")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Parents’ Readiness to Vaccinate Their Children Aged 5 to 17 Years Against Covid-19 and Its Associated Factors in Lira District, Uganda
Authors Puleh SS , Kigongo E , Opio IO, Akech SI, Opollo MS, Achan E, Acen J, Anyolitho MK , Acup W , Kabunga A
Received 12 January 2023
Accepted for publication 17 April 2023
Published 20 April 2023 Volume 2023:14 Pages 131—139
DOI https://doi.org/10.2147/PHMT.S404620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Roosy Aulakh
Sean Steven Puleh,1 Eustes Kigongo,2 Innocent Ojok Opio,1 Stella Immaculate Akech,1 Marc Sam Opollo,3 Everlyne Achan,3 Joy Acen,4 Maxson Kenneth Anyolitho,3 Walter Acup,5 Amir Kabunga6
1Department of Epidemiology and Biostatistics, Lira University, Lira City, Uganda; 2Department of Environmental Health and Disease Control, Lira University, Lira City, Uganda; 3Department of Community Health, Lira University, Lira City, Uganda; 4Department of Midwifery, Lira University, Lira City, Uganda; 5Department of Public Health, Gulu University, Gulu City, Uganda; 6Department of Psychiatry, Lira University, Lira City, Uganda
Correspondence: Eustes Kigongo, Department of Environmental Health and Disease Control, Lira University, P.O Box 1035, Lira City, Uganda, Tel +256770681031, Email [email protected]
Background: Data on parents’ readiness to vaccinate their children aged 5 to 17 years against COVID-19 is still scarce. This study assessed parents’ readiness to vaccinate their children aged 5 to 17 years against COVID-19 and factors associated in Lira district, Uganda.
Methods and Materials: A cross-sectional survey employing quantitative methods was conducted between October and November 2022 among 578 parents of children aged 5– 17 years in 3 sub-counties in Lira district. An interviewer-administered questionnaire was used to collect data. Data was analyzed using descriptive statistics including means, percentages, frequencies, and odds ratios. Logistic regression was used to determine associations between the factors and the readiness of parents at a 95% level of significance.
Results: Out of 634 participants, 578 responded to the questionnaire, giving a response rate of 91.2%. The majority of the parents (327, 56.8%) were female, had children aged between 12 and 15 years (266, 46.4%), and had completed primary education (351, 60.9%). Most of the parents were Christian (565, 98.4%), married (499, 86.6%), and had been vaccinated against COVID-19 (535, 92.6%). Results also indicated that 75.6% (ranging from 71.9% to 78.9%) of the parents were unwilling to vaccinate their children for the COVID-19 virus. The predictors of readiness were the age of the child (AOR: 2.02; 95% CI: 0.97– 4.20; p=0.05) and lack of trust in the vaccine (AOR: 3.33; 95% CI: 1.95– 5.71; p0.001).
Conclusion: Our study shows that parents’ readiness to vaccinate their children aged 5 to 17 years was only 24.6%, which is suboptimal. The predictors of hesitancy were the age of the child and a lack of trust in the vaccine. Based on our results, the Ugandan authorities should provide health education interventions targeting parents to combat mistrust with respect to COVID-19 and the COVID-19 vaccine and highlight the benefits of the vaccines.
Keywords: children, minors, hesitancy, readiness, vaccination
Background
After the outbreak of COVID-19, there were organized global campaigns for the prevention, early diagnosis, and treatment of the disease.1 It was evident that the best method to restrict the spread of COVID-19 and the risk of additional variations emerging was universal vaccination.2 Consequently, multiple vaccines have been developed and tested.3 The immunization of large sections of the pediatric and adult population in both high- and low-income countries where COVID-19 variants have been discovered is critical to the effectiveness of vaccination campaigns.1 As of April 8, 2022, the WHO has evaluated and recommended some of the vaccines against COVID-19 for use because they met the necessary criteria for safety and efficacy.4 While the majority of adults have been vaccinated in different countries, children are yet to be vaccinated,5 which requires a high level of acceptance and uptake. The Ugandan Ministry of Health will embark on the vaccination of children starting May 9, 2022.
Vaccination readiness had received significant attention.5 The 7C model of vaccine readiness6 is grounded in establishing the theoretical framework of facilitating and hindering psychological and structural factors of vaccination.5 The 7C model underlying vaccination readiness has seven components: confidence (trust in the safety of the vaccine), complacency (the need for vaccination due to perceived risk), constraints (no hurdles that hamstring vaccination), calculations (cost-benefit analysis of vaccination), collective responsibility (protecting others), compliance (sanctioning of people refusing vaccination), and conspiracy (low belief in fake news).5 These components explain a substantial variance in people’s intentions to vaccinate against COVID-19.5 Studies have shown that constraints and confidence predicted the parents’ intention to have their children vaccinated against influenza.7 However, studies show that many people are skeptical about the COVID-19 child vaccination.8 To achieve total and herd immunity against COVID-19, children must be covered in the immunization campaign.9 From an epidemiological perspective, if children are left unvaccinated when adults achieve immune protection, it is difficult to exclude the possibility that unvaccinated children become the virus shelter, as most COVID-19 cases in children are mild and asymptomatic.9
Parents’ vaccine hesitance may be a significant obstacle to immunization.10 Studies on parents’ readiness to vaccinate their children against COVID-19 have been conducted, revealing inconsistent results.11,12 In Japan, close to 60% of parents remained hesitant to vaccinate their children against COVID-19,10 in Turkey, 56.8% of parents were willing to vaccinate their children,13 in Saudi Arabia, 52% were hesitant to vaccinate their children,14 in the UK, approximately 48% of the participants were willing to vaccinate their children.15 In Italy, 10% of the participants were hesitant about immunization.16 This inconsistency may be attributed to sample size, settings, and time. Nevertheless, we are yet to have such studies in Uganda thus, this study.
Close to 30% of the world’s population is younger than 18 years17 and thus, in most cases, parents are involved in the decision to vaccinate their children.5 While studies on COVID-19 are ongoing, vaccine hesitancy might constitute a key obstacle to vaccination.18 The COVID-19 vaccination program, based on risk, was also launched on March 10, 2021 starting with health workers.19 However, as of November 2022, only 41.2% of Uganda’s population had received at least one dose of COVID-19 vaccines, while 27.4% were fully vaccinated.20 The parents and guardians are decision-makers on their children’s vaccination, and their vaccine hesitancy may increase the risks of COVID-19.1 Parents’ awareness and readiness regarding immunization are key factors that could contribute to their immunization decisions, as this improves vaccination status and could affect the success of vaccination programs.5 Uganda’s Ministry of Health wants to start immunizing of children against COVID-19.21,22 The Pfizer vaccine approved for use in children will be deployed to vaccinate them to reduce the risk of spreading COVID-19.21 Vaccination status, or intention to vaccinate oneself, correlates strongly with intending to vaccinate one’s children.23 However, little is known about parents’ readiness to have their children vaccinated. Thus, this study aimed to estimate parents’ readiness to vaccinate their children against COVID-19 and identify the predictors of vaccination hesitancy.
Methods and Materials
Study Setting
This study was conducted in three sub-counties (Itek, Lira, and Ogur) in Lira district, Northern Uganda. Lira district is located in Lango sub-region and is bordered by the districts of Pader in the north, Otuke in the north-east, Alebtong in the east, Dokolo in the south-east, Apac in the south-west, and Kole in the west. The district is located approximately 337 kilometers by road, north of Kampala, Uganda’s capital city.
Study Design
This was a cross-sectional survey employing only quantitative methods that was conducted from October 25 to November 20, 2022.
Study Participants and Sample Size Estimation
The study participants included parents or guardians of children aged 5–17 years. The sample size was determined using Kish Leslie’s formula (1965)24 based on a single population proportion estimation formula with assumptions of a 50% proportion, 1.96 Z (standard distribution), 95% CI, α=0.05, and a 10% non-response rate. A design effect of 1.5 was considered and the total sample was 634.
Sampling Criteria
We used multi-stage cluster sampling to identify the participants. In Lira district, there are 10 sub-counties. A simple random sampling was used to select three sub-counties. Lists of households were obtained from local council chairpersons (LC1). To select the households, a systematic random sampling was used. An interviewer-administered questionnaire was used to collect quantitative data. The study included all parents or guardians with children aged 5 to 17 within the selected cells who provided informed consent.
Data Collection Instruments
A standard questionnaire (Supplementary Material) was used to the collect data. We assessed parents’ readiness to vaccinate their children using the short version of the 7C vaccination readiness scales contextualized for COVID-19. It was developed by Geiger et al25 and has seven items on a 7-point Likert scale from 5=strongly agree to 1=strongly disagree. The seven components are confidence, complacence, constraints, calculation, collective responsibility, compliance and conspiracy. The primary outcome, which was COVID-19 vaccination readiness, is a dichotomous variable (definitely willing to vaccinate and not sure or unwilling to vaccinate). The independent variables for the study are the social-demographic factors (age, religion, education level, sex, occupation) and the clinical factors, like vaccination status and previous COVID-19 diagnosis, among others. The tool was pre-tested, and the Cronbach’s alpha was 0.79.
Procedures
Three research assistants were trained in preparation for data collection. Researcher-administered questionnaires were used to collect data from the respondents. The Local Council One Chairpersons (LC1s) helped to identify the prospective participants, who were then asked to be part of the study. Those who consented were recruited into the study. The purpose of the study, the methods of data collection, and the time frame for the study were explained to the participants before data collection. Informed consent forms were hand-delivered by the research assistants to the prospective respondents.
Statistical Analysis
Data were analyzed using STATA 17 software. We used a descriptive analysis to determine the proportions of various variables in the respondents’ characteristics, such as age, gender, and marital status. Logistic regression was used at the bivariate level to determine the relationship between dependent and independent variables. Additionally, odds ratio analyses were used to calculate the unadjusted associations between parents’ readiness and independent variables such as socio-demographic characteristics (such as age, marital status, level of education, and sex of participants). The odds ratio was calculated with a 95% level of confidence and a P-value of 0.05. Finally, for the multivariable analysis, variables that were significant in the bivariate analysis (p =0.2) were considered. Logistic regression was used to develop a suitable model to explain the determinants of parents’ readiness to vaccinate their children, with a statistical significance of p= 0.05.
Ethical Approval and Consent to Participation
This study was conducted in line with the Declaration of Helsinki. Ethical clearance was obtained from the Research Ethics Committee of Gulu University (GUREC-2022-282). Administrative permission was obtained from the Resident City Commissioner of Lira City and the Resident District Commissioner of Lira District, as well as the community’s Local Council One Chairperson. Written informed consent was obtained from all participants.
Results
Socio-Demographic Characteristics of Respondents
Out of 634 participants, 578 responded to the questionnaire, giving a response rate of 91.2%, as shown in Table 1. Table 2 shows that the majority of the parents (329, 56.9%) were female, had children aged between 12 and 15 years (267, 46.2%), and had completed primary education (353, 60.1%). Most of the parents were Christian (568, 98.3%), married (501, 86.7%), and had been vaccinated against COVID-19 (535, 92.6%).
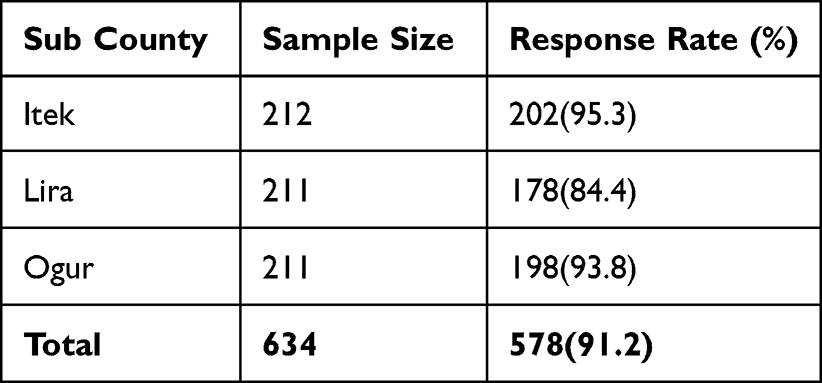 |
Table 1 Response Rate |
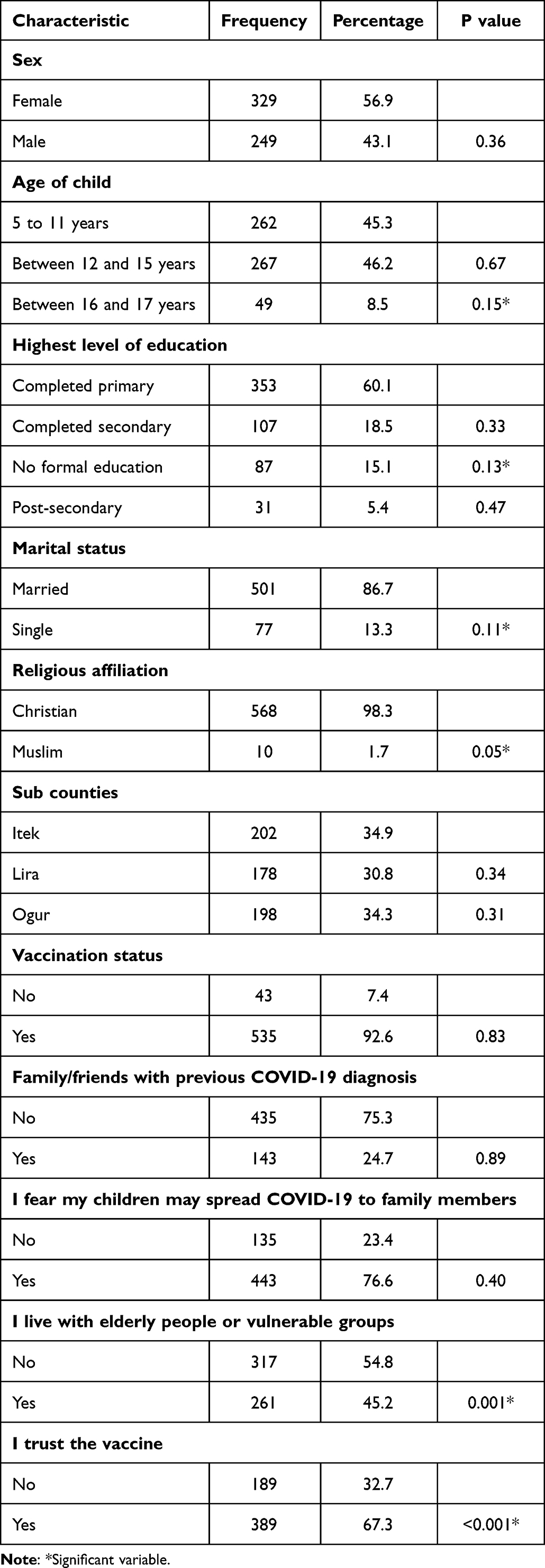 |
Table 2 Sociodemographic Characteristics and Other Factors |
Factors Influencing Parents’ Readiness to Vaccinate Their Children Against COVID-19
Our results show that the majority (75.6%) of the parents were unwilling to vaccinate their children for COVID-19. The age of the child (AOR: 2.02; 95% CI: 0.97–4.20; p=0.05) and trust in the vaccine (AOR: 3.33; 95% CI: 1.95–5.71; p0.001) were statistically significant predictors of parents’ readiness to vaccinate their children. Parents who had older children (16 to 17 years) were twice as likely to get their children vaccinated against COVID-19 compared to those who had younger children (below 12 years). Also, parents who had trust in the COVID-19 vaccine for children were 3.33 times more likely to allow their children to get vaccinated compared to those who did not have trust in the vaccine (Table 3).
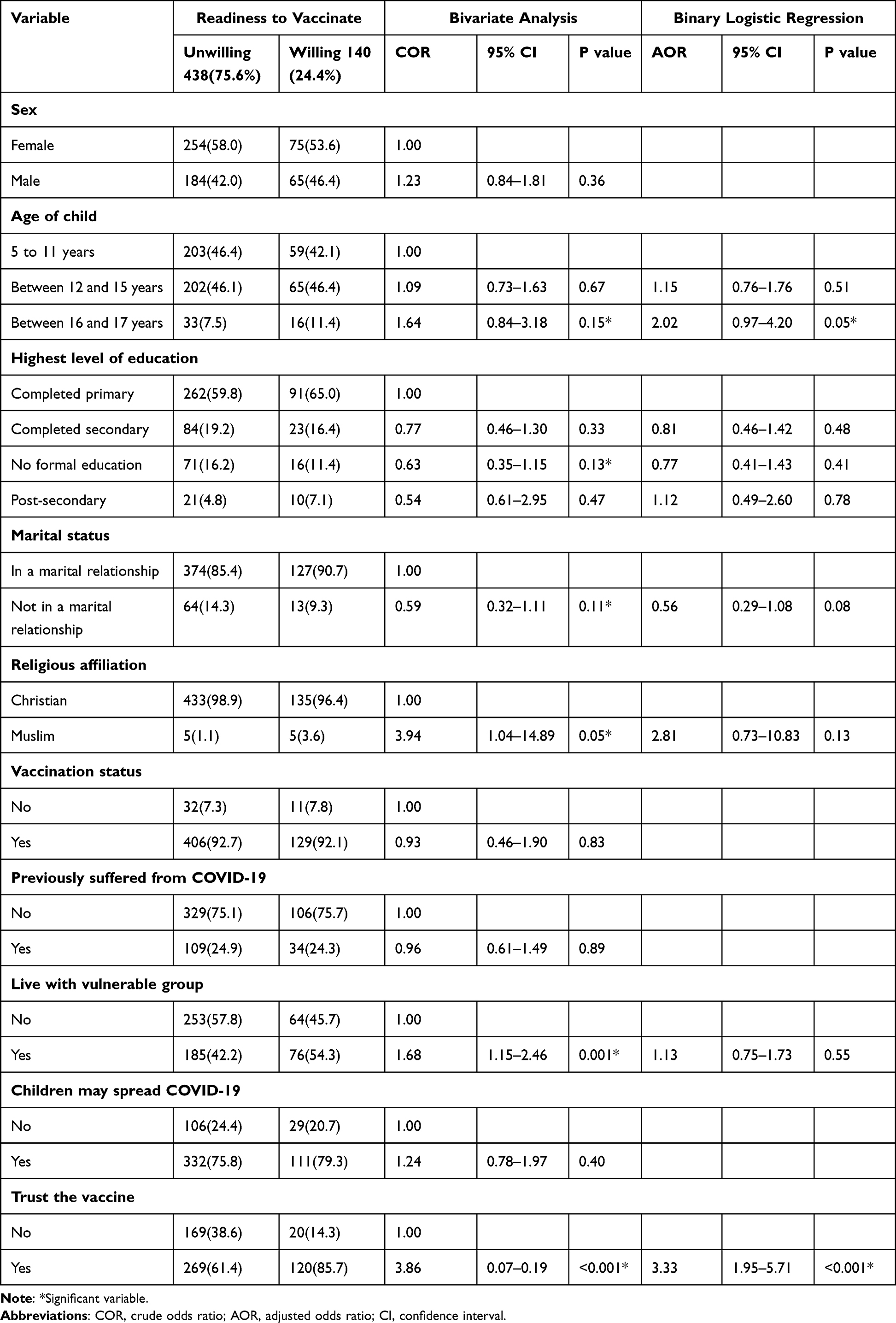 |
Table 3 Parents’ Readiness to Vaccinate Their Children for COVID-19 and Associated Factors |
Discussion
Our results indicate that 75.6% (71.9% to 78.9%) of the parents were not ready to vaccinate their children for COVID-19. The predictors of this hesitancy were the age of the child (AOR: 2.02; 95% CI: 0.97–4.20; p=0.05) and lack of trust in the vaccine (AOR: 3.33; 95% CI: 1.95–5.71; p<0.001). The apathy towards vaccination of children may be attributed to the antivaccination messaging, COVID-19 disinformation on social media,26 and lack of trust in vaccines observed in this study. This view is supported by various studies, which reported that vaccine safety is essential to upholding the public’s trust in vaccines.27 The 24.6% of parents willing to vaccinate their children is less than the 70% global target vaccination rate recommended by WHO,28 indicating that vaccination hesitancy, including parental refusal to vaccinate their children, remains a public health concern. Our results are not surprising, as WHO identified vaccine hesitancy as a major threat given its association with outbreaks and deaths from vaccine-preventable diseases.28 In line with our findings, other studies have revealed similar results.29 However, our results are higher than the 37.0% in Canada,30 63.7% in Turkey,31 and 57.1% in Japan.10 This difference may be attributed to the time lag between data collection. We collected data in 2022, when the COVID-19 threat seemed lower, while most studies were done in 2021, when there were infections and deaths resulting from COVID-19. However, these findings echo the growing concern about the support for COVID-19 vaccination.
Our results show that the parents whose children were older (aged 16 and 17 years) were more likely to have their children vaccinated against COVID-19 as opposed to their counterparts whose children were aged below 12 years (AOR: 2.02; 95% CI: 0.97–4.20; p = 0.05). The hesitancy to vaccinate younger children may be attributed to the perceived side effects of the vaccine among younger children compared to older children. Similar to our results, a study conducted in Saudi Arabia revealed that parents who had children aged 5 to 11 years were almost 10 times less likely to immunize their children against COVID-19.11 Similarly, in a national survey, almost 62% of parents were hesitant to vaccinate their children aged 5 to 11 years.29
Results in our study show that parents who had trust in the vaccine were three times more likely to have their children vaccinated against COVID-19 (AOR: 3.33; 95% CI: 1.95–5.71; p <0.001). This may not be surprising because other studies have reported similar views.27 Studies show that parents are most concerned about the serious side effects that are associated with the COVID-19 vaccine.12 Possible causes of the vaccine’s hesitancy may have been the vaccine’s newness and a lack of strong evidence of its safety. In Uganda, requiring written consent may cause anxiety among those planning to get vaccinated. Our results are in line with evidence from elsewhere that reported hesitancy is mainly due to the novelty of the vaccine.32
Strengths and Limitations
Our study had a large sample size, which gives us enough power to draw a strong conclusion regarding vaccine hesitancy. Secondly, understanding parents’ readiness to vaccinate their children aged 5 to 17 years in a rural setting is critical in designing interventions to increase vaccine uptake among this age category. However, our study had several limitations; we were unable to assess the parents’ wealth index and how it may influence hesitancy. Secondly, because of the study design, we were unable to assess the causal relationship between readiness and its determinants. Additionally, we did not assess the vaccination status of the children. This would have helped in providing information on the actual uptake of COVID-19 vaccination to policymakers. We did not consider parents’ attitudes towards the vaccine itself and the vaccination of their children, yet this could have influenced their readiness.
Conclusion
Our study shows that parents’ readiness to vaccinate their children aged 5 to 17 years was only 24.6%, which is suboptimal. The predictors of hesitancy were the age of the child and a lack of trust in the vaccine. Based on our results, the Ugandan authorities should provide health education interventions targeting parents to combat mistrust with respect to COVID-19 and the COVID-19 vaccine and highlight the benefits of the vaccines.
Data Sharing Statement
The raw data for this article is available from the principal investigator upon reasonable request.
Acknowledgments
We wish to acknowledge the study participants, the District Health Officer, and the research assistants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any funding.
Disclosure
The authors declare no conflict of interest.
References
1. Chen F, He Y, Shi Y. Parents’ and guardians’ willingness to vaccinate their children against COVID-19: a systematic review and meta-analysis. Vaccines. 2022;10(179):179. doi:10.3390/vaccines10020179
2. Zhou Y, Zhang J, Wu W, Liang M, Wu Q-S. Willingness to receive future COVID-19 vaccines following the COVID-19 epidemic in Shanghai, China. BMC Public Health. 2021;21:1–9. doi:10.1186/s12889-021-11174-0
3. Kashte S, Gulbake A, Iii SF, Gupta A. COVID-19 vaccines: rapid development, implications, challenges and future prospects. Hum Cell. 2021;34:711. doi:10.1007/s13577-021-00512-4
4. Fleming-Dutra KE, Wallace M, Moulia DL, et al. Interim recommendations of the advisory committee on immunization practices for use of moderna and Pfizer-BioNTech COVID-19 vaccines in children aged 6 months–5 years—United States; 2022.
5. Rees F, Geiger M, Lilleholt L, et al. Measuring parents’ readiness to vaccinate themselves and their children against COVID-19. Vaccine. 2022;40(28):3825–3834. doi:10.1016/j.vaccine.2022.04.091
6. Betsch C, Schmid P, Heinemeier D, et al. Beyond confidence: development of a measure assessing the 5C psychological antecedents of vaccination. PLoS One. 2018;13(12):e0208601. doi:10.1371/journal.pone.0208601
7. Zhao M, Liu H, Qu S, He L, Campy KS. Factors associated with parental acceptance of influenza vaccination for their children: the evidence from four cities of China. Hum Vaccines Immunother. 2021;17:457–464. doi:10.1080/21645515.2020.1771988
8. Verger P, Peretti-Watel P, Gagneux-Brunon A, et al. Acceptance of childhood and adolescent vaccination against COVID-19 in France: a national cross-sectional study in May 2021. Hum Vaccines Immunother. 2021;17:5082–5088.
9. Zou X, Cao B. COVID-19 vaccines for children younger than 12 years: are we ready? Lancet Infect Dis. 2021;21:1614–1615. doi:10.1016/S1473-3099(21)00384-4
10. Yoda T, Katsuyama H. Parents’ hesitation about getting their children vaccinated against COVID-19 in Japan. Hum Vaccines Immunother. 2021;17(12):4993–4998. doi:10.1080/21645515.2021.1981087
11. Aedh AI. Parents’Attitudes, their acceptance of the COVID-19 vaccines for children and the contributing factors in najran, Saudi Arabia: a cross-sectional survey. Vaccines. 2022;10:1264. doi:10.3390/vaccines10081264
12. Choi UI, Pang Y, Zheng Y, et al. Parents’ intention for their children to receive COVID-19 vaccine: implications for vaccination program in Macao. Front Pediatr. 2022;10. doi:10.3389/fped.2022.978661
13. Yigit M, Ozkaya-Parlakay A, Senel E. Evaluation of COVID-19 vaccine refusal in parents. Pediatr Infect Dis J. 2021;40:e134–e136. doi:10.1097/INF.0000000000003042
14. Aldakhil H, Albedah N, Alturaiki N, Alajlan R, Abusalih H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J Infect Public Health. 2021;14:1497–1504. doi:10.1016/j.jiph.2021.08.028
15. Bell S, Clarke R, Mounier-Jack S, Walker JL, Paterson P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: a multi-methods study in England. Vaccine. 2020;38:7789–7798. doi:10.1016/j.vaccine.2020.10.027
16. Montalti M, Rallo F, Guaraldi F, et al. Would parents get their children vaccinated against SARS-CoV-2? Rate and predictors of vaccine hesitancy according to a survey over 5000 families from Bologna, Italy. Vaccines. 2021;9:366. doi:10.3390/vaccines9040366
17. Thunström L, Ashworth M, Finnoff D, Newbold SC. Hesitancy toward a COVID-19 vaccine. Ecohealth. 2021;18:44–60. doi:10.1007/s10393-021-01524-0
18. Kasozi KI, MacLeod E, Ssempijja F, et al. Misconceptions on COVID-19 risk among Ugandan men: results from a rapid exploratory survey, April 2020. Front Public Health. 2020;8:416. doi:10.3389/fpubh.2020.00416
19. MOH. Uganda receives 864,000 doses of COVID-19 vaccines Uganda reliefWeb; 2021. Available from: https://reliefweb.int/report/uganda/uganda-receives-864000-doses-covid-19-vaccines.
20. Mathieu E, Mathieu E, Rodés-Guirao L, et al. Coronavirus Pandemic (COVID-19). Our World Data; 2020.
21. Wekesa C. Herd Immunity for Children Requires No Covid-19 Vaccination – Experts. The independent; 2022.
22. Usman IM, Ssempijja F, Ssebuufu R, et al. Community drivers affecting adherence to WHO guidelines against COVID-19 amongst rural Ugandan market vendors. Front Public Health. 2020;8(340). doi:10.3389/fpubh.2020.00340
23. Teasdale CA, Borrell LN, Shen Y, et al. Plans to vaccinate children for COVID-19: a survey of US parents. medRxiv. 2021;39:5082–5086.
24. Wiegand H, Kish L. Survey Sampling 1965, IX+ 643 S., 31 Abb., 56 Tab., Preis 83s. In: Biometrical Journal. Vol. 10. New York, London: John Wiley & Sons, Inc; 1968:88–89.
25. Geiger M, Rees F, Lilleholt L, et al. Measuring the 7Cs of vaccination readiness. Eur J Psychol Assess. 2021;384:261–269.
26. Ngai CSB, Singh RG, Yao L. Impact of COVID-19 vaccine misinformation on social media virality: content analysis of message themes and writing strategies. J Med Internet Res. 2022;24(e37806):e37806. doi:10.2196/37806
27. Goldman RD, Krupik D, Ali S, et al. Caregiver willingness to vaccinate their children against COVID-19 after adult vaccine approval. Int J Environ Res Public Health. 2021;18(10224):10224. doi:10.3390/ijerph181910224
28. World Health Organization. Ten health issues WHO will tackle this year; 2022. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
29. Almalki OS, Alfayez OM, Al Yami MS, Asiri YA, Almohammed OA. Parents’ hesitancy to vaccinate their 5–11 year old children against COVID-19 in Saudi Arabia: predictors from the health belief model. Front Public Health. 2022;10:842862. doi:10.3389/fpubh.2022.842862
30. Aggarwal S, Madaan P, Sharma M. Vaccine hesitancy among parents of children with neurodevelopmental disabilities: a possible threat to COVID-19 vaccine coverage. J Child Neurol. 2022;37:99. doi:10.1177/08830738211042133
31. Yılmaz M, Sahin MK. Parents’ willingness and attitudes concerning the COVID-19 vaccine: a cross-sectional study. Int J Clin Pract. 2021;75:e14364. doi:10.1111/ijcp.14364
32. Alhazza SF, Altalhi AM, Alamri KM, et al. Parents’ hesitancy to vaccinate their children against COVID-19, a country-wide survey. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.755073
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.