")
Back to Journals » Local and Regional Anesthesia » Volume 16
Postoperative Outcomes of Analgesic Management with Erector Spine Plane Block at T5 Level in Pediatric Patients Undergoing Cardiac Surgery with Sternotomy: A Cohort Study
Authors Cruz-Suárez GA , Rebellón Sánchez DE , Torres-Salazar D, Arango Sakamoto A , López-Erazo LJ, Quintero-Cifuentes IF, Vélez-Esquivia MA, Jaramillo-Valencia SA, Suguimoto-Erasso AJT
Received 20 October 2022
Accepted for publication 16 December 2022
Published 10 February 2023 Volume 2023:16 Pages 1—9
DOI https://doi.org/10.2147/LRA.S392307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stefan Wirz
Gustavo A Cruz-Suárez,1,2 David E Rebellón Sánchez,3,4 Daniela Torres-Salazar,2 Akemi Arango Sakamoto,4 Leidy Jhoanna López-Erazo,1,2 Iván F Quintero-Cifuentes,1,2 María A Vélez-Esquivia,2 Sergio A Jaramillo-Valencia,1 Antonio JT Suguimoto-Erasso1,2
1Fundación Valle del Lili, Anesthesiology Department, Cali, 760032, Colombia; 2Universidad Icesi, Facultad de Ciencias de la Salud, Departamento de Ciencias Clínicas, Cali, Colombia; 3Centro Internacional de Entrenamiento e Investigaciones Médicas (CIDEIM), Universidad Icesi, Cali, Colombia; 4Fundación Valle del Lili, Centro de Investigaciones Clínicas, Cali, 760032, Colombia
Correspondence: Gustavo A Cruz-Suárez, Fundación Valle del Lili, Anesthesiology Department, Cra. 98 # 18-49, Cali, 760032, Colombia, Tel +576023319090; Ext 4022, Email [email protected]
Introduction: There is limited evidence on the impact of erector spinae plane block (ESPB) as part of multimodal analgesia in pediatric population undergoing cardiac surgery.
Methods: A retrospective cohort study was conducted in patients under 18 years of age, who underwent cardiac surgery Risk Adjusted classification for Congenital Heart Surgery (RACHS-1) ≤ 3 by sternotomy. The study aims to evaluate the effect of ESPB as part of multimodal analgesia in pediatric patients undergoing cardiac surgery compared to conventional analgesia (CA) on relevant clinical outcomes: length of hospital stay, length of ICU stay, opioid consumption, time to extubation, mortality, and postoperative complications. The participants included were treated in a reference hospital in Colombia from July 2019 to June 2022.
Results: Eighty participants were included, 40 in the ESPB group and 40 in the CA group. There was a significant decrease (Log rank test p = 0.007) in days to length of hospital stay in ESPB group (median 6.5 days (IQR: 4– 11)) compared to the CA group (median 10.5 days (IQR: 6– 25)). Likewise, there was a higher probability of discharge from the ICU in the ESPB group (HR 1.71 (95% CI: 1.05– 2.79)). The ESPB group had lower opioid consumption (p < 0.05). There were no differences in time to extubation, mortality, and postoperative complications.
Conclusion: ESPB as part of multimodal analgesia in pediatric patients undergoing cardiac surgery is feasible and associated with shorter hospital length of stay, faster ICU discharge and lower opioid consumption.
Keywords: erector spinae plane block, cardiac surgery procedures, pediatric age group, anesthesia, perioperative, pediatric anesthesia
Introduction
The management of perioperative pain in patients with congenital heart disease undergoing surgery has evolved, leaning towards balanced anesthesia and regional techniques.1 Inadequate pain management in the perioperative period and cardiac surgery in pediatric patients may contribute to discomfort, prolonged intubation, recovery, and mobility delay.1–3 Pain control through multimodal analgesia is the mainstay of treatment; however, adverse events related to some of the drugs, such as opioids, could contribute to longer hospitalizations.1
Multiple strategies have been proposed to improve pain management, reduce undesired outcomes, and improve fast recovery.4–7 With the growing interest in the Enhanced Recovery After Surgery (ERAS) after cardiac surgery and the safety profile of local anesthetics, perioperative pain management focused on regional strategies has gained popularity as it may reduce opioid consumption.8,9 Regional ultrasound-guided analgesic modalities with a single anesthetic dose promise pain management during cardiac surgery without major complications.8,10–12 ESPB anesthetizes the dorsal and ventral branches of the spinal nerve roots, thus producing deep analgesia of the ipsilateral hemithorax.13
Although previous studies suggest that regional techniques during anesthesia in patients undergoing sternotomy effectively reduce operative and postoperative pain,14 there is limited evidence on the impact of those techniques, such as erector spinae plane block (ESPB), in pediatric population, and the evidence is currently limited to patients with septal and ventricular defects.1,2 In addition, pain management using ESPB in patients according to the RACHS-1 Classification Risk Score has not been reported and there is no information about the effectiveness of this technique in South America. This study aimed to compare postoperative outcomes in a cohort of Latin American pediatric patients undergoing low and moderate-risk cardiac surgery after multimodal analgesic management with ESPB compared to patients with conventional analgesia (CA) in terms of hospital and ICU length of stay, opioid consumption, time to extubation, mortality, and postoperative complications.
Materials and Methods
Study Design, Setting, and Participants
A retrospective cohort study was conducted at Fundación Valle del Lili, a tertiary hospital that serves as a reference center in pediatric cardiovascular surgery for southwestern Colombia. Patients under 18 years of age with cardiac pathology who underwent cardiovascular surgery with sternotomy as the only surgical approach or with a combined approach between July 2019 and June 2022 were pre-selected. Inclusion and classification criteria in the ESPB group were all pediatric patients with RACHS-1 risk classification less than or equal to three, who received ESPB at the end of surgery as part of multimodal analgesia management, at the discretion of the anesthesiologist in charge of the patient. The conventional analgesia (CA) group included all patients undergoing the same surgical procedures, with RACHS-1 risk classification less than or equal to three, treated without the ESPB. All patients were operated by two pediatric cardiovascular surgeons.
Outcomes and Exposure Measures
The primary outcome variable was time in days of hospital stay and ICU stay. Secondary outcomes were opioid consumption, extubation time, complications, and in-hospital mortality.
The exposure variable at the end of surgery was the type of analgesic intervention (ESPB group vs CA group). All patients classified in the ESPB group underwent a 0.7 mL/kg of 0.125% of bupivacaine bilateral single-shot in the intersection between each of the erector spine plane muscles and the transverse process of the fourth and fifth thoracic vertebrae. This was performed under ultrasound guidance and after performing an aseptic technique. The mentioned process was followed by opioid intravenous injections for both groups (morphine range between 50 and 200 µg/kg), alpha-2 agonists (dexmedetomidine 0.5 µg/kg/h), and paracetamol (10 mg/kg). For the CA group, opioid (morphine dose 0.1 mg/kg), paracetamol (10 mg/kg), and alpha-2 agonists (0.5 µg/kg/h) were administered at the same pre-established doses according to institutional protocol for perioperative pain management.
Covariates included demographics (age, gender, weight and height, body surface, comorbidities) and clinical (RACHS-1, type of surgery, cardiopulmonary bypass time, aortic cross-clamp, intraoperative opioid consumption). Post anesthesia information (time to extubation in hours and days, time to first rescue analgesia, postoperative vital signs: systolic, diastolic, and mean blood pressure, heart rate, oxygen saturation at 1, 3, 6, 12, 24, 48 hours, days of ICU stay, overall in hospital stay in days, complications, adverse events and postoperative pain evaluation according to the FLACC (Face, Legs, Activity, Cry, Consolability) scale at 1, 3, 6, 12, 24, 48 hours were also included. All data were obtained from the clinical history, and anesthetic variables were obtained from the anesthesia record. Two investigators extracted patient information in a protected electronic data collection form independently. When the information was completely collected, we randomly analyzed 10% of the database. If discordant data were found, errors were immediately corrected.
Sample Size
We calculated the sample size necessary to find a mean difference in the number of days of hospital stay of one or more days, aiming for a statistical power of 80%, with a confidence interval of 95% and an alpha of 0.05%. We calculated a minimum of 32 patients to achieve this objective for each group. A convenience sampling was conducted and all participants who met the inclusion criteria for the ESPB group were included. Afterwards, subjects with CA were completed to meet the ESPB group sample size according to the database provided by the institutional statistics department.
Statistical Methods
We used conventional descriptive statistical methods. For continuous data, normality was evaluated using q-q plot and Shapiro Wilk test. Continuous data with normal distribution is presented as mean and standard deviation, while those with no normal distribution are presented as median and interquartile range (IQR). Categorical variables are reported as absolute frequencies and percentages.
A bivariate analysis was performed between patients undergoing ESPB and those treated with CA to evaluate differences in baseline characteristics of both groups. To compare quantitative variables, Student’s t-test or Mann Whitney U-test were used according to the distribution of the variables. Categorical variables were analyzed using the Chi test or Fisher’s exact test according to compliance of statistical assumptions. After comparing the baseline characteristics of both clinical groups, comparisons were made for extubation time (days), opioid consumption (morphine or equivalents during hospital stay), postoperative complications (cardiovascular, pulmonary, fever, nausea and emesis, pruritus, rash), and mortality.
For the main outcomes, evaluation (hospital length of stay and ICU length of stay), Kaplan–Meier survival analyses were performed. Subsequently, the statistical significance between the differences in the survival curves was evaluated using the Log rank test and the Wilcoxon test (Breslow) according to the fulfillment of statistical assumptions. Univariate and multivariate Cox regression models were constructed to establish the strength of association between the intervention and the outcome variable. Those tests with a p-value <0.05 were considered statistically significant for all analyses. All analyses were performed in STATA version 16® (StataCorp, College Station, TX, USA).
Ethics Statement
This research is considered as research “without risk” in accordance with resolution 8430 of the Colombian Ministry of Health and “minimal risk” research according to the Federal Policy for the Protection of Human Subjects in Research of the United States. This study was approved and monitored by the Institutional Review Board of Fundación Valle de Lili (approval number: 083–2021, Act No. 06 of 2021). The guidelines and recommendations of the Council for International Organizations of Medical Sciences (CIOMS) were considered for all study procedures. Waiver of informed consent for the use of data was requested and accepted.
Results
Eighty participants were included; 40 (50%) corresponded to the CA group and 40 (50%) to the ESPB group. The median age in the study population was 9.5 months (IQR: 4–54), with no statistically significant differences between exposure groups (p=0.17).
The median weight for all patients was 7.5 kg (IQR: 4.8–17), and there were marginally significant differences in body surface area between treatment groups (p=0.08). In total, 50 (62.5%) participants had some comorbidity in addition to their cardiovascular pathology, with no significant differences between the ESPB group and the CA group (p=0.92). Likewise, no significant differences were found between the RACHS-1 classification in the treatment groups (p=0.6). And 16.25% of the participants were classified as risk 1 according to the RACHS-1 classification, 50% as risk 2, and 33.75% as risk 3. The median aortic cross-clamp and cardiopulmonary bypass time were 34 minutes and 52 minutes, respectively, with no significant differences between treatment groups (p>0.05). Table 1 summarizes the sociodemographic, clinical, and intraoperative characteristics of the study population.
 |
Table 1 Demographic, Clinical and Intraoperative Characteristics of the Study Population |
Additionally, no differences in postoperative vital signs hours were found (see Table S1). Overall, the median time to extubation in the CA group was 21 hours (IQR: 6–140) versus 6.5 hours (IQR: 3−72) in the ESPB group; however, these differences were not statistically significant (p=0.12). The ESPB group had lower opioid consumption than CA group ((Me 1242 µg/kg/48h vs Me 4854 µg/kg/48h (p=0.0014)). After classifying patients according to weight, it was found that patients with 6.3 kg or less required higher doses of opioids compared to those with more than 6.3 kg (1388 µg/kg/48h versus 350 µg/kg/48h, respectively (p<0.001). There were no complications associated with the ESPB technique, and the rate of adverse events between the ESPB and CA groups was not statistically different (p=0.5). Further details are presented in Tables 2 and 3.
 |
Table 2 Comparison of Postoperative Clinical Outcomes Between Therapeutic Groups |
 |
Table 3 Comparison of Postoperative Adverse Events Between Therapeutic Groups |
The Kaplan–Meier analysis showed that patients undergoing ESPB (Wilcoxon Breslow test p= 0.007 were more likely discharged sooner from the hospital (median of 6.5 days (IQR: 4–11)) compared to the CA group (median of 10.5 days (IQR: 6–25 days)) (see Figure 1). Bivariate analysis showed that patients in the ESPB group were significantly more likely to be discharged from the hospital during the entire study period than patients in the CA group (HR 1.73, 95% CI: 1.10–2.72). Likewise, when constructing a multivariate model that included type of treatment, RACHS-1 classification risk score, adverse events and the presence of comorbidities, a statistically significant difference was still found (HR 1.79, 95% CI: 1.11–2.87).
 |
Figure 1 Kaplan–Meier analysis of time to hospital discharge according to the type of analgesic intervention. |
Finally, we performed a second Kaplan–Meier analysis to evaluate the impact of ESPB on ICU length of stay, with significant differences in favor of the use of ESPB to reduce ICU length of stay (Wilcoxon Breslow p=0.02). When constructing the bivariate model, an HR of 1.75 (95% CI: 1.09–2.80) was found, which remained significant in the multivariate analysis (HR of 1.71 (95% CI: 1.05–2.79)) (see Figure 2 and Table 4).
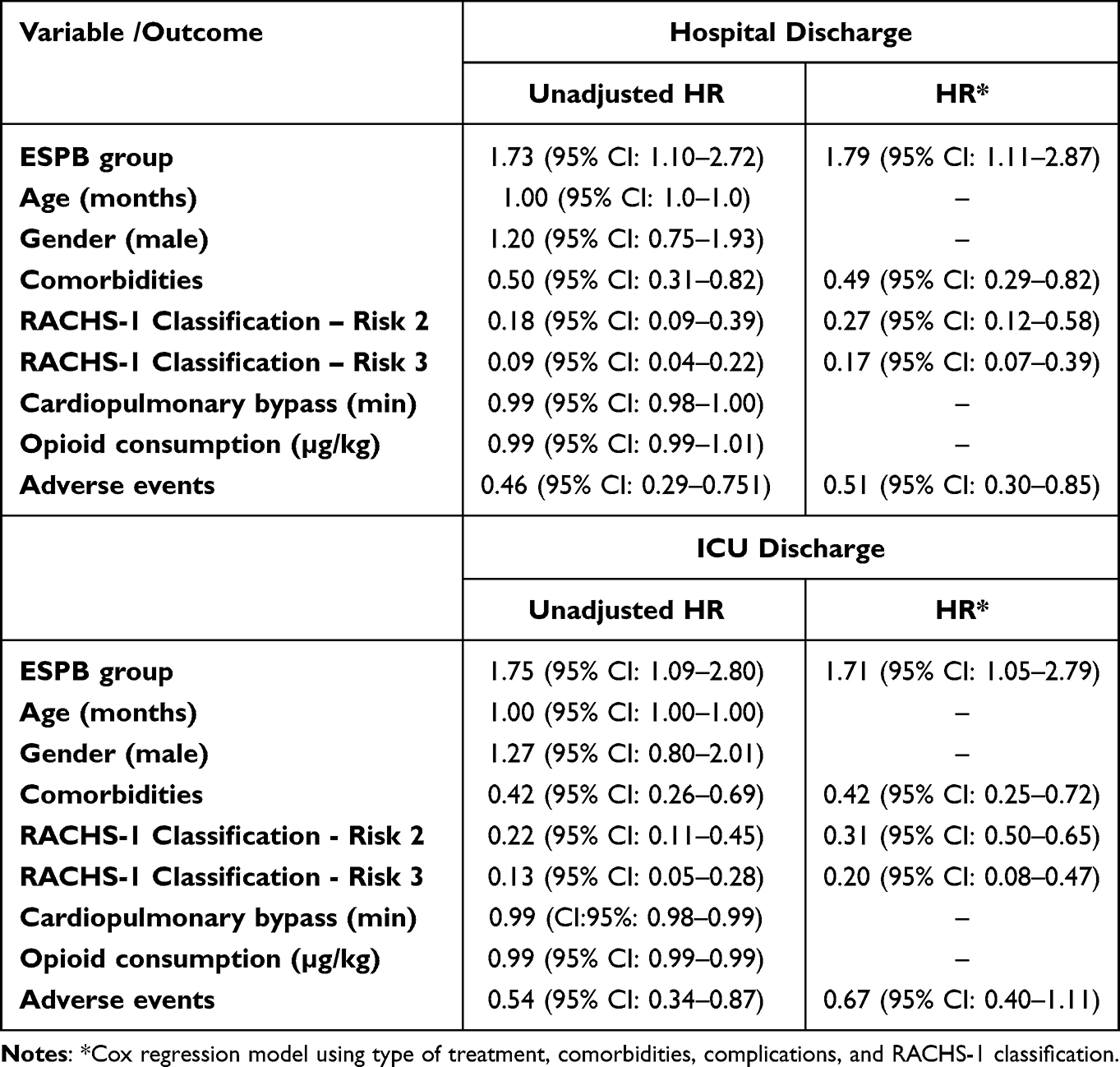 |
Table 4 Comparison of Unadjusted and Adjusted Hazard Ratios in Multivariate Cox Regression Models |
 |
Figure 2 Kaplan–Meier analysis of time to ICU discharge according to the type of analgesic intervention. |
We verified compliance with statistical assumptions for the construction of the models, the estimates were not affected by extreme values, and the independence test was verified (see Figures S1–S4).
Discussion
This study was performed to evaluate the effectiveness of bilateral ESPB in postoperative outcomes after pediatric cardiac surgery through sternotomy in a Latin American cohort. Our hypothesis was based on better pain control, decreased mechanical ventilation time, early feeding, reduction in the effect of pain over respiratory dynamics, prompt ICU discharge, and in-hospital length of stay. The ESPB was associated with reduced hospitalization and ICU length of stay compared with CA. This association, added to the absence of block-related complications, as well as the no difference in the proportion of adverse events compared to the CA group, support the applicability of ESPB in our setting as part of the perioperative management of pediatric patients to facilitate early recovery in cardiovascular surgery.8
Currently, ESPB is being used rarely among surgeries in the pediatric population. Hernández et al15 performed a single local anesthetic injection in the ESPB at the level of the transverse process of T1 in a 3-year-old boy who underwent resection of a giant parasternal lipoma. This block showed excellent pain control from T2 to T8 dermatomes without compromising hemodynamic stability. Another case report reports the successful use of an ESPB with continuous infusion in a 3-year-old boy with a history of hypoplastic heart syndrome who underwent thoracoscopic diaphragmatic aplication, obtaining analgesic coverage and excellent postoperative recovery.16 Kaushal et al12 and Karacear observed a significantly lower requirement for postoperative opioid doses in pediatric patients undergoing cardiac surgery. Our study did also find a difference in opioid consumption between the study groups, and ESPB group patients had lower consumption of opioids. In Tirotta’s study, patients over 6.3 kg were suggested to have bigger opioid consumption.5 However, in our study, patients weighing >6.3 kg were found to have lower opioid consumption per kilogram than patients below this point.
Adequate management of perioperative pain decreases the sympathetic response to stimulus.4 It is suggested that arterial hypotension in patients undergoing ESPB is due to a sympathetic block by diffusion of the local anesthetic towards the anterior region through the costotransverse foramen, penetrating the thoracic paravertebral space generating blockage of the spinal branches and sympathetic fibers.17 However, studies such as Kaushal et al12 and our study did not report hemodynamic changes in patients with ESPB during the first 24 hours (Table S1).
No complications were associated with ESPB in our registry. Anecdotal cases of complications such as pneumothorax, motor block, and local anesthetic intoxication (LAST), apparently due to rapid absorption18 associated with this procedure, have been described. In a prospective cohort study of bilateral ESPB with catheters, Roy et al reported mild complications associated with catheter insertion, such as mild leakage of the solution and a catheter kinked that did not compromise the administration of the drugs; nevertheless, no other complications were observed.12 Also, Cassai et al19 conducted a systematic review of studies, including ESPB in which no complications were reported. However, although the report of zero complications is encouraging, we cannot infer zero risks based on this evidence. Pneumothorax, involuntary motor block, local anesthetic systemic toxicity, hematomas, punction of organs, injection in the epidural or paravertebral space, and failure of the technique may occur.
Evidence on the use of EPSB in pediatric patients undergoing cardiovascular surgery by sternotomy is limited. In the clinical trial published by Kaushal et al,12 it was reported that patients undergoing ESPB had shorter ICU length of stay, which is consistent with our results. One of the strengths of our study is that we included length of hospital stay as another outcome of interest, which was not analyzed until Karacaer in a prospective, blinded, randomized controlled study. We found that the length of hospital stay was shorter in patients who underwent ESPB. Despite no differences in ICU and global hospital stay were found by Karacaer et al,20 greater sample size of randomized controlled studies is needed to clarify our results. In addition, the fact that we used Kaplan–Meier analysis and Cox regression models allow us to perform a better adjustment of factors associated with ICU length of stay and hospitalization, considering temporality and event occurrence rate between the ESPB and CA groups.
We found that the ESPB group was almost twice older as the CA group. A study by Agarwal et al in 2014 found that younger patients significantly required prolonged mechanical ventilation. Regardless of these reported results, since we found an apparent difference between the age of the participants included in both groups (ESPB and CA) and considering that age-related physiological changes could play a role in the inflammatory response and recovery processes after surgery, we decided to include age in the multivariate analysis model. However, when adjusting for these variables and other possible confounders, we found no association of age with clinical outcomes, and performing ESPB remained significantly associated with reduced ICU stay and hospital stay.21 In addition, in the Roy et al’s study, it was reported that patients with bilateral ESPB and continuous infusion of analgesia had adequate pain control, reduced the requirement for opioids at 48 hours and concluded that ESPB is a feasible alternative in patients over 5 years of age.12 Our study provides similar evidence and information about the safety of ESPB use in younger patients.
Some disadvantages of the study: first, the sample size was relatively small, although no published registry collects this number of cases among this population. Second, as a retrospective design, it may have been a potential for bias in care; for this reason, prospective trials are needed. Third, the pain evaluation during the perioperative period in the pediatric population is still challenging, for this reason, opioid consumption may be considered as an indirect pain evaluation.
Conclusions
In our study, ESPB used in Latin American pediatric patients undergoing moderate- and low-risk cardiovascular surgery according to the RACHS-1 risk category proved to be a feasible alternative for pain management with a reduction in hospital length of stay, ICU length of stay and lower opioid consumption. No differences were found in mortality or in the proportion of postoperative complications or adverse events. Randomized clinical trials including Latin American populations are required to verify the findings of our study before giving a strong recommendation in favor of the performance of ESPB in pediatric cardiovascular surgery.
Abbreviations
ESPB, erector spine plane block; CA, conventional analgesia; EC, extracorporeal circulation; HR, hazard ratio; ERAS, Enhanced Recovery After Strategy; ICU, intensive care unit; LAST, Local anesthetic intoxication; VAS, visual analog scale; NRS, numerical rating scale.
Acknowledgments
We would like to thank Fundación Valle del Lili and the group of anesthesiologists of the same institution.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tirotta CF, Munro HM, Salvaggio J, et al. Continuous incisional infusion of local anesthetic in pediatric patients following open heart surgery. Paediatr Anaesth. 2009;19(6):571–576. doi:10.1111/j.1460-9592.2009.03009.x
2. Ovroutski S, Kramer P, Nordmeyer S, et al. Early extubation is associated with improved early outcome after extracardiac total cavopulmonary connection independently of duration of cardiopulmonary bypass. Eur J Cardiothorac Surg. 2018;54(5):953–958. doi:10.1093/ejcts/ezy179
3. Bignami E, Castella A, Allegri M. Postoperative pain after cardiac surgery: an open issue. J Cardiothorac Vasc Anesth. 2018;32(1):e24–e25. doi:10.1053/j.jvca.2017.09.022
4. Andrew RW. Effects of regional analgesia on stress responses to pediatric surgery. Paediatr Anaesth. 2012;22(1):19–24. doi:10.1111/j.1460-9592.2011.03714.x
5. Vricella LA, Dearani JA, Gundry SR, Razzouk AJ, Brauer SD, Bailey LL. Ultra fast track in elective congenital cardiac surgery. Ann Thorac Surg. 2000;69(3):865–871. doi:10.1016/S0003-4975(99)01306-5
6. Liu SS, Block BM, Wu CL. Effects of perioperative central neuraxial analgesia on outcome after coronary artery bypass surgery: a meta-analysis. Anesthesiology. 2004;101(1):153–161. doi:10.1097/00000542-200407000-00024
7. Rigg JRA, Jamrozik K, Myles PS, et al. Epidural anaesthesia and analgesia and outcome of major surgery: a randomised trial. Lancet. 2002;359(9314):1276–1282. doi:10.1016/S0140-6736(02)08266-1
8. Townsley MM. Regional anesthesia in pediatric cardiac surgery: a road to enhanced recovery. J Cardiothorac Vasc Anesth. 2020;34(12):3373–3375. doi:10.1053/j.jvca.2020.08.047
9. Nasr VG, Gottlieb EA, Adler AC, et al. Selected 2018 highlights in congenital cardiac anesthesia. J Cardiothorac Vasc Anesth. 2019;33(10):2833–2842. doi:10.1053/j.jvca.2019.03.013
10. Krishna SN, Chauhan S, Bhoi D, et al. TEMPORARY REMOVAL: bilateral erector spinae plane block for acute post-surgical pain in adult cardiac surgical patients: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2019;33(2):368–375. doi:10.1053/j.jvca.2018.05.050
11. Roy N, Brown ML, Parra MF, et al. Bilateral erector spinae blocks decrease perioperative opioid use after pediatric cardiac surgery. J Cardiothorac Vasc Anesth. 2021;35(7):2082–2087. doi:10.1053/j.jvca.2020.10.009
12. Kaushal B, Chauhan S, Magoon R, et al. Efficacy of bilateral erector spinae plane block in management of acute postoperative surgical pain after pediatric cardiac surgeries through a midline sternotomy. J Cardiothorac Vasc Anesth. 2020;34(4):981–986. doi:10.1053/j.jvca.2019.08.009
13. Schwartzmann A, Peng P, Maciel MA, Forero M. Mechanism of the erector spinae plane block: insights from a magnetic resonance imaging study. Can J Anaesth. 2018;65(10):1165–1166. doi:10.1007/s12630-018-1187-y
14. Mittnacht AJC, Shariat A, Weiner MM, et al. Regional techniques for cardiac and cardiac-related procedures. J Cardiothorac Vasc Anesth. 2019;33(2):532–546. doi:10.1053/j.jvca.2018.09.017
15. Hernandez MA, Palazzi L, Lapalma J, Forero M, Chin KJ. Erector spinae plane block for surgery of the posterior thoracic wall in a pediatric patient. Reg Anesth Pain Med. 2018;43(2):217–219. doi:10.1097/AAP.0000000000000716
16. Cuadra-Fontaine JCD, Concha M, Vuletin F, Arancibia H. Continuous erector spinae plane block for thoracic surgery in a pediatric patient. Paediatr Anaesth. 2018;28(1):74–75. doi:10.1111/pan.13277
17. Pollak U, Bronicki RA, Achuff B-J, Checchia PA. Postoperative pain management in pediatric patients undergoing cardiac surgery: where are we heading? J Intensive Care Med. 2019. doi:10.1177/0885066619871432
18. De Cassai A, Bonanno C, Padrini R, et al. Pharmacokinetics of lidocaine after bilateral ESP block. Reg Anesth Pain Med. 2021;46(1):86–89. doi:10.1136/rapm-2020-101718
19. De Cassai A, Geraldini F, Carere A, Sergi M, Munari M. Complications rate estimation after thoracic erector spinae plane block. J Cardiothorac Vasc Anesth. 2021;35(10):3142–3143. doi:10.1053/j.jvca.2021.02.043
20. Karacaer F, Biricik E, Ilgınel M, Tunay D, Topçuoğlu Ş, Ünlügenç H. Bilateral erector spinae plane blocks in children undergoing cardiac surgery: A randomized, controlled study. J Clin Anesth. 2022 Sep;80:110797. doi: 10.1016/j.jclinane.2022.110797. Epub 2022 Apr 28. PMID: 35489304.
21. Agarwal HS, Wolfram KB, Saville BR, Donahue BS, Bichell DP. Postoperative complications and association with outcomes in pediatric cardiac surgery. J Thorac Cardiovasc Surg. 2014;148(2):609–616.e1. doi:10.1016/j.jtcvs.2013.10.031
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.