")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Real-World Evidence of Aripiprazole Tablets with Sensor: Treatment Patterns and Impacts on Psychiatric Healthcare Resource Utilization
Authors Hadzi Boskovic D, Liang S, Parab P, Wiggins E, Liberman JN
Received 27 January 2023
Accepted for publication 18 May 2023
Published 22 June 2023 Volume 2023:15 Pages 487—498
DOI https://doi.org/10.2147/CEOR.S402357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Dusica Hadzi Boskovic,1 Shuting Liang,2 Purva Parab,2 Emily Wiggins,2 Joshua N Liberman2
1Otsuka Pharmaceutical Development & Commercialization, Inc., Princeton, NJ, USA; 2Health Analytics, LLC, Clarksville, MD, USA
Correspondence: Dusica Hadzi Boskovic, Otsuka Pharmaceutical Development & Commercialization, Inc., 508 Carnegie Center, Princeton, NJ, 08540, USA, Tel +1 6468122719, Email [email protected]
Purpose: Maintaining adherence to antipsychotic (AP) medication is often challenging. Aripiprazole tablets with sensor (AS) contain an ingestible event marker and communicate with wearable patches and a smartphone app to provide objective medication ingestion data. This study evaluated real-world treatment patterns of AS usage and its impact on psychiatric healthcare resource utilization (HCRU).
Patients and Methods: This retrospective, observational cohort study identified individuals who initiated AS between 1/1/2019 and 6/30/2020 with 3 months baseline and 6 months of follow-up data using a commercial medical and pharmacy claims database (Clarivate). Controls were propensity score-matched (4:1) to AS initiators based on age (± 2 years), sex, diagnosis (major depressive disorder [MDD], schizophrenia, bipolar I disorder [BP-I], other), insurance, and baseline oral AP use (yes/no). Days of AP supply were evaluated using a general regression model. The frequency of psychiatric HCRU during follow-up was compared between groups using a zero-inflated regression model.
Results: Most AS initiators were diagnosed with MDD (61.2%) and were women (61.2%); mean age was 37.7 years (standard deviation: 14.1). Most AS initiators (53.1%) continued treatment for > 60 days (mean days of supply = 77). After adjusting for covariates, AS initiators had 41% more days of AP supply during follow-up compared with controls (P < 0.0001) and significantly lower adjusted odds ratios (ORs) for psychiatric outpatient visits (adjusted OR = 0.80; P < 0.05), emergency department visits (adjusted OR = 0.11; P < 0.05), inpatient visits (adjusted OR = 0.42; P < 0.05), and other medical services (adjusted OR = 0.25; P < 0.05).
Conclusion: Participants who implemented AS had significantly more days of AP supply and fewer psychiatric care visits. These preliminary results suggest AS usage can help build regular medication-taking habits and holds promise for reducing psychiatric HCRU. Additional studies with larger sample sizes are warranted to inform clinical practice and coverage decisions.
Keywords: serious mental illness, digital medicine system, digital health, clinical decision-making
Introduction
Adherence to long-term therapy is defined by the World Health Organization as the extent to which an individual’s behavior corresponds with recommendations from a healthcare provider (HCP).1 Medication nonadherence is an ongoing public health concern.2 In a meta-analysis of 569 studies across 17 illnesses, participants took, on average, 75.2% of their prescribed medication doses.3 Individuals living with serious mental illness (SMI) often struggle to take their medication regularly, with nonadherence rates that are equivalent to or worse than nonpsychiatric illnesses.4 Approximately half of patients with SMI, including schizophrenia and affective disorders such as major depressive disorder (MDD) and bipolar I disorder (BP-I) do not adhere to their medication.5–7 For patients with schizophrenia, estimated rates of medication nonadherence range from 34% to 81%.5 For patients with MDD, studies have reported a range of medication nonadherence of 10%–60%.8
Poor medication adherence has both clinical and economic consequences in patients with SMI. Clinically, studies have frequently associated medication nonadherence in individuals with SMI with worse outcomes, such as increased risk of relapse, greater chance of hospitalization and emergency department (ED) visits, increased risk of suicide, and poorer quality of life.7,9–13 For example, among adults with MDD covered by commercial insurance who newly initiated antidepressant therapy, those considered nonadherent (proportion of days covered < 80%) were more likely to have an inpatient hospitalization (incidence rate ratio [IRR] = 1.34; 95% confidence interval [CI] = 1.29–1.39; P <0.001) or an ED visit (IRR = 1.43; 95% CI = 1.40–1.45; P <0.001).14 Similarly, Liu and colleagues (2011) reported a claims-based analysis in which patients with MDD who were adherent to their medication were 17% less likely to have a psychiatric hospitalization and 28% less likely to have a psychiatric ED visit compared with those who were not adherent.15 Patients with bipolar disorder who were nonadherent to their medication were more likely to relapse (hazard ratio [HR] = 2.40; 95% CI = 2.04–2.83; P <0.001), be hospitalized (HR = 2.90; 95% CI = 2.26–3.72; P <0.001), or attempt suicide (HR = 2.82; 95% CI = 1.57–5.06; P <0.001).16 In a 2019 study of patients with schizophrenia, the risk of hospitalization increased nearly linearly as the gap in medication-taking persisted: a gap of 1–10 days was associated with an odds ratio (OR) of 1.98, while the OR for a gap of >30 days was 3.96.11
These negative patient outcomes can carry costly economic consequences. In a systematic review of mental health disorders, inpatient costs represented the largest contribution to the costs of medication nonadherence, with the adjusted cost of nonadherence per person with mental illness ranging from $3252–$19 363 per year.17 Compared with individuals in early episodes of SMI, those recently discharged from a psychiatric hospitalization had higher psychiatric-related healthcare resource utilization (HCRU) and higher annual costs ($15 398 vs $21 171, respectively).18 Conversely, improved medication adherence can help reduce the incidence of negative health outcomes, decrease HCRU, avoid pharmacy costs related to therapy escalation, and prevent the need for increased diagnostic testing due to lack of control of the primary illness.19
A key challenge facing providers and caregivers is the lack of objective measures of medication adherence that can be feasibly implemented in routine clinical practice.20,21 Subjective methods of monitoring adherence are common in current clinical practice, including self-reports (the most frequently used method), pill counting, and HCP assessment.20,22,23 However, subjective methods are often unreliable.20,22 A survey of 64 physicians found that 87.5% reported their psychiatric patients have >50% adherence; however, when their responses were compared with their patients’ medication blood levels, there was poor concurrence between the physician’s estimate and level of medication in the patient’s blood.24 To provide the most informed patient care, providers should ideally verify medication adherence with objective measures.25 Accurate medication adherence data can support providers when making clinical decisions (eg, treatment modification for patients whose symptoms are not well controlled)20,26 and help identify individuals who need additional support with adherence.27
Several advances in technology and medication formulations have emerged to improve the accuracy of determining medication adherence.28 For example, electronic pill bottles and pill organizers can generate date- and time-stamped data when medication is accessed, but do not ensure that a pill is actually ingested.20,27 Serum tests of antipsychotic (AP) levels can provide a readout of medication ingestion but do not record ingestion in real-time.20 In an analysis of interventions to improve medication adherence, those that helped participants overcome attention and memory problems were most likely to report improvements in medication adherence.29 Therefore, digital medicines containing ingestible sensors, which objectively document medication ingestion in real-time, may represent a significant innovation in direct measurement of medication adherence.27 Digital medicine systems enable individuals to view their own ingestion record over time and provide medication reminders.30,31
The aripiprazole tablets with sensor (AS) system32 is one example of this technology. The AS system consists of aripiprazole tablets embedded with an ingestible event marker, wearable patches, and a smartphone app, and is indicated for objectively measuring medication ingestion in adults with schizophrenia, BP-I, or MDD.32 The ingestible event marker embedded within the medication tablet is activated by stomach fluid after ingestion and communicates with the nonmedicated wearable patch.30,33 Users can access their data from a smartphone app, which collects data from the wearable patch, transmits to a secure server and provides summaries of patient data, collects self-reported mood and rest quality, and sends alerts and reminders.30 HCPs and invited members of the individual’s support network can access the individual’s data online through separate portals.33 The AS system provides data on medication ingestion, mood, rest, and activity to support informed treatment discussions and shared decision-making between individuals with SMI and their providers.34,35 It also informs treatment strategies in patients with inadequate treatment response who need medication adjustments versus those who struggle to take their medication.30,35 Prior studies of the AS system reported fewer inpatient hospitalizations of participants with schizophrenia in a clinical trial setting,36 high levels of satisfaction with its usability among most patients34 and providers,35 and low risk of adverse events associated with the technology.33,36 In one study, the AS system generated an adherence metric of ≥80%;33 studies of the ingestible sensor component in other therapeutic areas have reported the accuracy of pill ingestions as ranging from 84%–100% accurate.37 However, real-world evidence is lacking to support coverage decisions or to determine which individuals would benefit most from treatment with AS.
To date, few studies have investigated the AS system in clinical practice. This study was designed to provide preliminary evidence on AS usage and treatment patterns in a real-world clinical practice setting, and to compare psychiatric HCRU among AS initiators and propensity score-matched AP controls.
Materials and Methods
Study Design and Data Source
We conducted a retrospective, observational cohort study comparing AS initiators with propensity score-matched controls in the US. Individuals eligible for the study were identified using a commercially available database licensed from Clarivate (www.clarivate.com/products/real-world-data/), which includes submitted and remitted medical and pharmacy claims but no information on an individual’s insurance benefit eligibility. The study used de-identified data and thus was exempt from Institutional Review Board review, as per the Code of Federal Regulations 45 CFR § 46.104. The research was compliant with the Health Insurance Portability and Accountability Act.
Identification and Selection of Individuals for Study Inclusion
Eligible individuals were aged ≥18 years as of January 1, 2018. The case-finding period spanned from January 1, 2019, to June 30, 2020. Eligible AS initiators included those with an initial paid pharmacy claim for AS (identified using National Drug Codes [NDC] specified in Supplementary Table 1) dispensed by Orsini Specialty Pharmacy (Elk Grove Village, IL, USA), the sole authorized AS distributor (National Council for Prescription Drug Programs identifier: 1477416; National Provider Identifier: 1073608998). Eligible controls included those with a paid pharmacy claim for any non-AS oral AP in the case-finding period. The first fill date within the case-finding period was designated as the index date (ID). The baseline period was defined as 3 months prior to ID, the follow-up period as 6 months after ID. Continuous eligibility was defined by ≥1 medical or pharmacy claim in each quarter of the 3-month baseline period and the subsequent 6-month follow-up period.
Outcome Variables
The primary outcome was psychiatric HCRU in the follow-up period, which included psychiatric ED visits, inpatient admissions, outpatient visits, other medical services, and psychiatric pharmacy claims. Psychiatric medical services utilization was measured by the number of claims per participant per month (PPPM) for outpatient, inpatient, ED, and other medical services visits and defined by claims associated with a psychiatrist (identified using provider taxonomies) or an International Classification of Disease - Tenth Revision - Clinical Modification (ICD-10-CM) diagnosis of “F%” in the primary position. Psychiatric medical services labeled as “other” included behavioral health screening services, independent laboratory services, medication counseling, and emergency medical screening. Psychiatric pharmacy utilization was defined as the number of paid claims PPPM for psychiatric medications identified using the NDC. For AP controls, the proportion of participants with paid pharmacy claims for APs, antidepressants, and anxiolytics was used as a read-out of pharmacy utilization. For AS initiators, utilization measures included days of AP supply dispensed and count of paid AS claims.
Independent Variables
Participant-specific variables included age in years, gender, insurance type (commercial, Medicaid, and Medicare), primary psychiatric diagnoses, and Charlson Comorbidity Index38 (CCI) based on ICD-10 codes.39 Eligible diagnoses included MDD (ICD-10-CM codes: F32.x, F33.x), BP-I (codes: F31.x; excluded F31.81 codes for BP-II), schizophrenia and schizoaffective disorders (codes: F20.x, F25.x), and other diagnoses. CCI was calculated based only on the diagnosed comorbidities and was not adjusted for age. Additional independent variables included baseline AP use (yes/no) and baseline psychiatric HCRU defined by PPPM measures of outpatient, inpatient, and ED visits, other medical services, and pharmacy claims.
Propensity Score Matching
We used a 1-to-many propensity score matching approach for this study; previous studies of this method have reported that increasing the n of untreated controls relative to treated individuals increases precision and decreases variance, but also increases bias.40,41 To maximize precision while minimizing bias, eligible controls were propensity score-matched 4:1 with each AS initiator using a greedy matching approach and maximum allowable distance (caliper) of width = 0.02 standard deviations (SDs) of the logit of the propensity score.41,42 Prior reports have found little benefit to increasing the ratio of untreated controls to treated individuals beyond 4:1, likely due to the increased bias that accompanies larger untreated n.43 Propensity scores were estimated using a logistic regression model with the following variables: age (±2 years), gender, primary diagnosis (schizophrenia, MDD, BP-I, other), insurance type, baseline oral AP use (yes/no), and baseline psychiatric utilization (in PPPM units). Matching was conducted with random selection and without replacement. Differences between individual matching variables were assessed by standardized mean difference (SMD).
Statistical Analyses
Post-matching differences on the independent variables were compared between AS initiators and AP controls using χ²-tests and t-tests for categorical and continuous variables, respectively, at a significance level of 0.05. Unadjusted baseline and follow-up psychiatric utilization (in PPPM units) were compared using t-tests. For adjusted analyses of the frequency of psychiatric utilization, zero-inflated models were used to account for the excessive zeros in each outcome event.44 Each outcome model also controlled for its respective baseline utilization PPPM value (eg, the model for psychiatric ED visits controlled for baseline ED visits PPPM). Covariates were retained in the model using the forward selection method with a retention criterion of P <0.10. Model outcome coefficient estimates were exponentiated to derive adjusted ORs using the constant e (the base of the natural logarithm = 2.178) raised to the power of the exact value of the coefficient. For adjusted analyses of days of AP supply during follow-up, we used a generalized linear model with all independent variables as stated above and baseline days’ AP supply. All data management and statistical analyses were performed with SAS version 9.4 (Cary, NC, USA).
Results
Participant Disposition and Baseline Characteristics
A total of 27 314 140 individuals with ≥1 pharmacy claim between January 1, 2019, and June 30, 2020, were screened (Figure 1). The original pool of AS initiators included 92 individuals who had ≥1 pharmacy claim for AS filled by Orsini Specialty Pharmacy. Of these, 3 were excluded due to being <18 years of age, and 40 were excluded due to a lack of continuous eligibility. A total of 49 individuals were eligible for the AS initiator cohort (Figure 1). Using a 1:4 matching ratio based on propensity scores, 49 AS initiators were matched with 196 individuals from the AP control cohort who had a non-AS oral AP claim within 30 days of the matched case ID (Figure 1). Additional details of the matching process can be found in Material and Methods.
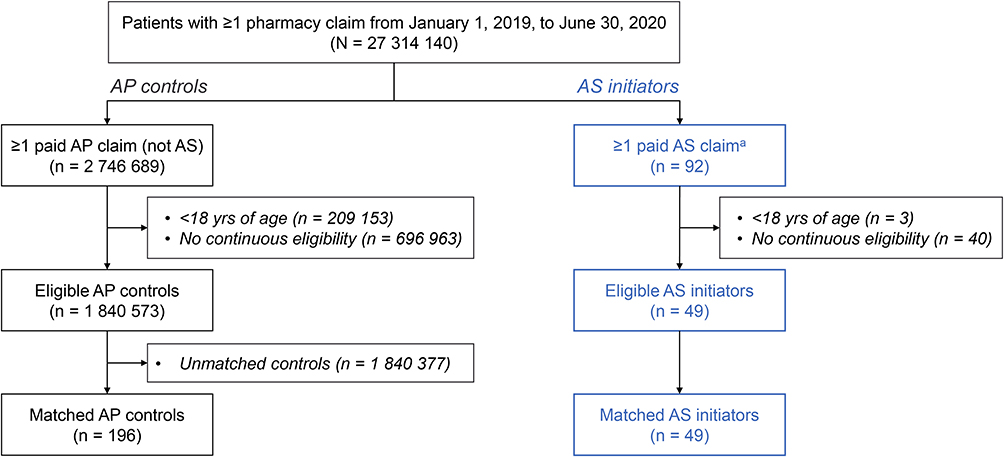 |
Figure 1 Participant disposition. Abbreviations: AP, antipsychotic; AS, aripiprazole tablets with sensor; yrs, years. Notes: aIncluded participants with claims for AS obtained through Orsini Specialty Pharmacy. |
Compared with the AP control population who successfully matched with AS initiators (n = 196), unmatched individuals (n = 1 840 377) were significantly more likely to be women (62.9% vs 60.7%), older (50.1 vs 37.5 years), and insured by Medicaid (64.0% vs 47.1%) or Medicare (20.4% vs 6.1%; P <0.05 for all comparisons). The unmatched individuals were also significantly more likely than AS initiators to have BP-I (15.2% vs 9.6%) or other psychiatric diagnoses (47.6% vs 12.7%) and had significantly higher CCI scores (1.1 vs 0.31; P <0.05 for all comparisons). Unmatched individuals were significantly more likely to use APs at baseline (39.1% vs 30.6%; P <0.05) and had significantly lower baseline psychiatric HCRU (P <0.05).
Most AS initiators were female (61.2%) with an average age of 37.7 years (SD: 14.1) (Table 1). As shown in Table 1, Medicaid was the most common insurance type for AP controls and AS initiators (47.1% vs 49.0%, respectively), followed by commercial insurance (46.2% vs 44.9%, respectively), with Medicare coverage as the least common (6.6% vs 6.1%, respectively). The most common psychiatric diagnosis for AP controls and AS initiators, respectively, was MDD (60.2% vs 61.2%), followed by schizophrenia (14.3% vs 12.2%), BP-I (9.6% vs 10.2%), and other (12.7% vs 12.2%), which included anxiety and post-traumatic stress disorder (Table 1). The mean CCI for AP controls was 0.31 (SD: 0.8) and for AS initiators was 0.45 (SD: 1.1). Baseline psychiatric usage was generally low PPPM, with 4.1%–5.7% of participants from both groups having an outpatient visit or using another medical service in a given month (Table 1). No significant difference was observed between AS initiators and matched controls for all covariates (Table 1).
 |
Table 1 Participant Demographics and Baseline Characteristics |
Utilization of Psychiatric Medications
A total of 60 AP controls (30.6%) had ≥1 paid pharmacy claim for AP at baseline compared with 12 AS initiators (24.5%); AP usage was 100% in both groups during the follow-up period (Table 2). The most common baseline oral AP for AP controls was quetiapine (12.2%) followed by aripiprazole (9.2%; Table 2). For AS initiators, the most common baseline oral AP was aripiprazole (20.4%) followed by risperidone (4.1%). Long-acting-injectable (LAI) AP use was low among both groups, with 4 participants using LAIs in the follow-up period among AP controls and 2 participants among AS initiators using LAIs in both baseline and follow-up periods. A total of 22.4% (n = 11) of AS initiators and 45.9% (n = 90) of AP controls used antidepressant medication at baseline. During follow-up, 16.3% of AS initiators used antidepressants compared with 75.5% of AP controls (P <0.05). Similarly, use of anxiolytics was higher in AP controls versus AS initiators at both baseline (10.7% vs 4.1%, respectively) and in the follow-up period (12.2% vs 2.0%, respectively; Table 2) but these differences did not reach statistical significance.
 |
Table 2 Psychiatric Medication Utilization at Baseline and Follow-Up |
At baseline, controls had a mean AP supply of 11.4 days (SD: 22.9) compared with AS initiators who had a mean AP supply of 7.7 days (SD: 18.7; Table 2). During follow-up, the mean days of AP supply increased to 149.1 days (SD: 58.0) among AS initiators compared with 30.5 days among AP controls (SD: 21.1; unadjusted P <0.0001 for the comparison). After adjusting for baseline days of AP supply and all covariates, AS initiators had 41% more days of AP supply than controls during follow-up (P <0.0001).
Most (n = 48) AS initiators received prescriptions from providers for 30-day supplies of AS, while 1 participant received a prescription for a 60-day supply of AS. As shown in Table 2, AS initiators remained on AS treatment, on average, for approximately 2.5 months (mean days of AS supply = 77.1; SD: 58.1; range: 30–210 days). A total of 26 AS initiators (53.1%) continued therapy beyond 30 days and 17 AS initiators (35.7%) continued beyond 90 days.
Utilization of Psychiatric Medical Services
The unadjusted PPPM frequency of psychiatric service utilization events is shown in Figure 2, while adjusted ORs for these events are shown in Table 3. As shown in Figure 2, the frequency of psychiatric service utilization events at baseline did not significantly differ between AP controls and AS initiators. During the 6-month follow-up period, AS initiators had significantly fewer ED visits compared with AP controls (0.01 vs 0.3 PPPM, respectively) and significantly fewer inpatient admissions (0.1 vs 1.4 PPPM, respectively; P <0.05 for both; Figure 2). AS initiators had significantly increased utilization of other medical services, including behavioral health screening services, independent laboratory services, medication counseling, and emergency medical screening (1.3 services used PPPM) compared with 0.7 services that used PPPM for AP controls (P <0.05; Figure 2). The number of outpatient visits PPPM did not significantly differ between AP controls (3.3 visits) compared with AS initiators (2.8 visits) during the follow-up period. The number of psychiatric pharmacy claims did not significantly differ between groups at either baseline or during the follow-up period.
 |
Table 3 Adjusted Odds Ratios for Psychiatric HCRU Events Using Zero-Inflated Regression Models |
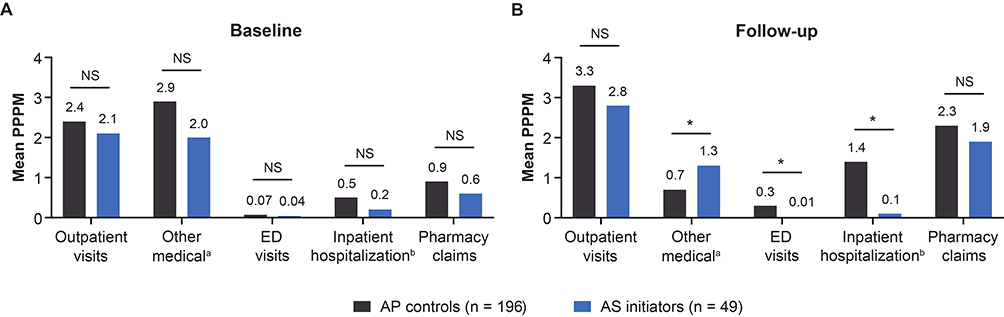 |
Figure 2 Frequency of psychiatric HCRU events at baseline and follow-up (unadjusted results). Abbreviations: AP, antipsychotic; AS, aripiprazole tablets with sensor; ED, emergency department; HCRU, healthcare resource utilization; NS, not significant; PPPM, per participant per month. Notes: (A) Baseline was defined as the 3-month period prior to index date. (B) Follow-up was defined as the 6-month period after index date. aServices provided. bAdmissions. *P <0.05. |
After adjusting for baseline covariates using a zero-inflated regression model, AS initiators had significantly fewer outpatient visits compared with controls (adjusted OR = 0.80, P <0.05) and inpatient admissions (adjusted OR = 0.42; P <0.05; Table 3). AS initiators also had significantly less utilization of other medical services (eg, behavioral health screening services, independent laboratory services, medication counseling, emergency medical screening) compared with AP controls (adjusted OR = 0.25, P <0.05; Table 3). AS initiators were less likely to have ED visits compared with AP controls (adjusted OR = 0.11; P <0.1; Table 3). The adjusted OR for pharmacy claims was 0.86 but did not significantly differ between groups.
Discussion
In this study of AS use in real-world psychiatric clinical practices in the US, more than half of AS initiators continued using the AS system beyond 30 days and almost one-third remained on AS beyond 90 days. Compared with controls who used oral APs, AS initiators had significantly more days of AP supply during the 6-month follow-up period. AS initiators had significantly lower usage of psychiatric acute care services, including both ED visits and inpatient hospitalizations. AS initiators also had significantly fewer outpatient visits and lower utilization of other medical services during the follow-up period compared with controls. While additional studies are needed for validation, these findings may support a role for the AS system in providing objective information to prescribers to guide clinical care strategies.
Iuga and colleagues (2014) developed a conceptual diagram of how medication nonadherence might perpetuate rising healthcare costs.19 In this model, individuals with medication nonadherence often experience poorer health outcomes, resulting in greater HCRU, which leads to higher accrued healthcare costs. These costs can be passed on to the individual with higher copays or increased premiums for employer-provided coverage; indirectly, reduced workplace productivity can also increase costs. These costs can negatively impact adherence, creating a cycle in which medication nonadherence impacts healthcare costs at a societal level.19 This model aligns with the position of the World Health Organization (2003): “Interventions aimed at improving adherence would provide a significant positive return on investment through primary prevention (of risk factors) and secondary prevention of adverse health outcomes.”1
Medication discontinuation is a component of adherence and is unfortunately common among individuals with SMI, with 26%–74% of people discontinuing their medication within the first year after an episode of psychosis.45 In our retrospective analysis of claims data, 53.1% of AS initiators continued therapy beyond 30 days and 35.7% continued beyond 90 days. This finding is notable, given a report by Yan and colleagues (2018), in which time to discontinuation for patients with schizophrenia given oral APs was 89 days and for BP-I was 84 days.46 For patients with MDD who initiated first-line therapy, 49.1% of patients discontinued within the study period, with median time to discontinuation of 161 days.47 In our study, AS initiators had, on average, 149.1 days of AP supply compared with 30.5 days for AP controls. These findings suggest AS may favorably affect medication persistence, defined as individuals continuing to take their medication as prescribed over time.48
Individuals’ medication adherence changes in a home-based setting versus more structured settings.49 The ability to objectively evaluate medication ingestion in individuals in their home environment is one of the benefits of the AS system; this information may help prescribers avoid unnecessary medication augmentation and more rapidly switch ineffective medications.50 In a 2021 publication, an open-label, single-arm, multicenter, phase 4 pragmatic study of the AS system generated a medication ingestion metric over 80%.33 In 2022, a phase 3b, mirror-image clinical trial conducted in adults with schizophrenia with ≥1 hospitalization reported that AS use improved medication ingestion by 26.5 percentage points compared with 3 months before, when the same participants used oral standard-of-care APs (P <0.0001).36 In that study, HCPs most frequently used the AS provider dashboard feature to access ingestion information and missed-dose alerts, which resulted in most HCPs recommending adherence counseling and/or additional education to their patients.35 In another study, when HCPs were given clinical vignettes of patients with schizophrenia, providers whose vignettes contained medication adherence data made different treatment decisions for nonadherent or poorly managed patients compared with providers who did not have that information.26
Medication nonadherence is frequently associated with increased healthcare expenditures and greater HCRU.45,51,52 In a mirror-image clinical study, usage of the AS system in the prospective interventional study phase significantly reduced participant hospitalizations by 21.3% percentage points compared with the retrospective study phase, when study participants had used oral AP (P <0.0001).36 In our study, AS initiators had significantly less usage of psychiatric acute care services (inpatient hospitalization and ED) as well as outpatient visits and other medical services in the 6-month follow-up period compared with AP controls. These data suggest AS may help reduce psychiatric HCRU, which is of high interest to individuals with SMI, their providers, and managed care coordinators.
Interventions aimed at improving the regularity of medication-taking among people with SMI can be effective at reducing hospitalization, one of the leading drivers of direct costs in psychiatric care. A recent meta-analysis of 46 studies found an overall positive effect after 6 months’ treatment with a variety of interventions aimed at improving medication adherence in patients with SMI (OR = 1.33; 95% confidence interval = 1.09–1.62 [P <0.01]).53 However, this effect was largely attenuated by 12 months, suggesting that studies focusing on durability of effect are key to understanding the factors that support sustained medication adherence. Real-world evidence of the patient and provider experience with the AS system will help identify which common barriers impact AS uptake, such as limited access, restricted formularies, switching to different formularies, and the costs of drugs or copayments.54 Studies in larger populations of the technical, clinical, usability, and cost factors are necessary to identify which strategies can help integrate digital technologies like AS into clinical practice.55 Finally, further study of the association between AS use and changes in individuals’ HCRU with a larger study population and longer follow-up is warranted to identify whether specific subpopulations might particularly benefit from the AS system.
Several limitations should be considered when interpreting these results, including the small sample size, heterogeneity of mental illness diagnoses and degree of severity among the study population, and the relatively brief duration of baseline and follow-up periods. These results are subject to the challenges routinely reported with use of administrative claims data,56 which are not collected for research but for reimbursement purposes.57 Primary medication nonadherence (ie, the individual never filled the prescription) is not captured by administrative claims data58 and thus was not measured by our study. Propensity score matching of AP controls and AS initiators did not include baseline use of antidepressant therapy or anxiolytics due to sample size limitations, resulting in mismatch between AP controls’ and AS initiators’ baseline use of these medications, which could introduce biases. Our population of AS initiators was selected by psychiatrists who were early adopters of the technology and may not represent typical use cases. Finally, selecting individuals for whom AS use may be appropriate is influenced by factors not measurable by claims data, including HCP judgment and the individual’s symptom severity.
Conclusion
Our results document the real-world experience of individuals prescribed AS and provide preliminary evidence suggesting those who used AS versus oral AP had more days of AP supply and reduced utilization of psychiatric outpatient services and acute care. While additional studies are needed to validate our findings, these results suggest the AS system may help address care gaps by providing objective medication-taking information to HCPs in real-time. This information can be used to guide more effective clinical care strategies and potentially reduce psychiatric HCRU.
Abbreviations
AP, antipsychotic; AS, aripiprazole tablets with sensor; BP-l, bipolar l disorder; CCI, Charlson Comorbidity Index; ED, emergency department; HCP, healthcare provider; HCRU, healthcare resource utilization; ID, index date; ICD-10-CM; International Classification of Disease-Tenth Revision-Clinical Modification; IRR, incidence rate ratio; LAI, long-acting injectable; MDD, major depressive disorder; NDC, National Drug Codes; OR, odds ratio; PPPM, per participant per month; SD, standard deviation; SMD, standardized mean difference; SMI, serious mental illness; US, United States.
Data Sharing Statement
The data that support the findings of this study are available from Clarivate, but these data are not publicly available. All relevant data are provided within the manuscript.
Acknowledgments
Medical writing support for this manuscript was provided by Shawna Matthews, PhD, of Oxford PharmaGenesis Inc., Newtown, PA, USA, in accordance with Good Publication Practice 2022 guidelines, and was funded by Otsuka Pharmaceutical Development & Commercialization, Inc., Princeton, NJ, USA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Otsuka Pharmaceutical Development & Commercialization, Inc., Princeton, NJ, USA. Medical writing support for this manuscript was funded by Otsuka Pharmaceutical Development & Commercialization, Inc., Princeton, NJ, USA.
Disclosure
DHB is an employee of Otsuka Pharmaceutical Development & Commercialization, Inc. SL, PP, EW, and JNL are employees of Health Analytics, LLC, which received funding from Otsuka to conduct the research. The authors report no other conflicts of interest in this work.
References
1. Adherence to long-term therapies: evidence for action. World Health Organization; 2003. Available from: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf.
2. Lee S, Jiang L, Dowdy D, Hong YA, Ory MG. Attitudes, beliefs, and cost-related medication nonadherence among adults aged 65 or older with chronic diseases. Prev Chronic Dis. 2018;15:E148.
3. DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med Care. 2004;42(3):200–209.
4. Cramer JA, Rosenheck R. Compliance with medication regimens for mental and physical disorders. Psychiatr Serv. 1998;49(2):196–201.
5. Greene M, Yan T, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. J Med Econ. 2018;21(2):127–134.
6. Jawad I, Watson S, Haddad PM, Talbot PS, McAllister-Williams RH. Medication nonadherence in bipolar disorder: a narrative review. Ther Adv Psychopharmacol. 2018;8(12):349–363.
7. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17.
8. Ho SC, Jacob SA, Tangiisuran B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290.
9. Haddad PM, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat Outcome Meas. 2014;5:43–62.
10. Ho SC, Chong HY, Chaiyakunapruk N, Tangiisuran B, Jacob SA. Clinical and economic impact of non-adherence to antidepressants in major depressive disorder: a systematic review. J Affect Disord. 2016;193:1–10. doi:10.1016/j.jad.2015.12.029
11. Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5). doi:10.4088/JCP.IN18031AH1C
12. Desalegn D, Girma S, Abdeta T. Quality of life and its association with current substance use, medication non-adherence and clinical factors of people with schizophrenia in Southwest Ethiopia: a hospital-based cross-sectional study. Health Qual Life Outcomes. 2020;18(1):82.
13. Harvey PD, Kane JM. Addressing patients’ unmet needs to improve outcomes in schizophrenia. J Clin Psychiatry. 2021;82(3):63.
14. Ta JT, Sullivan SD, Tung A, Oliveri D, Gillard P, Devine B. Health care resource utilization and costs associated with nonadherence and nonpersistence to antidepressants in major depressive disorder. J Manag Care Spec Pharm. 2021;27(2):223–239.
15. Liu X, Tepper PG, Able SL. Adherence and persistence with duloxetine and hospital utilization in patients with major depressive disorder. Int Clin Psychopharmacol. 2011;26(3):173–180.
16. Hong J, Reed C, Novick D, Haro JM, Aguado J. Clinical and economic consequences of medication non-adherence in the treatment of patients with a manic/mixed episode of bipolar disorder: results from the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) study. Psychiatry Res. 2011;190(1):110–114.
17. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982.
18. Forma F, Green T, Kim S, Teigland C. Antipsychotic medication adherence and healthcare services utilization in two cohorts of patients with serious mental illness. Clinicoecon Outcomes Res. 2020;12:123–132.
19. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35–44.
20. Shafrin J, May SG, Shrestha A, et al. Access to credible information on schizophrenia patients’ medication adherence by prescribers can change their treatment strategies: evidence from an online survey of providers. Patient Prefer Adherence. 2017;11:1071–1081.
21. Girling C, Packham A, Robinson L, Arden MA, Hind D, Wildman MJ. Implementing the use of objective medication adherence data in routine clinical practice via the digital CFHealthHub platform: situation analysis and strategy development using the theoretical domains framework. Implement Sci Commun. 2022;3(1):12.
22. Byerly M, Fisher R, Whatley K, et al. A comparison of electronic monitoring vs. clinician rating of antipsychotic adherence in outpatients with schizophrenia. Psychiatry Res. 2005;133(2–3):129–133.
23. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482.
24. Martin KB. Accuracy of psychiatrists’ assessment of medication adherence in an outpatient setting. Cureus. 2020;12(12):e11847.
25. Wouters H, Rhebergen D, Vervloet M, et al. Distinct profiles on subjective and objective adherence measures in patients prescribed antidepressants. Drugs. 2019;79(6):647–654.
26. Shafrin J, Schwartz TT, Lakdawalla DN, Forma FM. Estimating the value of new technologies that provide more accurate drug adherence information to providers for their patients with schizophrenia. J Manag Care Spec Pharm. 2016;22(11):1285–1291.
27. Stirratt MJ, Curtis JR, Danila MI, Hansen R, Miller MJ, Gakumo CA. Advancing the science and practice of medication adherence. J Gen Intern Med. 2018;33(2):216–222.
28. Steinkamp JM, Goldblatt N, Borodovsky JT, et al. Technological interventions for medication adherence in adult mental health and substance use disorders: a systematic review. JMIR Ment Health. 2019;6(3):e12493.
29. Barkhof E, Meijer CJ, de Sonneville LM, Linszen DH, de Haan L. Interventions to improve adherence to antipsychotic medication in patients with schizophrenia--a review of the past decade. Eur Psychiatry. 2012;27(1):9–18.
30. Fowler JC, Cope N, Knights J, et al. Hummingbird Study: a study protocol for a multicentre exploratory trial to assess the acceptance and performance of a digital medicine system in adults with schizophrenia, schizoaffective disorder or first-episode psychosis. BMJ Open. 2019;9(6):e025952.
31. Rohatagi S, Profit D, Hatch A, Zhao C, Docherty JP, Peters-Strickland TS. Optimization of a digital medicine system in psychiatry. J Clin Psychiatry. 2016;77(9):e1101–e1107.
32. Otsuka Pharmaceutical Co, Ltd. Abilify MyCite® (aripiprazole tablets with sensor), for oral use [prescribing information]. Tokyo, Japan: Otsuka Pharmaceutical Co, Ltd; 2022. Available from: https://www.otsuka-us.com/sites/g/files/qhldwo7076/files/media/static/ABILIFY-MYCITE-PI.pdf.
33. Fowler JC, Cope N, Knights J, et al. Hummingbird Study: results from an exploratory trial assessing the performance and acceptance of a digital medicine system in adults with schizophrenia, schizoaffective disorder, or first-episode psychosis. Neuropsychiatr Dis Treat. 2021;17:483–492.
34. Cochran JM, Fang H, Le Gallo C, Peters-Strickland T, Lindenmayer JP, Reuteman-Fowler JC. Participant engagement and symptom improvement: aripiprazole tablets with sensor for the treatment of schizophrenia. Patient Prefer Adherence. 2022;16:1805–1817.
35. Cochran JM, Fang H, Sonnenberg JG, Cohen EA, Lindenmayer JP, Reuteman-Fowler JC. Healthcare provider engagement with a novel dashboard for tracking medication ingestion: impact on treatment decisions and clinical assessments for adults with schizophrenia. Neuropsychiatr Dis Treat. 2022;18:1521–1534.
36. Cohen EA, Skubiak T, Hadzi Boskovic D, et al. Phase 3b multicenter, prospective, open-label trial to evaluate the effects of a digital medicine system on inpatient psychiatric hospitalization rates for adults with schizophrenia. J Clin Psychiatry. 2022;83(3):46.
37. Alipour A, Gabrielson S, Patel PB. Ingestible sensors and medication adherence: focus on use in serious mental illness. Pharmacy. 2020;8(2):5867.
38. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
39. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139.
40. Rassen JA, Shelat AA, Myers J, Glynn RJ, Rothman KJ, Schneeweiss S. One-to-many propensity score matching in cohort studies. Pharmacoepidemiol Drug Saf. 2012;21(Suppl 2):69–80.
41. Chen JW, Maldonado DR, Kowalski BL, et al. Best practice guidelines for propensity score methods in medical research: consideration on theory, implementation, and reporting. A Review. Arthroscopy. 2022;38(2):632–642.
42. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–161.
43. Austin PC. Statistical criteria for selecting the optimal number of untreated subjects matched to each treated subject when using many-to-one matching on the propensity score. Am J Epidemiol. 2010;172(9):1092–1097.
44. Feng CX. A comparison of zero-inflated and hurdle models for modeling zero-inflated count data. J Stat Distrib Appl. 2021;8(1):8.
45. Kaplan G, Casoy J, Zummo J. Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Prefer Adherence. 2013;7:1171–1180.
46. Yan T, Greene M, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of aripiprazole once-monthly 400 mg (AOM 400) versus oral antipsychotics in patients with schizophrenia or bipolar i disorder: a real-world study using US claims data. Adv Ther. 2018;35(10):1612–1625.
47. Gauthier G, Guerin A, Zhdanava M, et al. Treatment patterns, healthcare resource utilization, and costs following first-line antidepressant treatment in major depressive disorder: a retrospective US claims database analysis. BMC Psychiatry. 2017;17(1):222.
48. Joe S, Lee JS. Association between non-compliance with psychiatric treatment and non-psychiatric service utilization and costs in patients with schizophrenia and related disorders. BMC Psychiatry. 2016;16(1):444.
49. Mickelson RS, Holden RJ. Medication adherence: staying within the boundaries of safety. Ergonomics. 2018;61(1):82–103.
50. Shafrin J, Bognar K, Everson K, Brauer M, Lakdawalla DN, Forma FM. Does knowledge of patient non-compliance change prescribing behavior in the real world? A claims-based analysis of patients with serious mental illness. Clinicoecon Outcomes Res. 2018;10:573–585.
51. Roebuck MC, Kaestner RJ, Dougherty JS. Impact of medication adherence on health services utilization in Medicaid. Med Care. 2018;56(3):266–273.
52. Broder MS, Greene M, Chang E, Hartry A, Yan T, Yermilov I. Atypical antipsychotic adherence is associated with lower inpatient utilization and cost in bipolar I disorder. J Med Econ. 2019;22(1):63–70.
53. Gonzalez de Leon B, Del Pino-Sedeno T, Serrano-Perez P, Rodriguez Alvarez C, Bejarano-Quisoboni D, Trujillo-Martin MM. Effectiveness of interventions to improve medication adherence in adults with depressive disorders: a meta-analysis. BMC Psychiatry. 2022;22(1):487.
54. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497.
55. Mathews SC, McShea MJ, Hanley CL, Ravitz A, Labrique AB, Cohen AB. Digital health: a path to validation. NPJ Digit Med. 2019;2:38.
56. Norgaard M, Ehrenstein V, Vandenbroucke JP. Confounding in observational studies based on large health care databases: problems and potential solutions - a primer for the clinician. Clin Epidemiol. 2017;9:185–193.
57. Ulrich EH, So G, Zappitelli M, Chanchlani R. A review on the application and limitations of administrative health care data for the study of acute kidney injury epidemiology and outcomes in children. Front Pediatr. 2021;9:742888.
58. Joyce GF. Understanding primary nonadherence. Am J Pharm Benefits. 2010;2(2):111–118.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.