")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
The Association between Acupuncture Therapy and the Risk of Disability Development in Dementia Patients: A Nationwide Cohort Study
Authors Huang CY , Wu MY , Huang MC , Yu TS, Mayer PK, Yen HR
Received 22 August 2023
Accepted for publication 4 January 2024
Published 20 February 2024 Volume 2024:20 Pages 295—305
DOI https://doi.org/10.2147/NDT.S432556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Chia-Yu Huang,1,2 Mei-Yao Wu,3– 5 Ming-Cheng Huang,2,3 Teng-Shun Yu,6,7 Peter Karl Mayer,3,8,* Hung-Rong Yen2,3,5,8,9,*
1Department of Family Medicine, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan; 2Graduate Institute of Chinese Medicine, School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 3Department of Chinese Medicine, China Medical University Hospital, Taichung, Taiwan; 4School of Post-Baccalaureate Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 5Research Center for Traditional Chinese Medicine, Department of Medical Research, China Medical University Hospital, Taichung, Taiwan; 6Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan; 7College of Medicine, China Medical University, Taichung, Taiwan; 8International Master Program in Acupuncture, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 9Chinese Medicine Research Center, China Medical University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Hung-Rong Yen, School of Chinese Medicine, College of Chinese Medicine, China Medical University, 91 Hsueh-Shih Road, North District, Taichung, 404, Taiwan, ext. 3001 Fax +886-4-22365141, Email [email protected]
Purpose: Disability is the comorbidity of dementia for which there is no available preventive measure. The aim of this study was to investigate the association between acupuncture treatment and the risk of disability development in dementia patients.
Patients and Methods: A cohort study was performed using a nationwide health database in Taiwan. The included dementia patients were divided into acupuncture and non-acupuncture cohorts based on whether they received acupuncture treatment during the follow-up period. The variables in the two cohorts were controlled by 1:1 propensity-score matching. The difference in disability development in dementia patients between the acupuncture and non-acupuncture cohorts was also analyzed. Subgroup analyses were performed using socioeconomic variables, comorbidities and anti-dementia agents (donepezil, rivastigmine, galantamine and memantine) used for dementia treatment.
Results: A total of 9,760 dementia patients met our inclusion criteria, and patients were divided into an equal number (n=2,422) of acupuncture and non-acupuncture groups, respectively, after 1:1 propensity-score matching. The dementia patients had a lower risk of disability development after acupuncture treatment than those who did not receive acupuncture treatment (adjusted hazard ratio 0.65, 95% confidence interval 0.60– 0.70, p < 0.001). The results were independent of basic variables or comorbidities in the two cohorts. Patients who did not use anti-dementia agents had a lower risk of developing disability after receiving acupuncture intervention than those who used anti-dementia agents.
Conclusion: Our results revealed the relationship between acupuncture intervention and decreased risk of developing disability in dementia patients. The results are useful for dementia treatment, trial design and further planning of care programs.
Keywords: acupuncture, disability, dementia, traditional Chinese medicine
Introduction
Dementia is a neurodegenerative disease1 and most patients are diagnosed at middle or old age. Additionally, some subtypes of dementia could be found at relatively young ages, such as frontotemporal dementia.2 The primary clinical presentations of dementia patients vary, and delayed diagnosis is not uncommon.2 The prevalence of dementia worldwide doubles every 5 years,3 and it was estimated approximately 152.8 million cases will be identified in 2050.4 According to the etiologies, dementia can be divided into several subgroups: Alzheimer’s disease, vascular dementia and other dementia, including frontotemporal dementia and dementia with Lewy bodies, etc.5 Alzheimer’s disease is most commonly caused by mutant proteins, such as tau and amyloid beta which accumulate in the human brain and subsequently cause memory loss and cognitive dysfunction. Vascular dementia is caused by cerebral vascular damage, and the symptoms of such a patient depend on the site and severity of the associated brain damage;6 its relationship with Alzheimer’s disease is still controversial.7 Other dementia includes Lewy body disease and frontotemporal dementia, which are characterized by slow progression and relative memory preservation.8
The management of dementia could be divided into nonpharmacologic and pharmacologic approaches.9 Trying to elevate activity through exercise and social interaction, keeping proper sleep and personal hygiene, and maintaining psychological health are considered nonpharmacologic managements.8 Four types of medications that increase the acetylcholine concentration in the brain and decrease the effect of glutamate to relieve the course of dementia from Alzheimer’s disease are available: donepezil, rivastigmine, galantamine, and memantine.8 Donepezil, rivastigmine, and galantamine could be used for mild to moderate dementia, while memantine and donepezilI could be prescribed for moderate-to-severe dementia.8 However, the response rates of these agents are not favorable, and complications including dizziness, gastrointestinal uncomfortable, insomnia, fatigue, abnormal cardiac conduction, and liver dysfunction have been reported.10 Low motor function is the core mechanism of the aforementioned problems, and disability has been noted as a predictor of death.11 Thus, the study of preventive interventions for decreasing dementia complications, including integrative treatments, is becoming an important topic. The atypical antipsychotics, such as risperidone and olanzapine may be beneficial for controlling neuropsychiatric symptoms, but they also increase the risk of stroke.12
Chinese medicine is an Eastern-style integrative intervention that usually involves the use of Chinese herbs and acupuncture.13 A meta-analysis showed that acupuncture could potentially improve the Hasegawa Dementia Scale (HDS), Mini-Mental State Examination scores (MMSE), and Scale for the differentiation of syndromes of vascular dementia (SDSVD) in patients with vascular dementia.14 Compared to those treated for Alzheimer’s disease with Western medicine, patients in the acupuncture cohort were found to achieve preservation of their activities of daily living (ADL).15 The above evidence was collected from clinical trials in which patients were observed for several months. However, studies assessing middle- to long-term outcomes after acupuncture intervention are still lacking.
Public health insurance has been practiced in Taiwan for 28 years, and data on the clinical care of clinics and admissions are recorded in a health insurance database called the National Health Insurance Research Database (NHIRD) as deidentified personal medical information. To date, more than 99% of Taiwanese individuals have been covered by the NHIRD.13 In other words, the NHIRD is a large-scale, long-term follow-up healthcare database. All medical services from both Western and Chinese physicians are recorded in the NHIRD.13 The aim of our study was to use the NHIRD to investigate the association between acupuncture therapy and the risk of disability development in patients with dementia, including subgroup analyses according to the etiologies of dementia. The results could offer information that could not be obtained from short-term clinical trials or laboratory experimental studies.
Materials and Methods
Study Design and Setting
This is a retrospective cohort study performed by 1:1 propensity-score matching. Data from patients who were newly diagnosed with dementia from 1 January 2008 to 31 December 2016 in the Longitudinal Generation Tracking Database 2005 (LGTD2005) were collected. The index date and immortal time were defined as the first time that patients received acupuncture treatment and the interval from dementia being diagnosed to the index date, respectively. Patients were followed up until December 31, 2017, or withdrawn from the LGTD2005.
Participants
The inclusion criterion was a diagnosis of dementia found in ≥ 2 medical records. The exclusion criteria were (1) lacking of basic patient characteristics, such as sex, age, urbanization or income level, and (3) interruption of health insurance coverage. The patients meeting our inclusion criteria were divided into acupuncture and non-acupuncture cohorts depending on whether they accepted acupuncture interventions from the date of diagnosis of dementia to 31 December 2016.
Variables
The diagnosis of dementia was coded by the International Classification of Diseases, Ninth or Tenth Revision, Clinical Modification (ICD-9-CM/ICD-10-CM) codes: 290.0–290.4, 294.1, 331.0 to 331.2/F00, F01, F02, F03, and G30. The characteristics of the patients were sex, age, urbanization and income levels. There were 3 subgroups based on age: <64 years, 65–79 years, and ≥80 years. The definition of elderly individual in Taiwan is ≥65 years old16 and those who are aged ≥80 years could apply whole-day caregiver without limitation due to the higher prevalence rate of disability found in this age interval.17 The age had a high association with the disability which needs to conduct further subgroup analysis. Considering the convenience of medical visits in different areas and the affordability of medical expenses, we set urbanization and monthly income to be the variables, respectively. The level of urbanization was also divided into level 1 (highest) to level 3 (lowest).18,19 The income of the patients could be designed as 3 levels: ≥New Taiwan dollar (NTD)40,000, NTD20,000–39,999, and ≤ NTD20,000.20,21
Comorbidities were defined by the ICD-9-CM and ICD-10-CM codes when they existed in the medical records ≥2 times before the date of dementia diagnosis, such as diabetes mellitus (DM), hypertension (HTN), hyperlipidemia, cardiovascular diseases (CVD), chronic obstructive pulmonary disease (COPD), obesity, cancer, stroke and Parkinson’s disease (PD). Personal habits were also collected as smoking and alcoholism.
The anti-dementia agents are donepezil, rivastigmine, galantamine and memantine. According to the prescription guidelines, when patients used donepezil, rivastigmine and galantamine, they would be set as mild-to-moderate dementia. And patients were included in the moderate-to-severe dementia when they used memantine.8 Based on the manipulation of acupuncture, the types of acupuncture were divided into 2 cohorts: manual acupuncture and electroacupuncture. The primary outcome was the measurement of disability, which was defined as the placement of a urinary catheter, nasogastric tube, and tracheostomy tube in dementia patients.22
Data Sources and Ethical Considerations
We used the Longitudinal Generation Tracking Database 2005, containing 2 million individual medical records randomly collected from the NHIRD, as our source. There was no identified personal information in the database we used, and informed consent was waived. This study was approved by the Research Ethics Committee of China Medical University and Hospital, Taiwan (CMUH109-REC2-031(CR-3)).
Bias
To control for potential selection bias, propensity-score matching was used to minimize the difference between the acupuncture and non-acupuncture groups.
Statistical Methods
The chi-square test was used to calculate the difference in baseline characteristics between the acupuncture and non-acupuncture groups. The Kaplan‒Meier method and the Log rank test were used to detect the difference in disability noted between the two groups. The crude hazard ratio (cHR) and adjusted hazard ratio (aHR) were predicted by Cox proportional hazard regression analysis. We used SAS 9.4 (SAS Institute, Cary, NC, USA) and R software (R Foundation for Statistical Computing, Vienna, Austria) to perform our analyses, and when P was < 0.05, the difference was considered to be significant.
Results
There were 25,924 patients that met our inclusion criteria, but disability was noted before dementia in 16,141 patients, and personal characteristics were missing in 23 patients. Finally, 9,760 newly diagnosed dementia patients were divided into acupuncture and non-acupuncture groups. Then, a 1:1 propensity-score match was performed, and 2,422 dementia patients were found in each group (Supplementary Figure 1). The distributions of sex, mean age, urbanization level, income level, comorbidities, habits, or medication use in the two groups were not significant after 1:1 propensity-score matching (Table 1). And the median income of the two cohorts is the same (NTD22,800).
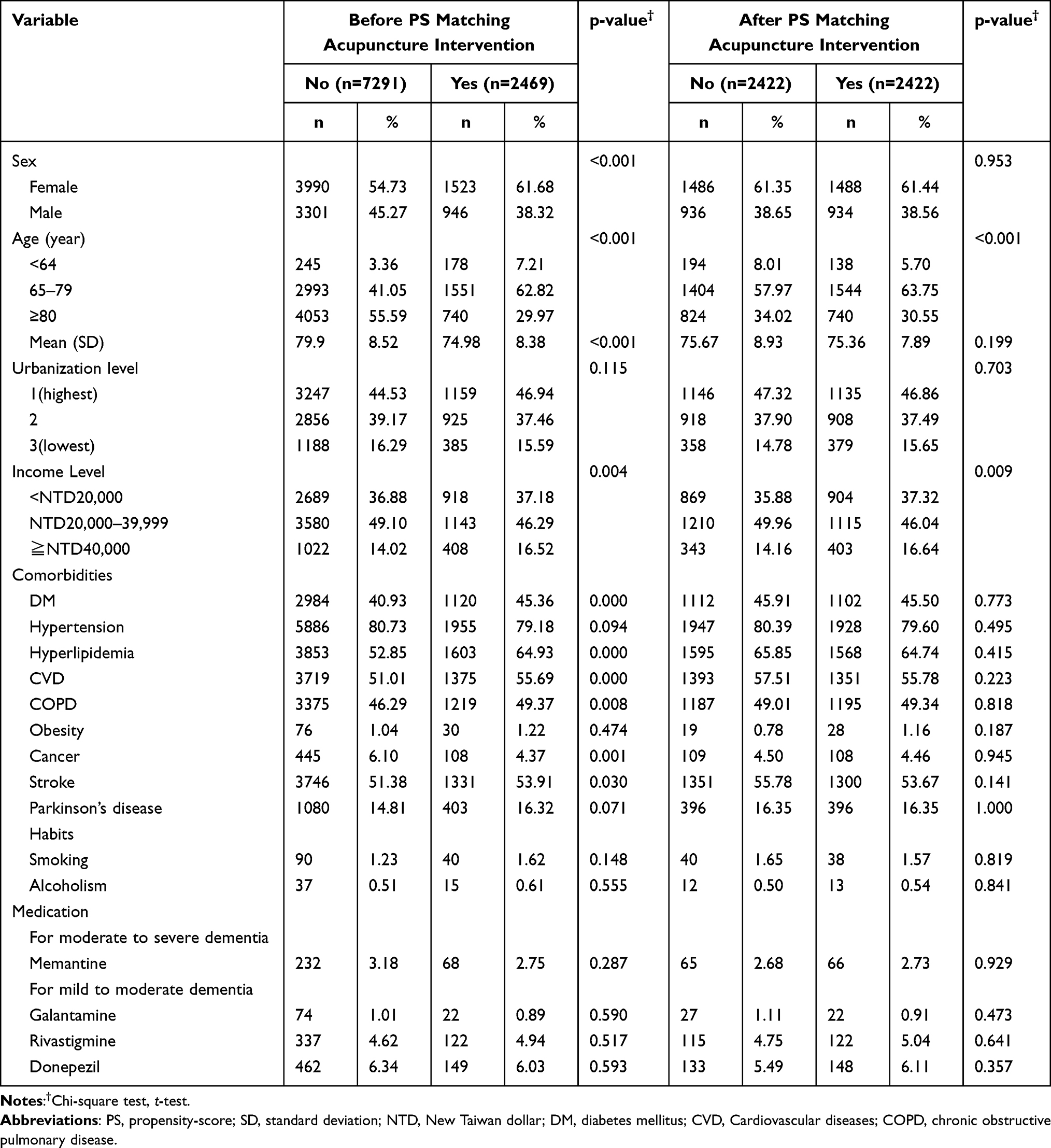 |
Table 1 Characteristics of Patients with Dementia Who Received Acupuncture Therapy and Patients with Dementia Who Did Not Receive Acupuncture Therapy |
Dementia patients who accepted acupuncture therapy had a lower risk of developing disability than those who did not accept acupuncture therapy (aHR 0.65, 95% confidence interval (CI) 0.60–0.70, p < 0.001, Supplementary Figure 2). Table 2 shows the effect of each variable on the results from acupuncture intervention through the Cox model with HRs and 95% CIs. Male dementia patients had a higher risk of having disability than female individuals did (aHR 1.33, 95% CI 1.22–1.44). The age intervals of ≥80 years old (aHR 2.60, 95% CI 2.11–3.20) and 65–79 years old (aHR 1.52, 95% CI 1.24–1.87) had a higher risk of disability development than those aged <65 years. Compared to those living in urbanization level 1, the patients living in level 2 (aHR 1.11, 95% CI 1.01–1.21) or level 3 (aHR 0.99, 95% CI 0.87–1.11) did not have a higher risk of becoming disabled. The risk of developing disability in subgroups of monthly income NTD20,000–39,999 or ≧NTD40,000 was not higher than <NTD20,000. Compared to patients who did not have DM (aHR 1.27, 95% CI 1.16–1.38), HTN (aHR 1.31, 95% CI 1.16–1.47), stroke (aHR 1.29, 95% CI 1.18–1.41), or PD (aHR 1.26, 95% CI 1.14–1.40), those who had comorbidities had a higher risk of disability. Hyperlipidemic patients had a lower risk of being diagnosed with disability than those who had this problem. The difference in disability development between patients who had or did not have CVD, COPD, obesity, or cancer was not significant. Whether anti-dementia agents, such as Witgen, Reminyl, Exelon, or Aricept, were used, they did not change the results of disability.
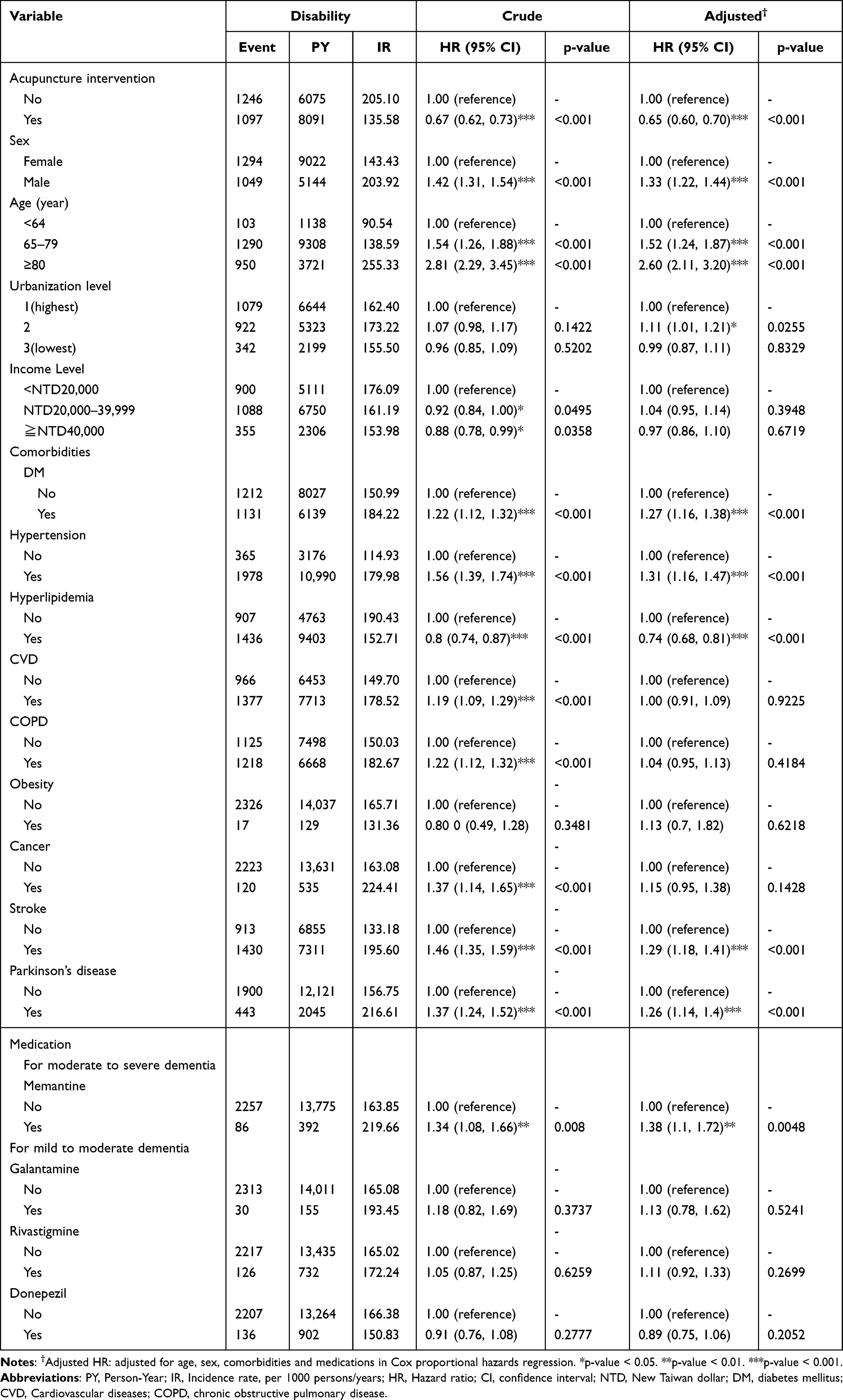 |
Table 2 Cox Model with Hazard Ratios and 95% Confidence Intervals of Disability Associated with Receiving Acupuncture and Covariates Among Patients with Dementia |
In the subgroup analyses, patients with all types of dementia had a lower risk of developing disability when they accepted acupuncture therapy than those who did not (Figure 1). Table 3 reveals that female (cHR 0.69, 95% CI 0.62–0.77; aHR 0.73, 95% CI 0.66–0.82, Supplementary Figure 3A) and male (cHR 0.63, 95% CI 0.56–0.71; aHR 0.58, 95% CI 0.51–0.65, Supplementary Figure 3B) who accepted acupuncture had a lower risk of finding disability than those who did not. In all the age subgroups (<64-year-old (cHR 0.60, 95% CI 0.40–0.89; aHR 0.62, 95% CI 0.41–0.93, Supplementary Figure 4A), 65–79-year-old (cHR 0.68, 95% CI 0.61–0.76; aHR 0.67, 95% CI 0.60–0.75, Supplementary Figure 4B), and ≥80-year-old (cHR 0.66, 95% CI 0.58–0.75; aHR 0.63, 95% CI 0.55–0.71, Supplementary Figure 4C)), lower risks of having disability occurred after patients accepted acupuncture therapy, compared with those who did not accept acupuncture therapy. Lower risks of being diagnosed with disability after acupuncture treatment were noted at all levels of urbanization: level 1 (cHR 0.65, 95% CI 0.58–0.73; aHR 0.62, 95% CI 0.55–0.70), level 2 (cHR 0.72, 95% CI 0.64–0.82; aHR 0.72, 95% CI 0.63–0.82), and level 3 (cHR 0.60, 95% CI 0.48–0.74; aHR 0.59, 95% CI 0.47–0.73). Patients with all levels of monthly income had a lower risk of disability development when they started to receive acupuncture therapy: <NTD20,000 (cHR 0.63, 95% CI 0.55–0.71; aHR 0.57, 95% CI 0.50–0.66), NTD20,000–39,999 (cHR 0.67, 95% CI 0.60–0.76; aHR 0.69, 95% CI 0.61–0.78), and ≧NTD40,000 (cHR 0.75, 95% CI 0.61–0.93; aHR 0.72, 95% CI 0.58–0.74). Regardless of whether patients had comorbidities of DM (cHR 0.66, 95% CI 0.59–0.75; aHR 0.65, 95% CI 0.58–0.74), HTN (cHR 0.68, 95% CI 0.62–0.74; aHR 0.66, 95% CI 0.60–0.72), hyperlipidemia (cHR 0.69, 95% CI 0.62–0.77; aHR 0.70, 95% CI 0.63–0.78), CVD (cHR 0.63, 95% CI 0.56–0.70; aHR 0.62, 95% CI 0.56–0.69), COPD (cHR 0.65, 95% CI 0.56–0.70; aHR 0.64, 95% CI 0.57–0.71), cancer (cHR 0.51, 95% CI 0.36–0.74; aHR 0.47, 95% CI 0.32–0.70), stroke (cHR 0.71, 95% CI 0.64–0.79; aHR 0.68, 95% CI 0.61–0.76), PD (cHR 0.60, 95% CI 0.50–0.73; aHR 0.58, 95% CI 0.48–0.70) or not (DM (cHR 0.67, 95% CI 0.60–0.75; aHR 0.64, 95% CI 0.57–0.71), HTN (cHR 0.64, 95% CI 0.52–0.78; aHR 0.60, 95% CI 0.49–0.75), hyperlipidemia (cHR 0.62, 95% CI 0.55–0.71; aHR 0.57, 95% CI 0.50–0.65), CVD (cHR 0.73, 95% CI 0.64–0.83; aHR 0.69, 95% CI 0.60–0.78), COPD (cHR 0.68, 95% CI 0.61–0.77; aHR 0.67, 95% CI 0.59–0.75), stroke (cHR 0.61, 95% CI 0.53–0.69; aHR 0.61, 95% CI 0.53–0.69), PD (cHR 0.68, 95% CI 0.62–0.75; aHR 0.67, 95% CI 0.61–0.73)), their risk of being diagnosed with a disability were lower after acupuncture intervention than that of those who did not receive acupuncture therapy. When patients did not have obesity, the risk of disability development was lower (cHR 0.67, 95% CI 0.62–0.73; aHR 0.65, 95% CI 0.60–0.70) after they received acupuncture therapy than that of those who did not receive acupuncture therapy. When patients did not receive Western anti-dementia agents but received acupuncture therapy, their risks of disability were lower than those who received agents: no-Witgen (cHR 0.66, 95% CI 0.61–0.72; aHR 0.64, 95% CI 0.59–0.70), no-Reminyl (cHR 0.67, 95% CI 0.62–0.72; aHR 0.65, 95% CI 0.60–0.71), no-Exelon (cHR 0.66, 95% CI 0.61–0.72; aHR 0.64, 95% CI 0.59–0.70) or no-Aricept (cHR 0.67, 95% CI 0.61–0.72; aHR 0.65, 95% CI 0.60–0.71; Supplementary Figure 5). Supplementary Tables 1 and 2 showed that compared no-acupuncture users, the risks of disability is lower in the users accepted manual acupuncture (cHR 0.65, 95% CI 0.59–0.70; aHR 0.63, 95% CI 0.58–0.69), electroacupuncture (cHR 0.47, 95% CI 0.28–0.79; aHR 0.51, 95% CI 0.30–0.87), and combination of manual acupuncture and electroacupuncture (cHR 0.61, 95% CI 0.51–0.73; aHR 0.61, 95% CI 0.51–0.72).
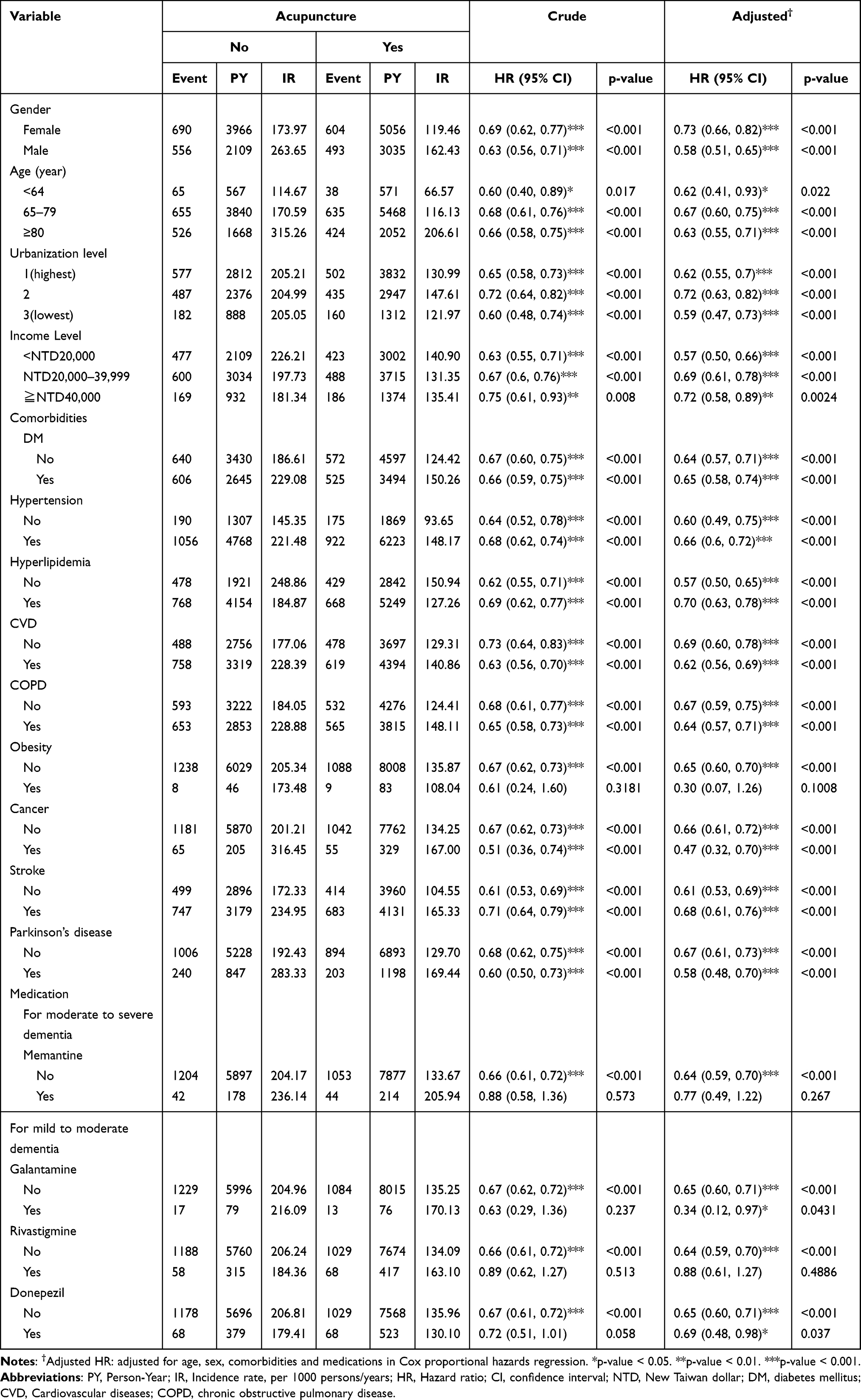 |
Table 3 Incidence Rates, Hazard Ratios and Confidence Intervals of Dementia Patients with Disability Who Received and Did Not Receive Acupuncture, Stratified by All Variables |
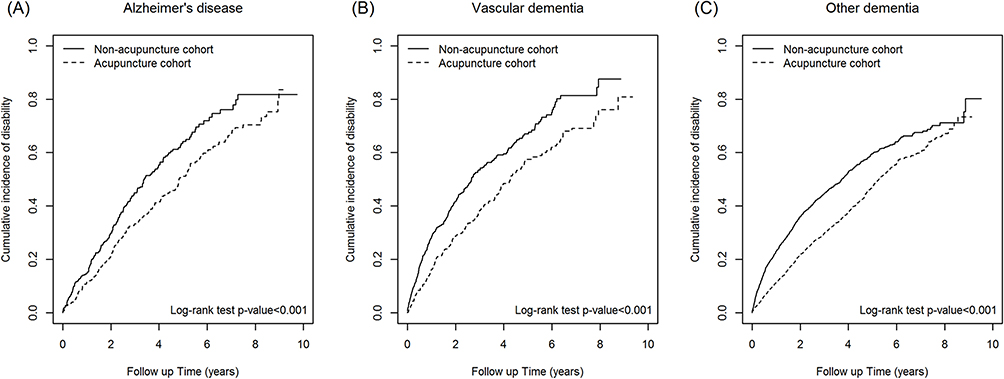 |
Figure 1 The difference of cumulative incidence of disability between acupuncture and non-acupuncture cohorts: (A) Alzheimer’s disease, (B) vascular dementia, and (C) other dementia. |
Discussion
Our results demonstrated that dementia patients could have a lower risk of disability as a result of acupuncture therapy. A significant relationship could be found in all the types of dementia. However, male sex, older age, and comorbidities, including DM, HTN, hyperlipidemia, stroke, and PD, were still risk factors contributing to a higher diagnosis of disability in dementia patients. From the results of subgroup analyses, most variable factors demonstrated their positive relationships with lowering the risk of disability after acupuncture treatment, except Western medication use.
The relationship between dementia and disability has been reported in longitudinal studies.23,24 Males had a slightly higher risk (standardized rate ratio 1.41, 95% CI 1.12–1.76) of developing disability than females, which is similar to our findings.23 Additionally, older dementia patients had a higher risk (OR 3.43, 95% CI 2.04–5.77) of having disability, which was shown in our participants.23 Stroke has been noted as a confounding factor (OR 5.54, 95% CI 2.86–10.72) contributing to dementia, and we matched this disease before further analysis.24 Although there was no significant relationship between CVD (OR 1.40, 95% CI 0.74–2.68) and dementia in a previous cohort study, we still controlled this variable factor for restricted results because CVD is still known as a potential risk factor.24 Dementia is a cognitive impairment disorder since that the association between cognitive impairment and disability was observed in a meta-analysis (Hedges’ g = 0.76, 95% CI 0.68–0.83).25
The possible mechanisms of dementia leading to disability could be divided into irreversible risk factors through biochemical pathways causing neurological, musculoskeletal, and systematic dysfunctions.26 Sex, age, and genetic traits are irreversible factors, and chronic diseases (obesity, HTN, dyslipidemia, and DM), malnutrition (swallowing problem, inadequate diet), personal habits (smoking and alcoholism), psychosocial problems (insomnia, depression, stress, and less social activity), and sensory impairments (hearing and vision) are reversible factors. The biochemical pathways are activated by inflammatory processes, oxidative stress, genetic instability, and mitochondrial and telomere dysfunction. Problems such as neurodegenerative processes and neurosynaptic dysfunction, sarcopenia, frailty, and osteopenia are found in the neurological and musculoskeletal systems and cause systematic destruction. Most of the irreversible and reversible factors were controlled in our study by propensity-score matching to confirm that a reliable result was produced.
Several interventions have been used to prevent dementia from causing disability: supplementation, physical and cognitive training, and integrative care. Significant differences were found with physical and cognitive training only. Although integrative care is the mainstream intervention for sarcopenic and frail individuals, the lack of detailed diet or exercise suggestions to patients may cause nonsignificant results. The role of acupuncture in preventing disability may come from controlling reversible factors, such as reducing inflammation and increasing physical activity. A meta-analysis reported that acupuncture has the potential to control obesity (weighted mean difference (WMD) −0.47 kg/m2, 95% CI −0.58 to −0.35),27 HTN (WMD −3.62 mmHg; 95% CI, −5.90 to −1.34),28 dyslipidemia (SMD: −2.53, 95% CI: −4.55 to −0.67),29 DM (−2.13 mmol/l, 95% CI −2.79 to −1.46),30 dysphagia (SMD 2.02, 95% CI: 0.82 to 3.22),31 smoking (relative risk 2.49, 95% CI 1.14 to 5.97),32 insomnia (SMD 8.96, 95% CI 3.97 to 13.95),33 depression (Hedges’ g = 0.76, 95% CI 0.18 to 0.63),34 stress (SMD −0.41, 95% CI −0.50 to −0.31),35 hearing problems (RR = 2.36, 95% CI 1.20–4.67),36 and vision dysfunction (SMD 0.18, 95% CI 0.17 to 0.20).37 Acupuncture was also shown to control inflammation36 and relieve oxidative stress38 in animal models. Although dementia is more prevalent females,39 the gender difference of disability is not obviously.23 Based on our findings, screening and controlling risk factors contributing disability are the important measurements, especially when the male dementia patients visit Chinese physicians for acupuncture treatment.
There were several limitations in our study. Causality could not be obtained from a retrospective cohort study. The severity of disability could not be found or calculated from our database. However, when dementia patients need tube placement, they have poor physical function which cannot support them in maintaining daily activity.22 The detailed prescription of acupuncture therapy was not recorded in our database. However, the main types of interventions, such as manual acupuncture, electroacupuncture and a combination of the two, could be identified and included in our variable factors. Biomarkers, images and cognitive tests could not be obtained from our database, but the formation of a diagnosis of dementia for insurance reimbursement in Taiwan would need the above information. The treatment dose of acupuncture, such as the frequency, length of treatment or numbers of acupoints has not meet a uniform conclusion, thus we did not perform the analysis here. Not all the types of dementia could be analyzed in our study due to the limited samples in the real-world database.
Conclusion
The association between acupuncture treatment and the lower risk of disability development in dementia patients has been demonstrated in our results. These findings offer a possible long-term effect of acupuncture therapy in the dementia patients which is rarely found in the previous studies. Our study is useful for patients as well as researchers to design novel outcome measures, such as disability in dementia patients who would accept acupuncture therapy. It is helpful to confirm the role of acupuncture treatment in the dementia course.
Acknowledgments
This research was supported by the China Medical University Hospital (DMR-111-192 and DMR-112-175) and Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW112-TDU-B-212-144004). We are grateful to Health Data Science Center, China Medical University Hospital, Taiwan for providing administrative, technical and funding support. The funders had no role in the study design, data collection and analysis, the decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. George EK, Reddy PH. Can healthy diets, regular exercise, and better lifestyle delay the progression of dementia in elderly individuals? J Alzheimers Dis. 2019;72:S37–S58.
2. Pasquier F, Richard F, Lebert F. Natural history of frontotemporal dementia: comparison with Alzheimer’s disease. Dement Geriatr Cogn Disord. 2004;17(4):253–257. doi:10.1159/000077148
3. Cao Q, Tan CC, Xu W, et al. The prevalence of dementia: a systematic review and meta-analysis. J Alzheimers Dis. 2020;73:1157–1166. doi:10.3233/JAD-191092
4. Nichols E, Steinmetz JD, Vollset SE; GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the global burden of disease study 2019. Lancet Public Health. 2022;7(2):e105–e125. doi:10.1016/S2468-2667(21)00249-8
5. van der Flier WM, Scheltens P. Epidemiology and risk factors of dementia. J Neurol Neurosurg Psychiatry. 2005;7:v2–v7. doi:10.1136/jnnp.2005.082867
6. Kumar A, Singh A. A review on Alzheimer’s disease pathophysiology and its management: an update. Pharmacol Rep. 2015;67:195–203. doi:10.1016/j.pharep.2014.09.004
7. O’Brien JT, Thomas A. Vascular dementia. Lancet. 2015;386(10004):1698–1706. doi:10.1016/S0140-6736(15)00463-8
8. Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. JAMA. 2019;322(16):1589–1599. doi:10.1001/jama.2019.4782
9. Di Santo SG, Prinelli F, Adorni F, et al. A meta-analysis of the efficacy of donepezil, rivastigmine, galantamine, and memantine in relation to severity of Alzheimer’s disease. J Alzheimers Dis. 2013;35(2):349–361. doi:10.3233/JAD-122140
10. Mitchell SL, Teno JM, Kiely DK, et al. The clinical course of advanced dementia. N Engl J Med. 2009;361:1529–1538. doi:10.1056/NEJMoa0902234
11. Noale M, Maggi S, Minicuci N, et al. Dementia and disability: impact on mortality. The Italian longitudinal study on aging. Dement Geriatr Cogn Disord. 2003;16:7–14. doi:10.1159/000069987
12. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. 2005;293:596–608. doi:10.1001/jama.293.5.596
13. Huang CY, Huang MC, Sun MF, et al. Acupuncture treatment reduced the risk of coronary heart disease in patients with depression: a propensity-score matched cohort study. Neuropsychiatr Dis Treat. 2021;17:2315–2325. doi:10.2147/NDT.S315572
14. Chen Y, Wang H, Sun Z, et al. Effectiveness of acupuncture for patients with vascular dementia: a systematic review and meta-analysis. Complement Ther Med. 2022;70:102857. doi:10.1016/j.ctim.2022.102857
15. Wang YY, Yu SF, Xue HY, et al. Effectiveness and safety of acupuncture for the treatment of Alzheimer’s Disease: a systematic review and meta-analysis. Front Aging Neurosci. 2020;12:98. doi:10.3389/fnagi.2020.00098
16. Definition of elderly individual in Taiwan. Available from: https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=D0050037.
17. The age limitation of whole-day caregiver application for disability in Taiwan. Available from: https://www.familycare.org.tw/news/10185.
18. Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006;4:1–22.
19. Cheng YY, Chang YT, Cheng HL, et al. Associations between arsenic in drinking water and occurrence of end-stage renal disease with modifications by comorbidities: a nationwide population-based study in Taiwan. Sci Total Environ. 2018;626:581–591. doi:10.1016/j.scitotenv.2018.01.043
20. Chou PH, Lin CC, Lin CH, et al. Prevalence of gastroesophageal reflux disease in major depressive disorder: a population-based study. Psychosomatics. 2014;55:155–162. doi:10.1016/j.psym.2013.06.003
21. Huang CY, Wu MY, Chang CL, et al. Coprescription trends in western medicine, Chinese herbal medicine and dental medicine among older adults in Taiwan from 1997 to 2013. Complement Ther Med. 2021;63:102782. doi:10.1016/j.ctim.2021.102782
22. Lee YH, Lu CW, Huang CT, et al. Impact of a home health care program for disabled patients in Taiwan: a nationwide population-based cohort study. Medicine. 2019;98:e14502. doi:10.1097/MD.0000000000014502
23. Sauvaget C, Yamada M, Fujiwara S, et al. Dementia as a predictor of functional disability: a four-year follow-up study. Gerontology. 2002;48(4):226–233. doi:10.1159/000058355
24. Agüero-Torres H, Fratiglioni L, Guo Z, et al. Dementia is the major cause of functional dependence in the elderly: 3-year follow-up data from a population-based study. Am J Public Health. 1998;88(10):1452–1456. doi:10.2105/AJPH.88.10.1452
25. Lindbergh CA, Dishman RK, Miller LS. Functional disability in mild cognitive impairment: a systematic review and meta-analysis. Neuropsychol Rev. 2016;26:129–159. doi:10.1007/s11065-016-9321-5
26. Lisko I, Kulmala J, Annetorp M, et al. How can dementia and disability be prevented in older adults: where are we today and where are we going? J Intern Med. 2021;289(6):807–830. doi:10.1111/joim.13227
27. Zhang RQ, Tan J, Li FY, et al. Acupuncture for the treatment of obesity in adults: a systematic review and meta-analysis. Postgrad Med J. 2017;93:743–751. doi:10.1136/postgradmedj-2017-134969
28. Zhang M, Zhu Y, Wang J, et al. Association between acupuncture and grade 1 hypertension: a systematic review and meta-analysis. Complement Ther Clin Pract. 2022;49:101649. doi:10.1016/j.ctcp.2022.101649
29. Wang XS, Wang YS, Li JJ, et al. Acupuncture and related therapies for hyperlipidemia: a network meta-analysis. Digit Chin Med. 2020;3:309–326. doi:10.1016/j.dcmed.2020.12.002
30. Chen C, Liu J, Sun M, et al. Acupuncture for type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2019;36:100–112. doi:10.1016/j.ctcp.2019.04.004
31. Lu Y, Chen Y, Huang D, et al. Efficacy of acupuncture for dysphagia after stroke: a systematic review and meta-analysis. Ann Palliat Med. 2021;10(3):3410–3422. doi:10.21037/apm-21-499
32. Dai R, Cao Y, Zhang H, et al. Comparison between acupuncture and nicotine replacement therapies for smoking cessation based on randomized controlled trials: a systematic review and bayesian network meta-analysis. Evid Based Complement Alternat Med. 2021;2021:9997516. doi:10.1155/2021/9997516
33. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
34. Tong P, Dong LP, Yang Y, et al. Traditional Chinese acupuncture and postpartum depression: a systematic review and meta-analysis. J Chin Med Assoc. 2019;82:719–726. doi:10.1097/JCMA.0000000000000140
35. Tong Q-Y, Liu R, Zhang K, et al. Can acupuncture therapy reduce preoperative anxiety? A systematic review and meta-analysis. J Integr Med. 2021;19(1):20–28. doi:10.1016/j.joim.2020.10.007
36. Du SQ, Wang XR, Zhu W, et al. Acupuncture inhibits TXNIP-associated oxidative stress and inflammation to attenuate cognitive impairment in vascular dementia rats. CNS Neurosci Ther. 2018;24:39–46. doi:10.1111/cns.12773
37. Sun W, Zhao Y, Liao L, et al. Effects of acupuncture on age-related macular degeneration: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2023;18:e0283375.
38. Zhang X, Wu B, Nie K, et al. Effects of acupuncture on declined cerebral blood flow, impaired mitochondrial respiratory function and oxidative stress in multi-infarct dementia rats. Neurochem Int. 2014;65:23–29. doi:10.1016/j.neuint.2013.12.004
39. Rodrigues MAP, Facchini LA, Thumé E, et al. Gender and incidence of functional disability in the elderly: a systematic review. Cad Saude Publica. 2009;25(suppl 3):S464–S476. doi:10.1590/S0102-311X2009001500011
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.