")
Back to Journals » The Application of Clinical Genetics » Volume 17
Preimplantation Genetic Testing for Aneuploidy Could Not Improve Cumulative Live Birth Rate Among 705 Couples with Unexplained Recurrent Implantation Failure
Authors Liu Y, Lan X, Lu J, Zhang Q, Zhou T, Ni T, Yan J
Received 19 October 2023
Accepted for publication 19 January 2024
Published 1 February 2024 Volume 2024:17 Pages 1—13
DOI https://doi.org/10.2147/TACG.S441784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Yang Liu,1– 6,* Xiangxin Lan,1– 6,* Juanjuan Lu,1– 6,* Qian Zhang,1– 6 Tingting Zhou,1– 6 Tianxiang Ni,1– 6 Junhao Yan1– 6
1Center for Reproductive Medicine, Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 2Key Laboratory of Reproductive Endocrinology of Ministry of Education, Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 3Shandong Key Laboratory of Reproductive Medicine, Jinan, Shandong, 250012, People’s Republic of China; 4Shandong Provincial Clinical Research Center for Reproductive Health, Jinan, Shandong, 250012, People’s Republic of China; 5Shandong Technology Innovation Center for Reproductive Health, Jinan, Shandong, 250012, People’s Republic of China; 6National Research Center for Assisted Reproductive Technology and Reproductive Genetics, Shandong University, Jinan, Shandong, 250012, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tianxiang Ni; Junhao Yan, Center for Reproductive Medicine, Shandong University, Jinan, People’s Republic of China, Tel +0531-85651172, Email [email protected]; [email protected]
Objective: We evaluate whether next-generation sequencing (NGS)-based preimplantation genetic testing for aneuploidy (PGT-A) improves the cumulative pregnancy outcomes of patients with unexplained recurrent implantation failure (uRIF) as compared to conventional in vitro fertilization or intracytoplasmic sperm injection (IVF/ICSI).
Patients and Methods: This was a retrospective cohort study (2015– 2022). A total of 705 couples diagnosed with uRIF were included in the study. 229 women transferred blastocysts based on morphological grading (IVF/ICSI) and 476 couples opted for PGT-A to screen blastocysts by NGS. Women were further stratified according to age at retrieval (< 38 years and ≥ 38 years). The primary outcome was the cumulative live-birth rate after all the embryos were transferred in a single oocyte retrieval or until achieving a live birth. Confounders were adjusted using binary logistic regression models.
Results: Cumulative live-birth rate was similar between the IVF/ICSI group and the PGT-A group after stratified by age: IVF/ICSI vs PGT-A in the < 38 years subgroup (49.7% vs 57.7%, adjusted OR (95% CI) = 1.25 (0.84– 1.84), P = 0.270) and in the ≥ 38 years subgroup (14.0% vs 19.5%, adjusted OR (95% CI) = 1.09 (0.41– 2.92), P = 0.866), respectively. Nonetheless, the PGT group had a lower first-time biochemical pregnancy loss rate (17.0% vs 8.7%, P = 0.034) and a higher cumulative good birth outcome rate (35.2% vs 46.4%, P = 0.014) than the IVF/ICSI group in the < 38 years subgroup. Other pregnancy outcomes after the initial embryo transfer and multiple transfers following a single oocyte retrieval were all similar between groups.
Conclusion: Our results showed no evidence of favorable effects of PGT-A treatment on improving the cumulative live birth rate in uRIF couples regardless of maternal age. Use of PGT-A in the < 38 years uRIF patients would help to decrease the first-time biochemical pregnancy loss and increase the cumulative good birth outcome.
Keywords: preimplantation genetic testing for aneuploidy, unexplained recurrent implantation failure, cumulative live-birth rate, cumulative good birth outcome
Introduction
In recent years, an increasing number of infertile couples have the opportunity to achieve fertility wishes through in vitro fertilization and embryo transfer (IVF-ET) technology.1 However, there are still 50%-60% of patients who are unable to achieve pregnancy due to embryo implantation failure.2 Recurrent implantation failure (RIF) is defined as the implantation failure after multiple embryo transfers with good quality.3,4 The etiology of RIF is complex and primarily involves gamete or embryo quality and its development potential, endometrial microenvironment, immunological mechanism, prethrombotic state, and other aspects.5,6 After ruling out the above common etiologies, there are still some patients undergoing RIF with unknown reasons, defined as unexplained RIF (uRIF).
uRIF is considered as a great challenge for the advancement of assisted reproductive technologies. Studies have demonstrated that embryo aneuploidy is the main reason for miscarriage or implantation failure,7,8 which is more common in couples with advanced maternal age (AMA). It is evidenced that the embryo aneuploidy rate among RIF patients ranged from 43% to 58%,9–11 even as high as 79%.12 Considering the increased risk of embryo aneuploidy, RIF has been listed as one of the most common indications for preimplantation genetic testing for aneuploidies (PGT-A) worldwide.13–15 Although PGT-A is a potential technique for improving pregnancy outcomes by screening out euploid embryos, there is currently no consensus on its application. According to the American Society of Reproductive Medicine (ASRM), it is not recommended to use PGT-A as a routine pregnancy aid for all infertile women.16 Recently, a large clinical trial found no difference in cumulative live-birth rate between PGT-A and conventional IVF in good-prognosis population.17
For RIF patients, there are currently limited studies evaluating the application values of PGT-A and the findings are inconsistent. Two retrospective cohort studies by Greco et al in 2014 and Du et al in 2023 analyzed the pregnancy outcomes with or without PGT-A among young RIF women, and both found that the clinical pregnancy rate after PGT-A was significantly increased, without reporting live birth rate.10,18 Two small-size studies among RIF women, one was retrospected by Pantou et al with young female age in 2022 and another was prospective multicentered by Sato et al with advanced female age in 2019, both found that live birth rate per embryo transfer after PGT-A was significantly increased, but the live birth rate per patient was not significantly improved.11,12 These studies only included a single embryo transfer cycle, evaluated the efficacy of PGT-A in terms of pregnancy outcome per transfer with a small sample size, which is not fully relevant in clinical practice.
Therefore, there is currently insufficient evidence to prove the effectiveness of PGT-A in uRIF patients. Researches with a larger study population on cumulative live birth outcomes are still needed. In this study, our objective was to compare the cumulative live birth rate and other cumulative pregnancy outcomes with or without PGT-A among uRIF women, as well as pregnancy outcomes after the initial embryo transfer.
Materials and Methods
Study Population
This study included 705 uRIF couples, who underwent one or more oocytes retrieval cycles from January 2015 to January 2022 at the Reproductive center of Shandong University. uRIF was defined as recurrent implantation failure without known etiologies of RIF after ≥3 times embryo transfers, or after transferred ≥4–6 good-quality cleavage-stage embryos or ≥3 good-quality blastocysts. Exclusion criteria included parental chromosomal abnormalities, uterine anatomical abnormalities, endocrine dysfunction, autoimmune disorders, thrombosis, infection, use of donated oocytes or sperm, and use genetic testing other than PGT-A. Patients were divided into the PGT-A group and the conventional IVF/ICSI group based on whether they received PGT-A in the research cycle. The first oocyte retrieval cycle after uRIF diagnosis with frozen blastocyst transfers was included in the study, with all the acquired embryos transferred or until a live birth was achieved.
Ovarian Stimulation and Embryo Culture
Appropriate ovarian stimulation regimens were applied to each patient based on female age, ovarian reserve function, and previous responses to gonadotropins. The ovarian stimulation protocols including super-long, long, short gonadotropin-releasing hormone (GnRH) agonists, antagonists, and other protocols used in our center, which had been described in detail in previous studies.17,19 When at least two follicles with a diameter of ≥18 mm were observed, human chorionic gonadotropin (hCG) (Pregnyl, Livzon, Guangdong, China) was administered to trigger final maturation of oocytes. After 34 to 36 hr, oocytes were retrieved through ultrasound-guided transvaginal aspiration.
Patients in the PGT-A group were fertilized using ICSI. The IVF/ICSI group patients underwent IVF or ICSI based on the semen quality of their male partners. Embryos were cultured in sequential culture media, with G1-PLUS (Vitrolife) from fertilization to Day 2 or Day 3 and then with G2-PLUS (Vitrolife) to Day 5/Day 6/Day 7. All embryos were cultured to the blastocyst stage.
Preimplantation Genetic Testing for Aneuploidy
According to Gardner criteria,20 the blastocysts were morphologically scored based on three components: blastocyst expansion, inner cell mass, and trophectoderm development. For blastocysts with score 4BC or better on Day 5 of embryo culture, trophectoderm biopsy was performed with the laser method. 3–5 trophectoderm cells were aspirated and detached from the blastocyst. Next, the aggregates of trophectoderm cells were placed intact into a PCR tube after several washes through hypotonic solution. The operation procedure of NGS followed instructions by manufacturers. Euploid embryos were selected for subsequent transfer.
Endometrial Preparation and Luteal-Phase Support
Single frozen embryo transfer was performed after at least two menstrual cycles after oocyte retrieval. Endometrial preparation regimens included natural ovulation cycle, ovulation induction cycle, and programmed cycle, as previous reported.21 The luteal-phase supports including dydrogesterone and vaginal progesterone gel et al were given on the endometrial transformation day and continued until 12 weeks of gestation. The level of serum hCG was measured 2 weeks after transfer to confirm conception. Transvaginal ultrasonography was performed 3 weeks later to confirm clinical pregnancy, which was defined as the detection of an intrauterine gestational sac. Ultrasonography was repeated at 12 weeks of gestation to confirm ongoing pregnancy.
Outcomes and Definitions
The primary outcome was cumulative live birth rate following a single oocyte retrieval. Other pregnancy outcomes included cumulative rates of good birth outcome, biochemical, clinical, and ongoing pregnancy, and pregnancy loss after all embryo transfer cycles following a single oocyte retrieval, as well as rates of biochemical, clinical, and ongoing pregnancy, and pregnancy loss after the initial embryo transfer. Live birth was defined as the delivery of a live-born infant at ≥28 weeks of gestation after embryo transfer. The cumulative live birth rate was calculated by dividing the number of women who had a live birth after 28 weeks of gestation by the total number of women in the PGT-A or IVF/ICSI group. A good birth outcome was defined as a live birth at ≥37 weeks of gestation, with a birth weight between 2500 and 4000 g and without a major congenital anomaly.22 Time to reach live birth was evaluated by comparison of time length from oocyte retrieval to achieving live birth. Definitions of other pregnancy outcomes were described previously.19
Statistical Analysis
Stratified analysis was performed according to female age (<38 years and ≥38 years) in this study, taking into account the fact that maternal age has a significant effect on embryo euploidy.23,24 Continuous variables were described using mean and standard deviation (SD) or median and interquartile range, according to their data distribution, with the difference determined by Student’s t test and Mann–Whitney U-test. Categorical variables were represented using counts and percentages and compared with the chi-square test or Fisher's exact test.
Adjusted analyses for the primary outcome of cumulative live birth rate and good birth outcome rate were performed using a binary logistic regression model to estimate odds ratios (ORs) with corresponding 95% confidence intervals (CIs), considering potential confounders that were not fully balanced and prespecified as P < 0.05 for baseline comparisons between groups. These potential confounders included age, body mass index (BMI), anti-Mullerian hormone (AMH), endometrial thickness, and previous embryo transfers. Forest maps were conducted using the website www.bioinformatics.com.cn.
Overall, P < 0.05 was considered statistically significant. All the statistical analyses were performed with SPSS version 26.0 software.
Results
The Baseline Characteristics of uRIF Couples
A total of 705 couples diagnosed with uRIF were included in the study, of which, 476 underwent PGT-A (343 in <38 years subgroup, 133 in ≥38 years subgroup), and 229 who did not opt for PGT-A were considered as IVF/ICSI controls (179 in <38 years subgroup, 50 in ≥38 years subgroup). Most of the baseline characteristics were comparable between PGT-A and IVF/ICSI groups in two age subgroups (Table 1). In women <38 years old, the PGT-A group had less previous embryo transfer cycles (4.10±1.41 vs 3.61±1.96, P = 0.001), and a higher level of AMH (1.32 (1.32, 3.36) vs 2.69 (1.45, 4.68), P < 0.001). In women ≥38 years old, the PGT-A group had a higher number of antral follicles in both ovaries (7.0 (3.0, 10.0) vs 10.0 (6.0, 13.0), P = 0.016) and a thicker endometrium (0.69±0.20 vs 0.77±0.25, P = 0.029).
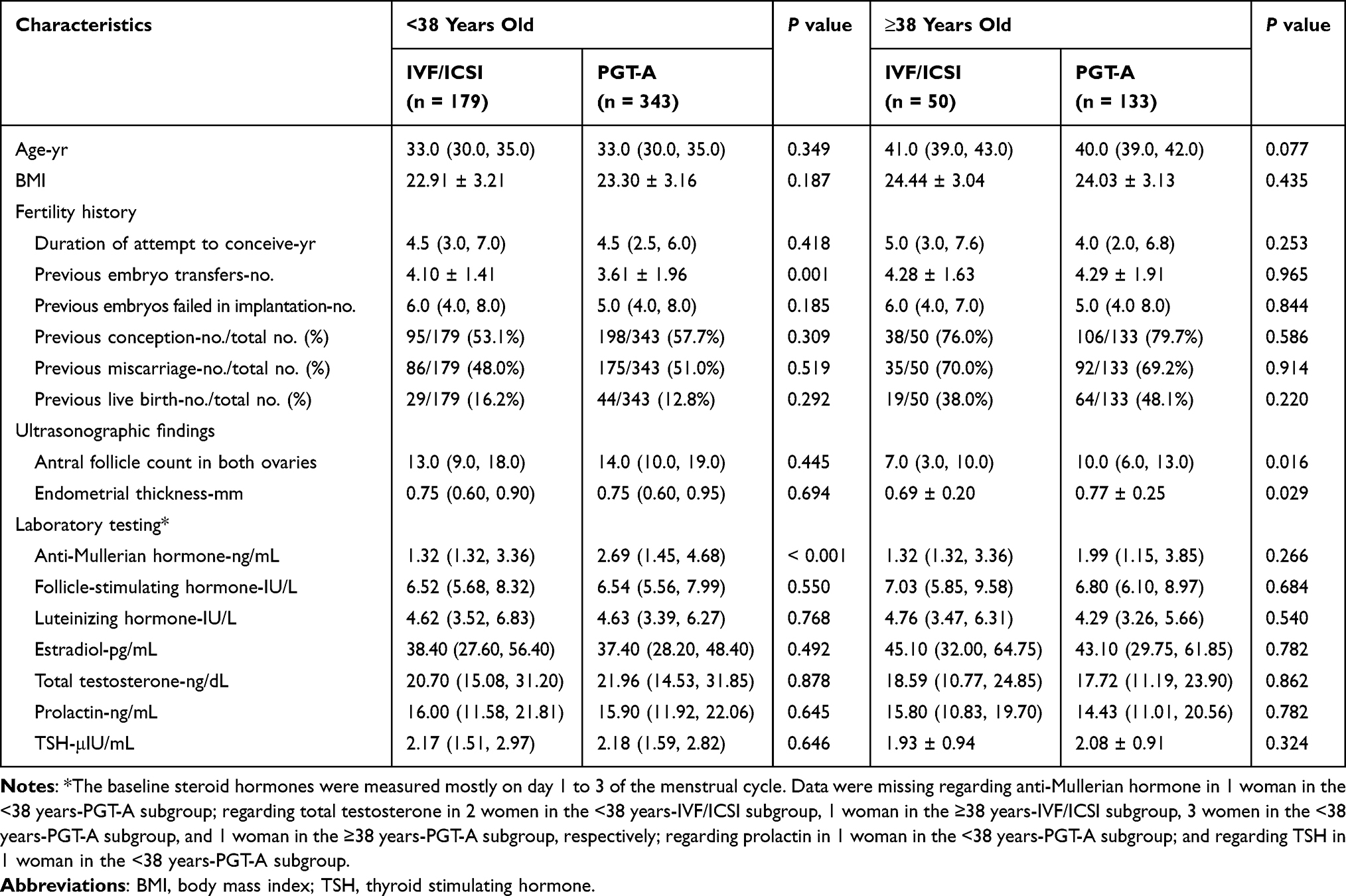 |
Table 1 Characteristics of Patients at Baseline |
Results of Ovarian Stimulation and Embryo Culture
Information on oocyte retrieval and embryo development is shown in Table 2. Couples in the PGT-A group had more good-quality embryos on day 5 or 6 in both <38 years subgroup (3.0 (2.0, 5.0) vs 4.0 (3.0, 7.0), P < 0.001) and ≥38 years subgroup (2.0 (1.0, 2.0) vs 2.0 (1.0, 3.5), P = 0.002) compared with IVF/ICSI group. In the ≥38 years subgroup, the number of large follicles above 14cm (4.0 (3.0, 7.0) vs 7.0 (5.0, 9.0), P = 0.001) and estradiol level (1590.00 (697.58, 2119.00) vs 2141.00 (1399.00, 2926.00), P = 0.001) on hCG trigger day were both lower in the IVF/ICSI group than in the PGT-A group. The embryo euploidy rate was 51.2% in the <38 years subgroup and 30.5% in the ≥38 years subgroup. 17.5% (60/343) couples in the <38 years subgroup did not screen out euploid embryos, while it was as high as 59.4% (79/133) in the ≥38 years subgroup. Notably, 19.8% (165/834) embryos in the <38 years and 9.9% (35/354) embryos in the ≥38 years subgroup were tested to be chromosomal mosaic. According to safety factors, mosaicisms are not recommended for transfer in our center. However, in this study, 44 women did not obtain euploid embryos, while they had mosaic embryos. Eighteen of them requested to transfer mosaic embryos and ended up with two preterm birth and four full-term deliveries (all six live births were in the <38 years subgroup).
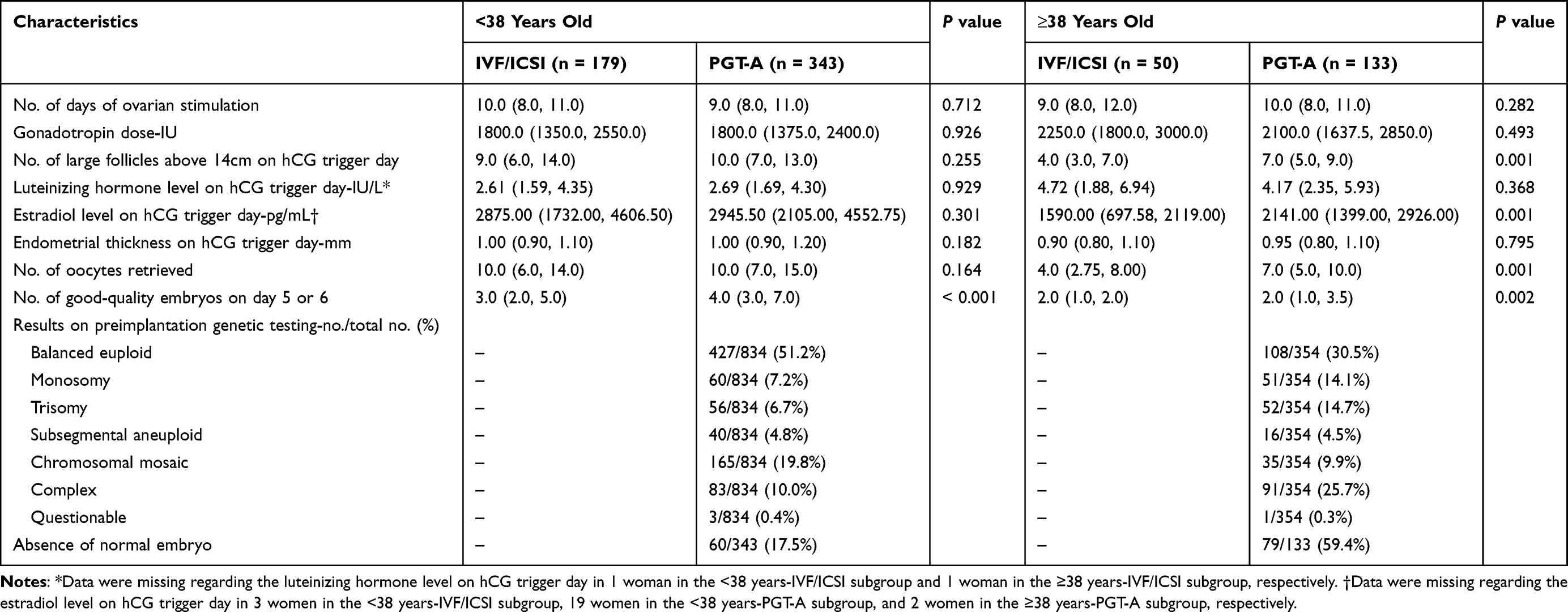 |
Table 2 Outcomes of Controlled Ovarian Hyperstimulation |
Pregnancy Outcomes and Neonatal Complications Between Groups
Among <38 years subgroup, 283 women had 251 embryos transferred in 378 transfer cycles. The cumulative rates of live birth (49.7% in the IVF/ICSI group vs 57.7% in the PGT-A group, P = 0.081) and clinical pregnancy loss (16.8% in the IVF/ICSI group vs 11.1% in the PGT-A group, P = 0.133) were similar between the two groups. Nevertheless, the cumulative rate of good birth outcome (35.2% vs 46.4%, P = 0.014) was higher in the PGT-A group compared with the IVF/ICSI group. The first-time biochemical pregnancy loss rate (17.0% vs 8.7%, P = 0.034) was lower in the PGT-A group compared with the IVF/ICSI group. In addition, there were no significant differences in pregnancy outcomes after the initial transfer between groups (Table 3). Among ≥38 years subgroup, 54 women underwent 67 transfer cycles of single frozen embryo. There was no significant difference between IVF/ICSI and PGT-A group in cumulative rates of live birth (14.0% in the IVF/ICSI group vs 19.5% in the PGT-A group, P = 0.384) or clinical pregnancy loss (38.9% in the IVF/ICSI group vs 22.2% in the PGT-A group, P = 0.197). Other pregnancy outcomes after the first embryo transfer or following a single oocyte retrieval were also similar between IVF/ICSI and PGT-A groups (Table 3). We have plotted Figure 1 to show overall pregnancy outcomes and the changing trends with pregnancy course across study groups. Pregnancy outcomes were universally better in the <38 years subgroup. Biochemical pregnancy, clinical pregnancy, ongoing pregnancy, and live-birth rate decrease gradually with pregnancy course. As shown by the yellow dotted lines, both the first-time live birth rate and the cumulative live birth rate tend to be lower in the IVF/ICSI group and decrease with increasing age.
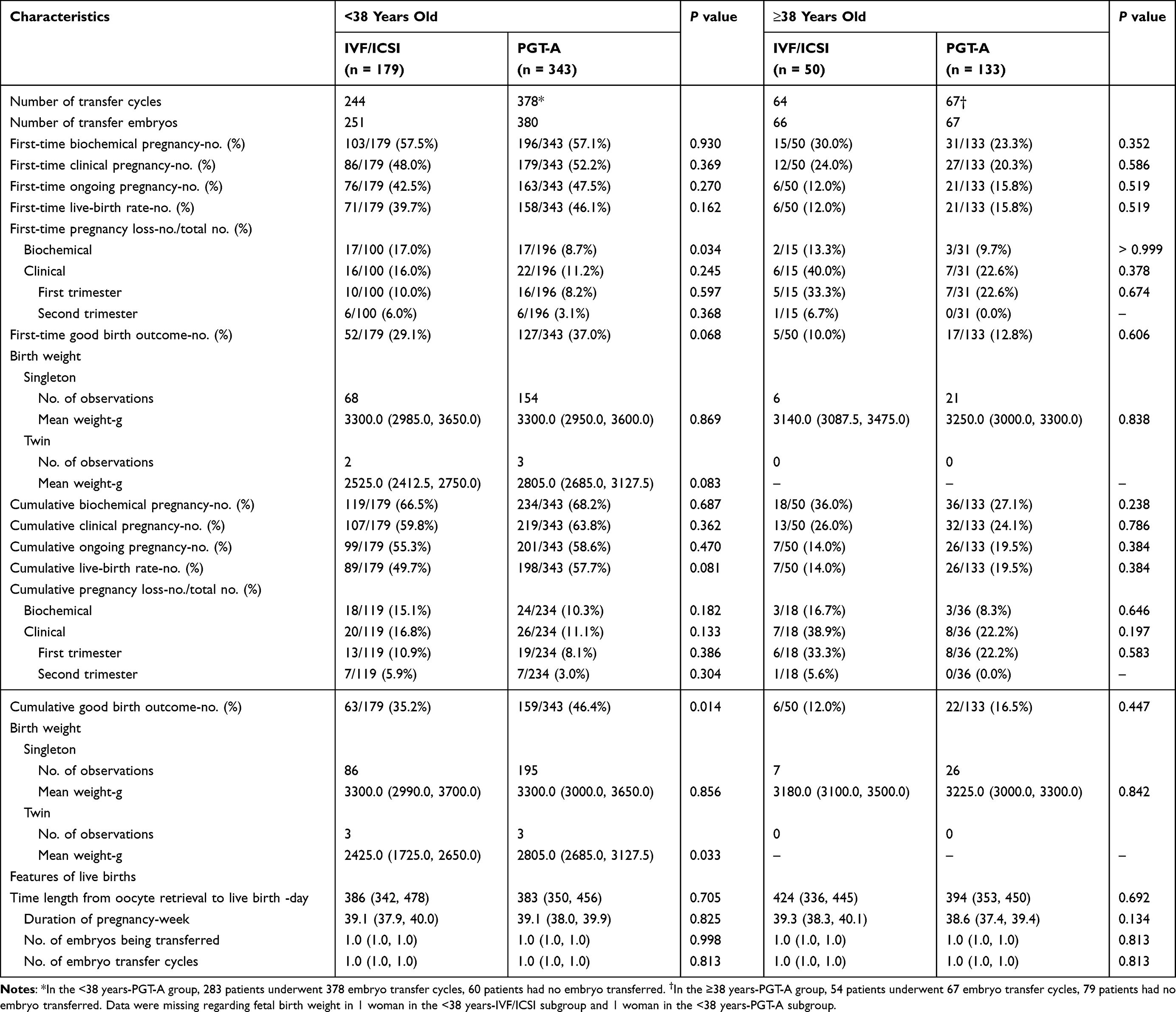 |
Table 3 Cumulative Live-Birth Rate and Secondary Outcomes |
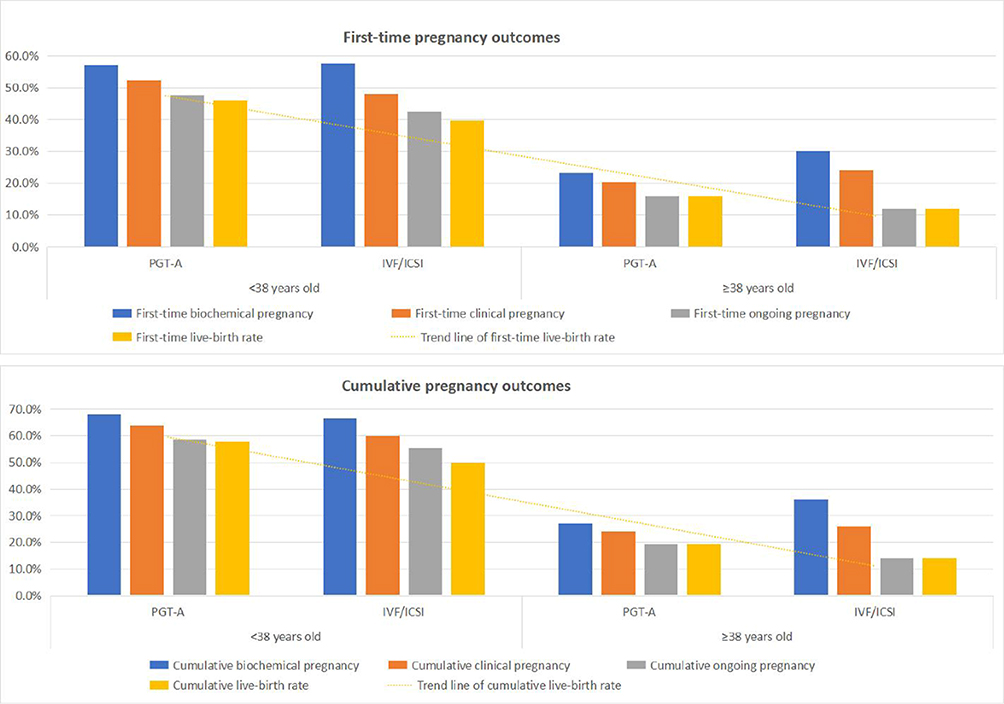 |
Figure 1 Overall pregnancy outcomes and the changing trends with pregnancy course across study groups. |
In addition, to clarify whether PGT-A application would reduce the time to achieve live birth, we compared the time length from oocyte retrieval to live birth between IVF/ICSI and PGT-A. The results showed no significant difference between groups no matter in the <38 years or ≥38 years subgroups. The number of embryos and transfer cycles needed for achieving live birth were also similar between groups (Table 3). Regarding pregnancy and neonatal complications, the incidence of gestational hypertension, diabetes and other obstetric or perinatal complications were all similar between the two groups (Table 4).
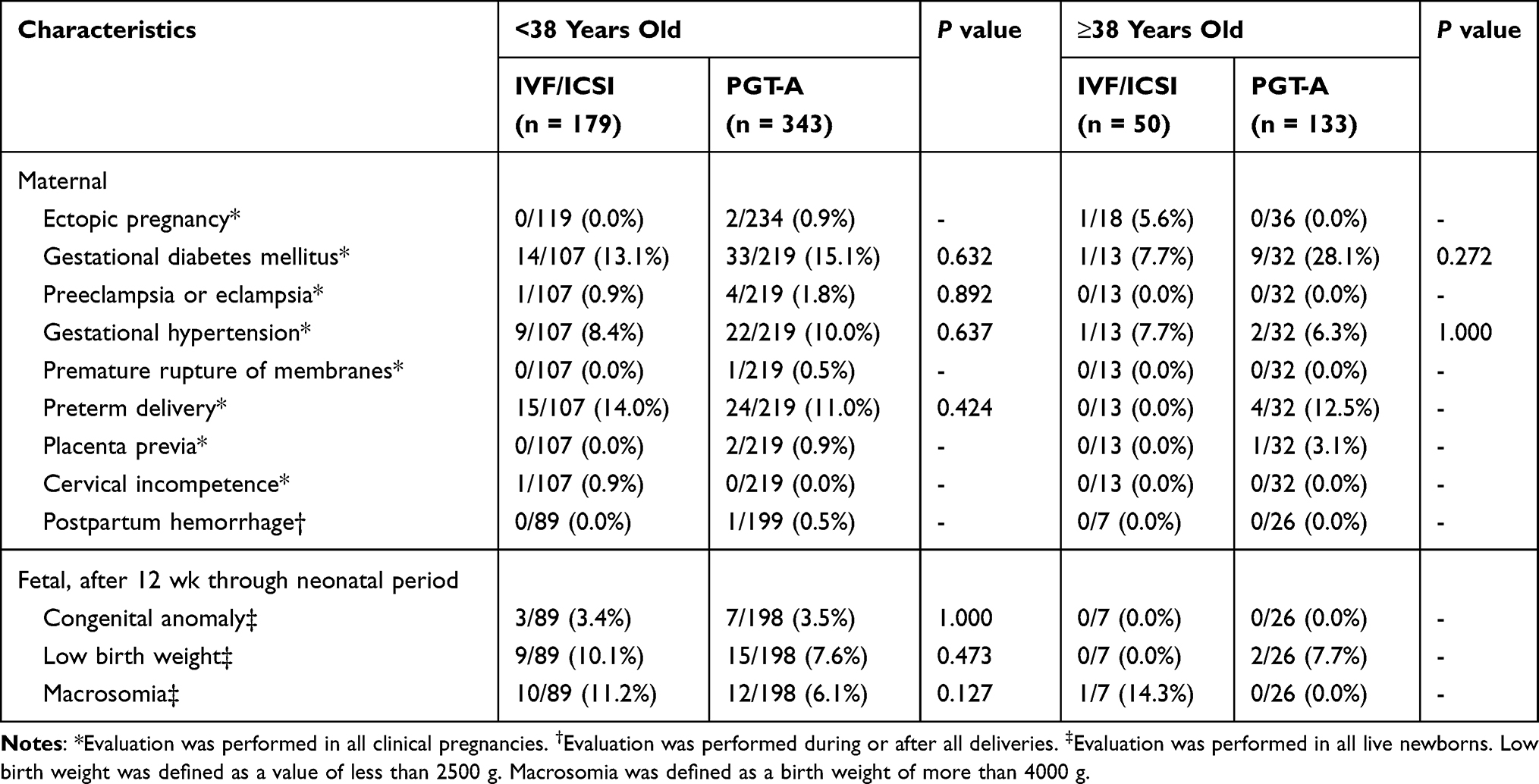 |
Table 4 Adverse Events |
Logistic Regression Analysis of Cumulative Live Birth Rate and Good Birth Outcome
To exclude the impact of confounding factors and interactions, we employed the binary logistic regression model, which is widely used to calculate odds ratio and adjust risk factors.25 In women both aged <38 years and aged ≥38 years, after adjusting for confounding factors, including maternal age, BMI, AMH, the number of previous transfer cycles, and endometrial thickness, there was no association found by the logistic regression analysis between PGT-A treatment and cumulative live birth rate or good birth outcome rate (Figures 2 and 3, Supplemental Tables 1 and 2). Higher AMH levels and lower ages were associated with cumulative live birth rate and good birth outcome rate.
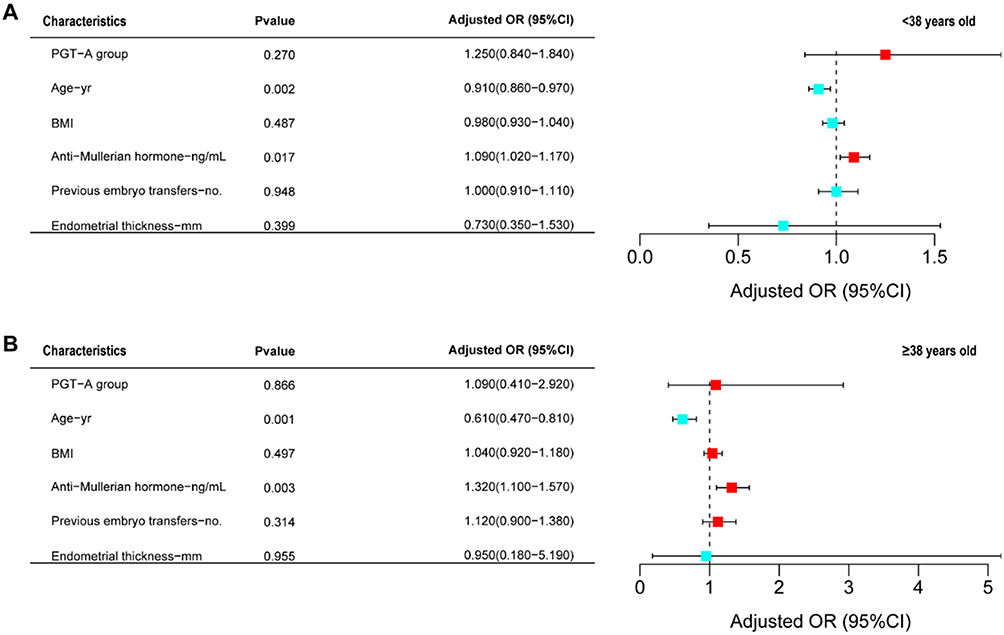 |
Figure 2 Logistic regression models showing variables independently associated with in cumulative live-birth rate. The forest map represents the odd ratios of logistic regression analysis for cumulative live-birth rate in <38 years old group (A) and ≥38 years old group (B). Adjusted ORs were assessed by binary logistic regression adjusting for age, BMI, AMH, endometrial thickness, and previous embryo transfers. The squares and horizontal lines indicate the adjusted ORs and 95% CIs. |
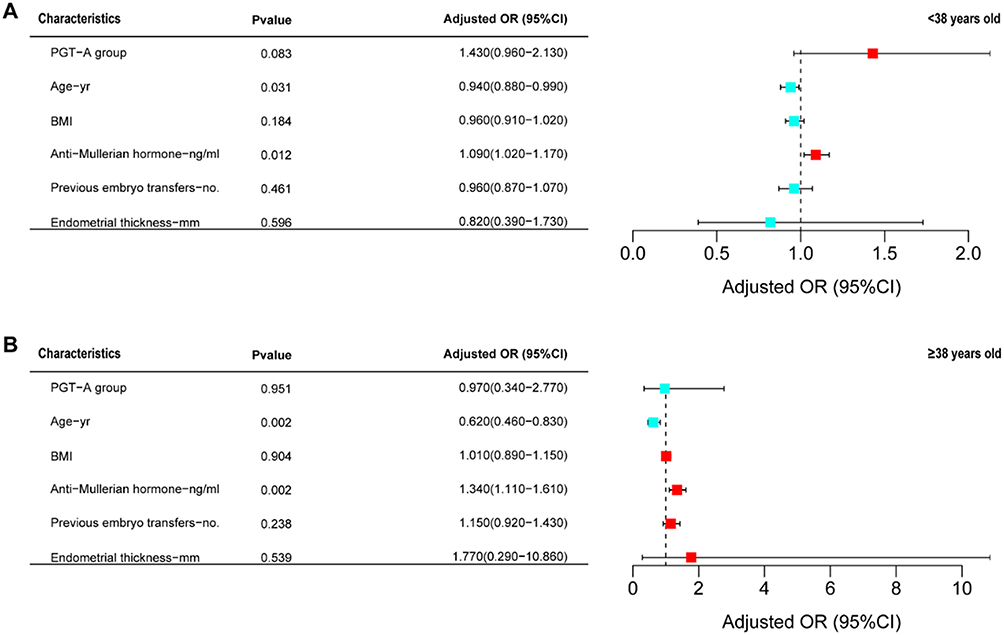 |
Figure 3 Logistic regression models showing variables independently associated with cumulative good birth outcome. The forest map represents the odd ratios of logistic regression analysis for cumulative good birth outcome in <38 years old group (A) and ≥38 years old group (B). Adjusted ORs were assessed by binary logistic regression adjusting for age, BMI, AMH, endometrial thickness, and previous embryo transfers. The squares and horizontal lines indicate the adjusted ORs and 95% CIs. |
Discussion
This study included 705 uRIF couples across more than 7 years and for the first time comprehensively investigated the efficacy of PGT-A on the cumulative live birth rate after frozen embryo transfer cycles following a single oocyte retrieval. The female age ranged from 24 to 48 years. Our results showed no evidence of favorable effects of PGT-A treatment on improving the cumulative live birth rate in uRIF couples regardless of maternal age (<38 years or ≥38 years). However, the cumulative rate of good birth outcome was higher after PGT-A among women aged <38 years old.
We chose cumulative live birth rate after a given oocyte-retrieval cycle as the primary outcome, which could fully reflect the final treatment outcome of a treatment cycle and was considered as the most important patient-centered outcome for evaluating IVF success.12 In most previous studies, clinical pregnancy rate or ongoing pregnancy rate or live birth rate per embryo transfer were used as the primary outcome to demonstrate a beneficial effect of PGT-A for RIF.10,11,18,26 However, these outcome measures have not taken into account patients who do not obtain transferable euploid embryos after PGT-A and could not reflect the impact of discarding embryos that may have live-birth potential but have been diagnosed with false aneuploidy or mosaicism.17 Note that our results showed that the cumulative live birth rate of uRIF couples after PGT-A was comparable to that of IVF/ICSI.
The main possible explanations for the ineffectiveness of PGT-A were the high mosaicism proportion and the unavoidable false-positive results from trophectoderm biopsies, which led to much waste of viable embryos.27 It is reported that the incidence of embryo mosaicism is estimated to be 3–20% by trophectoderm biopsy.28 Some previous studies indicated that mosaic embryos may have the potential to develop into chromosomally normal newborns, resulting in a live-birth rate of 30% to 47%.29–31 As shown in our results, there were 18 women request for transfer of mosaic embryos and 6 women achieved live births after transfer of mosaic embryos. However, mosaic embryos were not recommended to transfer for safety concern in our center. Furthermore, possible harm for embryo development and implantation potential caused by trophectoderm biopsies was another important reason.32
Due to lack of euploid embryos, there were totally 60/343 (17.5%) of women aged <38 years who had no embryos transferred, while the proportion was as high as 79/133 (59.4%) among women aged ≥38 years in this study. The condition that a proportion of PGT-A patients having no euploid embryos to transfer was also the reason for the discrepancy between the increased live birth rate per transfer and the unimproved live birth rate per patient reported by the retrospective study by Pantou et al and the multicenter, prospective study by Sato et al11,12 Consistently, our study also showed that the live birth rate after the first embryo transfer per patient was comparable with or without PGT-A regardless of maternal age (<38 years or ≥38 years).
Nonetheless, the PGT-A group had a lower first-time biochemical pregnancy loss rate and a higher cumulative good birth outcome rate among women aged <38 years. First-time biochemical pregnancy loss and good birth outcome have not been reported by previous studies as indicators for the assessment of PGT-A for RIF. This means that PGT-A technology might do a better job of selecting embryos with the viability of successfully getting through the whole pregnancy procedure and achieving a good birth outcome. Moreover, blank skipped transfer cycles due to screening out aneuploid embryos would reduce the physical and psychological harm on women from possible pregnancy failure, which are important factors for later obtaining of a good birth outcome.
The effectiveness of PGT-A in the ≥38 years group is significantly undermined due to low oocyte acquisition, high aneuploidy and mosaicism rate, and consequently a lot of women have no embryos available for transfer. Consistent with our findings, two trials targeting AMA couples also found no improvement in the cumulative live birth rate after PGT-A.33,34
The strengths of the present study are as follows: First, the sample size is large, including 476 couples with PGT-A and 229 with conventional IVF/ICSI. Second, we performed stratified analysis according to female age and chose the appropriate outcome measures-the live birth rate and good birth outcome following a single oocyte retrieval cycle as well as those following the first embryo transfer cycle, which were more clinically relevant. Moreover, we established strict inclusion and exclusion criteria. For example, we included the first oocyte retrieval cycle after diagnosis of uRIF to eliminate confounding effects. The limitation of this study was its retrospective nature; therefore, not all variables were under control. The administration of PGT-A was optional and not randomized.
Conclusions
The cumulative live birth rate of uRIF patients is comparable between IVF/ICSI and PGT-A regardless of maternal age. PGT-A benefitted younger uRIF patients (aged <38 years) with a higher cumulative good birth outcome rate than IVF/ICSI in this study. Our findings would give recommendations for genetic counseling practice in clinics for RIF couples. PGT-A should be applied with caution. High-quality randomized clinical trials are needed to find patients with indications that may benefit from PGT-A.
Ethical Statements
Our study was approved by the Institutional Review Board of Reproduction Medicine of Center for Reproductive Medicine, Shandong University (IRB No.140). Data collection followed the Declaration of Helsinki and had obtained informed consent from the participants.
Acknowledgments
This study was funded by National Key Research and Development Program (2021YFC2700604, 2022YFC2703202), Shandong Provincial Key Research and Development Program (2021LCZX02), General Program of National Natural Science Foundation of China (82171648), Taishan Scholars Program for Young Experts of Shandong Province (tsqn201812154), Taishan Scholars Program for Young Experts of Shandong Province (tsqn202312388), Youth Program of Shandong Provincial Natural Science Foundation of China (ZR2021QH075), and General Program of Shandong Provincial Natural Science Foundation of China (ZR2022MH087) for data fee (scientific research informed consent, etc.), paper modification, publication fee, and so on.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Calhaz-Jorge C, De Geyter C, Kupka MS, et al. Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE†. Hum Reprod. 2017;32(10):1957–1973. doi:10.1093/humrep/dex264
2. Wei D, Liu JY, Sun Y, et al. Frozen versus fresh single blastocyst transfer in ovulatory women: a multicentre, randomised controlled trial. Lancet. 2019;393(10178):1310–1318. doi:10.1016/s0140-6736(18)32843-5
3. Thornhill AR, deDie-Smulders CE, Geraedts JP, et al. ESHRE PGD Consortium ‘Best practice guidelines for clinical preimplantation genetic diagnosis (PGD) and preimplantation genetic screening (PGS)’. Hum Reprod. 2005;20(1):35–48. doi:10.1093/humrep/deh579
4. Shaulov T, Sierra S, Sylvestre C. Recurrent implantation failure in IVF: a Canadian Fertility and Andrology Society Clinical Practice Guideline. Reprod Biomed Online. 2020;41(5):819–833. doi:10.1016/j.rbmo.2020.08.007
5. Cao H, You D, Yuan M, Xi M. Hysteroscopy after repeated implantation failure of assisted reproductive technology: a meta-analysis. J Obstet Gynaecol Res. 2018;44(3):365–373. doi:10.1111/jog.13571
6. Valdes CT, Schutt A, Simon C. Implantation failure of endometrial origin: it is not pathology, but our failure to synchronize the developing embryo with a receptive endometrium. Fertil Steril. 2017;108(1):15–18. doi:10.1016/j.fertnstert.2017.05.033
7. Kohn TP, Kohn JR, Darilek S, Ramasamy R, Lipshultz L. Genetic counseling for men with recurrent pregnancy loss or recurrent implantation failure due to abnormal sperm chromosomal aneuploidy. J Assist Reprod Genet. 2016;33(5):571–576. doi:10.1007/s10815-016-0702-8
8. Lee E, Illingworth P, Wilton L, Chambers GM. The clinical effectiveness of preimplantation genetic diagnosis for aneuploidy in all 24 chromosomes (PGD-A): systematic review. Hum Reprod. 2015;30(2):473–483. doi:10.1093/humrep/deu303
9. Cozzolino M, Diaz-Gimeno P, Pellicer A, Garrido N. Evaluation of the endometrial receptivity assay and the preimplantation genetic test for aneuploidy in overcoming recurrent implantation failure. J Assisted Reproduction Genetics. 2020;37(12):2989–2997. doi:10.1007/s10815-020-01948-7
10. Greco E, Bono S, Ruberti A, et al. Comparative genomic hybridization selection of blastocysts for repeated implantation failure treatment: a pilot study. Biomed Res Int. 2014;2014:457913. doi:10.1155/2014/457913
11. Pantou A, Mitrakos A, Kokkali G, et al. The impact of preimplantation genetic testing for aneuploidies (PGT-A) on clinical outcomes in high risk patients. J Assisted Reproduction Genetics. 2022;39(6):1341–1349. doi:10.1007/s10815-022-02461-9
12. Sato T, Sugiura-Ogasawara M, Ozawa F, et al. Preimplantation genetic testing for aneuploidy: a comparison of live birth rates in patients with recurrent pregnancy loss due to embryonic aneuploidy or recurrent implantation failure. Hum Reprod. 2019;34(12):2340–2348. doi:10.1093/humrep/dez229
13. Carvalho F, Coonen E, Goossens V, et al. ESHRE PGT Consortium good practice recommendations for the organisation of PGT. Hum Reprod Open. 2020;2020(3):hoaa021. doi:10.1093/hropen/hoaa021
14. Hefeng Huang JQ, Liu J, Chen Z-J, et al. Expert consensus on preimplantation genetic diagnosis/screening. Chine J Med Genetics. 2018;35(2):151–155.
15. Cimadomo D, de Los Santos MJ, Griesinger G, et al. ESHRE good practice recommendations on recurrent implantation failure. Hum Reprod Open. 2023;2023(3):hoad023. doi:10.1093/hropen/hoad023
16. Practice Committees of the American Society for Reproductive M, the Society for Assisted Reproductive Technology. Electronic address Aao, Practice Committees of the American Society for Reproductive M, the Society for Assisted Reproductive T. The use of preimplantation genetic testing for aneuploidy (PGT-A): a committee opinion. Fertil Steril. 2018;109(3):429–436. doi:10.1016/j.fertnstert.2018.01.002
17. Yan J, Qin Y, Zhao H, et al. Live Birth with or without Preimplantation Genetic Testing for Aneuploidy. N Engl J Med. 2021;385(22):2047–2058. doi:10.1056/NEJMoa2103613
18. Du Y, Guan Y, Li N, et al. Is it necessary for young patients with recurrent implantation failure to undergo preimplantation genetic testing for aneuploidy? Front Endocrinol. 2023;14:1020055. doi:10.3389/fendo.2023.1020055
19. Shi Y, Sun Y, Hao C, et al. Transfer of Fresh versus Frozen Embryos in Ovulatory Women. N Engl J Med. 2018;378(2):126–136. doi:10.1056/NEJMoa1705334
20. Gardner DC. In-vitro culture of human blastocysts. 1999.
21. Ghobara T, Gelbaya TA, Ayeleke RO. Cycle regimens for frozen-thawed embryo transfer. Cochrane Database Syst Rev. 2017;7(7):Cd003414. doi:10.1002/14651858.CD003414.pub3
22. Kissin DM, Kulkarni AD, Kushnir VA, Jamieson DJ. Number of embryos transferred after in vitro fertilization and good perinatal outcome. Obstet Gynecol. 2014;123(2 Pt 1):239–247. doi:10.1097/AOG.0000000000000106
23. Franasiak JM, Forman EJ, Hong KH, et al. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril. 2014;101(3):656–663.e1. doi:10.1016/j.fertnstert.2013.11.004
24. Demko ZP, Simon AL, McCoy RC, Petrov DA, Rabinowitz M. Effects of maternal age on euploidy rates in a large cohort of embryos analyzed with 24-chromosome single-nucleotide polymorphism-based preimplantation genetic screening. Fertil Steril. 2016;105(5):1307–1313. doi:10.1016/j.fertnstert.2016.01.025
25. Norton EC, Dowd BE, Maciejewski ML. Odds Ratios-Current Best Practice and Use. JAMA. 2018;320(1):84–85. doi:10.1001/jama.2018.6971
26. Bhatt SJ, Marchetto NM, Roy J, Morelli SS, McGovern PG. Pregnancy outcomes following in vitro fertilization frozen embryo transfer (IVF-FET) with or without preimplantation genetic testing for aneuploidy (PGT-A) in women with recurrent pregnancy loss (RPL): a SART-CORS study. Hum Reprod. 2021;36(8):2339–2344. doi:10.1093/humrep/deab117
27. Gleicher N, Barad DH, Patrizio P, Orvieto R. We have reached a dead end for preimplantation genetic testing for aneuploidy. Hum Reprod. 2022;37(12):2730–2734. doi:10.1093/humrep/deac052
28. Practice C. Genetic Counseling Professional Group of the American Society for Reproductive Medicine. Electronic address aao. Clinical management of mosaic results from preimplantation genetic testing for aneuploidy (PGT-A) of blastocysts: a committee opinion. Fertil Steril. 2020;114(2):246–254. doi:10.1016/j.fertnstert.2020.05.014
29. Greco E, Minasi MG, Fiorentino F. Healthy Babies after Intrauterine Transfer of Mosaic Aneuploid Blastocysts. N Engl J Med. 2015;373(21):2089–2090. doi:10.1056/NEJMc1500421
30. Victor AR, Tyndall JC, Brake AJ, et al. One hundred mosaic embryos transferred prospectively in a single clinic: exploring when and why they result in healthy pregnancies. Fertil Steril. 2019;111(2):280–293. doi:10.1016/j.fertnstert.2018.10.019
31. Zhang L, Wei D, Zhu Y, Gao Y, Yan J, Chen ZJ. Rates of live birth after mosaic embryo transfer compared with euploid embryo transfer. J Assist Reprod Genet. 2019;36(1):165–172. doi:10.1007/s10815-018-1322-2
32. Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med. 2007;357(1):9–17. doi:10.1056/NEJMoa067744
33. Rubio C, Bellver J, Rodrigo L, et al. In vitro fertilization with preimplantation genetic diagnosis for aneuploidies in advanced maternal age: a randomized, controlled study. Fertil Steril. 2017;107(5):1122–1129. doi:10.1016/j.fertnstert.2017.03.011
34. Verpoest W, Staessen C, Bossuyt PM, et al. Preimplantation genetic testing for aneuploidy by microarray analysis of polar bodies in advanced maternal age: a randomized clinical trial. Hum Reprod. 2018;33(9):1767–1776. doi:10.1093/humrep/dey262
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.