoral communities. It also helps adolescents acquire essential life skills to deal with and develop positive attitudes toward School-linked FHS. Almost all adolescents have access to high schools; hence, we were used to implementing the school-linked module-based friendly health education intervention in thirty clusters of high school sections. This study intends to assess the effect of a School-Linked module-based friendly health education on SRH knowledge in the pastoral community of the Guji zone.
Methods and Materials
Study Areas and Participants
We conducted this research in two pastoral communities in the east Guji Zone. East Guji Zone is one of the Oromia Regional state of Ethiopia, located in the southern part of the region. As per the CSA 2007 Population Projection report, the adolescent population for 2021 is 132,882.31 Participants were high school adolescent students (aged 14–19) recruited from Gorodola and Wadara district high schools. The school sessions were selected based on adolescents’ demographic characteristics and distance from one another. The parents and adolescents were clarified on the research goal and provided informed consent before participating in the intervention. Lastly, four high schools were categorized into 15 clusters for each trial, and control arms participated in the study. The source population is middle and late-aged adolescents (ages 14–16 and 17–19, respectively) enrolled in randomly selected schools. The investigation was conducted from November 2020 to May 2021 (see Figure 1).
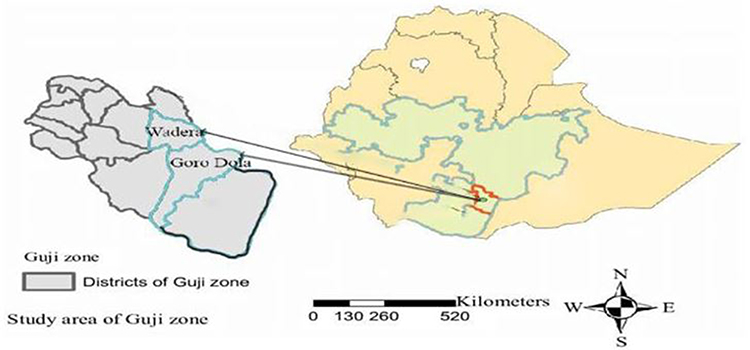 |
Figure 1 Study areas map of school-linked life skills interventional study in East Guji Zone, Oromia, south Ethiopia November 2020–May 2021. |
Study Design
A pre-post-test study design was used in a school-linked cluster-randomized controlled trial investigation to evaluate the effect of school-linked module-based friendly health education on adolescents’ sexual and reproductive health knowledge.
Sampling Size Determination
We determined the sample size according to randomized controlled trials that recommended paired equal-sized clusters for each trial and control cluster.32,33 We have categorized 30 clusters, each with 15 cluster sessions for trial and control arms (95% CI, power 90%),32–34 (Barais et al, 2018).32 We calculate the observations per cluster session using a two-sample proportion comparison. We compare the number of observations per cluster session using a two-sample proportion. “We calculated the sample size for the school-linked cluster-randomized controlled trial investigation”. After determining the grade margin of the study units, we have chosen the sample units and respondents.
We calculated the sample size using stata12 software and 179 for each treatment and control arm. Assumption 2 as the design effect and 10% as the respondent rate.35,36 The middling cluster size required was 30 for a sample size of 788 adolescent students (half for intervention and control). The research sample units were (Grades 9–12) (see Figure 2).
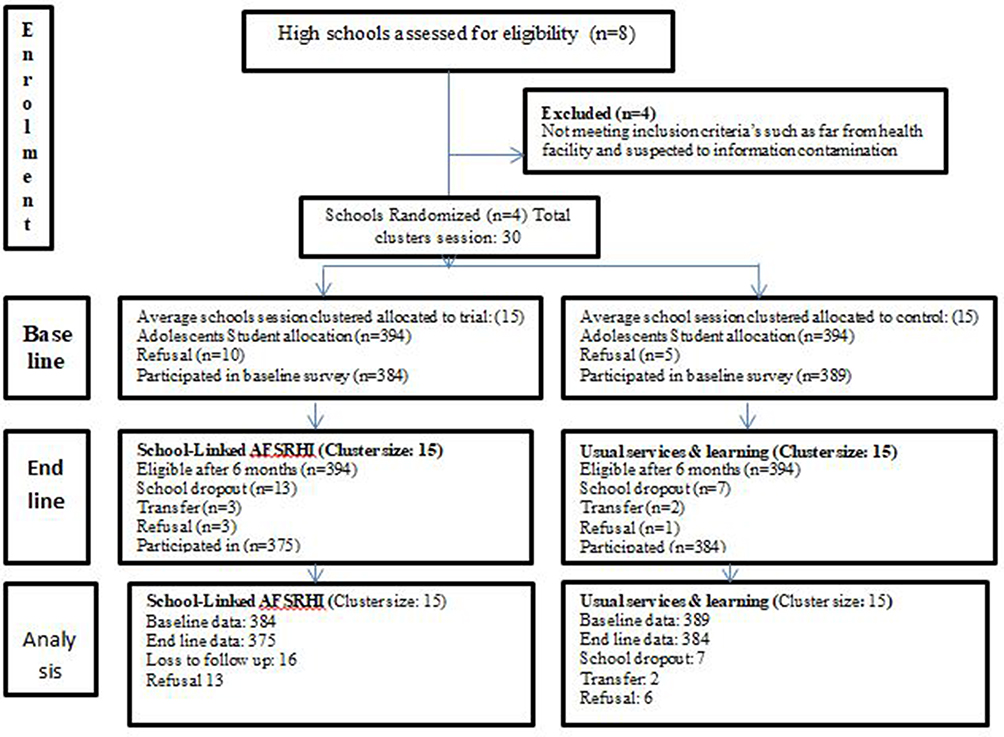 |
Figure 2 School-linked sexual and reproductive health interventional study clustering sampling process in the east Guji zone, Ethiopia. November 2020 to May 2021 (n=1532). |
Sampling Procedures and Randomization
We designated Gorodola and Wadara districts among the pastoral districts of the East Guji Zone. The districts were selected as both districts had yet to receive an experimental study to increase adolescents’ SRH knowledge. We used high school sessions as cluster randomization units among selected districts and performed personal randomization among all school sections. We randomly assigned sample sizes to each intervention and control cluster in a 1:1 analogous ratio.37
Eligibility
The study participants were adolescent students aged (14.15,16,17,18,19), who enrolled in high schools within randomized districts. We excluded adolescent students newly enrolled in nominated high schools for less than 6 months from the study. Exclusion criteria: We used Exclusion criteria to identify participants who should not participate in the study. In this case, we excluded the newly enrolled students from the study. This exclusion may be due to ensuring that the students have had enough time to adjust to their new school environment before being included in the study.
Double Blinding
We ensured that adolescent students did not know whether they were in intervention clusters or control. We ensured that trainers were aware of the intervention package but did not know if other schools had included it in the program as an intervention or control. Likewise, data collectors did not know which groups were receiving the intervention or the availability of control clusters.
Descriptions of Intervention
Intervention Cluster- I
To facilitate adolescents’ module-based friendly health education, we collected facility-based baseline data to identify the status of adolescents’ SRH knowledge and categorize factors that predict adolescents’ SRH knowledge. The school-linked Module-based friendly health education program addresses the identified gaps and factors that enhance SRH knowledge. Almost all adolescents had received school-linked Module-based friendly-health education program packages provided at two platforms: school-linked module-based friendly health Education and reproductive health club. The trial group participated in a school-linked module-based friendly-health education program that included 96 sessions, each lasting 30 minutes (total of 28.8 hours). The intervention targeted four categories of primary outcomes of friendly health education: the nature of adolescents, sexual education, understanding gender, gender equality and equity, and adolescents’ sexual and reproductive health problems. All adolescents in the intervention schools have attended the 40-minute sessions 4 times a month for six consecutive months (see Table 1).
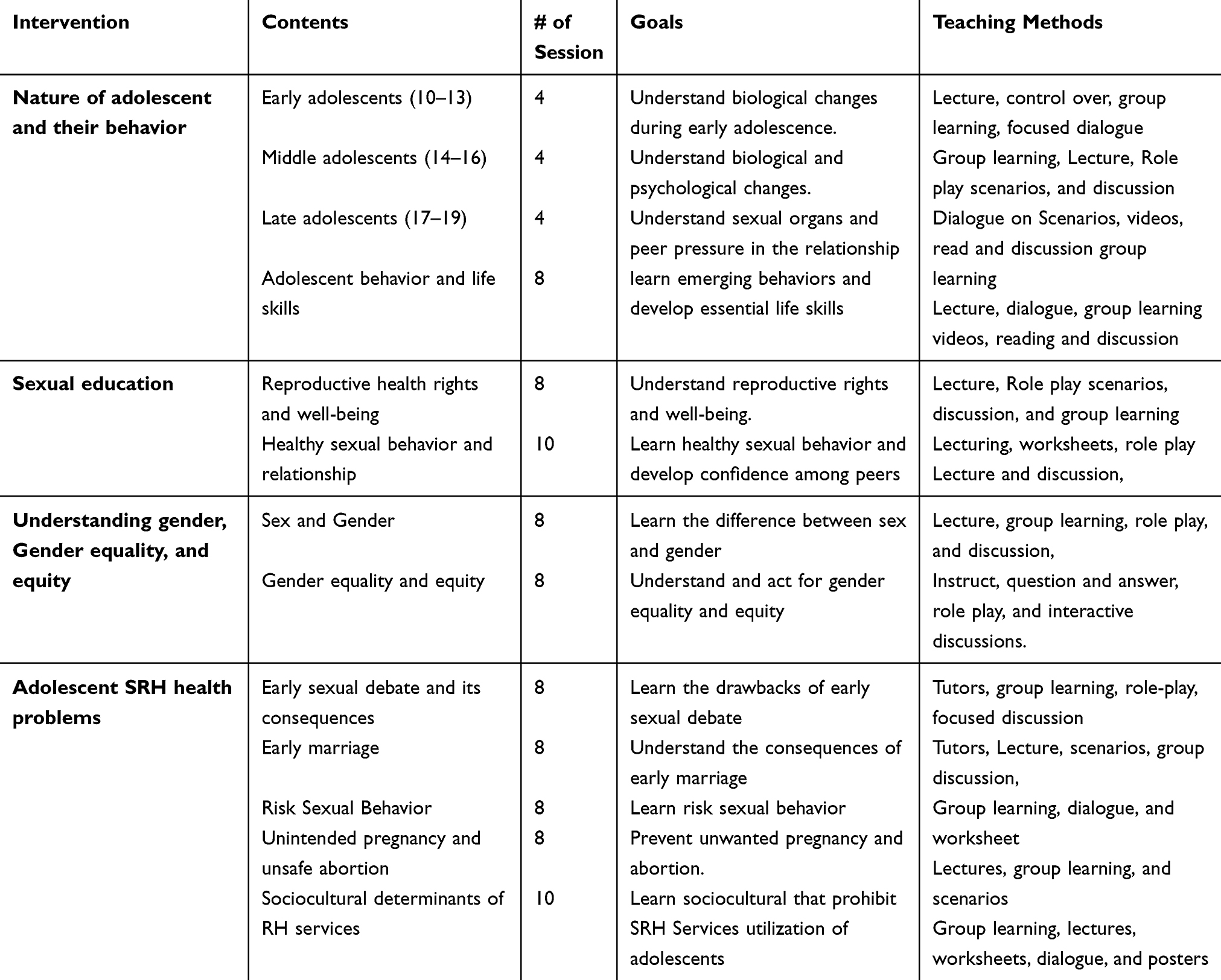 |
Table 1 Descriptions of a School-Linked Module-Based Friendly Health Education Program for Adolescents Among Trial Schools in Gorodola District, Guji Zone, Ethiopia, November 2020 to May 2021 |
Control Arm II
Adolescents in control groups have not received any intervention packages and have not participated in any school-linked module-based friendly-health education program. Moreover, we had not discussed selected module-based, friendly health education topics in the school reproductive health club.
Intervention Process
We followed a detailed outline and a systematic approach to develop the experimental trial’s intervention package. We created guidance tools and training manuals for health service providers and school officers. We have provided orientation for health and school officers and detailed training for health workers, data collectors, and supervisors. We started the experimental study after performing the pretest in both study arms. The intervention was launched in November 2020 and ended in May 2021.
Tools and Techniques
We used a pretested, structured questionnaires to collect the data. We developed the tools after reviewing relevant literature.25,38,39 We translated the English version of the questionnaire into Oromiffa, the language of the study area. The Oromiffa version of the questionnaire was printed and distributed to data collectors. We used similar questionnaires to collect data and conduct face-to-face interviews on baseline and end-line studies. This study has used Bandura’s social cognitive theory model as a guiding framework. The theory has conceptualized the cognitive appraisals in terms of triadic, reciprocal, and asymmetric influences among the environment, person, and behavior.40,41 We used this framework to postulate that the intervention has influenced adolescent knowledge through direct and indirect cognitive processes that are supposed to improve SRH knowledge. The assumption was to present the intended intervention among the study group to produce an outcome of interest through triadic, reciprocal, and asymmetric relationships between the personal, environmental, and behavioral factors42,43 (see Figure 3).
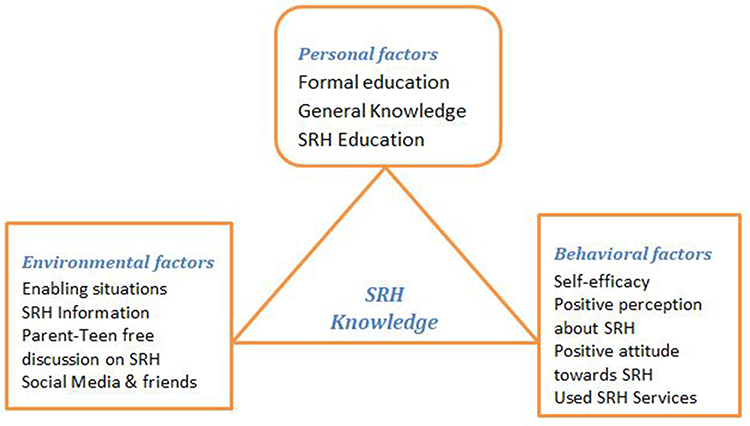 |
Figure 3 School-linked module-based friendly health education Social cognitive theory framework adopted from Bandura (2014). High school adolescents of Guji Zone, South Ethiopia, February 2022. |
Variables and Measurement
This experimental study aimed to determine the effect of school-linked module-based friendly health education on improving adolescents’ SRH knowledge. We compared the SRH knowledge between the trials and control clusters on the end-line survey. Likewise, factors that enhance SRH knowledge were studied. We identified SRH knowledge as the outcome variable and categorized the independent variables as personal, behavioral, and environmental-level factors while taking the school’s section as a cluster variable. Hence, the five SRH knowledge cognitive mediators used were information, knowledge, enabling situations, perceptions, and self-efficacy. We analyzed and measured the cognitive variables influencing behavior changes in adolescents’ SRH knowledge.
We used 25 items to measure appropriate SRH knowledge in this study. Agree/one had appropriate information, knowledge, enabling situations, perceptions, and self-efficacy, and disagree/zero if not. The level of SRH knowledge was categorized using mean scores; thus, a knowledge score above the mean is termed appropriate SRH knowledge.42
Data Management and Analysis
We entered the data into Epidata software version 3.1 and analyzed it using SPSS version 23.0. We checked the data for any missed values and outliers. We employed the mean, proportion, and standard deviations to describe descriptive data. We removed the items based on factor loading criteria. We used the chi-square association test to compare the status of SRH knowledge between the trial and control groups. The bivariate analysis identified factors enhancing SRH knowledge to test the correlation between each independent variable and the variables of interest. This study employed an independent sample Student’s t-test.44,45
To test the model’s fitness for the multi-level model, the researchers used the log-likelihood ratio (LR) test. The first model was used to determine the effect of cluster variation on SRH knowledge. We conducted the second model for individual factors, the third for behavioral factors, and the fourth for environmental factors. We examined the linear regression model’s assumptions (normality, independence, homoscedasticity, and multicollinearity). We utilized a backward stepwise linear regression model that included all significant independent variables at p<0.05 and (95% CI). In the study, we performed a bivariate analysis first to explore the relationship between variables. In the second, third, and fourth models, we included only the variables with p-values less than 0.25. However, the final model only included variables with p <0.05. We compared the mean difference in adolescents’ SRH knowledge between the intervention and control groups using paired sample independent t-tests.44,46
We compared the mean difference in adolescents’ SRH knowledge between the intervention and control groups using paired sample independent t-tests.43–45 We used factor analysis and reliability tests to check the internal consistency of the data and model fitness.45,46
Results
Socio-Demographic Characteristics
Baseline
773 (98%) adolescents aged 14 to 19 were recruited from 4 high schools and 30 clusters in the pastoral districts of Gorodola and Wadara. 384 (49.7%) were from intervention clusters, whereas 389 (50.3%) were from control clusters. The mean age in the trial arms was 17.34 (SD = 1.37), compared to 17.26 (SD = 1.3) in the control group. The mean learning level of participants in the trial arm was 10.2 (SD 1.269), compared to 10.68 (SD = 0.75) in the control arm (Table 2).
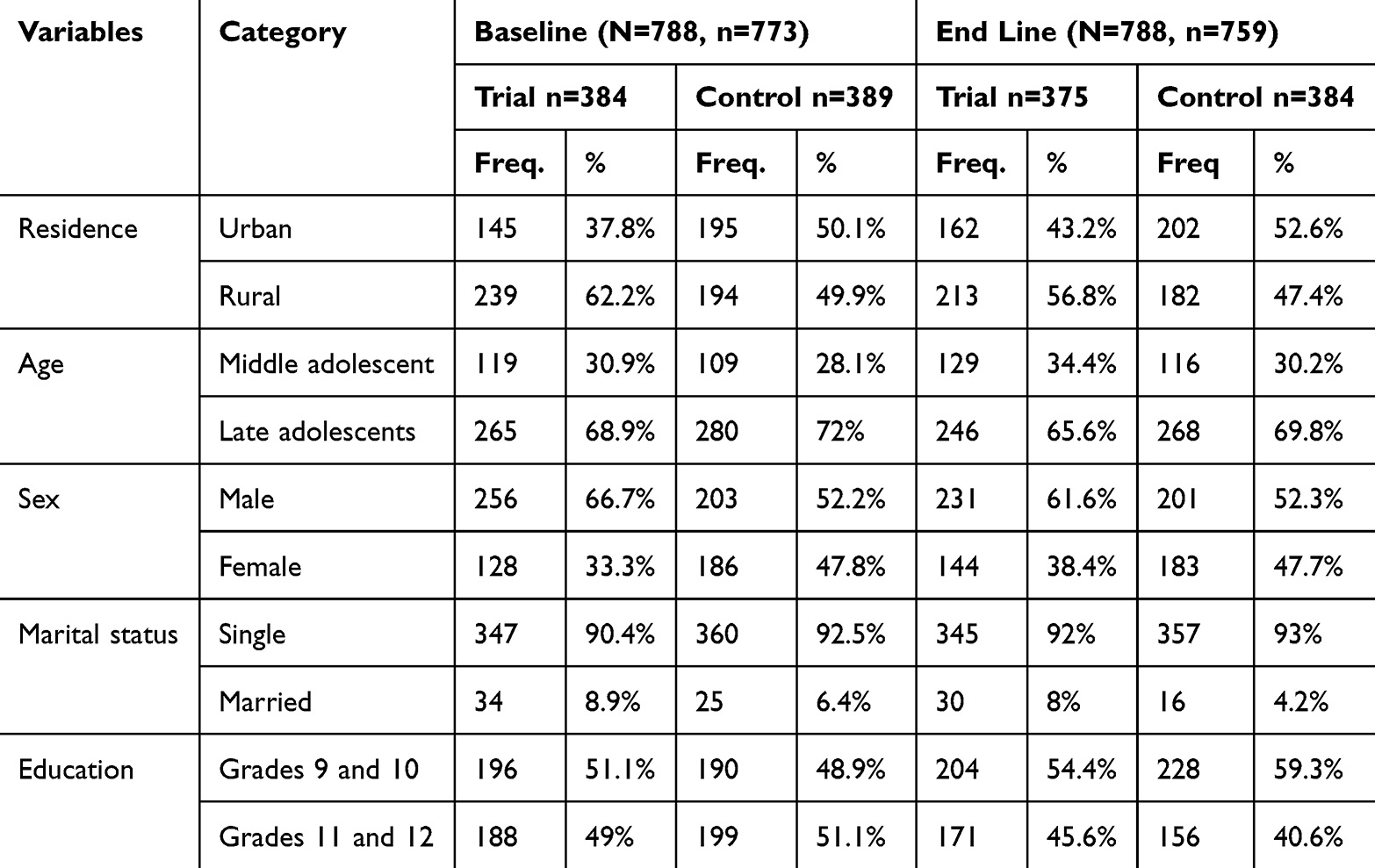 |
Table 2 Socio-Demographic Characteristics of Research Participants Disaggregated by Baseline and End Line, Trial and Control Clusters, East Guji Zone, Oromia, Ethiopia, November 2020 to May 2021, (n=1532) |
End Line
We obtained Data from 759 (93.3%) adolescents among 30 school sections in similar pastoral districts. 375 (47.58%) came from intervention clusters, whereas 384 (48.73%) came from control clusters. The mean age in the experimental group was 17.26 (SD = 1.511), compared to 17.28 (SD = 1.398) in the control group. The mean learning level of the trial was 9.93 (SD 0.997), compared to 10.08 (SD 0.933) in the control arms (Table 2).
Comparison of Two Populations’ Mean
The outcomes of the independent t-test showed that the mean (SRH) Knowledge among adolescent students recruited as the intervention group (M = 0.7316, SD = 0.10845, N = 375) was significantly different from the control group (M = 0.6629, SD = 0.09855, N = 384), t (9.139), p<0.001. As a result, we rejected the null hypothesis at a 95% CI for the difference between the two population means, employing a t-test distribution with 383 degrees of freedom at a 95% confidence interval (0.02907, 0.07457).
Status of Adolescents’ SRH Knowledge
Baseline
The baseline survey findings showed that the proportion of adolescents with SRH knowledge was 168 (44%) among the intervention and 235 (60.4%) among the control clusters. The mean scores of SRH knowledge were (0.4416) among the experimental arms and (0.4926) among control clusters at P<0.001; 95% CI= (−0.07377 to −0.0283), with negative mean diff. −0.051) (Table 3).
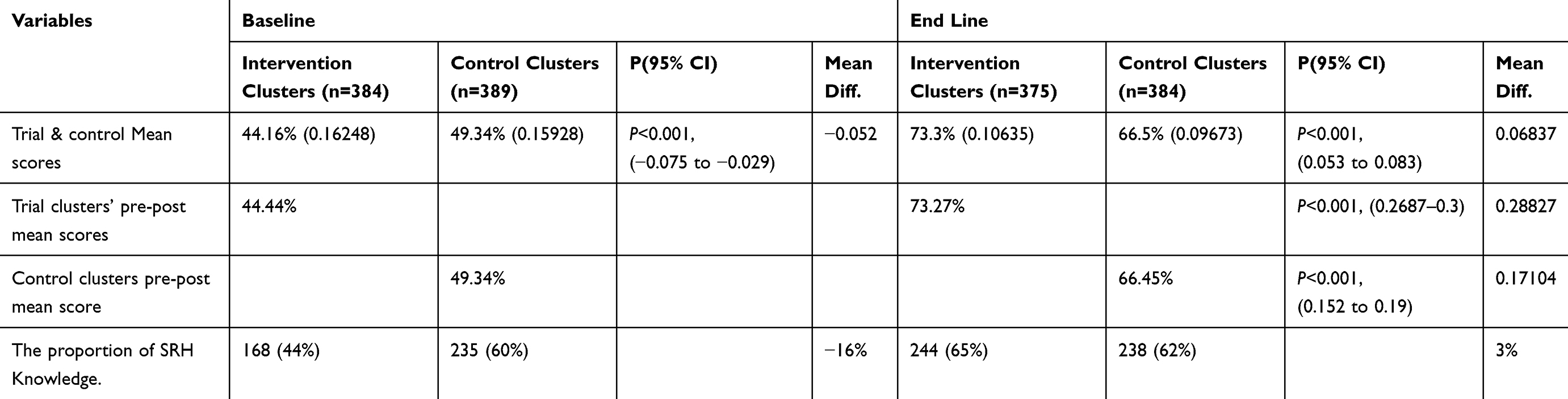 |
Table 3 Mean Scores, Proportion, Standard Deviations, and Comparison of SRH Knowledge Among High School Adolescents, East Guji Zone, Oromia, Ethiopia, February 2022 |
End Line
The end line findings showed that the proportion of adolescents’ SRH knowledge was 244 (65.1%) among the intervention and 238 (62%) among the control clusters. However, after the trial, the mean SRH knowledge scores showed that the test group had more progressive scores than the control arm with a statistically significant difference (73.16%) (66.29%) among the control clusters at P<0.001; 95% CI=0.054 to 0.083, with positive mean diff. = 0.0687) (Table 3).
Effect of the Intervention
Effectiveness of School-Linked Module-Based Friendly Health Education Intervention Program on Improves SRH Knowledge: A paired sample independent t-test analysis revealed a statistically significant mean difference in SRH Knowledge improvement over time between the intervention and control arms (6.87%, 95% CI (0.05395 to 0.08347, P<0.001). Compared to the control clusters, the mean scores of adolescents with improved SRH knowledge were significantly higher in the intervention clusters 375(73.16%) vs 384(66.29%) p<0.001) (see Figure 4).
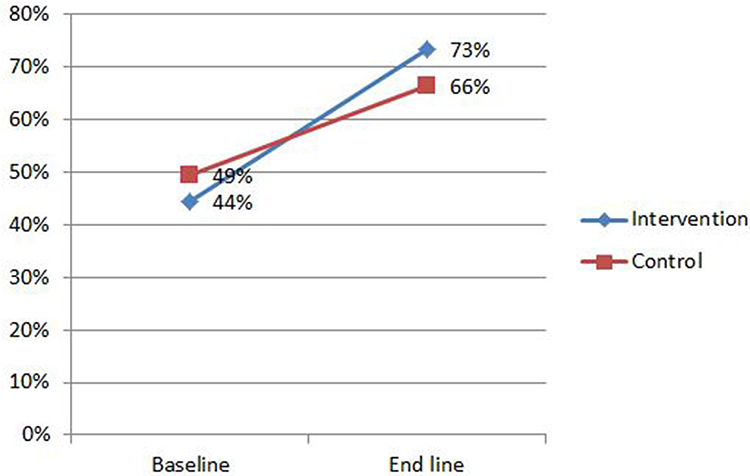 |
Figure 4 Line Graph compares mean scores of SRH knowledge at baseline and end line among control and intervention arms in high school adolescents, East Guji Zone, Ethiopia, February 2022. |
Factors Contributing to SRH Knowledge Improvement
The results from Multiple linear regressions models analysis revealed that, of the personal level factors, communicated on AFSRH information and know FHS provided at nearby health facility were significant, (model 2), among the behavioral-level factors, confident enough to make safe and informed decisions, believed health care providers are respecting right and need-based FHS choice, right to utilize friendly health Services, when you had several options from which to choose, I believe Healthcare providers have properly kept my secrets, ever utilized SRH Services, having sexual relationship with many girl/boy have no risks, assertiveness is respecting your right by aggression and utilized SRH services at pocketed private health facilities were significant (model 3), and environmental-level factors, information of health facility provided FHS, freely discuss about SRH issues, my parents are comfortable with right and need base AFHS utilization and well informed about friendly Health services were significant (model 4). However, only two factors at the personal level and three factors at the behavioral level became significant in the final model to predict SRH Knowledge.
Adolescents who received communication on SRH information demonstrated significant progress in mean proper SRH knowledge scores compared to the control arm, with an unstandardized coefficient (β) of 0.038, 95% CI, 0.028–0.052, surpassing those in the control clusters. Adolescents in the experimental clusters (β: 0.045, 95% CI: 0.033–0.057) were predicted to be more confident in making safe and informed decisions than those in the control clusters. Adolescents in the intervention clusters were more predicted to possess mean SRH knowledge (β: 0.05, 95% CI: 0.035–0.066) than those in the control cluster. Likewise, the control group has also registered significant increments. The study displayed that adolescents in the trial clusters who received compassionate care were more likely at (β: 0.107, 95% CI: 0.092–0.122) to improve mean SRH knowledge than those in the control clusters. Likewise, the control group has also revealed a significant mean score increment. Paradoxically utilized SHS at pocketed Pvt, health facilities at the intervention arm had increased at (β: 0.045, 95% CI: 0.032–0.059), but almost no change in the control group. The Pearson chi-square analysis revealed a significant association between variables of interest and school-linked SRH module-based friendly health education at (65.550, p<0.001) (Table 4).
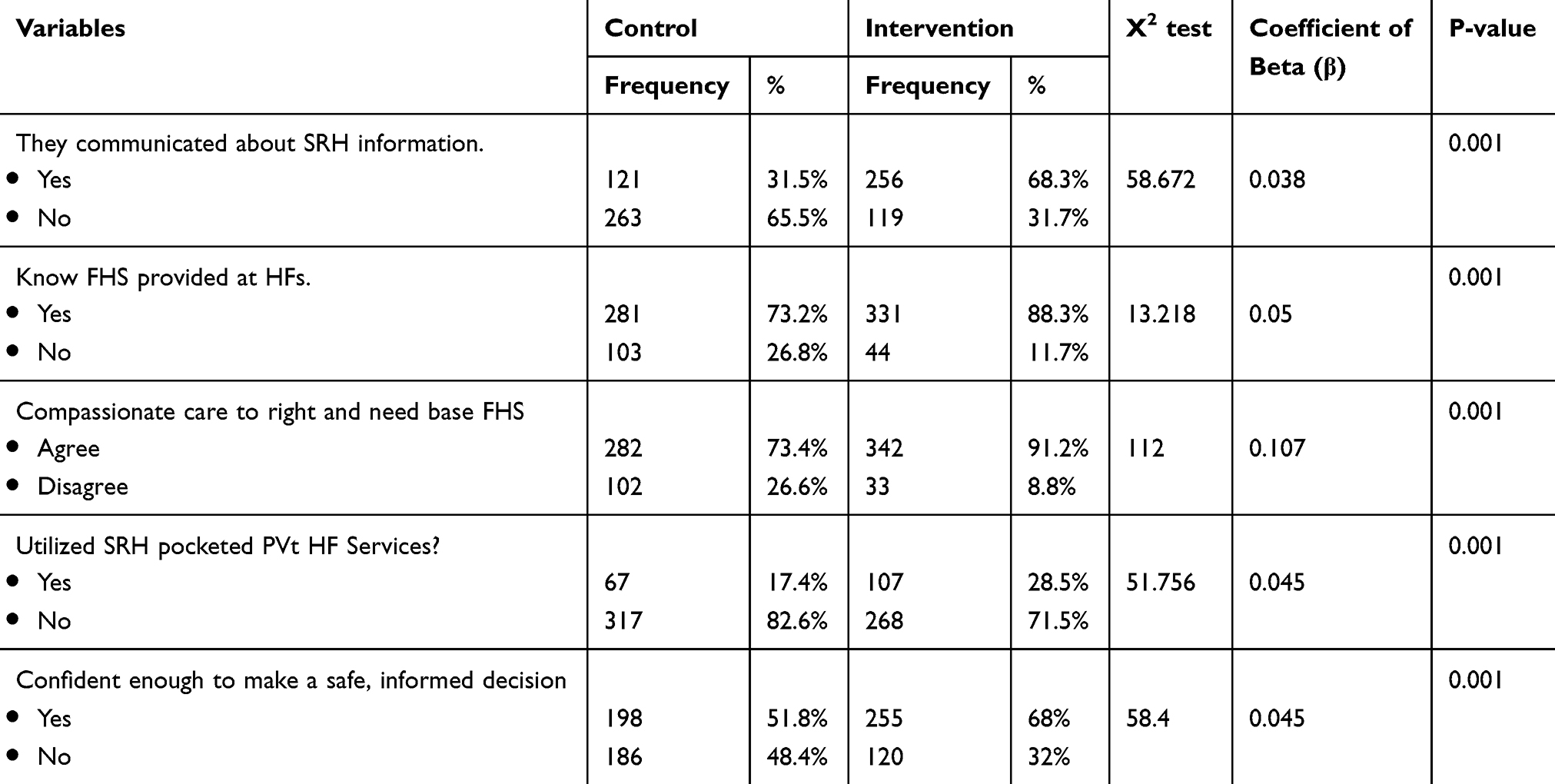 |
Table 4 Comparison of Mean Scores of Covariates Predicts Sexual and Reproductive Health Knowledge Among High Schools in Guji Zone, Ethiopia, February 2022 (n =759) |
Discussion
The results indicated that the intervention program significantly enhanced adolescents’ SRH knowledge in the study areas. Module-based, friendly health education packages were an interactive model to improve adolescents’ SRH knowledge. In this study, individual- and behavioral-level factors predicted more improvement in enhancing SRH knowledge than environmental-level factors.
It implies that school-linked module-based friendly health education significantly influenced adolescents’ SRH knowledge, extending to variables operating at the individual and behavioral levels. The outcomes of this study indicated that school-linked module-based friendly health education improved adolescents’ SRH knowledge with increased communication of SRH Information, identified health facilities that provided friendly health services (FHS), providers compassionate care, and developed the confidence to make safe and informed decisions through interactive learning.6
The outcome indicated that a module-based friendly health education program significantly improved sexual and reproductive health knowledge in the intervention arm. These outcomes are reliable with the results of school-based studies that experiment to assess the effect of a school-based sexual health education program on SRH knowledge among high school adolescent students.14,15,47 Moreover, the study by Nair et al recommended that school-based SRH education influenced positive changes in sexual behavior.48 However, the mean differences in adolescents’ SRH knowledge between the two study arms were minor (0.0684). It may explain the reason that adolescents in the control arm might access some sexual and Reproductive health info from different sources, including teachers, friends, and Social media. This suggestion corresponds with Menna et al49 and other school-based studies,19,50–52 and,12 which showed that adolescents received SRH information from peers, teachers, and media.
“Our study demonstrated that individual-level and behavioral-level factors had predicted more enhancement in SRH knowledge than environmental-level factors”. The report suggests that the government might focus on individual and behavioral-level factors. Likewise, the result indicated that SRH Knowledge in the intervention and control groups was a negative mean difference in the baseline study. However, after the trial, the mean differences in SRH Knowledge between the trial and control group were improved. The mean difference showed that the module-based friendly health education program had significantly altered SRH Knowledge in the intervention group.
Furthermore, the mean difference within the intervention group was higher than in pre-trial outcomes with significant positive changes. The Pearson chi-square analysis demonstrated a significant association between the outcome variable and school-linked module-based friendly health education intervention. Adolescents in the trial clusters enhance SRH knowledge compared to the control arm. This result suggests that school-linked module-based friendly health education interventions significantly correlate with improved adolescents’ SRH knowledge. In the end-line survey, the proportion of adolescents with SRH knowledge increased from 168 (44%) to 244 (65%). The change in proportion is 21%. Additionally, the mean SRH knowledge increased from 0.4416 at baseline to 0.7327 at the end line. This finding is consistent with,48 which tried to evaluate the effectiveness of school-based SRH education among school-age adolescents. Similarly, the finding was almost in line with the study conducted in Adet Tana Haik, Ethiopia, by 59.6%.20 However, the finding was lesser than studies conducted in the Amhara region and Mekelle high school, Tigray Ethiopia, 88% and 90.7%,9,51 Uganda, 95%,53 but greater than other studies in Ethiopia, 24.5%,8 in India, 28% and 33.5%,13 and in Nepal, 41%.54
According to the findings, each additional day of compassionate care provided by HCPs during the school-linked module-based friendly health education intervention is projected to increase SRH knowledge by 0.107. This finding aligns with Mengistie et al, who revealed that most health workers in Ethiopia had positive attitudes toward SRH services.55–57 it implies that experiential learning programs were more effective than non-trial learning programs.
Strength and Limitations
We implement a double-masked approach. Hence, adolescents and data collectors were uninformed of the intervention and the availability of different study arms. Likewise, the research relied on the public school linked with nearby health facilities that performed the interventions. Correspondingly, the data collectors were unconscious if they were in the intervention or control arms. The research compared baseline and end-line dependent variables between the trial and control clusters. High schools/clusters were listed and employed before the randomization.
On the other hand, we conducted this research exclusively in government schools; thus, the findings cannot be generalized to adolescents enrolled in private schools. On the other hand, the experimental period was comparatively small, from (November 2020 to May 2022). Consequently, we may not be able to evaluate the impact. Therefore, long-term experimental support by the qualitative study is crucial for further studies.
Conclusion and Recommendation
In conclusion, the School-Linked Module-based friendly health education Intervention program has significantly increased SRH knowledge among high school adolescent students in the east Guji zone, Ethiopia. Accordingly, we reject a null hypothesis on the significant difference between the two population mean using paired an independent t-test distribution with 374 degrees of freedom at 95% CI (0.26872, 0.3). Providing school-linked, module-based, friendly health education intervention programs and compassionate care by health care providers were the most important predictors of SRH knowledge.
The findings suggest that MoH could strengthen school-linked module-based friendly health education intervention programs within adolescent-friendly health settings and motivate healthcare providers to deliver compassionate care. Moreover, as recommended, the program could focus on continuously providing SRH information to enhance SRH knowledge among school adolescents. Therefore, health authorities, school administrators, and relevant stakeholders should consider adopting a school-linked module-based friendly health education program approach.
Abbreviations
AFHS, Adolescent Friendly Health Services; AFSRH, Adolescent Friendly Sexual and Reproductive Health; FHS, Friendly Health Services; MBFHEP, Module Based Friendly Health Education program; MoH, Ministry of Health; HCP, Health Care Providers; RHB, Regional Health Bureau; RH, Reproductive Health; MoH, Ministry of Health; SRH, Sexual and reproductive health.
Data Sharing Statement
All data in this study were already available in this article. However, suppose additional specific data and other study documents are required. In that case, we can share the data via a link after the publication of the manuscript after the deidentification of specific individual information.
Ethical Consideration
We obtained ethical clearance from Jimma University (Ref.No IHRPCA/721/202, dated 17/08/2020) and the Health Bureau of Oromia Region (Lakk/Ref No BEFO/MBTF/2081, dated 27/01/2013, ETC. or 07/10/2020). We confirmed that our study complies with the Declaration of Helsinki, and participants and parental informed consent included publication of anonymized response. The study protocol of the study included verbal informed consent and parents/guardians provided provided informed consent on the behalf of the study participants under age of 18, which was already approved by Ethical Review Board.
Acknowledgment
The authors gratefully acknowledge Jimma University, the Ministry of Health Ethiopia, the Oromia Regional Health Bureau, and Guji Zonal and Districts Health and Education offices for their irreplaceable support in this study. Additionally, we thank all study contributors, high school directors, homeroom teachers, data collectors, and supervisors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Obach A, Sadler M, Jofré N. Salud sexual y reproductiva de adolescentes en Chile: el rol de la educación sexual. Revista de Salud Pública. 2017;19(6):848–854. doi:10.15446/rsap.V19n6.70023
2. Sani AS, Abraham C, Denford S, Ball S. School-based sexual health education interventions to prevent STI / HIV in sub-Saharan Africa: a systematic review and meta-analysis. BMC Public Health. 2016;16(1). doi:10.1186/s12889-016-3715-4
3. Rizkia M, Ungsianik T. Improving female adolescents knowledge, emotional response, and attitude toward menarche after implementing menarcheal preparation. Reprod Health Educ. 2015;2:84–91.
4. Wilkins NJ, Rasberry C, Liddon N, et al. Addressing HIV/sexually transmitted diseases and pregnancy prevention through schools: an approach for strengthening education, health services, and school environments that promote adolescent sexual health and well-being. Revista espanola de anestesiologia y reanimacion. 2023;70(4):540–549. doi:10.1016/j.redare.2023.09.008
5. Dapari R, Safrin M, Bashaabidin M, et al. Health Education Module Based on Information – motivation – behavioural Skills (IMB) for Reducing Depression, Anxiety, and Stress among Adolescents in Boarding Schools: a Clustered Randomised Controlled Trial; 2022.
6. Yakubu I, Garmaroudi G, Sadeghi R, Tol A, Yekaninejad MS. Assessing the impact of an educational intervention program on sexual abstinence based on the health belief model amongst adolescent girls in Northern Ghana, a cluster randomized control trial. Reprod Health. 2019;2:1–12.
7. Lawrence TZ, Akintobi TH, Miller A, Archie-booker E. Assessment of a culturally-tailored sexual health education program for African American Youth. Int J Environ Res Public Health. 2017;15(1):1–13. doi:10.3390/ijerph15010001
8. Oljira L, Berhane Y, Worku A. Assessment of comprehensive HIV/AIDS knowledge level among in-school adolescents in eastern Ethiopia. J Int AIDS Soc. 2013;16:11–15.
9. Patrice-Coy C, Johnson EJ, Boodram CAS. Sexual behavior of female adolescents on the spread of HIV/AIDS and other STDs in Carriacou. Medicine. 2016;95(36). doi:10.1097/MD.0000000000004800
10. Kassa TA, Luck T, Bekele A, Riedel-heller SG. Sexual and reproductive health of young people with disability in Ethiopia: a study on knowledge, attitude, and practice: a cross-sectional study. Global Health. 2016;12:1–11. doi:10.1186/s12992-016-0142-3
11. Lim MSC, Zhang X-D, Kennedy E, et al. Sexual and reproductive health knowledge, contraception uptake, and factors associated with unmet need for modern contraception among adolescent female sex workers in China. PLoS One. 2015;10(1):e0115435. doi:10.1371/journal.pone.0115435
12. Ajike SO, Mbegbu VC. Adolescent / youth utilization of reproductive health services: knowledge still a barrier 2. Need Adole Youth. 2016;2(3):17–22.
13. Gupta M, Bhatnagar N, Bahugana P. Inequity in awareness and utilization of adolescent reproductive and sexual health services in the union territory, Chandigarh, North India. Indian J Public Health. 2015;59(1):9. doi:10.4103/0019-557X.152846
14. Sommart J, Sota C. The effectiveness of a school-based sexual health education program for junior high school students in Khon Kaen, Thailand. Procedia Soc Behav Sci. 2013;91:208–214. doi:10.1016/j.sbspro.2013.08.419
15. Ducation E, Zhang F-P, Mäkelä S, Poutanen M, Huhtaniemi I. Policy S School -B Ased, And S Chool -L Inked S Exual H Ealth. Endocrinology. 2004;146(2):596–600. doi:10.1210/en.2004-0913
16. Godana G, Garoma S, Ayers N. Effect of a school-linked life skills intervention on adolescents sexual and reproductive health skills in Guji zone, Ethiopia (CRT)— a generalized linear model. Front Public Health. 2023;2:11.
17. Borawski EA, Tufts KA, Trapl ES. Effectiveness of health education teachers and school nurses teaching sexually transmitted infections/human immunodeficiency virus prevention knowledge and skills in high school. J Sch Health. 2016;85(3):189–196.
18. Sidamo NB, Hussen S, Shimbre MS, et al. Effectiveness of curriculum-based sexual and reproductive health education on healthy sexual behaviors among year one students at Arba Minch University: a quasi-experimental study. PLoS one. 2023:1–15. doi:10.1371/journal.pone.0288582
19. Deshmukh DD, Chaniana SS Knowledge about sexual and reproductive health in adolescent school-going children of 8th, 9th, and 10th Standards; 2020.
20. Ayalew M, Nigatu D, Sitotaw G, Debie A, Noutoshi Y. Knowledge and attitude towards sexual and reproductive health rights and associated factors among Adet Tana Haik College students, Northwest Ethiopia: a cross-sectional study. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-018-4038-6
21. Kusheta S, Bancha B, Habtu Y, Helamo D, Yohannes S. Adolescent-parent communication on sexual and reproductive health issues and its factors among secondary and preparatory school students in Hadiya Zone, Southern Ethiopia: institution based cross-sectional study. BMC pediatrics. 2019;1–11.
22. Krugu JK, Mevissen FEF, Prinsen A, Ruiter RAC, Gold J, Free C. Who’s that girl ? A qualitative analysis of adolescent girls views on factors associated with teenage pregnancies in Bolgatanga, Ghana. Reprod Health. 2016;13:1–12. doi:10.1186/s12978-015-0112-x
23. de Lijster GPA, Felten H, Kok G, Kocken PL. Effects of an interactive school-based program for preventing adolescent sexual harassment: a cluster-randomized controlled evaluation study. J Youth Adolesc. 2016;45(5):874–886. doi:10.1007/s10964-016-0471-9
24. Brittain AW, Carolina A, Briceno L, et al. Systematic Review Update. 2019;55(5):725–735.
25. Meena JK, Verma A, Kishore J, Ingle GK. Sexual and Reproductive Health: knowledge, Attitude, and Perceptions among Young Unmarried Male Residents of Delhi. Int J Reprod Med. 2015;2015:1–6. doi:10.1155/2015/431460
26. Kennedy EC, Bulu S, Harris J, Humphreys D, Malverus J, Gray NJ. ”these issues are not talked about at home”: a qualitative study of the sexual and reproductive health information preferences of adolescents in Vanuatu. BMC Public Health. 2014;14(1). doi:10.1186/1471-2458-14-770
27. Germain BA. Human Rights. 2013;1–20.
28. Oljira L National Adolescent and Youth Health Strategy (2016–2020) Federal Democratic Republic of Ethiopia Health Ministry; 2020.
29. Hettiarachchi R, Sivayogan S, Gnanissara SAP. Effectiveness of an Educational Intervention on Sexual and Reproductive Health Education Directed at School Teachers in the Kalutara District. NSF. Colombo; 2009:32.
30. Tesema D, Tamirat M, Tadele A. Sexual behaviors and its association with life skills among school adolescents of Mettu town. South West Ethiopia. 2020;2:4.
31. CSA. Summary and Statistical Report of the 2007 Population and Housing Census of Ethiopia; 2008.
32. Kennedy-shaffer L, Hughes MD. HHS Public Access. Clinical Trials. 2022;19(1):42–51. doi:10.1177/17407745211059845
33. Breukelen GJP. The efficient design of cluster randomized trials with treatment-dependent costs and treatment-dependent unknown variances; 2018:3027–3046.
34. Barais M, Roussel HV, Costa D, Derriennic J, Pereira B, Cadier S Premature ejaculation in primary care: communication strategies versus usual care for male patients consulting for a sexual, urogenital or psychological reason – GET UP: study protocol for a cluster randomized controlled trial. 2018;1–10.
35. van Breukelen GJP, Candel MJJM. Efficient design of cluster randomized trials with treatment-dependent costs and treatment-dependent unknown variances. Stat Med. 2018;37(21):3027–3046. doi:10.1002/sim.7824
36. Lemeshow. Sample size determination in health studies; 1991.
37. Stephen FT, Lanre A. Efficiency Of proportional allocation procedure over other allocation procedures in stratified random sampling. Int J Adv Res Publ. 2019;2(4):1–4.
38. Suskie LA. Questionnaire Survey Research What Works.
39. Roopa S. Questionnaire Designing for a Survey 1. J In Orthod Soc2012;46:273–277.
40. Stajkovic A, Sergent K Social cognitive theory a model of triadic influences; 2020.
41. Nabavi RT Theories of developmental psychology title: bandura’s social learning theory & social cognitive learning theory razieh tadayon nabavi; 2014.
42. Savaya R The logic model: a tool for incorporating theory in development and evaluation of programs; 2014.
43. Smith JD, Li DH, Rafferty MR The implementation research logic model: a method for planning, executing, reporting, and synthesizing implementation projects; 2020:1–12.
44. Dhakal CP Interpreting the basic outputs (SPSS) of multiple linear regression; 2019.
45. A.Woodwars ACEW. Statistical Analysis Quick Reference Guidebook with SPSS Examples. University of Texas, Southwestern Medical Center; 2007.
46. Faraway JJ Practical regression and Anova using R. Unpubl Work No details; 2002.
47. Amaugo LG, Papadopoulos C, Ochieng BMN, Ali N. The effectiveness of HIV/AIDS school-based sexual health education programs in Nigeria: a systematic review. Health Educ Res. 2014;29(4):633–648. doi:10.1093/her/cyu002
48. Nair MKC, Paul MK, Leena ML. Effectiveness of a reproductive sexual health education package among school going adolescents. Ind J Pediatr2012;79:64–68.
49. Menna T, Ali A, Worku A, Gao S. Effects of peer education intervention on HIV / AIDS related sexual behaviors of secondary school students in Addis Ababa, Ethiopia: a quasi-experimental study. Reprod Health. 2015;12:1–8. doi:10.1186/1742-4755-12-1
50. Brief E EVIDENCE Are parents talking to adolescents about sexuality ? Evidence from four slums in Ghana; 2015.
51. Gultie T, Hailu D, Workineh Y. Age of menarche and knowledge about menstrual hygiene management among adolescent school girls in Amhara province, Ethiopia: implication to health care workers & school teachers. PLoS One. 2014;9(9):1–9.
52. Cegolon L, Bortolotto M, Bellizzi S, Cegolon A, Mastrangelo G, Xodo C. Birth control knowledge among freshmen of four Italian universities. Sci Rep. 2020;10(1):1–16. doi:10.1038/s41598-019-56847-4
53. Kemigisha E, Bruce K, Nyakato VN, et al. Sexual health of very young adolescents in South Western Uganda: a cross-sectional assessment of sexual knowledge and behavior. Reprod Health. 2018;1–8.
54. Adhikari R, Vannak U, Sokhey L, Ngo TD, Gold J, Free C. Knowledge on the legislation of abortion and experience of abortion among female youth in Nepal: a cross-sectional study. Reprod Health. 2016;13:1–9. doi:10.1186/s12978-016-0166-4
55. Mengistie B, Tilahun M, Reda AA, Egata G. Health workers’ attitudes toward sexual and reproductive health services for unmarried adolescents in Ethiopia. Reprod Health. 2012;9(1):19. doi:10.1186/1742-4755-9-19
56. Edwards PV, Roberts ST, Chelwa N, et al. Perspectives of adolescent girls and young women on optimizing youth-friendly HIV and sexual and reproductive health care in Zambia. Front Global Women Health. 2021;2:1–10.
57. Gausman J, Othman A, Qotob R, et al. Health care professionals attitudes towards youth-friendly sexual and reproductive health services in Jordan: a cross-sectional study of physicians, midwives, and nurses. Reprod Health. 2021;1–12.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.