")
Back to Journals » Patient Preference and Adherence » Volume 18
Perceived Determinants of Health-Related Behaviors Among Patients with Coronary Heart Disease After Percutaneous Coronary Intervention: A Longitudinal Qualitative Study
Authors Su X, Zhang Y , Zhou H, Ma F , Jin X, Bai Y , Wei W , Zhang X, Zhou M
Received 3 December 2023
Accepted for publication 24 February 2024
Published 6 March 2024 Volume 2024:18 Pages 591—606
DOI https://doi.org/10.2147/PPA.S452943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xu Su,1,* Yimei Zhang,1,* Huilin Zhou,1 Fang Ma,1 Xiaorong Jin,1 Yangjuan Bai,2 Wei Wei,3 Xiong Zhang,1 Min Zhou1
1Department of Nursing, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China; 2Cardiology Department, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China; 3Digestive Surgery Department, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Ma, Department of Nursing, The First Affiliated Hospital of Kunming Medical University, No. 295, Xichang Road, Kunming, 650032, People’s Republic of China, Email [email protected]
Purpose: Studies had reported some influencing factors of health behavior among patients with coronary heart disease(CHD) after percutaneous coronary intervention(PCI). However, considering that human perceptions are complex, unrestricted and dynamically changing. A longitudinal qualitative study was conducted to explore the determinants of health-related behaviors of patients after PCI and dynamic changes of these determinants at the 1st, 3rd, and 6th months.
Patients and Methods: Using purposive sampling, 18 patients undergoing PCI were interviewed. The conventional content analysis method was used to identify categories and subcategories. Semi-structured, face-to-face or telephone in-depth interviews were conducted at the cardiology unit of a tertiary referral hospital in Yunnan Province, China from March 2022 to January 2023.
Results: Seven categories with some subcategories were constructed from the data, categorized into three domains. Firstly, individual factors include (i) Personal coping with healthy lifestyle requirements (tried but failed; I can do it), (ii) individual perception and feeling toward disease (knowing about the disease; belief of cure; fears of relapse), and (iii) personal benefits (improved health; meaning of life). Secondly, social factors include (i) social facilitators (family resources; healthcare support), (ii) social barriers (inconvenient medical care service; conflicting information). Finally, cultural factors include (i) way of living (dietary habits; key roles of yan (cigarette) and jiu (alcohol) in Chinese society), (ii) way of thinking (fatalism and Confucian familism).
Conclusion: The determinants of health-related behaviors of patients after PCI are multifaceted and dynamic. Different interventions should be formulated to promote patients’ adherence to health behaviors. Moreover, priority should be given to the impact of traditional Chinese philosophy on the health behaviors of patients after PCI, and the health promotion program for these patients should be culturally sensitive. In addition, future research should further explore the determinants of health behaviors among diverse ethnic minorities after PCI, which has not been fully inquired in this study.
Keywords: coronary heart disease, percutaneous coronary intervention, health behavior adherence, qualitative research, Chinese traditional culture
Introduction
Coronary heart disease (CHD) is a main ischemic heart disease caused by coronary atherosclerosis, which is a main cause of global morbidity and mortality.1,2 As the most common revascularization modality for the treatment of CHD, percutaneous coronary intervention (PCI) provides rapid and effective treatment, which has the advantages of minimally invasive harm, shorter hospitalization time, clear cost-effectiveness and less pain.3,4 In recent decades, PCI has been widely used globally and it has been reported that the average number of patients undergoing PCI per year reached 800,000 in Europe and 1 million in the USA.5
Although PCI can relieve obstruction in a stenotic coronary artery and achieve better outcomes through improved stent technology, CHD cannot be cured by PCI and restenosis still exists after PCI,6 which pose a huge burden on the patients and healthcare system as well. As a chronic illness, CHD can only be managed and secondary prevention programs are especially important for patients with CHD after PCI, such as a healthy lifestyle and regular medication-taking.7,8 However, these health behaviors in people after PCI are unsatisfactory. It is reported that although adherence to secondary prevention 3 months after discharge was relatively good in patients after PCI, only 15% to 50% of patients with CHD continue to exercise 3 to 6 months after cardiac rehabilitation program graduation and the number is decreasing with time going on.9,10
Research into the determinants of health-related behaviors among patients with CHD after PCI is essential for the development of effective interventions to improve their health behaviors. Some researchers have identified that quick relief of symptoms, shorter hospital stay and patients’ misconceptions of being cured by PCI might hinder patients’ willingness to change unhealthy lifestyles.11,12 Other studies reported that inadequate information from physicians and nurses, concerns about drug side effects, the severity of the disease, and economic situation affect patients’ adherence with treatment.13–16 Cultural context provides a clearer lens through which researchers might view and understand health behavior, which is essential for targeting health behavior change.17,18 However, cultural context is seldom addressed in the researches about the determinants of health-related behavior among patients after PCI. In addition, the influencing factors of patients’ health-related behaviors will not be static and are changing over time. To our knowledge, current studies have focused on specific timepoints, and researches considering the dynamic of these determinants over time are limited. Therefore, cultural setting and time lapse should be included in the exploration of influencing factors of health-related behaviors among patients after PCI.
In China, there are currently over 11.39 million patients with CHD, and the total number of registered cases of PCI is 1,164,117 in 2021 in Chinese Mainland, excluding military hospital cases, an increase of 20.18% compared to 2020.19 However, studies showed that 60.8% of patients did not meet the recommended physical activity standards in the guidelines,20 and about one-third of patients did not comply with smoking cessation and medication after PCI in China.21,22 China is a unified multi-ethnic nation composed of the Han ethnic group and 55 other ethnic minorities, with a long history and rich culture. Diverse geographical environments and cultural habits among ethnic groups might result in special characteristics in their diet and lifestyle. Therefore, it is necessary to explore the health-related determinants of patients post PCI in this setting.
Most previous studies are quantitative or cross-sectional qualitative research that can only provide valuable “snapshots”, whereas human perceptions are complex, unrestricted, evolving and changing over time.23,24 The use of longitudinal qualitative research provides an appropriate way to reach this aim. It spans two methodologies, longitudinal and qualitative that can capture the dynamic and unique nature of the lived experiences of patients over time.25 3 months after PCI is considered as relatively good concerning patient’ adherence to secondary prevention, and pre and after this timepoint might be appropriate for patients to reflect multiple points of view. Therefore, this study aims to explore the influencing factors of health-related behaviors among patients with CHD at the 1st, 3rd, and 6th months after PCI in a Chinese cultural background.
Methods
Study Design
A longitudinal, qualitative descriptive study was conducted in this study, which not only comprehensively describes the dynamic health phenomena of patients through repeated interviews or observations, but also reflects the continuous and immediate situation of people’s health experiences, personal development, or changes in healthcare systems, trajectories, and changes.26 This is in line with the theme of this study, which explores the perceived determinants of health-related behaviors in patients with CHD after PCI. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist informed the development, analysis and reporting of this study (see Supplementary Material File 1).27
Setting and Participants
This study was conducted at a comprehensive tertiary hospital located in the capital city of Yunnan Province, China. It provides services to a wide geographical area of the province and some patients from neighboring provinces. Yunnan Province is located in southwestern China, serving as the gateway to the Southwest Silk Road, which is an important international trade route between China and the Mediterranean in history.28 Moreover, there are 25 ethnic minorities living in the province, of which 15 only live in Yunnan.29 These ethnic groups have different traditions, geography, and lifestyles, and their unique cultural backgrounds may have varying degrees of impact on the health behaviors adopted by patients after PCI.
The purposive sampling method was used to recruit participants with different ages, genders, occupations and ethnic groups. Patients who met the following criteria were included: (a) patients diagnosed with CHD and had undergone PCI, (b) patients aged 18 years or older without psychiatric disorders or cognitive impairment, and (c) patients who voluntarily participated in this study and signed informed consent forms. The following patients were excluded: (a) patients with severe comorbidities, such as heart failure and severe pulmonary disease. (b) participants who did not completely participate in three interviews.
Data Collection
Data were collected from March 2022 to January 2023 by the same interviewer (XS, a female graduate nursing student), who had completed a graduate-level qualitative research course and had experience conducting qualitative interviews. The interviewer released recruitment information to all patients who had received PCI in the ward and explained the purpose and process of this study to them. After the patient expressed interest in participating in this study, an informed consent form was provided and signed. Their demographic data such as gender, age, occupation, and ethic group, were recorded simultaneously, as well as contact information needed for subsequent interviews.
Semi-structured audio-recorded interviews were conducted by phone or face-to-face interviews. The interviewer will record the first interview date of each participant and contact them for the interview at the 3rd and 6th months after the surgery. If patients were hospitalized or undergoing follow-up examinations at the interview timepoints, patients were invited to participate in face-to-face interviews in the meeting room of the ward or a silent place in the garden of the hospital. If patients were not in the hospital at the interview timepoints, telephone interviews were performed when patients were at home and in their leisure time. The interviewer asked questions in clear and concise language, and no one else was present during the interview to ensure a relaxed and quiet environment. She tried to hide and separate her viewpoints from the participants’ positions to avoid bias in interviews. Participants’ nonverbal behaviors such as expressions and body languages, and field notes were recorded during face-to-face interviews. The interviewer established a trust relationship with participants by patiently answering their questions and providing them with the necessary health knowledge through several interviews. The interview records were transcribed verbatim within 24 hours by XS. A total of 59 interviews were conducted, followed by 41 reinterviews after the initial one, and each interview lasted between 25 and 60 minutes. After transcription was completed, the interviewer returned the manuscript to the participants and verified the interview content with them to confirm the accuracy of the obtained materials.
The interview guide (Table 1) was developed based on the Health Belief Model and relevant literature related to CHD patients after PCI.30,31 Some questions are as follows: “How do you view the recurrence of heart problems?” “How is your postoperative health status? How is the disease affecting you now?” The guide was continuously adjusted according to participants’ accounts and the process of concurrent analysis. Before the formal interview, 2–3 patients were invited to perform a mock interview to verify the questions to be used during the semi-structured, in-depth interviews, and these samples were not included in the final study. Data collection stopped after the 18th participant because the saturation point was reached and no new viewpoints were found in subsequent interviews.
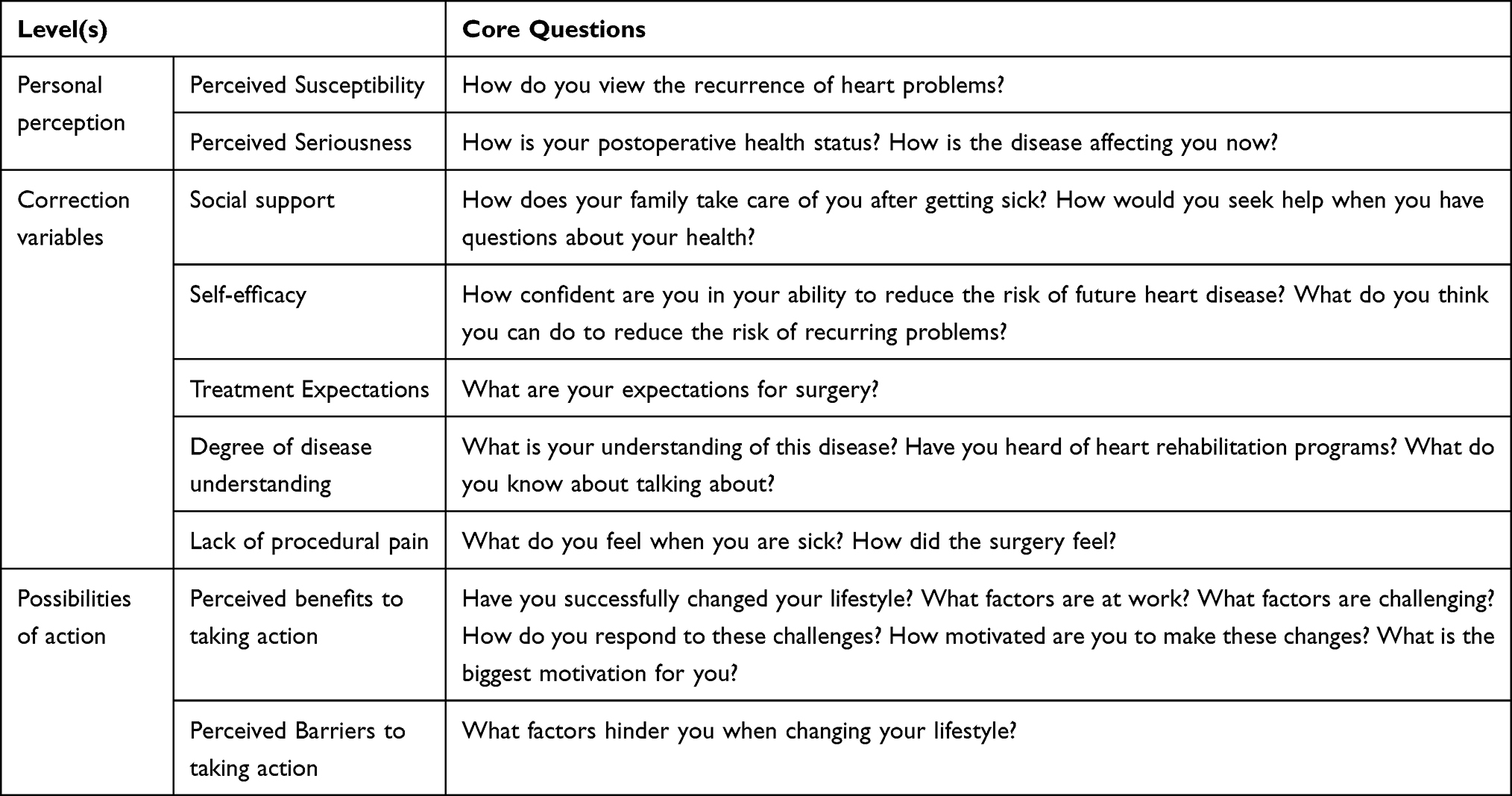 |
Table 1 Semi-Structured Interview Guide Proposed Based on Health Behavior Model |
Data Analysis
The interview data were analyzed using the conventional content analysis method.32 Initially, the interviewer repeatedly listened to the audiotaped interviews before transcribing them into texts to familiarize them with the participants’ viewpoints. Secondly, interview transcripts were reviewed and interpreted by two authors (XS, and YM, Z.) and imported into the NVivo 12 software. Thirdly, texts related to determinants of health-related behaviors were divided into meaning units, which were condensed to smaller units and then abstracted and coded. Additionally, based on the differences and similarities of codes, eleven categories and some subcategories were abstracted. Finally, three domains were formed according to the interrelationships between categories. Two authors independently coded and then discussed early coding decisions with the corresponding author to reach consensus.
Ethical Considerations
The study followed the Helsinki Declaration, and has been approved by the Ethics Committee of the First Affiliated Hospital of Kunming Medical University (Ref:2022-L-66). Participants were informed to understand the purpose, process, and anonymized publication of this study, and ongoing consent was checked before starting to subsequent interviews. All participants were identified by serial numbers (e.g. P1, P2. “P” means “Participant”, T1, T2 … “T” means “Time”). Interview records were stored in a password secured computer file and only the identified researcher could access these records.
Rigor
The rigor of this study is evaluated based on its credibility, confirmability, dependability, and transferability. Peer-debriefing was performed to ensure credibility. Confirmability was established by providing adequate information about the research. Dependability was ensured by accurately recording research details and discussing with other peer researchers. Transferability was achieved by providing in-depth and rich descriptions of findings. In addition, the interviewer had not served any patients before, so she did not establish any relationship with the participants before the first interview. Assumptions and biases related to the research questions were discussed by the researchers throughout data collection and analysis. Moreover, the disagreements in the research were discussed and resolved through meeting frequently.
Results
Twenty-five patients who had undergone PCI were selected to participate in interviews. After the first interview, seven patients lost contact during the follow-up period (two for the second time, and five for the third time). Eighteen patients aged 41 to 72 participated in all three interviews, including 15 males and three females. Consequently, the sample does not represent both genders equally. However, a previous study reported that the prevalence of CHD in males is higher than that in females, so fewer female patients receive PCI.33 This may explain why the proportion of males in this study was much higher than that of females. For nationality, 13 were Han, three were Hui, one was Tibetan and one was Bai. Participant demographics are summarized in Table 2.
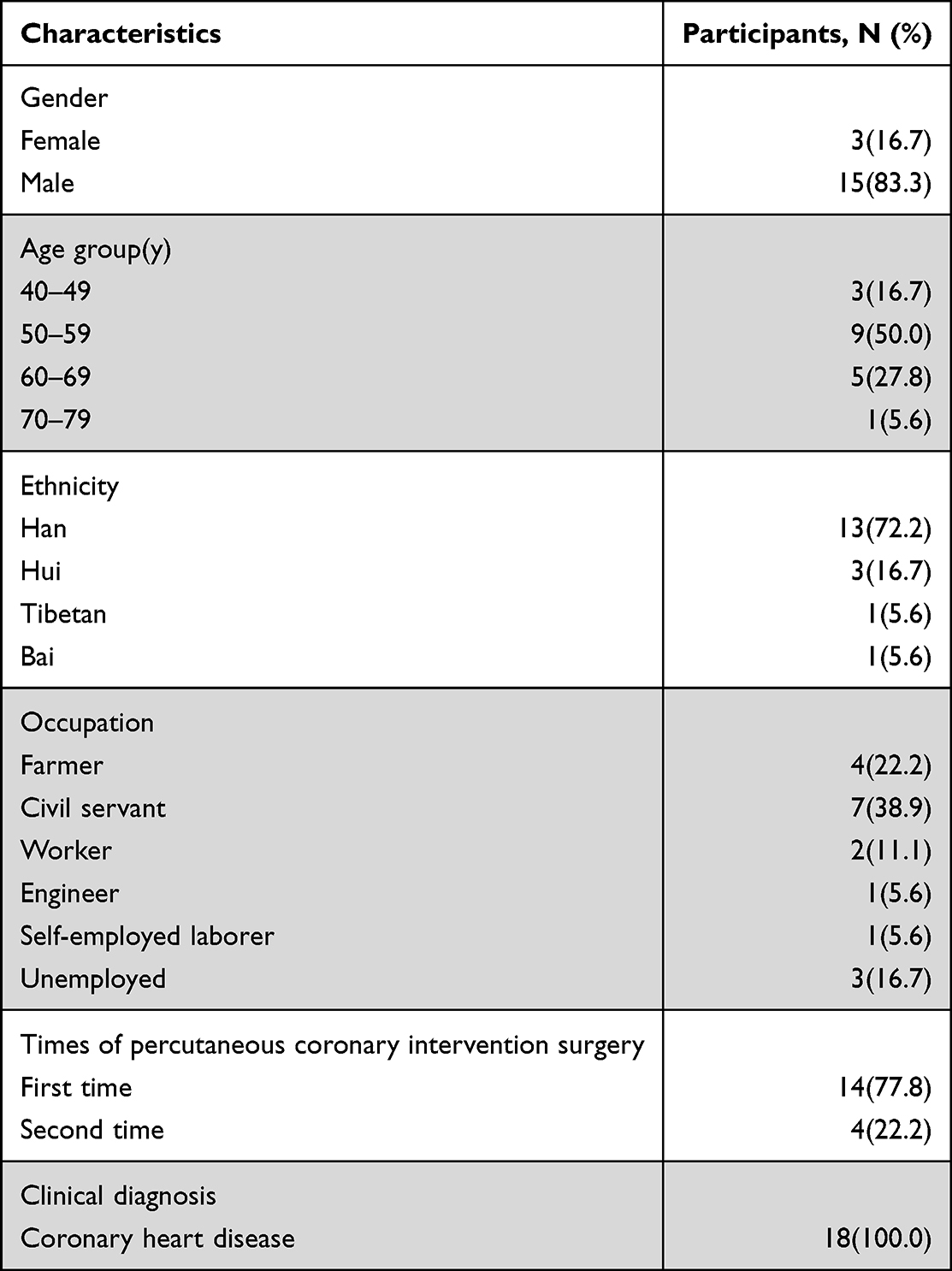 |
Table 2 Participant Demographics |
Seven categories with some subcategories were constructed from the data, categorized into three main domains. Firstly, individual factors include (i) Personal coping with healthy lifestyle requirements (tried but failed; I can do it), (ii) individual perception and feeling toward disease (knowing about the disease; belief of cure; fears of relapse), and (iii) personal benefits (improved health; meaning of life). Secondly, social factors include (i) social facilitators (family resources; healthcare support), (ii) social barriers (inconvenient medical care service; conflicting information). Finally, cultural factors include (i) way of living (dietary habits; key roles of yan (cigarette) and jiu (alcohol) in Chinese society), (ii) way of thinking (fatalism and Confucian familism). Among the categories and subcategories, belief of cure, improved health, and meaning of life were generated in the last two interviews, whereas fatalism and conflicting information appeared in the first two interviews and were not generated in the third time. They are shown in Table 3 and Figure 1. After these interviews, some participants kept contact with the interviewer and expressed their agreement with our research findings.
 |
Table 3 Domains, Categories, and Subcategories in Different Timepoints |
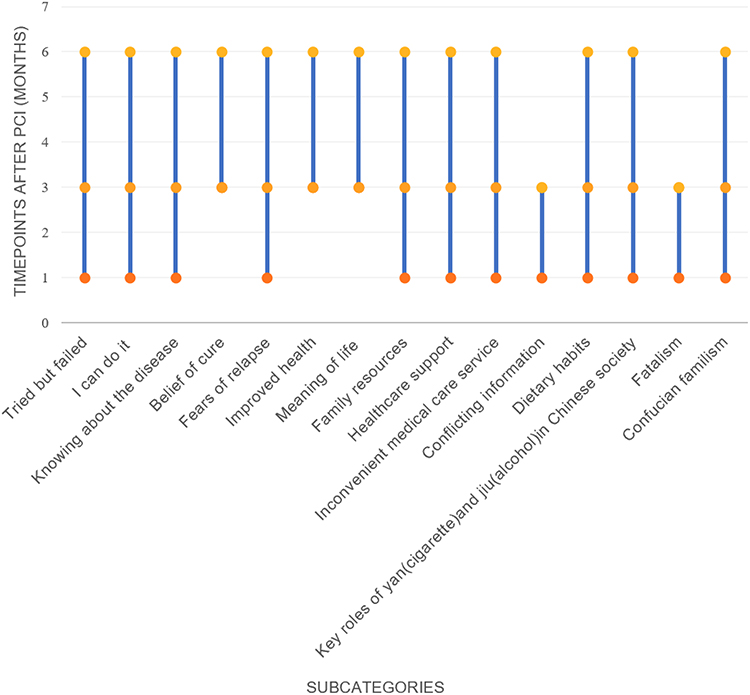 |
Figure 1 Longitudinal Changes of Subcategories at Different Timepoints. The horizontal axis represents subcategories while the dots of vertical axis represent the time point when subcategories appear. |
Domain A: Individual Factors
Category 1: Personal Coping with Healthy Lifestyle Requirements
Subcategory 1: Tried but Failed
Tried but failed was generated in three interviews. Some participants expressed that they tried to follow healthy lifestyle, but they could not resist the temptation of delicious food or cigarettes, even if they knew that these things were not good for their condition. In the end, they failed to practice health behaviors.
When I saw bacon and wine being brought to on the table, I couldn’t help but eat and drink, unless I left the place where I was, I couldn’t stop… [P16, T3]
To be honest, I once tried to quit smoking, however, it is like taking Marijuana. When it’s time to taking, you’ll feel dizzy if you don’t take. [P7, T2]
Subcategory 2: I Can Do It
I can do it was generated in three interviews. Some participants stated that they could adhere to a healthy lifestyle for the sake of health, and they truly did that and maintained it.
After the surgery, I believe I can quit smoking and drinking for my health, and I did it, now I won’t drink a sip of wine… [P5, T1]
Category 2: Individual Perception and Feeling Toward Disease
Subcategory 1: Knowing About the Disease
Knowing about the disease was generated in three interviews. Some participants lacked disease-related knowledge at the beginning. They did not know what to eat, how to exercise, which led them to adopt many unhealthy behaviors. However, most participants could actively learn some knowledge, obtain health information independently (search online or consult a doctor) and apply this health information to their daily lives over time.
I didn’t know before that smoking was so harmful to blood vessels, but later I learned that nicotine can accelerate platelet aggregation, which can also cause blockage in my blood vessels, right? I keep it in mind, so I can’t smoke anymore, then I quit it… [P16, T2]
Subcategory 2: Belief of Cure
Belief of cure was generated in the last two interviews. Some participants reflected that they had been cured and that there was no need to practice health behaviors. They smoked and did not follow medical advice to take medication or see the doctor regularly. Moreover, some participants believed that PCI would solve their health problems even if the disease relapsed. They thought the surgery did not cause them much pain, so they attached less importance to their health behaviors.
This is just a minor operation, I think I’m recovering very well… smoking should be fine. [P2, T3]
There is no need to take medication… If something wrong, I’ll put in another one(stent). Anyway, I have been implemented four stents, and it doesn’t matter if adding another one. Stents can cure me. [P7, T3]
Subcategory 3: Fear of Relapse
Fear of relapse was generated in three interviews. Some participants were afraid of the recurrence of CHD, and thinking of the disease all day, which made them anxious with no motivation to maintain health behaviors. In contrast, due to fear of relapse, some participants tried their best to avoid relapse, such as adjusting their diet habits proactively, taking medicine according to the doctor’s advice and insisting on exercising. All of the above highlights the “double-edged sword” role of fear of relapse in patients’ health behaviors.
I heard there is still a risk of blood vessel block again after percutaneous coronary intervention… I’m worried and afraid, I am haunted by the idea of relapse and I don’t care about healthy diet or exercise. [P18, T1]
En…I’m very worried about the blood vessels getting clogged again, so I hope I can persist, and adjust my diet well to avoid further congestion… [P9, T2]
Category 3: Personal Benefits
Subcategory 1: Improved Health
Improved health was generated in the last two interviews. Some participants reported that they had experienced the benefits of adhering to health behaviors. For example, they had lost weight and pulmonary function improved after quitting smoking, and they were willing to adhere to a healthy lifestyle for the long term.
After taking medication regularly and adjusting diet, my weight remains normal, blood lipids have decreased…I also feel the benefit of quitting smoking. I used to cough a lot, my lungs were often infected, now I can breathe well and no longer cough. [P11, T2]
Subcategory 2: Meaning of Life
Meaning of life was generated in the last two interviews. Some participants reported that they gained happiness and had a more profound understanding of their own life value. They stated that even though some of their health behaviors had little effect in the short term, they enjoyed exercising and changing their diet. They are more willing to keep healthy lifestyle, thus forming a virtuous cycle.
At the beginning, it may be a bit difficult to control diet. As you get used to it, you will realize that it is not as difficult as before. After losing weight, your health is better and your life starts to become meaningful. [P3, T3]
I feel like my whole life has changed, I am now in a better mindset and more willing to make new changes to maintain my health…everything is moving to the right direction. [P4, T3]
Domain B: Social Factors
Category 1: Social Facilitators
Subcategory 1: Family Resources
Most participants talked about the importance of family resources during three interviews. Some participants believed that they could practice health behaviors well with the help of family members. However, some participants stated that they did not have favorable conditions to adopt a healthy lifestyle and if they had available resources, they could practice health behaviors either.
There are doctors in my family. My wife is a retired doctor, my daughter-in-law has a master’s degree from a medical college. I tell them about my condition, they prescribe medication for me, so I never miss taking medication. [P16, T2]
There are many people in our family who eat together, and it’s impossible to cook for me alone. [P8, T3]
Subcategory 2: Healthcare Support
Healthcare support was generated in three interviews. Some participants stated that going to the hospital was troublesome and inconvenient and they gave up the follow up visits to the doctor. Whereas, some participants expressed that a good medical environment is beneficial for the development of health behavior, including doctors’ skills and personality.
I’m afraid of going to the hospital and having to undergo various examinations that I don’t know about, which makes me feel troublesome and cumbersome. Thus I don’t want to go for a check at all. [P3, T1]
The doctors here are highly skilled and patient. They often ask me if I feel uncomfortable after the surgery, they explained the dietary notes to me… so I will do as they said. [P5, T2]
Category 2: Social Barriers
Subcategory 1: Inconvenient Medical Care Service
Inconvenient medical care service was generated in three interviews. Some participants thought that the process of going to the hospital for a follow-up examination is inconvenient, whether on the way to the hospital or in the hospital. Therefore, they did not want to go to hospital even they should be treated and followed up.
It takes two hours from my home to the high-speed rail station, and six hours from the high-speed rail station to the hospital. It’s too far, so if I can tolerate the pain, I don’t want to go to the hospital. [P4, T1]
In hospital, especially in large ones, it is necessary to make appointments in advance, and payment and examination are all in different places, which leaves me at a loss. [P3, T2]
Subcategory 2: Conflicting Information
Conflicting information was generated in the first two interviews. Some participants expressed confusion due to the large amount of conflicting or ambiguous information. They do not know who to listen to and what kind of choices to make.
There exists too much health information online. The doctors in the hospital also gave me a lot of information, but lots of information were somewhat different, so I don’t know who to believe or how to manage my lifestyle. [P1, T2]
Domain C: Cultural Factors
Category 1: Way of Living
Subcategory 1: Dietary Habits
Dietary habits were generated in three interviews. Some participants stated in their neighborhood, they always loved to eat sour and hot food such as pickles, ham and bacon etc. They believed that these habits have been deeply ingrained in their blood and were difficult to change.
I am Bai and we always enjoy pickled products such as ham, salted meat, and sausages. I have been eating this way since I was young, and I never thought about eating anything else. It is a traditional dietary habit… [P16, T1]
We eat a lot of salt, and dried beef is marinated… The habit of cooking is difficult to change. [P18, T2]
Subcategory 2: Key Roles of Yan (Cigarette) and Jiu (Alcohol) in Chinese Society
The key role of yan (cigarette) and jiu (alcohol) was generated in three interviews. Some participants expressed that yan and jiu were important means of making friends, and jiu was a kind of social media and symbol of respect for people. They indicated that it was difficult to refuse jiu in various social situations.
I started smoking when I was seventeen years old…I was curious at that time. Everyone is smoking, passing cigarettes back and forth can make friends… [P6, T1]
The minority nationality in our aera love drinking, you won’t hear the truth if you don’t drink with them. When you hold a glass of wine, they will consider you as their friend and tell you sincere words. Otherwise, they will think that you look down on them. [P11, T1]
Category 2: Way of Thinking
Subcategory 1: Fatalism
During the first two interviews, some participants believed that having CHD was not influenced by their own behaviors but by fate. They stated that fate was doomed and could not be changed, and they lacked the motivation to practice health behaviors. However, in the third interview, no participants mentioned fatalism.
If God wants you to get this disease, you will have to get sick. [P6, T1]
It’s hard to say, some people get sick even if they don’t drink, and some people drink every day but nothing happens. After all, it’s determined by fate. [P11, T1]
Subcategory 2: Confucian Familism
Confucian familism was generated in three interviews. Some participants believed that in order to alleviate family concerns, they should actively practice health behaviors such as taking medication regularly, which showed their responsibility for the families. Some participants expressed that to take care of their children and support elderly parents, they had to engage in hard work and put families’ benefits first instead of their own health.
My mother is concerned about my condition after percutaneous coronary intervention, for her, I should listen to the doctor’s advice and take medicine regularly. [P14, T1]
I can’t lead a regular life now. My daughter needs a lot of money in college and my parents also need support, so I have to work all the time. [P13, T3]
Discussion
Our study provides additional perspectives and insights into the dynamic changes in the determinants of health-related behaviors of patients with CHD after PCI over time. Compared to previous studies and combined with Chinese traditional culture, some new determinants occurred. The determinants of health-related behaviors of patients include individual, social and cultural factors. Belief of cure, improved health and meaning of life were generated in the last two interviews. Conflicting information and fatalism were generated in the first two interviews. Other categories and subcategories were generated in three interviews.
“Personal coping with healthy lifestyle requirements” includes negative coping such as “tried but failed” and positive coping such as “I can do it”. This may be explained by patient’s self-efficacy, which is the main predictor of self-care behaviour in patients with CHD and can affect long-term compliance with various health-related behaviors including diet.34,35 Patients with high self-efficacy tend to maintain a good health behavior, whereas patients with low self-efficacy have poor self-care such as adopting unhealthy lifestyle.36 Present studies have shown that patients with CHD tends to have a low to moderate average self-efficacy level,35 and it is reported that self-efficacy of patients with CHD was in the middle level among Chinese population.37 Given the critical role of self-efficacy in health-related behaviors of patients with CHD and its moderate level, effective interventions targeting improving patiens’ self-efficacy are needed, including vicarious learning through observing and modeling the behavior of others who can adhere to the health-related behavior, and support of professionals or family members based on any one of four principles (Mastery, Modeling, Social persuasion, and Understanding) of Bandura’s cognition theory.38
Our research findings indicated that patients’ disease-related knowledge affects one’s attitudes towards health-related behaviors, and is crucial for inducing changes in individual’s health-related behaviors.39,40 Therefore, the significant impact of disease-related knowledge on patients’ adherence to health behaviors must be considered. Multiple ways to acquire disease-related knowledge, such as discharge guidance from physicians and nurses, and health manuals should be provided to improve their health behaviors in the end.
Our study identified that belief of cure influenced patients’ health behaviors and this determinant occurred sometime after PCI. The reason is that although patients have symptoms that are relieved immediately after PCI, the experience of hospitalization and surgery remind them that they are still patients and need to be cared for or cured.31 However, with time goes by, patients are feeling much better and have the idea that they are cured, and some participants mistakenly hold the belief that they have been cured by PCI, so they no longer adhere to health behaviors, which is in correspondence with previous studies.11 Therefore, it is necessary to inform patients early about the uncertain benefits of stents and provide health education to make them aware that CHD is a chronic disease that cannot be cured solely through PCI.41 In our study, fear of relapse was found out to have conflicting effects on patients’ health behaviors, which is supported by other studies. A study reported that fear of relapse caused patients to be psychologically distressed and that their health behaviors were negatively affected.42 In contrary, a previous study also showed that fear of relapse seems to motivate patients to participate in cardiac rehabilitation and maintain healthy lifestyle.31 Although fear of recurrence has shown positive aspects in our research and some studies, there is still insufficient research in the field of cardiovascular disease. Therefore, future studies are needed to verify its impact on patients’ health behaviors.
Our study showed that personal benefits such as improved health and meaning of life could motivate patients to adhere to a healthy lifestyle, which has been reported in other studies.43,44 A study has shown that arterial dysfunction caused by catheterization recovers 4–12 weeks later, at this stage, patients are not yet able to fully engage in health behaviors.45 With the recovery of arterial function, patients gradually adopt health behaviors that bring health benefits and meaning of life to patients.44 This may be the reason why these determinants emerged in the last two interviews. The changes in health behaviors and the meaning of life (subjective well-being) have a long-term impact on the other party, and these mutual long-term benefits are driving forces for promoting personal and social health, which is beneficial for political decision-making.44 Thus nurses and physicians should make full use of personal benefits to encourage patients to practice health behavior.
Our results showed that patients with available family resources have more confidence and capability in fulfilling health behaviors. Family support, household income, and marriage are the driving forces for healthy lifestyle changes and participation in cardiac rehabilitation.46–48 Healthcare providers should help patients and their families make full use of family resources to promote the health behavior practices of patients. In our study, participants expressed that they did not participate in follow-up visits to the doctor due to fears of various unknown examinations and cumbersome procedures in the hospital. This is in consistent with the result of Pettersen and associates,14 in which physicians having too many patients and too little time results in insufficient information obtained by patients, and hectic hospital conditions also make them avoid going to the hospital. However, some patients expressed that the guidance from healthcare professionals (HCPs) can enable them to practice health behaviors, which has been supported by other studies.15,46 Therefore, in order to promote patients to practice health behaviors, professional and clear health guidance should be provided by HCPs, and the premise is that policymakers should also provide favorable conditions for them, such as an orderly and relaxed consultation environment.
Inconvenient medical care service, affected patients’ behaviors in treatment and follow-up, which is consistent with other studies.49,50 In China, due to the disparity in urban-rural development, medical resources are concentrated in large urban hospitals, while rural medical institutions are relatively poor.50 Rural residents living in remote areas with inconvenient transportation often face with the dilemma of accessing medical services.50 Therefore, Chinese medical system for allocating medical resources still needs to be further improved. Besides, remote healthcare and simplification of medical appointment booking procedures may help address the aforementioned barriers. Our findings suggested that conflicting information make patients confused about how to take medication and manage their lifestyle correctly. Nurses, physicians and pharmacists are important sources of patients’ conflicting information, and the internet plays an indispensable role in patients’ access to health information.51,52 Multiple information sources increase the risk of conflicting information. Conflicting information was generated in the first two interviews but did not appear in the third interview. This may be associated with the fact that PCI has a shortened hospitalization time, which might result in less in-hospital education time and a low level of patient knowledge.12 Patients with less knowledge might be confused by inconsistent information at first, which might influence patients’ health behavior adoption.52 Patients’ ability to access information improves by surfing the internet and communicating with the healthcare team over time.53,54 Therefore, in the later stage, patients are not confused by conflicting information. Accurate health guidance and information need to be provided by healthcare teams (including nurses, physicians and pharmacists) to help patients avoid information confusion, be aware of the risk factors and better engage in health behaviors.
Our results showed that participants enjoyed eating pickled, spicy and sour foods, which are common around their neighborhood and difficult to change. In China, each ethnic group has unique dietary habits, which are often associated with the cardiovascular disease they suffer from.55 For example, Tibetan residents’ meat consumption mainly consists of red meat such as yak beef and lamb, their main beverages are buttered tea and barley liquors, which provide a large source of protein, fat, and sodium for the Tibetan diet, and the latter two are often related to cardiovascular disease and other chronical diseases.56 Besides, people believe that the taste of food is more important than its health benefits, they have been accustomed to the salty taste of food and do not want to make changes.57,58 Detailed dietary guidance should be provided and the relationship between unhealthy dietary habits and CHD should be explained to patients by HCPs based on their cultural background.
Yan (cigarette) and jiu (alcohol) are important components in the long history and culture of China, playing important roles in celebrations, gatherings, and maintaining a working relationship.59,60 Our study showed that participants smoke and drank jiu under the influence of their peers, as well as to work and make friends, which is in accordance with previous studies.59,60 In Chinese culture, cigarettes are often gifted as “the name card” to business partners or employers or given as a “gift” to elders to express filial piety.61 In addition, cigarettes are often used as a form of entertainment, and people like to sit in the house smoking and chatting together.61 As the main growing region of tobacco, Yunnan Province has higher tobacco exposure levels than the national level, which may become one of the obstacles for people to quit smoking.29 System and cultural factors pose challenges for tobacco reduction in China. Policymakers should formulate corresponding programmes to facilitate smoking cessation and control the sale of tobacco, and highlighting the urgent need for China to implement comprehensive bans on smoking throughout the country.62
Baijiu (alcohol) has a history of more than 9000 years and is used in various scenarios.63 In ancient times, generals and warriors would be rewarded with goblets of wine by king, bandits would drink alcohol to celebrate an especially lucrative robbery and jiu is also used for wedding banquets and children’s man yue jiu (滿月酒), which is the occasion that their parents invite family and friends to attend a feast when their children are one month old.64 In Chinese culture, refusing someone’s invitations to drink jiu is regarded as impolite, and even adolescent drinking is considered a socially acceptable behavior.65 Furthermore, ethnic minorities in China have a strong tradition of drinking, and tend to exhibit a higher prevalence of drinking than Han people.66 The long-standing alcohol culture hinders patients from practicing health behaviors. However, aboriginal culture enculturation has been found to be an important protective factor for alcohol consumption. Chinese traditional culture was dramatically affected by Confucianism, which encourages moderate and moral drinking, yet against frequent and solitary drinking.67 Moderate drinking of baijiu is considered as beneficial for health, and it also strengthens the close connection between social circles and families.59
Influenced by Buddhism and Taoism, some Chinese patients attribute their life events, including health and disease, to Ming (also known as fate), which is in consistent with our results.68 In China, Buddhism emphasizes the cycle of life, and the occurrence, nature, duration, and content of a relationship are considered destined or inevitable.64 Taoism advocates “let it be”, it portrays a belief in a natural lifecycle, according to which followers perceive death to be a natural and undisturbed form.69 Under these cultural backgrounds, people will use reincarnation, fate, and karma to explain their disease. This attitude alleviates patients’ sense of helplessness to some extent, but this fatalism may also hinder patients’ health behaviors and compliance.68 Therefore, when planning intervention measures for patients, it is important to understand their cognition about disease situations to promote their positive coping behaviors. Fatalism was generated in the first two interviews and disappeared in the last interview. This may be because the fact patients feel stressed about losing control over external factors after PCI in the early stage and they are more likely to explain such events using fatalism belief.70 Nevertheless, patients gradually feel better and believe that they have control of their lives, and they realize the importance of living in the present and their sense of responsibility toward their families, which provides them with the courage and motivation to continue living and reduces their sense of helplessness toward life.68
Chinese familism is deeply influenced by Confucianism, which provides the most important values and institutional system for Chinese people and influences their behavior and cognition.64 It has both positive and negative effects on patients’ health behaviors, which is a novel finding of this study. Our study showed that patients take medication regularly and practice healthy lifestyles to alleviate family concerns. This is an important manifestation of Chinese filial piety, in which the personal body is considered a gift from their parents or ancestors and individuals should take care of their own bodies to fulfill their obligations to the family.71 In addition, our results showed that patients had to choose hard jobs to support their parents and children, which led patients unable to continue leading a regular lifestyle. This can be explained by another aspect of filial piety, in which children have an obligation to respect and obey their parents, as well as to provide emotional and economic assistance.72,73 Meanwhile, Chinese parents seek available resources for their children such as bearing higher educational costs.74 Under this cultural influence, parents may sacrifice their health to meet family members’ needs. HCPs should identify the reasons behind patients’ health-related behaviors considering cultural issues and use the positive aspects to offset negative ones, which may facilitate their health behaviors.
Strengths and Limitations
This study explored the determinants of health-related behaviors among patients with CHD after PCI using longitudinal qualitative research method in a unique cultural background. It helps to understand patients’ views on the determinants of health-related behaviors in specific cultural contexts over time. The results can inspire HCPs and researchers from other regions of China and worldwide to explore the determinants of patients’ health behaviors and develop culturally sensitive time specific strategies. However, there are some limitations to this study. Firstly, the participants in this study only came from Yunnan Province, China, which reduces the generalizability of this study. Secondly, due to language limitations and the low proportion of ethnic minorities, our sample only includes three ethnic minorities, which may lead to the neglect of the impact of other ethnic cultures on the health behaviors of patients. Further research can be conducted between different hospitals and ethnic groups, and experimental studies can be combined to verify the impact of determinants on the health behavior of a large number of patients.
Conclusion
This study explored the determinants of health-related behaviors of patients with CHD after PCI in the context of Chinese cultural background at different timepoints. The results indicated that individual factors, social conditions, and cultural factors all have impacts on their health-related behaviors, which might guide the development of intervention measures for patients with CHD after PCI. In particular, we suggest that health promotion programs for patients after PCI should be culturally sensitive. In addition, attention should be given to the dynamic changes in determinants of health-related behaviors when providing intervention measures for patients. For example, measures to rectify the wrong perception of belief of cure, and role models showing improved health and meaning of life should be stressed among patients in later stages after PCI. Furthermore, the effects of conflicting information and fatalism on patients’ health behaviors are the focus for health care professionals in the early stage after PCI.
Abbreviations
CHD, Coronary heart disease; PCI, Percutaneous coronary intervention; COREQ, Consolidated criteria for reporting qualitative research; HCPs, healthcare professionals.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The author thanks all participants who voluntarily participated in this study, as well as nurses who provided assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ananth CV, Rutherford C, Rosenfeld EB, et al. Epidemiologic trends and risk factors associated with the decline in mortality from coronary heart disease in the United States, 1990–2019. Am Heart J. 2023;263:46–55. doi:10.1016/j.ahj.2023.05.006
2. Lin J, Yang R, Zhang Y, et al. The mediation effects of metabolic and immune–inflammation factors on the depression–premature coronary heart disease association. J Affect Disord. 2023;331:434–441. doi:10.1016/j.jad.2023.03.046
3. Hu YY, Jiang X, Mao FY, et al. Effect of positive event recording based on positive psychology on healthy behaviors and readmission rate of patients after PCI: a study protocol for a prospective, randomized controlled trial. Trials. 2022;23(1):1013. doi:10.1186/s13063-022-06964-9
4. Prashar A, Mitchell K, Hopkins A, Sader M, Prasan AM. Cost-effectiveness and safety of same-day Discharge after elective percutaneous coronary intervention. Hearts. 2021;2(4):561–569. doi:10.3390/hearts2040043
5. Qin S, Gu Y, Song T. Effect of peer support on patient anxiety during the coronary angiography or percutaneous coronary intervention perioperative period: a protocol for a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2020;10(3):e031952. doi:10.1136/bmjopen-2019-031952
6. Hu W, Jiang J. Hypersensitivity and in-stent restenosis in coronary stent materials. Front Bioeng Biotechnol. 2022;10:1003322. doi:10.3389/fbioe.2022.1003322
7. Wang Y, Xian Y, Chen T, et al. Effect of lifestyle changes after percutaneous coronary intervention on revascularization. BioMed Res Int. 2020;2020:1–6.
8. Rahhal A, Mahfouz A, Khir F, et al. Medications adherence post‐primary percutaneous coronary intervention in acute myocardial infarction: a population‐based cohort study. J Clin Pharm Ther. 2021;46(3):772–779. doi:10.1111/jcpt.13348
9. Slovinec D’Angelo ME, Pelletier LG, Reid RD, Huta V. The roles of self-efficacy and motivation in the prediction of short- and long-term adherence to exercise among patients with coronary heart disease. Health Psychol. 2014;33(11):1344–1353. doi:10.1037/hea0000094
10. Lu M, Hravnak M, Ma J, et al. Prediction of changes in adherence to secondary prevention among patients with coronary artery disease. Nurs Res. 2020;69(5):E199–E207. doi:10.1097/NNR.0000000000000433
11. Perk J, Hambraeus K, Burell G, Carlsson R, Johansson P, Lisspers J. Study of patient information after percutaneous coronary intervention (SPICI): should prevention programmes become more effective? EuroIntervention. 2015;10(11):e1–e7. doi:10.4244/EIJV10I11A223
12. Wójcicki K, Krycińska R, Tokarek T, et al. Knowledge and prevalence of risk factors for coronary artery disease in patients after the first and repeated percutaneous coronary intervention. Kardiol Pol. 2020;78(2):147–153. doi:10.33963/KP.15070
13. Kähkönen O, Saaranen T, Kankkunen P, Lamidi ML, Kyngäs H, Miettinen H. Predictors of adherence to treatment by patients with coronary heart disease after percutaneous coronary intervention. J Clin Nurs. 2018;27(5–6):989–1003. doi:10.1111/jocn.14153
14. Pettersen TR, Fridlund B, Bendz B, et al. Challenges adhering to a medication regimen following first-time percutaneous coronary intervention: a patient perspective. Int J Nurs Stud. 2018;88:16–24. doi:10.1016/j.ijnurstu.2018.07.013
15. Kähkönen O, Oikarinen A, Vähänikkilä H, Kyngäs H. Association between perceived health and adherence to treatment after percutaneous coronary intervention: a long‐term follow‐up study. J Adv Nurs. 2022;78(6):1653–1664. doi:10.1111/jan.15069
16. Xiao L, Wang P, Fang Q, Zhao Q. Health-promoting lifestyle in patients after percutaneous coronary intervention. Korean Circ J. 2018;48(6):507. doi:10.4070/kcj.2017.0312
17. Hamzah SR, Suandi T, Ismail M, Muda Z. Association of the personal factors of culture, attitude and motivation with health behavior among adolescents in Malaysia. Int J Adolesc Youth. 2019;24(2):149–159. doi:10.1080/02673843.2018.1482772
18. Iwelunmor J, Newsome V, Airhihenbuwa CO. Framing the impact of culture on health: a systematic review of the PEN-3 cultural model and its application in public health research and interventions. Ethn Health. 2014;19(1):20–46. doi:10.1080/13557858.2013.857768
19. Peking Union Medical College Press. National Center for Cardiovascular Diseases Annual Report on Cardiovascular Health and Diseases in China (2022). Peking: Peking Union Medical College Press; 2023:8–9.
20. Liu F, Han J, Wang Y, Jin Y. The later status and impact factors of physical activity among patients after percutaneous coronary intervention in China. Am J Health Behav. 2022;46(6):654–663. doi:10.5993/AJHB.46.6.8
21. Liu J, Zhuyu Z, Gaoyu C, et al. Long-term effect of persistent smoking on the prognosis of Chinese male patients after percutaneous coronary intervention with drug-eluting stent implantation. J Cardiol. 2013;62(5):283–288. doi:10.1016/j.jjcc.2013.05.010
22. He QH, Zheng J, Liu JL, Wang J, You LM. Predictors of Medication Adherence of Patients With Coronary Heart Disease After Percutaneous Coronary Intervention: a Structural Equation Modeling Based on the Extended Theory of Planned Behavior. J Cardiovasc Nurs. 2022;37(4):350–358. doi:10.1097/JCN.0000000000000755
23. SmithBattle L, Lorenz R, Reangsing C, Palmer JL, Pitroff G. A methodological review of qualitative longitudinal research in nursing. Nurs Inq. 2018;25(4):e12248. doi:10.1111/nin.12248
24. Tuthill EL, Maltby AE, DiClemente K, Pellowski JA. Longitudinal qualitative methods in health behavior and nursing research: assumptions, design, analysis and lessons learned. Int J Qual Methods. 2020;19:160940692096579. doi:10.1177/1609406920965799
25. Balmer DF, Richards BF. Conducting qualitative research through time: how might theory be useful in longitudinal qualitative research? Adv Health Sci Educ. 2022;27(1):277–288. doi:10.1007/s10459-021-10068-5
26. Audulv Å, Hall EOC, Kneck Å, et al. Qualitative longitudinal research in health research: a method study. BMC Med Res Methodol. 2022;22(1):255. doi:10.1186/s12874-022-01732-4
27. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
28. Ma F, Li J, Liang H, Bai Y, Song J. Baccalaureate nursing Students’ perspectives on learning about caring in China: a qualitative descriptive study. BMC Med Educ. 2014;14(1):42. doi:10.1186/1472-6920-14-42
29. Wang XM, Wu C, Golden AR, Le C. Ethnic disparities in prevalence and patterns of smoking and nicotine dependence in rural southwest China: a cross-sectional study. BMJ Open. 2019;9(9):e028770. doi:10.1136/bmjopen-2018-028770
30. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
31. Throndson K, Sawatzky JAV, Schultz A. Exploring the perceptions and health behaviours of patients following an elective ad-hoc percutaneous coronary intervention: a qualitative study. Can J Cardiovasc Nurs. 2016;26(2):25–33.
32. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
33. Zhuo Q, Liang H, Bai Y, et al. Perceptions of patients undergoing percutaneous coronary intervention on pre‐operative education in China: a qualitative study. Health Expect. 2021;24(1):121–130. doi:10.1111/hex.13156
34. Chair SY, Wong KB, Tang JYM, Wang Q, Cheng HY. Social support as a predictor of diet and exercise self-efficacy in patients with coronary artery disease. Contemp Nurse. 2015;51(2–3):188–199. doi:10.1080/10376178.2016.1171726
35. Sugiharto F, Nuraeni A, Trisyani Y, Putri A, Armansyah N, Zamroni A. A scoping review of predictors associated with self-efficacy among patients with coronary heart disease. Vasc Health Risk Manag. 2023;19:719–731. doi:10.2147/VHRM.S435288
36. Pedretti RFE, Hansen D, Ambrosetti M, et al. How to optimize the adherence to a guideline-directed medical therapy in the secondary prevention of cardiovascular diseases: a clinical consensus statement from the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2023;30(2):149–166. doi:10.1093/eurjpc/zwac204
37. Zhu Y, Song Y, Wang Y, et al. Relationships among social support, self-efficacy, and patient activation in community-dwelling older adults living with coronary heart disease: a cross-sectional study. Geriatr Nur. 2022;48:139–144. doi:10.1016/j.gerinurse.2022.09.008
38. Ouyang RG, Long Y, Zhang JQ, Cao Z. Interventions for improving self-efficacy in patients after stroke based on self-efficacy-related principles of Bandura’s cognition theory: a systematic review and meta-analysis. Top Stroke Rehabil. 2023;30(8):820–832. doi:10.1080/10749357.2023.2172832
39. Jung HG, Yang YK. Factors influencing health behavior practice in patients with coronary artery diseases. Health Qual Life Outcomes. 2021;19(1):3. doi:10.1186/s12955-020-01635-2
40. Cao Q, Xu L, Wen S, Li F. Investigating the influence of the shared decision-making perception on the patient adherence of the home- and exercise-based cardiac rehabilitation after percutaneous coronary intervention. Patient Prefer Adherence. 2021;15:411–422. doi:10.2147/PPA.S292178
41. Pilar IM, William L, Rebecca G, et al. Patient perspectives on the benefits and risks of percutaneous coronary interventions: a qualitative study. Patient Prefer Adherence. 2021;15:721–728. doi:10.2147/PPA.S302146
42. Hall DL, Jimenez RB, Perez GK, et al. Fear of cancer recurrence: a model examination of physical symptoms, emotional distress, and health behavior change. J Oncol Pract. 2019;15(9):e787–e797. doi:10.1200/JOP.18.00787
43. Sialino LD, Wijnhoven HAH, Van Oostrom SH, et al. Perspectives of older women in the Netherlands: identifying motivators and barriers for healthy lifestyles and determinants of healthy aging. BMC Public Health. 2023;23(1):664. doi:10.1186/s12889-023-15611-0
44. Stenlund S, Koivumaa-Honkanen H, Sillanmäki L, Lagström H, Rautava P, Suominen S. Changed health behavior improves subjective well-being and vice versa in a follow-up of 9 years. Health Qual Life Outcomes. 2022;20(1):66. doi:10.1186/s12955-022-01972-4
45. Tryfonos A, Green DJ, Dawson EA. Effects of catheterization on artery function and health: when should patients start exercising following their coronary intervention? Sports Med. 2019;49(3):397–416. doi:10.1007/s40279-019-01055-3
46. Kähkönen O, Kyngäs H, Saaranen T, Kankkunen P, Miettinen H, Oikarinen A. Support from next of kin and nurses are significant predictors of long-term adherence to treatment in post-PCI patients. Eur J Cardiovasc Nurs. 2020;19(4):339–350. doi:10.1177/1474515119887851
47. Li J, Song J, Zhu XL, Chen MF, Huang XF. Analysis of status quo and influencing factors for health-promoting lifestyle in the rural populace with high risk of cardiovascular and cerebrovascular diseases. BMC Cardiovasc Disord. 2023;23(1):118. doi:10.1186/s12872-023-03129-7
48. Sun L, Wu T, Zhang M, Huang S, Zeng Z, Wu Y. Investigation on family support system and willingness of patients to participate in cardiac rehabilitation after percutaneous coronary intervention. Evid Based Complement Alternat Med. 2022;2022:3633188. doi:10.1155/2022/3633188
49. Zhou Y, Huo Q, Du S, et al. Social support and self-efficacy as mediating factors affecting the association between depression and medication adherence in older patients with coronary heart disease: a multiple mediator model with a cross-sectional study. Patient Prefer Adherence. 2022;16:285–295. doi:10.2147/PPA.S337634
50. Wu Y, Wang Q, Zheng F, et al. Effects of the implementation of transport-driven poverty alleviation policy on health care–seeking behavior and medical expenditure among older people in rural areas: quasi-experimental study. JMIR Public Health Surveill. 2023;9:e49603.
51. Hämeen-Anttila K, Jyrkkä J, Enlund H, Nordeng H, Lupattelli A, Kokki E. Medicines information needs during pregnancy: a multinational comparison. BMJ Open. 2013;3(4):e002594. doi:10.1136/bmjopen-2013-002594
52. Santos B, Blondon KS, Van Gessel E, et al. Patients’ perceptions of conflicting information on chronic medications: a prospective survey in Switzerland. BMJ Open. 2022;12(11):e060083. doi:10.1136/bmjopen-2021-060083
53. Ayton DR, Barker AL, Peeters GM, et al. Exploring patient-reported outcomes following percutaneous coronary intervention: a qualitative study. Health Expect. 2018;21(2):457–465. doi:10.1111/hex.12636
54. Ramstad K, Pettersen TR, Brors G, et al. Had percutaneous coronary intervention, now what? Searching the internet for health information. Eur Heart J. 2021;42(Supplement_1):
55. Zhao R, Zhao L, Gao X, et al. Geographic variations in dietary patterns and their associations with overweight/obesity and hypertension in China: findings from China Nutrition and Health Surveillance (2015–2017). Nutrients. 2022;14(19):3949. doi:10.3390/nu14193949
56. Yan Q. Dietary patterns and lifestyles in Tibet and southeastern China in relation to the prevalence of certain chronic diseases. Highlights Sci Eng Technol. 2022;2:46–53. doi:10.54097/hset.v2i.554
57. Bi Z, Liang X, Xu A, et al. Hypertension prevalence, awareness, treatment, and control and sodium intake in Shandong Province, China: baseline results from Shandong–ministry of health action on salt reduction and hypertension (SMASH), 2011. Prev Chronic Dis. 2014;11:130423. doi:10.5888/pcd11.130423
58. Chen J, Liao Y, Li Z, et al. Determinants of salt-restriction-spoon using behavior in China: application of the Health Belief Model. PLoS One. 2013;8(12):e83262. doi:10.1371/journal.pone.0083262
59. Chan RHW, Dong D, Kim JH. Drinking expectancies among Chinese young adults: a qualitative study from Hong Kong. Int J Environ Res Public Health. 2022;19(19):11865. doi:10.3390/ijerph191911865
60. DeLay D, Shen M, Cook RE, Zhao S, Logis H, French DC. Peers influence the tobacco and alcohol use of Chinese adolescents. J Res Adolesc. 2023;33(2):591–602. doi:10.1111/jora.12828
61. Mao A, Yang T, Bottorff JL, Sarbit G. Personal and social determinants sustaining smoking practices in rural China: a qualitative study. Int J Equity Health. 2014;13(1):12. doi:10.1186/1475-9276-13-12
62. Mao A, Bottorff JL, Oliffe JL, Sarbit G, Kelly MT. A qualitative study on Chinese Canadian male immigrants’ perspectives on stopping smoking: implications for Tobacco Control in China. Am J Mens Health. 2018;12(4):812–818. doi:10.1177/1557988316644050
63. Sakandar HA, Hussain R, Farid Khan Q, Zhang H. Functional microbiota in Chinese traditional Baijiu and Mijiu Qu (starters): a review. Food Res Int. 2020;138:109830. doi:10.1016/j.foodres.2020.109830
64. Catherine TLS. Themes in Chinese Psychology. Singapore: Cengage Learning Asia Pte Ltd; 2008.
65. Yoon S, Lam WWT, Sham JTL, Lam TH. Learning to drink: how Chinese adolescents make decisions about the consumption (or not) of alcohol. Int J Drug Policy. 2015;26(12):1231–1237. doi:10.1016/j.drugpo.2015.09.001
66. Yu Z, Assanangkornchai S, Wichaidit W, He L, Feng C. Inter-ethnic differences in self-reported alcohol-related harm to children in Han vs. Yi ethnic minority households in Yunnan Province, China. J Ethn Subst Abuse. 2023;1–14. doi:10.1080/15332640.2022.2164755
67. He J, Assanangkornchai S, Cai L, McNeil E. Disparities in drinking patterns and risks among ethnic majority and minority groups in China: the roles of acculturation, religion, family and friends. Drug Alcohol Depend. 2016;159:198–206. doi:10.1016/j.drugalcdep.2015.12.028
68. Xie C, Li L, Li Y. “Alive day is the day”: a qualitative study of experiences of learned helplessness in maintenance haemodialysis patients. Risk Manag Healthc Policy. 2023;16:231–245. doi:10.2147/RMHP.S401205
69. Goss PE, Strasser-Weippl K, Lee-Bychkovsky BL, et al. Challenges to effective cancer control in China, India, and Russia. Lancet Oncol. 2014;15(5):489–538. doi:10.1016/S1470-2045(14)70029-4
70. Zuo B, Zhang X, Wen Fang F, Zhao Y. The influence of stressful life events on depression among Chinese university students: multiple mediating roles of fatalism and core self-evaluations. J Affect Disord. 2020;260:84–90. doi:10.1016/j.jad.2019.08.083
71. Wesołowski Z. The virtues of Xiao (Filial Piety) and Ti (Brotherly Obedience) as two pillars of Confucian Familism. Stud Warm. 2022;59:315–336.
72. Hung ATW. Family caring for the elderly during the pandemic in Hong Kong: perspective from Confucian Familism. Public Adm Policy. 2022;25(1):13–24.
73. Smith CS, Hung LC. The influence of eastern philosophy on elder care by Chinese Americans: attitudes toward long-term care. J Transcult Nurs. 2012;23(1):100–105. doi:10.1177/1043659611423827
74. Bifarin O, Quinn C, Breen L, Zhang B, Oyebode J. Intersections between the culture of Xiao (孝) and caring for older relatives in China: perspectives of United Kingdom-based Chinese students on future care for their parents. Ageing Soc. 2022;1–21. doi:10.1017/S0144686X22001118
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.