")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Penehyclidine for Prevention of Postoperative Nausea and Vomiting in Patients Undergoing Gynecological Laparoscopic Surgery Under Combined Intravenous and Inhalation Anesthesia: A Randomized, Double-Blind, Placebo-Controlled Trial
Authors Zhao K , Gao Y, Zhang J, Wang S, Chen J, Guo F , Wang S
Received 7 December 2023
Accepted for publication 13 February 2024
Published 1 March 2024 Volume 2024:18 Pages 685—697
DOI https://doi.org/10.2147/DDDT.S453327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Kai Zhao,1,2 Yali Gao,1,2 Jianping Zhang,1,2 Shan Wang,1,2 Jiaqi Chen,1,2 Fenglin Guo,1,2,* Sheng Wang1,2,*
1Department of Anesthesiology, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China (USTC), Hefei, Anhui, People’s Republic of China; 2Department of Anesthesiology, Anhui Provincial Hospital, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fenglin Guo; Sheng Wang, Department of Anesthesiology, The First Affiliated Hospital of USTC (Anhui Provincial Hospital), Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +86 15395006763 ; +86 19156007726, Email [email protected]; [email protected]
Purpose: We designed this study to investigate the effect of intravenous use of penehyclidine on postoperative nausea and vomiting (PONV) after gynecological laparoscopic surgery.
Patients and Methods: Ninety-two Women Patients (Aged ≥ 18) Scheduled for Elective Gynecologic Laparoscopy Were Enrolled in the Current Study. Patients Were Equally Randomized Assigned Into Penehyclidine group (PHC group: received a bolus of penehyclidine 10 μg/kg during the induction of anesthesia, then followed by a continuous infusion of 10 μg/kg penehyclidine at a fixed rate of 2.0 mL/h in postoperative intravenous analgesia pump over 48h, 0.5 mg upper limit respectively) or Control group (received 0.9% saline in replace of penehyclidine at the same time points). The primary outcome measure was the incidence of postoperative nausea and vomiting in the postanesthesia care unit and ward area. Quality of Recovery-15 (QoR-15) scores and general comfort questionnaire (GCQ) scores were assessed on postoperative day (POD) 1, 2.
Results: Patients between two groups had comparable baseline characteristics. Compared with the Control group, the incidence and severity of PONV, postoperative nausea (PON), and postoperative vomiting (POV) were significantly lower in the PHC group at 2h (PONV: P = 0.002, P = 0.004, respectively; PON: P = 0.018, P = 0.038, respectively; POV: P = 0.011, P = 0.072, respectively), 24h (PONV: P = 0.003, P = 0.001, respectively; PON: P = 0.010, P = 0.032, respectively; POV: P = 0.006, P = 0.044, respectively), and 48h (PONV: P = 0.003, P = 0.002, respectively; PON: P = 0.007, P = 0.019, respectively; POV: P = 0.002, P = 0.013, respectively) after surgery. The QoR-15 and GCQ scores of the PHC group were significantly higher than those of the Control group at POD 1, 2 (P < 0.001; P < 0.001, respectively).
Conclusion: Our findings suggest that perioperative intravenous application of penehyclidine can effectively prevent postoperative nausea and vomiting in gynecological laparoscopic surgery patients and improve postoperative recovery.
Keywords: penehyclidine, gynecologic laparoscopy, postoperative nausea and vomiting, quality of recovery
Introduction
Postoperative nausea and vomiting is a common complication after general anesthesia, the incidence of which is about 30% in all surgical types,1,2 and the prevention and management of PONV are not very satisfactory. Previous studies have shown that some factors may increase the risk of PONV, such as female sex, a history of motion sickness or previous PONV, use of opioids, a significantly long duration of surgery, and non-smoking status.3,4 In certain types of surgery, such as gynecological laparoscopic surgery in high-risk patients, the incidence of PONV is as high as 80%.5–7 In addition to the above factors that may increase the incidence of PONV, the establishment of artificial pneumoperitoneum, use of inhaled anesthetics and surgical operations are likely to cause a significant increase in the incidence of PONV. PONV is likely to cause wound cracking, aggravate postoperative pain, delay postoperative recovery, prolong hospital stay, and reduce patient comfort and satisfaction.
Vomiting is a complex neural reflex that activates the sensation of vomiting through receptors such as cholinergic (muscarine), dopaminergic, histamine, or 5-serotonergic receptors when the afferent pathway is stimulated.8 Despite advances in prevention and treatment, it is still impossible to effectively prevent and control the occurrence of PONV in clinic, especially most patients undergoing gynecological laparoscopic surgery need to face serious postoperative nausea and vomiting, which needs to be solved urgently.6,9
Currently, the commonly used antiemetic drugs mainly include 5-hydroxytryptamine (5-ht3) receptor antagonists, antihistamines, neurokinin 1 (NK-1) receptor antagonists, anticholinergics, dopamine receptor antagonists and glucocorticoids. In order to effectively prevent the occurrence of PONV, the combination of two or more antiemetic drugs is often used in clinical practice for high-risk patients, and the occurrence of PONV is jointly reduced by reducing the dosage of inhalation anesthetics and opioids.
In recent years, good progress has been made in the research of antiemetic drugs, and anticholinergics have been proved to reduce the incidence of PONV.10,11 Transdermal scopolamine patch is a recommended anticholinergic drug for preventing of PONV.5,12 Penehyclidine is a novel anticholinergic drug that eliminates long half-lives. It is widely used as a premedication to reduce salivary secretion as a selective blocker of acetylcholine receptors for type 1 and type 3 muscarinic acetylcholine receptor.13,14 Previous studies have shown that the mechanism of penehyclidine reducing the incidence of PONV is complex, which may be related to its blocking of the muscarinic acetylcholine receptor, which is involved in the development of PONV through various mechanisms. Recent clinical studies have shown that penehyclidine for prevention of PONV has made good progress in some surgical procedures, such as ophthalmology,15 laparoscopic bariatric surgery,16 thyroid surgery17 and stomatology surgery.18
Patients undergoing gynecological laparoscopic surgery are at high risk for PONV. Whether penehyclidine can reduce the incidence of PONV in these patients is worth studying and discussing. Therefore, the purpose of this study was to investigate the effect of penehyclidine on PONV in gynecological laparoscopic surgery and explore its effect on postoperative recovery quality.
Materials and Methods
The protocol was approved by the Ethics Committee of the First Affiliated Hospital, University of Science and Technology of China (2022KY Ethics Review No. 245), and the trial was registered in the Chinese Clinical Trial Registry (ChiCTR2200065258). The trial was conducted in accordance with the guidelines of the Declaration of Helsinki with Good Clinical Practice. This report adheres to the CONSORT guidelines. The study is a single-center, double-blind, prospective, randomized clinical trial, and all patients were recruited from November 2022 to June 2023. All patients who volunteered to participate in this study were recruited after passing the ethical review, and they were given a detailed explanation of the study protocol and informed of the possible benefits and potential risks of the trial. Written informed consents were obtained from all patients or family authorized before enrollment.
Patients
Ninety-two women scheduled for elective laparoscopic surgery under general anesthesia were included, with age over 18, American Society of Anesthesiologists (ASA) physical status II–III and receiving patient-controlled intravenous analgesia (PCIA). The exclusion criteria were as follows: pregnant or lactating women; body mass index (BMI) ≥ 35 kg/m2; preoperative usage of antiemetic or anticholinergic drugs; a history of severe nausea and vomiting or severe motion sickness before surgery; a history of glaucoma and myasthenia gravis; severe cardiovascular, respiratory, liver and kidney dysfunction, or coagulation dysfunction; language comprehension disorder or mental disorder; refusing to sign written informed consent.
Randomization and Blinding
Eligible patients were randomly assigned to the penehyclidine group (Group P) and the control group (Group C) in a 1:1 ratio by a computer-generated random sequence.
The group numbers were contained in an opaque, sealed envelope. The anesthesia nurse who is not involved in the subsequent trial process opened the envelope before induction of anesthesia and prepared the appropriate medications, and penehyclidine and saline are colorless and transparent, with no difference in appearance. All anesthesia managers, postoperative assessments and data analysis staff were blinded to the group allocation.
Anesthetic Management and Intervention
All patients fasted for 8h and forwent water for 4h before receiving general anesthesia. After patients entered the operation room, vital signs were routinely monitored, including electrocardiogram (ECG), pulse oxygen saturation (SpO2), non-invasive cuff blood pressure, end-expiratory CO2 (PETCO2) and bispectral index (BIS). Arterial blood pressure was monitored by radial artery puncture catheterization under local anesthesia (Allen test is necessary before puncture). The two groups were given the same anesthesia induction regimen except for the intervention: after adequate preoxygenation, intravenous administration followed by midazolam (0.04 mg/kg), Sufentanil (0.5 μg/kg), etomidate (0.3 mg/kg), rocuronium (0.8 mg/kg) and prophylactic dexamethasone 10 mg. Intervention: Patients in PHC group received a bolus of penehyclidine 10 μg/kg during the induction of anesthesia, then followed by a continuous infusion of 10 μg/kg penehyclidine at a fixed rate of 2.0 mL/h in postoperative intravenous analgesia pump over 48h. The upper limit of induction and infusion of penehyclidine was 0.5 mg, respectively. While in Control group, individuals received volume-matched 0.9% saline in replace of penehyclidine at the same time points as a placebo. When the BIS < 60 with muscle relaxation, a suitable tracheal catheter was performed to control breathing. Mechanical ventilation parameters were set as follows: tidal volume (VT) 6–8 mL/kg, respiratory rate (RR) 12–16 beats/min, airway pressure <30mmHg, and PETCO2 34–45 mmHg (1 mmHg = 0.133 kPa, considering the effect of pneumoperitoneum, short-term hypercapnia is acceptable). Anesthesia maintenance was as follows: sevoflurane 1%, remifentanil 0.1–0.3 μg/kg/min and propofol 2–5 mg/kg/h. During surgery, BIS values were controlled between 40 and 60 by adjusting the concentration of sevoflurane and the infusion rate of intravenous anesthesia maintenance drugs, and cis-atracurium was supplemented as needed. During the operation, the basic level of the patient’s preoperative blood pressure and heart rate, the necessary depth of anesthesia and the surgical needs of the surgeon should be comprehensively considered to maintain the blood pressure and heart rate at an appropriate level. If severe fluctuations occur during anesthesia, consider timely adjustment and treatment with vasoactive drugs to maintain the stability of vital signs.
After surgery, patients were routinely transferred to post-anesthesia care unit (PACU) for anesthesia resuscitation. After extubation, if NRS ≥ 4, fentanyl 1 µg/kg would be given (iv), and Oxycodone (a strong analgesic, 0.07mg/kg, iv) was necessary when effective analgesia is still not available.
An intravenous analgesic pump is attached for relieving pain and preventing nausea and vomiting. The regimen of penehyclidine or placebo infusion was achieved by a PCIA device. The configuration and parameter settings of PCIA were as follows: sufentanil (1.25–1.5 μg/kg), flurbiprofen axetil 100 mg, ondansetron 8 mg and penehyclidine (10 μg/kg, maximal dosage 0.5mg) or volume-matched normal saline diluted to 100 mL, 2 mL/h, bolus 2 mL, lock time 15 min. The information about the drugs involved in this study will be described in the Supplementary.
Primary and Secondary Study Outcomes
Primary outcomes were the incidence of PONV within 48 h after gynecological laparoscopic surgery. Secondary outcomes were as follows: incidence of 2 h, 24 h PONV; incidence of 2 h, 24 h, 48h PON and POV; Severity of PONV, PON and POV within 2 h, 24 h, 48 h; QoR-15 scores on preoperative (Pre) day and POD 1 and POD 2; comfort level on POD 1 and POD 2; consumption of propofol, remifentanil, sevoflurane and sufentanil; the incidence of perioperative adverse events; the numerical rating scale for pain (NRS) on POD 1 and POD 2; the time to first flatus postoperatively; the types and dosage of drugs used for rescue antiemetic therapy in the ward were also recorded.
PONV was defined as at least one episode of nausea or vomiting or a combination of both symptoms. The severity of PONV was evaluated as follows: 0: no symptoms of nausea or vomiting; 1 (mild): mild nausea or vomiting occured once; 2 (moderate): moderate to severe nausea, or vomiting more than 2 times, or nausea required only one rescue antiemetic therapy; 3 (severe): more than two episodes of vomiting, or needing more than one rescue antiemetic medication. The severity of PON was assessed with a numeric rating scale (0:no symptoms of nausea; 1:mild; 2: moderate; 3: severe). The severity of POV is assessed by the number of episodes of vomiting (0: no vomiting; 1: vomiting episodes occurring 1–2 times; 2: vomiting episodes occurring 3–5 times; 3: vomiting episodes occurring > 5 times). QoR-1519 is commonly used to evaluate the quality of recovery after general anesthesia due to its high validity, reliability, reactivity, and clinical feasibility. Ratings range from 0 (very poor) to 150 (excellent). The degree of pain was evaluated by the numeric rating scale (NRS, 0 indicates no pain, and 10 means excruciating pain). The Kolcaba Comfort Scale (GCQ) was used to evaluate the postoperative comfort. The scale consists of 28 items, including 4 dimensions: physiological, psychological spirit, social culture and environment. The Likert 4-level scoring method was adopted, with 1 to 4 points indicating “strongly disagree” to “strongly agree” respectively. Reverse questions 1–4 indicate “strongly agree” to “strongly disagree” respectively. The total score was 28 to 112 points. The higher the score, the more comfortable the patient.
Statistical Analysis
The study of yang et al showed that the incidence of PONV within 48h after gynecological laparoscopic surgery was 62.92%.20 Assuming a reduction of at least 30% in the incidence of PONV in the penehyclidine group could be considered clinically significant. The estimated sample size was 43 patients per group, with a power of 80% and an α risk of 0.05. To compensate for possible loss of follow-up or rejection, a 10% drop-out would be considered.
Finally, 94 patients were included in this study. The sample size was calculated with PASS (version15, NCSS, LLC, Kaysville, UT, USA).
For continuous data, Shapiro–Wilk was used to test the normality of data and Levene’s was used to test the homogeneity of variance. Data conforming to the normal distribution were expressed as mean ± standard deviation (Mean ± SD), using Student’s t-test. The non-normal distribution data were expressed as median (M) and inter-quartile range (IQR), and Mann–Whitney U-test was used. Enumeration data were expressed as frequency (%). Enumeration data and categorical variables were analyzed using either the chi-squared test or Fisher’s exact test, as appropriate. All P values were two-sided, and P < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics (Version 20.0, IBM SPSS, Chicago, IL, USA) and GraphPad Prism (Version 8, GraphPad Software, La Jolla, CA, USA).
Result
During the recruitment period, 110 patients were selected from the First Affiliated Hospital of University of Science and Technology of China for elective gynecological laparoscopic surgery, 8 of whom were excluded because they did not meet the inclusion criteria or refused to be included. A total of 102 patients were eventually randomized, 52 in the PHC group and 50 in the Control group. Subsequently, 95 patients were included in the intention-to-treat analysis and 7 patients were excluded: 3 for the change of surgical mode (laparoscopic surgery to open surgery), and 4 for refusing follow-up. Ultimately, 92 patients were included in the per-protocol analysis, and 3 patients were excluded for refusing PCIA (Figure 1).
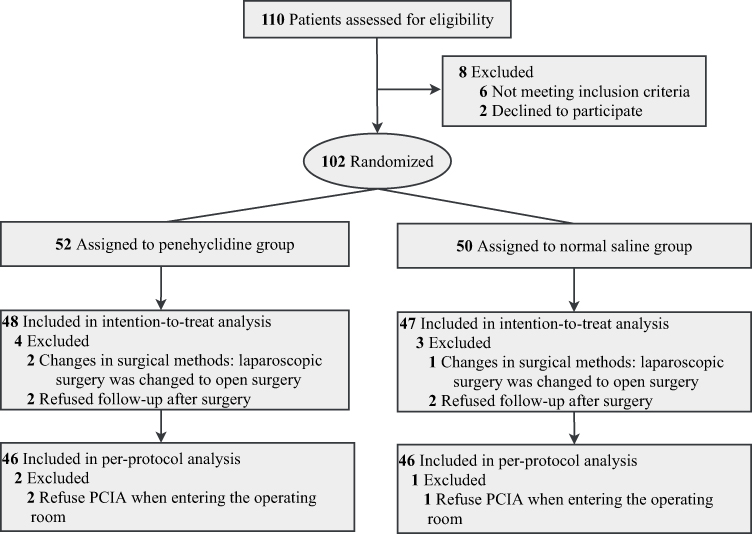 |
Figure 1 Flow Diagram of the Study. |
Demographic Characteristics and Surgical Data
There were no statistically significant differences in baseline characteristics and surgical data between the two groups (Table 1).
 |
Table 1 Patient Characteristics and Surgical Data |
Study Endpoints
The incidence of PONV, PON and POV in the PHC group within 48h after operation were 19 (41.3%), 17 (37.0%) and 7 (15.2%), respectively, which were significantly lower than those in the Control group (P = 0.003; P = 0.007; P = 0.002, respectively, Table 2, Figure 2A, C, E). The number of patients receiving rescue antiemetic therapy in the PHC group decreased significantly within 48h after operation (P = 0.001, Table 2).
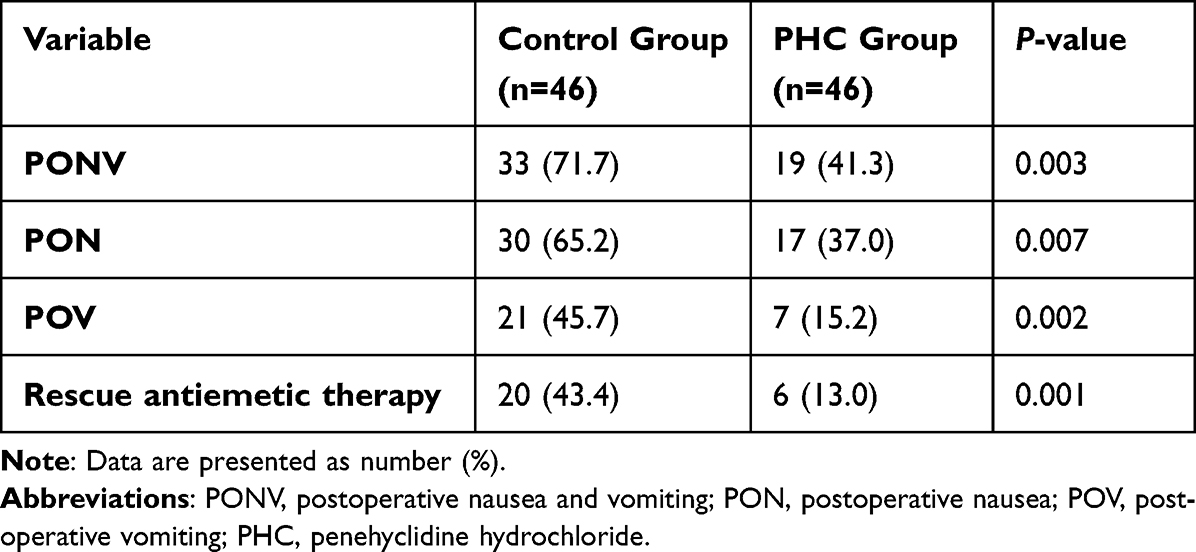 |
Table 2 Comparison of Primary and Secondary Outcomes Within 48 h Postoperatively Between the Two Groups |
 |
Figure 2 Incidence and Severity of PONV, PON and POV Between Two Groups. Abbreviations: PONV, postoperative nausea and vomiting; PON, postoperative nausea; POV, postoperative vomiting; PHC, penehyclidine hydrochloride. Notes: Data are presented as percentage (%). The percentage on the Y-axis represents the cumulative incidence of events over time periods. (A) Incidence of PONV; (B) Severity of PONV; (C) Incidence of PON; (D) Severity of PON; (E) Incidence of POV; (F) Severity of POV. PONV: “0”, no symptoms of nausea or vomiting; “1” (mild), mild nausea or vomiting occured once; “2” (moderate), moderate to severe nausea, or vomiting more than 2 times, or nausea required only one rescue antiemetic therapy; “3” (severe), more than two episodes of vomiting, or needing more than one rescue antiemetic medication. PON: “0”, no symptoms of nausea; “1”, mild; “2”, moderate; “3”, severe. POV: “0”, no vomiting; “1”, vomiting episodes occurring 1–2 times; “2”, vomiting episodes occurring 3–5 times; “3”, vomiting episodes occurring > 5 times. *Adjusted P < 0.05 different from Control group at 2 h after surgery. **Adjusted P < 0.05 different from Control group at 24 h after surgery. #Adjusted P < 0.05 different from Control group at 48 h after surgery. |
Compared with the Control group, the incidence of PONV, PON and POV in the PHC group reduced significantly within 2h (P = 0.002; P = 0.018; P = 0.011, respectively), 24h (P = 0.003; P = 0.010; P = 0.006, respectively) and 48h (P = 0.003; P = 0.007; P = 0.002, respectively) after operation (Figure 2A, C, E). Meanwhile, the severity of PONV, PON and POV in the PHC group also reduced significantly within 2h (P = 0.004; P = 0.038; P = 0.072, respectively), 24h (P = 0.001; P = 0.032; P = 0.044, respectively) and 48h (P = 0.002; P = 0.019; P = 0.013, respectively) after operation (Figure 2B, D, F).
The scores of QoR-15 1 day before surgery were comparable between two group. Compared with the Control group, the QoR-15 scores of the PHC group were significantly higher on POD 1 and 2, with statistically significant differences (P < 0.001; P < 0.001, respectively), but the difference did not reach the minimal clinically important difference (MCID) of 8.0 points.21 Similarly, compared with the Control group, the postoperative comfort level of the PHC group was significantly improved, and GCQ scores were significantly increased on POD 1 and 2, with statistically significant differences (P < 0.001; P < 0.001, respectively, Table 3).
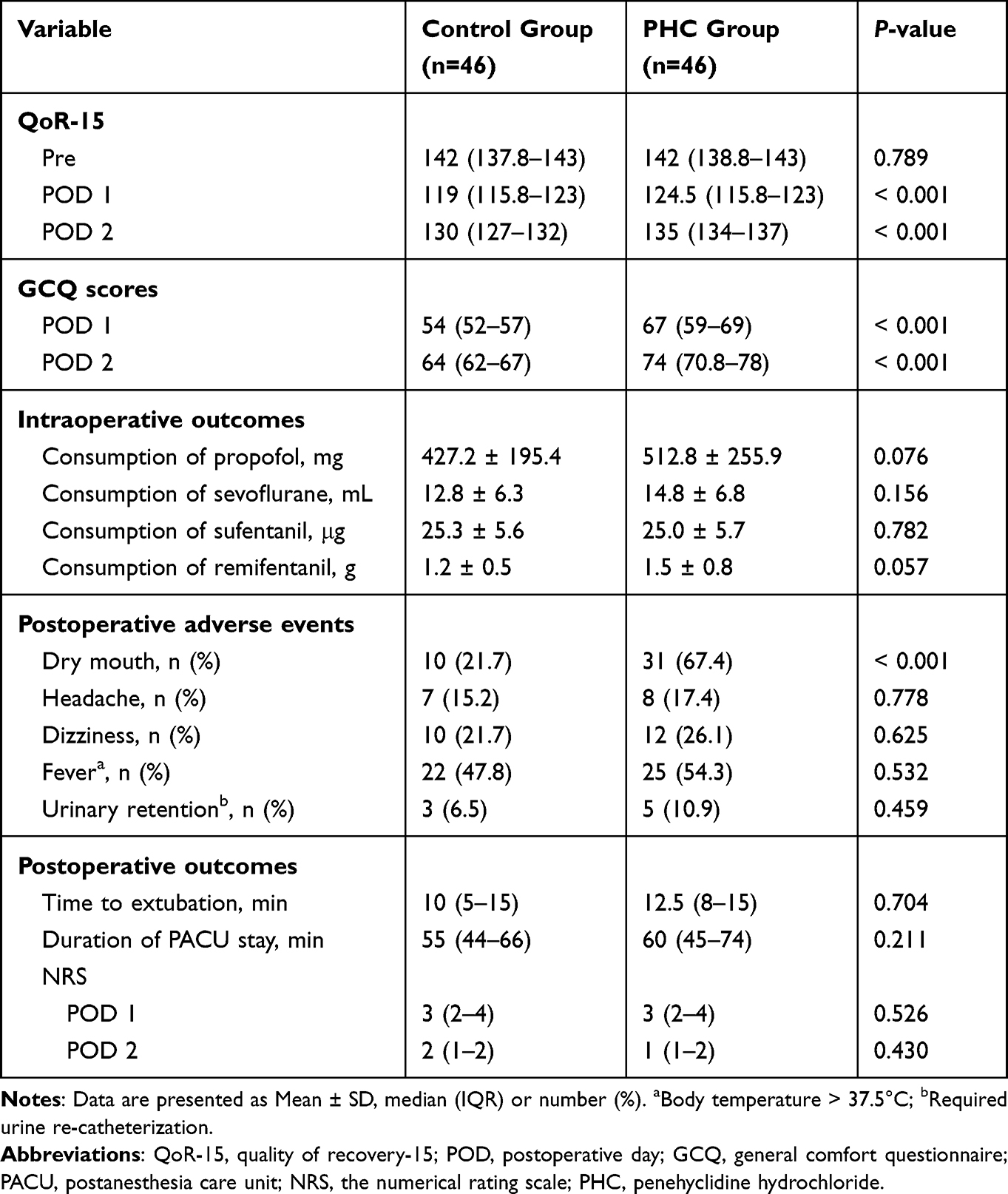 |
Table 3 Perioperative Measurements Between the Two Groups |
There was no significant difference in the consumption of propofol, sevoflurane, sufentanil and remifentanil between the two groups (P > 0.05, Table 3).
The incidence of postoperative dry mouth in PHC group was significantly higher than that in Control group, and the difference was statistically significant (P < 0.001). There was no significant difference in the incidence of postoperative adverse events such as headache, dizziness, fever and urinary retention between the two groups (P > 0.05, Table 3).
There was no significant difference in extubation time and residence time in PACU between the two groups (P > 0.05). Similarly, postoperative NRS scores were not statistically significant between the two groups (P > 0.05, Table 3).
Penehyclidine was associated with delayed recovery of gastrointestinal function after surgery. Compared with the Control group, Kaplan–Meier curve showed that penehyclidine significantly extended the time to first flatus postoperatively (median onset time, 36 VS 30 h; P = 0.033, Figure 3).
 |
Figure 3 Kaplan–Meier Curves of the Time to Not First Flatus Postoperatively Between the Two Groups. Abbreviation: PHC, penehyclidine hydrochloride. |
Discussion
The severity of postoperative nausea and vomiting is significantly associated with overall postoperative recovery quality, relevant postoperative clinical outcomes, perioperative comfort, and satisfaction experience, which has led clinicians to make extensive efforts and conducted thorough exploration to reduce the PONV. In this study, a randomized double-blind clinical trial was conducted to study the effect of intravenous injection combined with PCIA pump infusion of penehyclidine on the incidence of PONV. The findings revealed that penehyclidine reduced the incidence of PONV by 30.4% in gynecological laparoscopic surgery, leading to a significant improvement in recovery quality as well as higher levels of patient comfort and satisfaction.
The mechanism of PONV, which is one of the most common events in cases of delayed recovery and reduce comfort and satisfaction of patients after laparoscopic surgery, has not yet been completely clear. Consensus guidelines for PONV management indicate that gynecological surgery and laparoscopic surgery are associated with an increased risk of PONV.5 In order to facilitate the operation of the abdominal cavity, the surgeon needs to use carbon dioxide to create an artificial pneumoperitoneum, and also use special positions such as the Trendelenburg position. The Trendelenburg position can cause a series of physiological changes, such as increased intracranial blood flow and increased venous return resistance, which together lead to increased intracranial pressure. CO2 artificial pneumoperitoneum will cause hypercapnia, which will increase blood pressure, while the increase of intracranial blood CO2 concentration will cause intracranial vascular dilation, resulting in increased intracranial pressure. Arslan22 and Klockgether-Radke et al23 found that mechanical factors caused by gastric and intestinal pressure induced by artificial pneumoperitoneal cavity, neurological factors causing parasympathetic nerve stimulation, and chemical factors caused by hypercarbia vomiting center may be one of the reasons for inducing PONV. Guo et al24 believe that the increase in intracranial pressure caused by the Trendelenburg position and artificial pneumoperitoneum is one of the reasons for PONV during laparoscopic surgery. Current clinical studies25,26 strongly suggests that CO2 pneumoperitoneum plays an important role in the pathogenesis of PONV.
The novel long-acting anticholinergic drug, penehyclidine, exhibits high selectivity for M1 and M3 acetylcholine receptors while lacking any impact on M2 receptors.13 Recent studies have demonstrated the effect of penehyclidine in preventing PONV. In a recent prospective study of 100 patients with total thyroidectomy, Lu et al found that a single dose of intravenous penehyclidine after induction of anesthesia significantly reduced the incidence of PONV, especially 2–24 h after thyroidectomy.17 In another prospective study of 228 pediatric patients undergoing strabismus surgery, Sun et al found a significant reduction in the incidence and severity of PONV 48 h after induction of anesthesia in patients given pentaethyl ether (0.01 mg/kg, maximal dose 0.5 mg, intravenously).15 However, Ding et al found that penehyclidine (bolus 5mg, IV) did not reduce the incidence and severity of postoperative PONV in bariatric surgery patients.16 In a study of patients undergoing gynecological laparoscopic surgery, Zhang et al observed that a single dose of penehyclidine before anesthesia also did not reduce the incidence of PONV.27
Some of the above studies are based on a single dose of intravenous penehyclidine to investigate the prevention of PONV. Penehyclidine has obtained different results in the prevention of PONV, which may be related to its pharmacokinetic effects such as elimination half-life time and surgical specificity. The elimination half-life of penehyclidine is about 24 hours, causing its preventive effect on PONV to diminish or disappear after 24 hours.15,27 Yang et al observed that the incidence of PONV 48 hours after surgery in gynecologic laparoscopic patients remained high (62.92%).20 We therefore designed this trial to infuse penehyclidine via a PCIA device to 48 hours after surgery, to compensate for its relatively short elimination half-life, reduce the occurrence of PONV to improve the prognosis. We found that the incidence of PONV decreased significantly in the penehyclidine infusion group, which was basically consistent with the results of Wang et al.18 Compared with the dose given by Wang et al,18 the dose of penehyclidine in our study was larger (total 1.0 mg), but fortunately we did not find severe delirium and other psychiatric symptoms in the patients after the operation, which may be related to the relatively young median age of female patients and the small number of patients at high risk of POD28,29 included in this study.
In order to enhance the accuracy of predicting PONV occurrence, the Apfel score was used to evaluate it. The Apfel simplified risk score was derived from four predictors: female sex, history of PONV and / or motion sickness, nonsmoking status, and use of postoperative opioids.3 The subjects included in this study were women, almost all of whom had no history of smoking and had received post-operative treatment for PCIA, resulting in an Apfel score ≥ 3. When there are 3 or more risk factors are present, the probability of experiencing PONV exceeds 60%, which aligns with the findings of this study. The latest PONV guidelines recommend multimodal prophylaxis for patients with one or more risk factors.30 Previous consensus guidelines have also highlighted gynecological laparoscopic surgery as high-risk for PONV and recommended employing two or more antiemetic drugs, such as serotonin 5-HT3, dopamine D2 and histamine H1 antagonists, corticosteroids, etc.5,31–33 Therefore, in this study dexamethasone 10mg was administered prior to induction along with ondansetron added to postoperative PCIA regimen. However, it is noteworthy that despite these interventions the incidence of PONV remained considerably high within our population sample. In view of their widespread usage and safety profile, Ondansetron and dexamethasone were selected as prophylactic medications in this investigation. Ondansetron represents the most commonly employed and extensively studied 5-HT3 receptor antagonist, which is regarded as a “gold standard” treatment option for managing PONV.34 Studies35–37 have demonstrated that doses equal to or exceeding 8mg (0.01 mg/kg) of dexamethasone can effectively reduce the incidence of PONV. These two drugs have been used clinically over many years without any significant adverse reactions.
Compared with the Control group that received dexamethasone and ondansetron as prophylactic antiemetics, PONV was significantly lower in the intravenous and postoperative PCIA infusion of PHC group. Considering the unclear mechanism of penehyclidine’s effect on PONV, we speculate that the following reasons may be responsible. Firstly, penehyclidine reduces vagal reflex and inhibits its afferent activation by acting on M1-type receptors, thereby alleviating PONV. Secondly, previous studies have confirmed that penehyclidine can relieve gastrointestinal smooth muscle spasm by acting on M3 cholinergic receptors in digestive glands and smooth muscle, effectively reducing postoperative gastric pressure. Thirdly, previous studies have found that post-treatment with penehyclidine ether can improve intestinal mucosal injury caused by limb ischemia-reperfusion and reduce intestinal mucosal barrier function damage.38 We speculate that the decrease in PONV may be related to the improvement of intestinal microcirculation. Fourthly, recent animal and clinical trials have found that penehyclidine can play an anti-inflammatory role by regulating inflammatory mediators, which may ameliorate the high intracranial pressure caused by hypercapnia induced by gynecologic laparoscopic CO2 pneumoperitoneum, thereby alleviating brain edema, reducing the sensitivity of vestibular system, and reducing the incidence of PONV.
Common adverse reactions following intravenous penehyclidine include dry mouth, dizziness, blurred vision, delirium, urinary retention, hyperthermia, hallucinations, disorientation, and coma. In this study, dry mouth symptoms were observed in 31 individuals (67.4%) in the PHC group, which was significantly higher compared to the Control group (10 individuals; 21.7%). This could be attributed to its impact on M3 receptors leading to reduced glandular secretion from respiratory submucosal glands. No significant differences were found between the two groups regarding other adverse events such as headache, dizziness, fever and urinary retention (cumulative number: 42 vs 50). Additionally, we noted a delayed postoperative time for first flatus in the PHC group compared to the Control group due to its anticholinergic effect on the gastrointestinal tract, resulting in delayed recovery of intestinal function. The median time for first flatus postoperatively was prolonged by 6.5 hours, which may be certain clinically significant. Furthermore, some patients in the PHC group experienced dry skin and facial flushing but these symptoms accounted for only a small proportion and resolved shortly after discontinuation of medication. In addition, some patients in the PHC group had dry skin and facial flushing, but only accounted for a small proportion, and the symptoms disappeared soon after stopping the drug.
There are certain limitations that need to be acknowledged within the context of our research. Firstly, we were unable to monitor the plasma concentration of penehyclidine, and in order to achieve our desired effect, the doses in the regimen we chose (0.5mg IV, 0.5mg infusion via PCIA) were relatively larger than those of other investigators.18 Fortunately, no serious adverse reactions associated with penehyclidine were reported during our study period. Nevertheless, further exploration is required to determine the optimal dosage for future studies. Secondly, we specifically selected gynecologic laparoscopic surgery patients who were at a high risk for PONV and followed a multimodal prophylaxis protocol as per guideline recommendations; hence, we could not evaluate the isolated effect of penehyclidine on preventing PONV in this specific patient population undergoing gynecologic laparoscopic surgery alone. Lastly, it should be noted that the effectiveness of penehyclidine in preventing PONV may not be universally applicable across all surgical procedures due to variations in risk levels associated with different types of surgeries.
Conclusion
Multimodal prophylaxis strategies have not demonstrated efficacy in reducing the incidence of PONV in patients undergoing gynecological laparoscopic surgery. However, based on the combination of multiple drugs, a combination approach involving the administration of a 10 μg/kg bolus dose during anesthesia induction followed by an infusion of 10 μg/kg penehyclidine with PCIA device after the operation has shown significant potential in reducing the incidence of PONV, improving postoperative recovery quality, and enhancing patient comfort levels in gynecological laparoscopic surgery. Anesthesiologists may consider implementing an intravenous bolus plus postoperative infusion regimen of penehyclidine for patients at high risk of experiencing PONV.
Data Sharing Statement
The individual participants’ data underlying the results reported in this article may be accessed with approval from the corresponding author 6 months after publication of this study. The study protocol, statistical analysis plan, and clinical study report will also be made available.
Acknowledgments
All authors appreciate the support from the gynecological medical staff of the First Affiliated Hospital of USTC (Anhui Provincial Hospital).
Disclosure
All authors have no conflicts of interest in this work.
References
1. Apfel CC, Korttila K, Abdalla M, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350(24):2441–2451. doi:10.1056/NEJMoa032196
2. Habib AS, Gan TJ. Evidence-based management of postoperative nausea and vomiting: a review. Can J Anaesth. 2004;51:326–341. doi:10.1007/BF03018236
3. Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
4. Sinclair DR, Chung F, Mezei G. Can postoperative nausea and vomiting be predicted? Anesthesiology. 1999;91:109–118. doi:10.1097/00000542-199907000-00018
5. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2020;131:411–448. doi:10.1213/ANE.0000000000004833
6. Tao B, Liu K, Wang D, et al. Effect of intravenous oxycodone versus sufentanil on the incidence of postoperative nausea and vomiting in patients undergoing gynecological laparoscopic surgery. J Clin Pharmacol. 2019;59:1144–1150. doi:10.1002/jcph.1408
7. Zheng XZ, Cheng B, Luo J, et al. The characteristics and risk factors of the postoperative nausea and vomiting in female patients undergoing laparoscopic sleeve gastrectomy and laparoscopic gynecological surgeries: a propensity score matching analysis. Eur Rev Med Pharmacol Sci. 2021;25:182–189. doi:10.26355/eurrev_202101_24383
8. Horn CC, Wallisch WJ, Homanics GE, et al. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi:10.1016/j.ejphar.2013.10.037
9. Ames WA, Machovec K. An update on the management of PONV in a pediatric patient. Best Pract Res Clin Anaesthesiol. 2020;34:749–758. doi:10.1016/j.bpa.2020.05.007
10. Pergolizzi JV, Philip BK, Leslie JB, Taylor R, Raffa RB. Perspectives on transdermal scopolamine for the treatment of postoperative nausea and vomiting. J Clin Anesth. 2012;24(4):334–345. doi:10.1016/j.jclinane.2011.07.019
11. Zhong W, Shahbaz O, Teskey G, et al. Mechanisms of nausea and vomiting: current knowledge and recent advances in intracellular emetic signaling systems. Int J Mole Sci. 2021;22(11). doi:10.3390/ijms22115797
12. Antor MA, Uribe AA, Erminy-Falcon N, et al. The effect of transdermal scopolamine for the prevention of postoperative nausea and vomiting. Front Pharmacol. 2014;5:55. doi:10.3389/fphar.2014.00055
13. Wang Y, Gao Y, Ma J, et al. Pleiotropic effects and pharmacological properties of penehyclidine hydrochloride. Drug Design Dev. 2018;12:3289–3299. doi:10.2147/DDDT.S177435
14. Xiao H, Liao Z, Tong R, et al. Penehyclidine hydrochloride: a potential drug for treating COPD by attenuating toll-like receptors. Drug Design Dev. 2012;6:317–322. doi:10.2147/DDDT.S36555
15. Sun J, Cao X, Lu T, Li N, Min X, Ding Z. Penehyclidine mitigates postoperative nausea and vomiting and intraoperative oculocardiac reflex in patients undergoing strabismus surgery: a prospective, randomized, double-blind comparison. BMC Anesthesiol. 2021;21(1):49. doi:10.1186/s12871-021-01266-0
16. Ding X, Chen D, Che J, Xu S, Liang H, Gui B. Penehyclidine hydrochloride for treating postoperative nausea and vomiting after laparoscopic bariatric surgery: a double-blinded randomized controlled trial. BMC Anesthesiol. 2023;23(1):135. doi:10.1186/s12871-023-02078-0
17. Lu T, Li R, Sun J, Chen J. Evaluation of penehyclidine for prevention of postoperative nausea and vomiting in patients undergoing total thyroidectomy under total intravenous anaesthesia with propofol-remifentanil. BMC Anesthesiol. 2022;22(1):317. doi:10.1186/s12871-022-01857-5
18. Wang LK, Cheng T, Yang XD, Xiong GL, Li N, Wang DX. Penehyclidine for prevention of postoperative nausea and vomiting following bimaxillary orthognathic surgery: a randomized, double-blind, controlled trial. J Anesth. 2022;36(1):122–136. doi:10.1007/s00540-021-03017-4
19. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
20. Yang H, Gu X, Xu M, et al. Preventing nausea and vomiting after gynecological laparoscopic surgery by patient-controlled intravenous analgesia with a naloxone admixture: a randomized controlled trial. Medicine. 2022;101(29):e29584. doi:10.1097/MD.0000000000029584
21. Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, Dennis A. Minimal clinically important difference for Three Quality of Recovery Scales. Anesthesiology. 2016;125(1):39–45. doi:10.1097/ALN.0000000000001158
22. Arslan M, Ciçek R, Kalender HÜ, Yilmaz H. Preventing postoperative nausea and vomiting after laparoscopic cholecystectomy: a prospective, randomized, double-blind study. Curr Ther Res Clin Exp. 2011;72(1):1–12. doi:10.1016/j.curtheres.2011.02.002
23. Klockgether-Radke A, Piorek V, Crozier T, Kettler D. Nausea and vomiting after laparoscopic surgery: a comparison of propofol and thiopentone/halothane anaesthesia. Eur J Anaesthesiol. 1996;13(1):3–9. doi:10.1097/00003643-199601000-00002
24. Guo W, Ding J, Jin X, Li G. Effect of cerebral oxygen saturation on postoperative nausea and vomiting in female laparoscopic surgery patients. Medicine. 2017;96(41):e8275. doi:10.1097/MD.0000000000008275
25. Besir A, Tugcugil E. Comparison of different end-tidal carbon dioxide levels in preventing postoperative nausea and vomiting in gynaecological patients undergoing laparoscopic surgery. J Obstet Gynaecol. 2021;41(5):755–762. doi:10.1080/01443615.2020.1789961
26. Gin E, Lowen D, Tacey M, Hodgson R. Reduced laparoscopic intra-abdominal pressure during laparoscopic cholecystectomy and its effect on post-operative pain: a double-blinded randomised control trial. J Gastrointest Surg. 2021;25(11):2806–2813. doi:10.1007/s11605-021-04919-0
27. Zhang Z, Zhuang Y, Ouyang F, Zhang A, Zeng B, Gu M. Penehyclidine enhances the efficacy of tropisetron in prevention of PONV following gynecological laparoscopic surgery. J Anesth. 2012;26(6):864–869. doi:10.1007/s00540-012-1443-1
28. Rong X, Ding ZC, Yu HD, Yao SY, Zhou ZK. Risk factors of postoperative delirium in the knee and Hip replacement patients: a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):76. doi:10.1186/s13018-020-02127-1
29. Uzoigwe CE, O’Leary L, Nduka J, et al. Factors associated with delirium and cognitive decline following Hip fracture surgery. Bone Joint J. 2020;102-B(12):1675–1681. doi:10.1302/0301-620X.102B12.BJJ-2019-1537.R3
30. Uribe AA, Bergese SD. What is the ideal combination antiemetic regimen? Best Pract Res Clin Anaesthesiol. 2020;34(4):701–712. doi:10.1016/j.bpa.2020.10.009
31. Kovac AL. Prevention and treatment of postoperative nausea and vomiting. Drugs. 2000;59(2):213–243. doi:10.2165/00003495-200059020-00005
32. Carlisle JB, Stevenson CA. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2006;2006(3):CD004125. doi:10.1002/14651858.CD004125.pub2
33. Gan TJ. Mechanisms underlying postoperative nausea and vomiting and neurotransmitter receptor antagonist-based pharmacotherapy. CNS Drugs. 2007;21(10):813–833. doi:10.2165/00023210-200721100-00003
34. Tricco AC, Soobiah C, Blondal E, et al. Comparative efficacy of serotonin (5-HT3) receptor antagonists in patients undergoing surgery: a systematic review and network meta-analysis. BMC Med. 2015;13:136. doi:10.1186/s12916-015-0371-y
35. Yamanaga S, Posselt AM, Freise CE, Kobayashi T, Tavakol M, Kang SM. A single perioperative injection of dexamethasone decreases nausea, vomiting, and pain after laparoscopic donor nephrectomy. J Transplant. 2017;2017:3518103. doi:10.1155/2017/3518103
36. Yue C, Wei R, Liu Y. Perioperative systemic steroid for rapid recovery in total knee and Hip arthroplasty: a systematic review and meta-analysis of randomized trials. J Orthop Surg Res. 2017;12(1):100. doi:10.1186/s13018-017-0601-4
37. Mihara T, Ishii T, Ka K, Goto T. Effects of steroids on quality of recovery and adverse events after general anesthesia: meta-analysis and trial sequential analysis of randomized clinical trials. PLoS One. 2016;11(9):e0162961. doi:10.1371/journal.pone.0162961
38. Zhang Y, Leng YF, Xue X, Zhang Y, Wang T, Kang YQ. Effects of penehyclidine hydrochloride in small intestinal damage caused by limb ischemia-reperfusion. World J Gastroenterol. 2011;17(2):254–259. doi:10.3748/wjg.v17.i2.254
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.